
Early Postpartum Stress, Anxiety, Depression, and Resilience Development among Danish First-Time Mothers before and during First-Wave COVID-19 Pandemic

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Outcomes
2.2. Statistical Methods
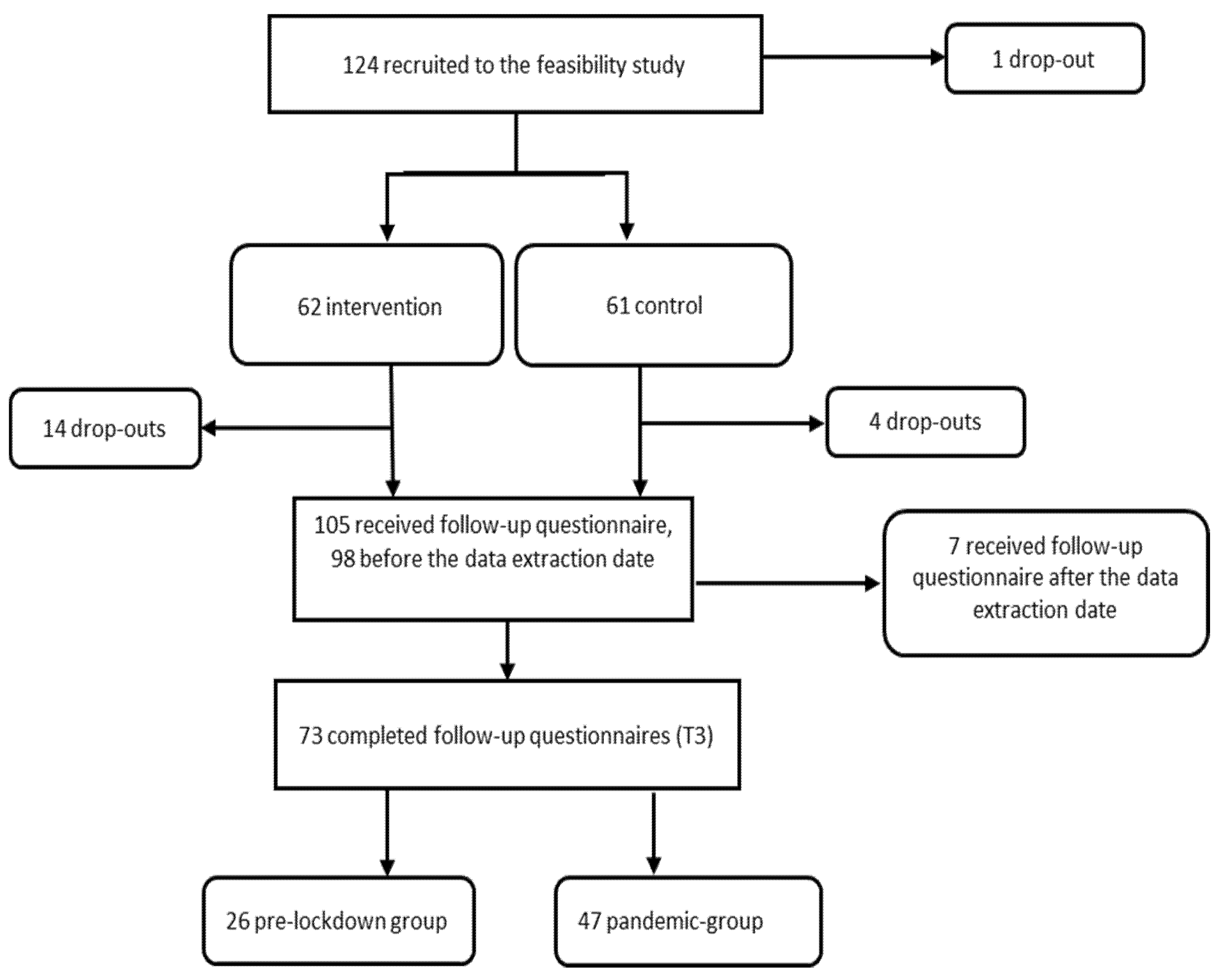
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Börnhorst, C.; Wijnhoven, T.M.A.; Kunešová, M.; Yngve, A.; Rito, A.I.; Lissner, L.; Duleva, V.; Petrauskiene, A.; Breda, J. WHO European Childhood Obesity Surveillance Initiative: Associations between sleep duration, screen time and food consumption frequencies. BMC Public Health 2015, 15, 442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sundhedstyrelsen. Håndtering af COVID-19: Retningslinje i den Kommunale Sundhedstjeneste for Børn og Unge (Sundhedsplejen); Sundhedstyrelsen [The National Board of Health]: Copenhagen, Denmark, 2020. [Google Scholar]
- Iversen, K.; Bundgaard, H.; Hasselbalch, R.B.; Kristensen, J.H.; Nielsen, P.B.; Pries-Heje, M.M.; Knudsen, A.D.; Christensen, C.E.; Fogh, K.; Norsk, J.B.; et al. Risk of COVID-19 in health-care workers in Denmark: An observational cohort study. Lancet Infect. Dis. 2020, 20, 1401–1408. [Google Scholar] [CrossRef]
- Galbally, M.; van Rossum, E.F.; Watson, S.; de Kloet, E.R.; Lewis, A. Trans-generational stress regulation: Mother-infant cortisol and maternal mental health across the perinatal period. Psychoneuroendocrinology 2019, 109, 104374. [Google Scholar] [CrossRef] [PubMed]
- Kurth, E.; Spichiger, E.; Cignacco, E.; Kennedy, H.P.; Glanzmann, R.; Schmid, M.; Staehelin, K.; Schindler, C.; Stutz, E.Z. Predictors of Crying Problems in the Early Postpartum Period. J. Obstet. Gynecol. Neonatal Nurs. 2010, 39, 250–262. [Google Scholar] [CrossRef] [PubMed]
- Martini, J.; Petzoldt, J.; Knappe, S.; Garthus-Niegel, S.; Asselmann, E.; Wittchen, H.-U. Infant, maternal, and familial predictors and correlates of regulatory problems in early infancy: The differential role of infant temperament and maternal anxiety and depression. Early Hum. Dev. 2017, 115, 23–31. [Google Scholar] [CrossRef] [PubMed]
- Petzoldt, J.; Wittchen, H.-U.; Einsle, F.; Martini, J. Maternal anxiety versus depressive disorders: Specific relations to infants’ crying, feeding and sleeping problems. Child Care Health Dev. 2016, 42, 231–245. [Google Scholar] [CrossRef] [PubMed]
- Whitaker, K.; Young-Hyman, D.; Vernon, M.; Wilcox, S. Maternal Stress Predicts Postpartum Weight Retention. Matern. Child Health J. 2014, 18, 2209–2217. [Google Scholar] [CrossRef] [Green Version]
- Suzuki, S. Psychological status of postpartum women under the COVID-19 pandemic in Japan. J. Matern. Neonatal Med. 2020, 1–3. [Google Scholar] [CrossRef] [PubMed]
- Ceulemans, M.; Hompes, T.; Foulon, V. Mental health status of pregnant and breastfeeding women during the COVID-19 pandemic: A call for action. Int. J. Gynecol. Obstet. 2020, 151, 146–147. [Google Scholar] [CrossRef] [PubMed]
- Oskovi-Kaplan, Z.A.; Buyuk, G.N.; Ozgu-Erdinc, A.S.; Keskin, H.L.; Ozbas, A.; Tekin, O.M. The Effect of COVID-19 Pandemic and Social Restrictions on Depression Rates and Maternal Attachment in Immediate Postpartum Women: A Preliminary Study. Psychiatr. Q. 2021, 92, 675–682. [Google Scholar] [CrossRef]
- Farewell, C.V.; Jewell, J.; Walls, J.; Leiferman, J.A. A Mixed-Methods Pilot Study of Perinatal Risk and Resilience During COVID-19. J. Prim. Care Community Health 2020, 11, 2150132720944074. [Google Scholar] [CrossRef]
- Mollard, E.; Kupzyk, K.; Moore, T. Postpartum stress and protective factors in women who gave birth in the United States during the COVID-19 pandemic. Women’s Health 2021, 17, 17455065211042190. [Google Scholar] [CrossRef] [PubMed]
- Lavoie, J.; Pereira, L.C.; Talwar, V. Children’s Physical Resilience Outcomes: Meta-Analysis of Vulnerability and Protective Factors. J. Pediatr. Nurs. 2016, 31, 701–711. [Google Scholar] [CrossRef] [PubMed]
- Traub, F.; Boynton-Jarrett, R. Modifiable Resilience Factors to Childhood Adversity for Clinical Pediatric Practice. Pediatrics 2017, 139, e20162569. [Google Scholar] [CrossRef] [PubMed]
- Zautra, A.J. Resilience: One part recovery, two parts sustainability. J. Pers. 2009, 77, 1935–1943. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. A global measure of perceived stress. J. Health Soc. Behav. 1983, 24, 385–396. [Google Scholar] [CrossRef]
- Connor, K.M.; Davidson, J.R. Development of a new resilience scale: The Connor-Davidson Resilience Scale (CD-RISC). Depress. Anxiety 2003, 18, 76–82. [Google Scholar] [CrossRef]
- Cohen, S.; Janicki-Deverts, D.; Miller, G.E. Psychological Stress and Disease. JAMA 2007, 298, 1685–1687. [Google Scholar] [CrossRef]
- Bak, P.L.; Midgley, N.; Zhu, J.L.; Wistoft, K.; Obel, C. The Resilience Program: Preliminary evaluation of a mentalization-based education program. Front. Psychol. 2015, 6, 753. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friese, M.; Messner, C.; Schaffner, Y. Mindfulness meditation counteracts self-control depletion. Conscious. Cogn. 2012, 21, 1016–1022. [Google Scholar] [CrossRef] [PubMed]
- Dawson, M.A.; Hamson-Utley, J.J.; Hansen, R.; Olpin, M. Examining the Effectiveness of Psychological Strategies on Physiologic Markers: Evidence-Based Suggestions for Holistic Care of the Athlete. J. Athl. Train. 2014, 49, 331–337. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lovibond, P.; Lovibond, S. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Eskildsen, A.; Dalgaard, V.L.; Nielsen, K.J.; Andersen, J.H.; Zachariae, R.; Olsen, L.R.; Jã¸rgensen, A.; Christiansen, D. Cross-cultural adaptation and validation of the Danish consensus version of the 10-item Perceived Stress Scale. Scand. J. Work. Environ. Health 2015, 41, 486–490. [Google Scholar] [CrossRef] [PubMed]
- Lauridsen, L.S.; Willert, M.V.; Eskildsen, A.; Christiansen, D. Cross-cultural adaptation and validation of the Danish 10-item Connor-Davidson Resilience Scale among hospital staff. Scand. J. Public Health 2017, 45, 654–657. [Google Scholar] [CrossRef] [PubMed]
- Danish Translation of DASS21. Available online: http://www2.psy.unsw.edu.au/dass//Danish/Danish.htm (accessed on 25 October 2020).
- Antony, M.M.; Bieling, P.J.; Cox, B.J.; Enns, M.W.; Swinson, R.P. Psychometric properties of the 42-item and 21-item versions of the Depression Anxiety Stress Scales in clinical groups and a community sample. Psychol. Assess. 1998, 10, 176–181. [Google Scholar] [CrossRef]
- Cunningham, N.K.; Brown, P.M.; Brooks, J.; Page, A. The structure of emotional symptoms in the postpartum period: Is it unique? J. Affect. Disord. 2013, 151, 686–694. [Google Scholar] [CrossRef]
- Moreno, C.; Wykes, T.; Galderisi, S.; Nordentoft, M.; Crossley, N.; Jones, N.; Cannon, M.; Correll, C.U.; Byrne, L.; Carr, S.; et al. How mental health care should change as a consequence of the COVID-19 pandemic. Lancet Psychiatry 2020, 7, 813–824. [Google Scholar] [CrossRef]
- Pariente, G.; Broder, O.W.; Sheiner, E.; Battat, T.L.; Mazor, E.; Salem, S.Y.; Kosef, T.; Wainstock, T. Risk for probable post-partum depression among women during the COVID-19 pandemic. Women Ment. Health 2020, 23, 767–773. [Google Scholar] [CrossRef]
- 1615 L. St NW, Suite 800Washington, og D. 20036USA202-419-4300|M.-857-8562|F.-419-4372|M. Inquiries. COVID-19 Response Approved by Most in 14 Nations with Advanced Economies. Pew Research Center’s Global Attitudes Project. 27 August 2020. Available online: https://www.pewresearch.org/global/2020/08/27/most-approve-of-national-response-to-covid-19-in-14-advanced-economies/ (accessed on 28 August 2020).
- Mappa, I.; Distefano, F.A.; Rizzo, G. Effects of coronavirus 19 pandemic on maternal anxiety during pregnancy: A prospectic observational study. J. Périnat. Med. 2020, 48, 545–550. [Google Scholar] [CrossRef]
- Berthelot, N.; Lemieux, R.; Garon-Bissonnette, J.; Drouin-Maziade, C.; Martel, É.; Maziade, M. Uptrend in distress and psychiatric symptomatology in pregnant women during the coronavirus disease 2019 pandemic. Acta Obstet. Gynecol. Scand. 2020, 99, 848–855. [Google Scholar] [CrossRef]


{kind=link}
| Pre-Lockdown Group (n = 26) | Pandemic Group (n = 47) | |||||
|---|---|---|---|---|---|---|
| % | Mean | SD | % | Mean | SD | |
| Allocation group | ||||||
| Intervention | 50.0 | 38.3 | ||||
| Control | 50.0 | 61.7 | ||||
| Civil status | ||||||
| Living with partner | 96.1 | 100 | ||||
| Single | 3.9 | 0 | ||||
| Education | ||||||
| High school or less | 11.5 | 10.6 | ||||
| Low up to 3 y | 3.9 | 4.3 | ||||
| Medium, 3–5 y | 30.8 | 34.0 | ||||
| High > 5 | 53.9 | 51.1 | ||||
| Age (years) | 30.2 | 3.9 | 30.7 | 3.4 | ||
| Gestational age (weeks) | 40.2 | 1.3 | 40.0 | 1.2 | ||
| Birth weight (g) | 3596 | 529 | 3453 | 410 | ||
| Pre-pregnancy BMI (kg/m2) | 23.4 | 2.7 | 23.2 | 2.8 | ||
| PSS T0 (Score) | 10.7 | 5.8 | 12.1 | 4.5 | ||
| DASS T0 Stress (Score) | 6.0 | 5.3 | 7.0 | 5.6 | ||
| DASS T0 Anxiety (Score) | 2.7 | 3.3 | 2.7 | 2.8 | ||
| DASS T0 Depression (Score) | 1.4 | 1.7 | 2.2 | 2.2 | ||
| CD-RISC T0 (Score) | 95.7 | 7.8 | 96.3 | 9.9 | ||
| Pre-Lockdown (n = 26) | Pandemic Group (n = 47) | Differences between Pre-Lockdown and Pandemic Group, Crude | Differences between Pre-Lockdown and Pandemic Group, Adjusted | ||||||
|---|---|---|---|---|---|---|---|---|---|
| Change from baseline to follow-up, adjusted | 95% CI | Change from baseline to follow-up, adjusted | 95% CI | Difference, group means | 95% CI | Difference, group means | 95% CI | p-value | |
| PSS | 1.12 | −1.39; 3.62 | 1.82 | −0.07; 3.71 | −0.43 | −4.1; 3.3 | 0.70 | −2.45; 3.85 | 0.66 |
| DASS Stress | 1.85 | −0.40; 4.11 | 1.10 | −0.62; 2.81 | 1.16 | −4.2; 1.8 | −0.76 | −3.59; 2.08 | 0.60 |
| DASS Anxiety | −0.99 | −2.03; 0.04 | −0.52 | −1.31; 0.27 | 0.56 | −0.98; 2.11 | 0.47 | −0.84; 1.77 | 0.48 |
| DASS Depression | 0.29 | −1.15; 1.74 | 1.17 | 0.08; 2.27 | 0.59 | −1.2; 2.4 | 0.88 | −0.95; 2.71 | 0.34 |
| CD-RISC | 0.36 | −3.12; 3.83 | 1.55 | −1.04; 4.14 | 0.89 | −3.8; 5.6 | 1.19 | −3.16; 5.54 | 0.59 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ladekarl, M.; Olsen, N.J.; Winckler, K.; Brødsgaard, A.; Nøhr, E.A.; Heitmann, B.L.; Specht, I.O. Early Postpartum Stress, Anxiety, Depression, and Resilience Development among Danish First-Time Mothers before and during First-Wave COVID-19 Pandemic. Int. J. Environ. Res. Public Health 2021, 18, 11734. https://doi.org/10.3390/ijerph182211734
Ladekarl M, Olsen NJ, Winckler K, Brødsgaard A, Nøhr EA, Heitmann BL, Specht IO. Early Postpartum Stress, Anxiety, Depression, and Resilience Development among Danish First-Time Mothers before and during First-Wave COVID-19 Pandemic. International Journal of Environmental Research and Public Health. 2021; 18(22):11734. https://doi.org/10.3390/ijerph182211734
Chicago/Turabian StyleLadekarl, Monica, Nanna Julie Olsen, Karoline Winckler, Anne Brødsgaard, Ellen Aagaard Nøhr, Berit Lilienthal Heitmann, and Ina Olmer Specht. 2021. "Early Postpartum Stress, Anxiety, Depression, and Resilience Development among Danish First-Time Mothers before and during First-Wave COVID-19 Pandemic" International Journal of Environmental Research and Public Health 18, no. 22: 11734. https://doi.org/10.3390/ijerph182211734
APA StyleLadekarl, M., Olsen, N. J., Winckler, K., Brødsgaard, A., Nøhr, E. A., Heitmann, B. L., & Specht, I. O. (2021). Early Postpartum Stress, Anxiety, Depression, and Resilience Development among Danish First-Time Mothers before and during First-Wave COVID-19 Pandemic. International Journal of Environmental Research and Public Health, 18(22), 11734. https://doi.org/10.3390/ijerph182211734