
Health Care Services Utilization of Persons with Direct, Indirect and without Migration Background in Germany: A Longitudinal Study Based on the German Socio-Economic Panel (SOEP)



Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Measures
2.3. Statistical Analysis
3. Results
3.1. Sample Characteristics
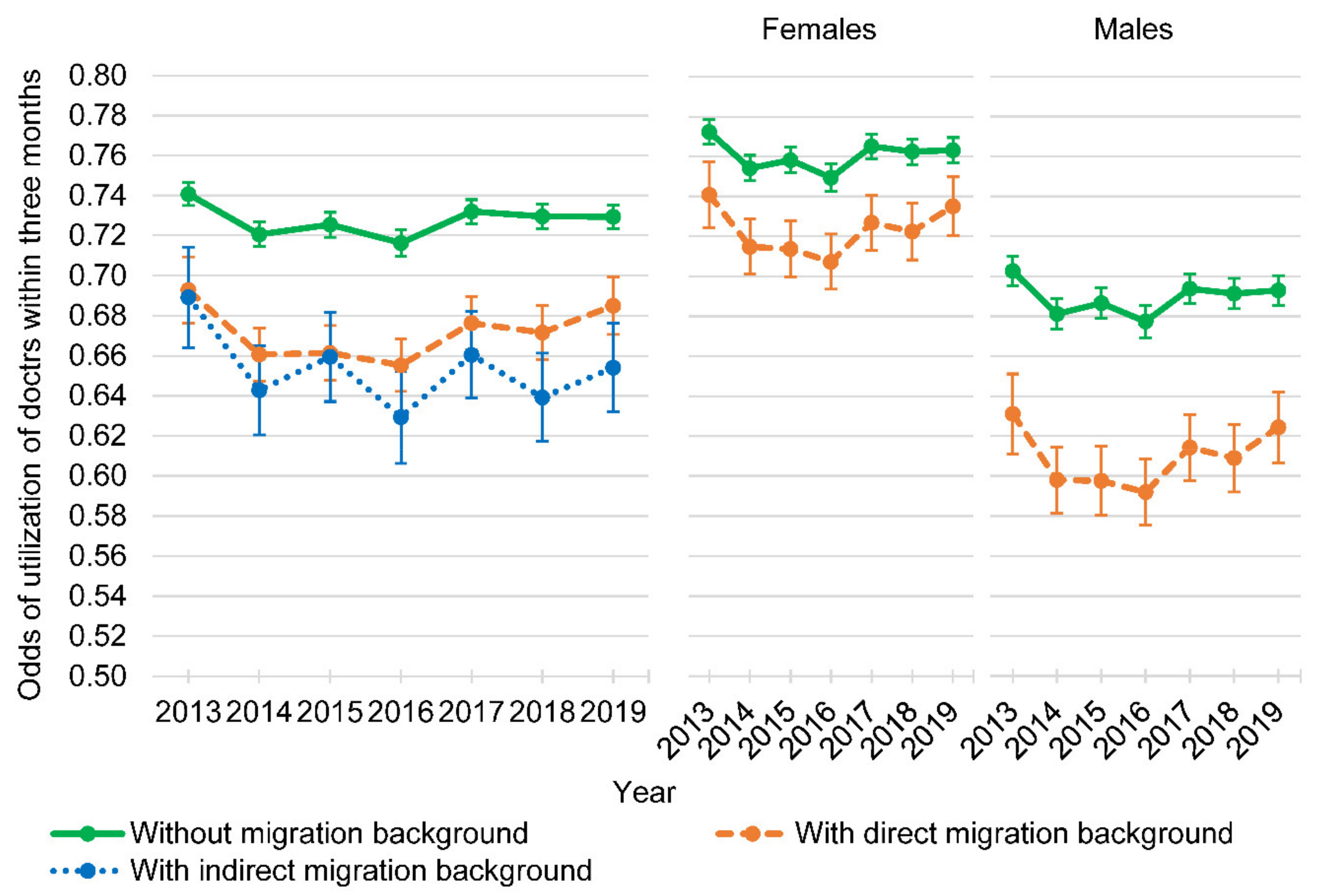
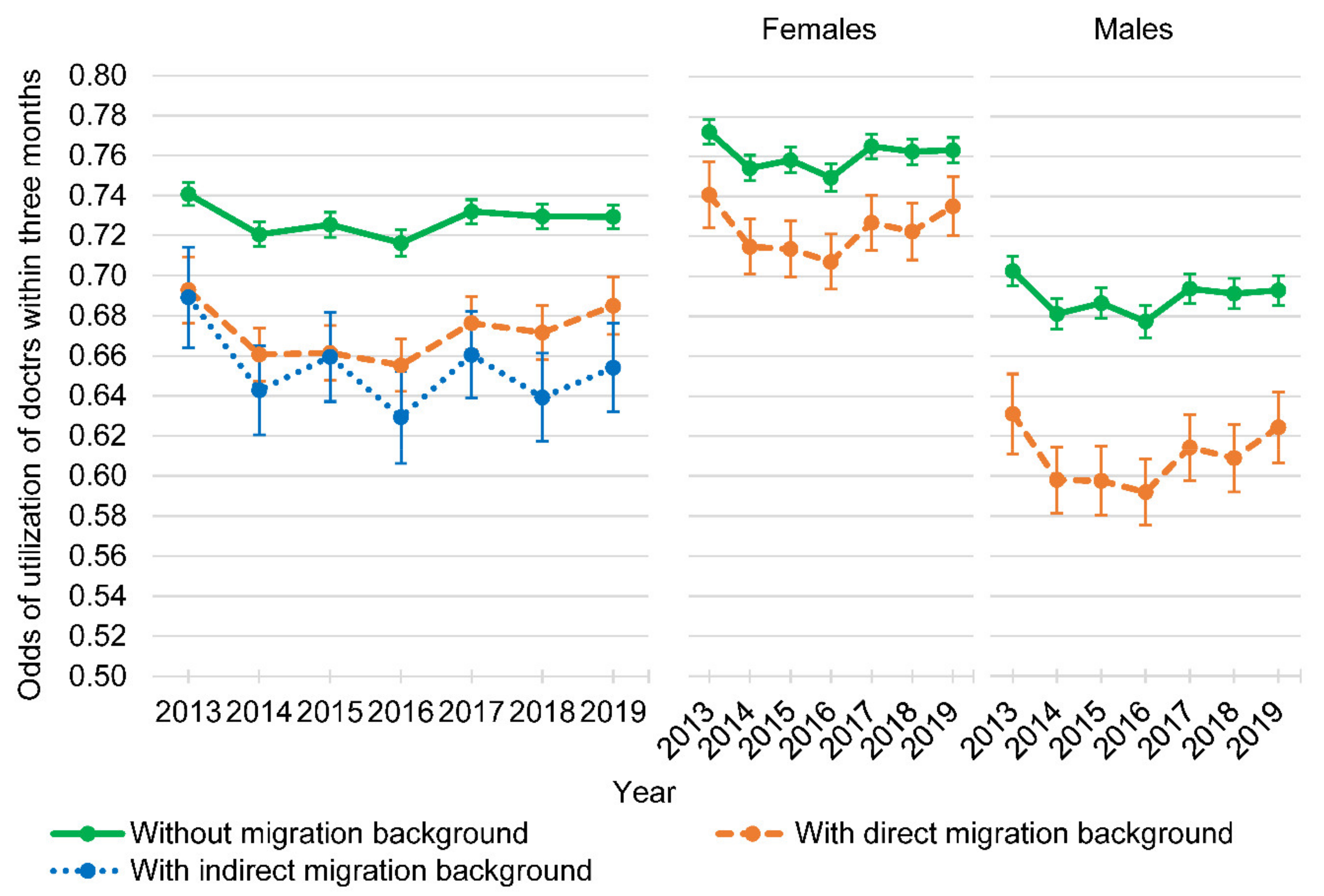
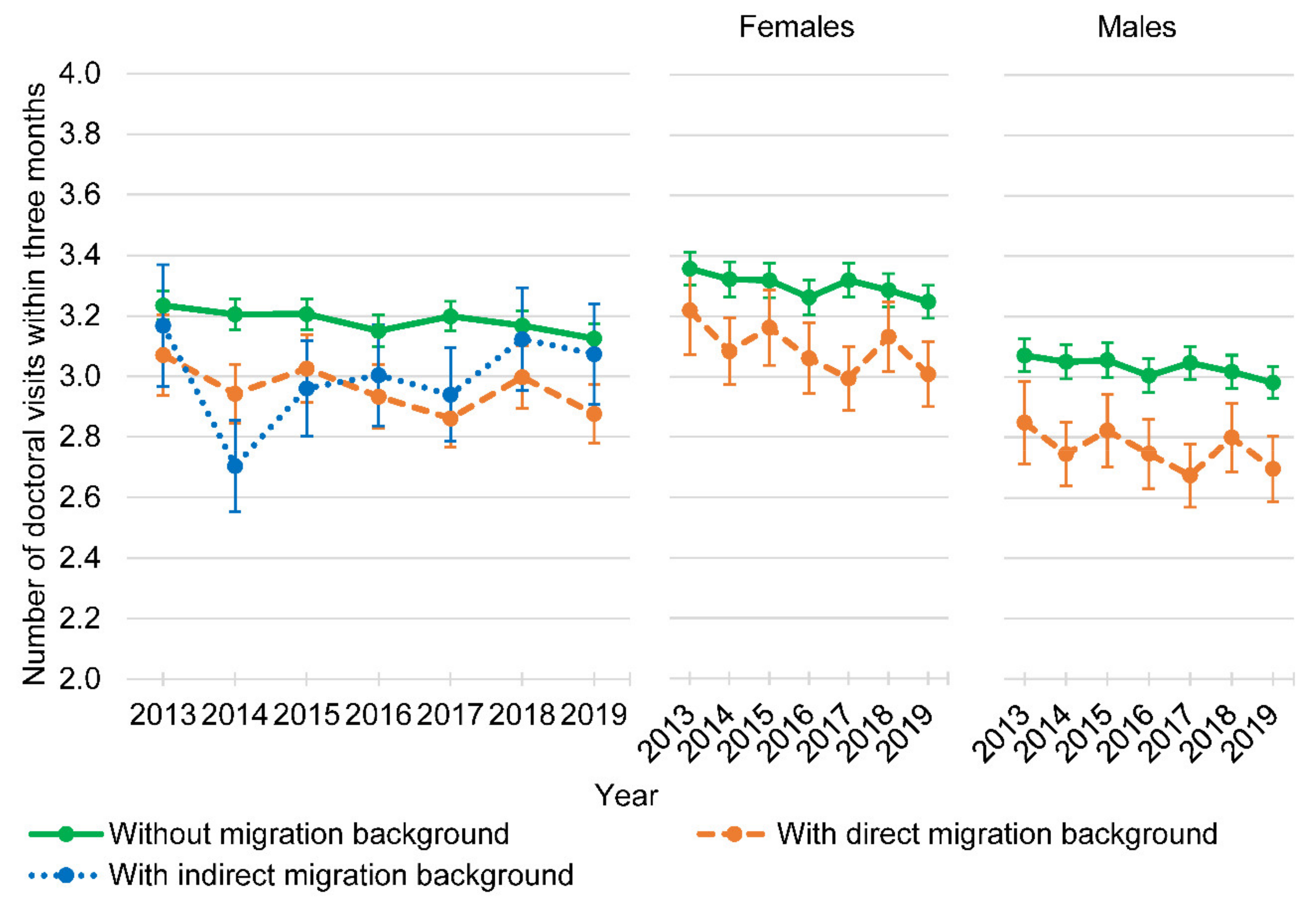
3.2. Doctoral Visits within Three Months
3.3. Nights in Hospital within the Last Year
4. Discussion
4.1. Main Findings
4.2. Previous Research and Possible Explanations
4.3. Generalizability
4.4. Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Statistisches Bundesamt (Destatis). Migration und Integration. Bevölkerung nach Migrationshintergrund und Geschlecht. Available online: https://www.destatis.de/DE/Themen/Gesellschaft-Umwelt/Bevoelkerung/Migration-Integration/Tabellen/liste-migrationshintergrund-geschlecht.html (accessed on 11 June 2021).
- Salt, J. Trends in Europe’s international migration. In Migration and Health in the European Union; Rechel, B., Mladovsky, P., Devillé, W., Rijks, B., Petrova-Benedit, R., Eds.; Open University Press: New York, NY, USA, 2011; pp. 17–36. [Google Scholar]
- Razum, O.; Karrasch, L.; Spallek, J. Migration: A neglected dimension of inequalities in health? Bundesgesundheitsblatt Gesundheitsforschung Gesundh. 2016, 59, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Razum, O. Migration, Mortalität und der Healthy-migrant-Effekt. In Gesundheitliche Ungleichheit: Grundlagen, Probleme, Perspektiven; Richter, M., Hurrelmann, K., Eds.; VS Verlag für Sozialwissenschaften: Wiesbaden, Germany, 2009; pp. 267–282. [Google Scholar]
- Klein, J.; von dem Knesebeck, O. Inequalities in health care utilization among migrants and non-migrants in Germany: A systematic review. Int. J. Equity Health 2018, 17, 160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Graetz, V.; Rechel, B.; Groot, W.; Norredam, M.; Pavlova, M. Utilization of health care services by migrants in Europe-a systematic literature review. Br. Med. Bull. 2017, 121, 5–18. [Google Scholar] [CrossRef] [PubMed]
- Andersen, R.; Newman, J.F. Societal and individual determinants of medical care utilization in the United States. Milbank Mem. Fund Q. Health Soc. 1973, 51, 95–124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Andersen, R.; Davidson, P. Improving access to care in America: Individual and contextual indicators. In Changing the US Health Care System: Key Issues in Health Services Policy and Management; Kominski, G.F., Ed.; Jossey-Bass: San Fransisco, CA, USA, 2014. [Google Scholar]
- Grochtdreis, T.; König, H.-H.; Dams, J. Health-related quality of life of persons with direct, indirect and no migration background in Germany: A cross-sectional study based on the German Socio-Economic Panel (SOEP). Int. J. Environ. Res. Public Health 2021, 18, 3665. [Google Scholar] [CrossRef]
- Nesterko, Y.; Braehler, E.; Grande, G.; Glaesmer, H. Life satisfaction and health-related quality of life in immigrants and native-born Germans: The role of immigration-related factors. Qual. Life Res. 2013, 22, 1005–1013. [Google Scholar] [CrossRef]
- Morawa, E.; Erim, Y. Health-related quality of life and sense of coherence among Polish immigrants in Germany and indigenous Poles. Transcult Psychiatry 2015, 52, 376–395. [Google Scholar] [CrossRef] [Green Version]
- Glaesmer, H.; Wittig, U.; Braehler, E.; Martin, A.; Mewes, R.; Rief, W. Health care utilization among first and second generation immigrants and native-born Germans: A population-based study in Germany. Int. J. Public Health 2011, 56, 541–548. [Google Scholar] [CrossRef]
- Nesterko, Y.; Turrion, C.M.; Friedrich, M.; Glaesmer, H. Trajectories of health-related quality of life in immigrants and non-immigrants in Germany: A population-based longitudinal study. Int. J. Public Health 2019, 64, 49–58. [Google Scholar] [CrossRef]
- Igel, U.; Brähler, E.; Grande, G. The influence of perceived discrimination on health in migrants. Psychiatr. Prax. 2010, 37, 183–190. [Google Scholar] [CrossRef]
- Razum, O.; Rohrmann, S. The healthy migrant effect: Role of selection and late entry bias. Gesundheitswesen 2002, 64, 82–88. [Google Scholar] [CrossRef] [PubMed]
- Aarabi, G.; Reissmann, D.R.; Seedorf, U.; Becher, H.; Heydecke, G.; Kofahl, C. Oral health and access to dental care-a comparison of elderly migrants and non-migrants in Germany. Ethn. Health 2018, 23, 703–717. [Google Scholar] [CrossRef] [PubMed]
- Aparicio, M.L.; Döring, A.; Mielck, A.; Holle, R. Differences between Eastern European immigrants of German origin and the rest of the German population in health status, health care use and health behaviour: A comparative study using data from the KORA-Survey 2000. Soz. Prav. 2005, 50, 107–118. [Google Scholar] [CrossRef] [PubMed]
- Brenne, S.; David, M.; Borde, T.; Breckenkamp, J.; Razum, O. Are women with and without migration background reached equally well by health services? The example of antenatal care in Berlin. Bundesgesundheitsblatt Gesundheitsforschung Gesundh. 2015, 58, 569–576. [Google Scholar] [CrossRef]
- David, M.; Borde, T.; Brenne, S.; Henrich, W.; Breckenkamp, J.; Razum, O. Caesarean Section Frequency among Immigrants, Second- and Third-Generation Women, and Non-Immigrants: Prospective Study in Berlin/Germany. PLoS ONE 2015, 10, e0127489. [Google Scholar] [CrossRef] [PubMed]
- David, M.; Borde, T.; Brenne, S.; Ramsauer, B.; Henrich, W.; Breckenkamp, J.; Razum, O. Comparison of Perinatal Data of Immigrant Women of Turkish Origin and German Women-Results of a Prospective Study in Berlin. Geburtshilfe Frauenheilkd 2014, 74, 441–448. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- David, M.; Schwartau, I.; Anand Pant, H.; Borde, T. Emergency outpatient services in the city of Berlin: Factors for appropriate use and predictors for hospital admission. Eur. J. Emerg. Med. 2006, 13, 352–357. [Google Scholar] [CrossRef] [PubMed]
- Geyer, S.; Peter, R.; Siegrist, J. Socioeconomic differences in children’s and adolescents’ hospital admissions in Germany: A report based on health insurance data on selected diagnostic categories. J. Epidemiol. Community Health 2002, 56, 109–114. [Google Scholar] [CrossRef] [PubMed]
- Kavuk, I.; Weimar, C.; Kim, B.T.; Gueneyli, G.; Araz, M.; Klieser, E.; Katsarava, Z. One-year prevalence and socio-cultural aspects of chronic headache in Turkish immigrants and German natives. Cephalalgia 2006, 26, 1177–1181. [Google Scholar] [CrossRef]
- Koller, D.; Lack, N.; Mielck, A. Social differences in the utilisation of prenatal screening, smoking during pregnancy and birth weight--empirical analysis of data from the Perinatal Study in Bavaria (Germany). Gesundheitswesen 2009, 71, 10–18. [Google Scholar] [CrossRef]
- Reime, B.; Lindwedel, U.; Ertl, K.M.; Jacob, C.; Schücking, B.; Wenzlaff, P. Does underutilization of prenatal care explain the excess risk for stillbirth among women with migration background in Germany? Acta Obstet. Gynecol. Scand. 2009, 88, 1276–1283. [Google Scholar] [CrossRef]
- Simoes, E.; Kunz, S.; Schmahl, F. Utilisation gradients in prenatal care prompt further development of the prevention concept. Gesundheitswesen 2009, 71, 385–390. [Google Scholar] [CrossRef] [PubMed]
- Spallek, J.; Lehnhardt, J.; Reeske, A.; Razum, O.; David, M. Perinatal outcomes of immigrant women of Turkish, Middle Eastern and North African origin in Berlin, Germany: A comparison of two time periods. Arch. Gynecol. Obstet. 2014, 289, 505–512. [Google Scholar] [CrossRef] [PubMed]
- Zeeb, H.; Baune, B.T.; Vollmer, W.; Cremer, D.; Krämer, A. Health situation of and health service provided for adult migrants—A survey conducted during school admittance examinations. Gesundheitswesen 2004, 66, 76–84. [Google Scholar] [CrossRef]
- Bächle, C.; Haastert, B.; Holl, R.W.; Beyer, P.; Grabert, M.; Giani, G.; Icks, A. Inpatient and outpatient health care utilization of children and adolescents with type 1 diabetes before and after introduction of DRGs. Exp. Clin. Endocrinol. Diabetes 2010, 118, 644–648. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fassmer, A.M.; Luque Ramos, A.; Boiselle, C.; Dreger, S.; Helmer, S.; Zeeb, H. Tabakkonsum und Inanspruchnahme medizinischer Leistungen im Jugendalter–Eine Analyse der KIGGS Daten. Gesundheitswesen 2019, 81, 17–23. [Google Scholar] [CrossRef] [PubMed]
- Gruber, S.; Kiesel, M. Inequality in health care utilization in Germany? Theoretical and empirical evidence for specialist consultation. J. Public Health 2010, 18, 351–365. [Google Scholar] [CrossRef]
- Hirschfeld, G.; Wager, J.; Zernikow, B. Physician consultation in young children with recurrent pain-a population-based study. PeerJ 2015, 3, e916. [Google Scholar] [CrossRef] [Green Version]
- Huber, J.; Lampert, T.; Mielck, A. Inequalities in health risks, morbidity and health care of children by health insurance of their parents (statutory vs. private health insurance): Results of the German KiGGS study. Gesundheitswesen 2012, 74, 627–638. [Google Scholar] [CrossRef] [PubMed]
- Icks, A.; Rosenbauer, J.; Strassburger, K.; Grabert, M.; Giani, G.; Holl, R.W. Persistent social disparities in the risk of hospital admission of paediatric diabetic patients in Germany-prospective data from 1277 diabetic children and adolescents. Diabet. Med. 2007, 24, 440–442. [Google Scholar] [CrossRef]
- Kamtsiuris, P.; Bergmann, E.; Rattay, P.; Schlaud, M. Use of medical services. Results of the German Health Interview and Examination Survey for Children and Adolescents (KiGGS). Bundesgesundheitsblatt Gesundheitsforschung Gesundh. 2007, 50, 836–850. [Google Scholar] [CrossRef]
- Bermejo, I.; Frank, F.; Maier, I.; Hölzel, L.P. Health care utilisation of migrants with mental disorders compared with Germans. Psychiatr. Prax. 2012, 39, 64–70. [Google Scholar] [CrossRef]
- Sundmacher, L.; Kopetsch, T. Waiting times in the ambulatory sector—The case of chronically ill patients. Int. J. Equity Health 2013, 12, 77. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brücker, H.; Kroh, M.; Bartsch, S.; Goebel, J.; Kühne, S.; Liebau, E.; Schupp, J. The New IAB-SOEP Migration Sample: An Introduction into the Methodology and the Contents. SOEP Survey Paper 216, Series C; DIW Berlin: Berlin/Nürnberg, Germany, 2014. [Google Scholar]
- SOEP Group. SOEP-Core v34–PPATHL: Person-Related Meta-Dataset. SOEP Survey Papers 762: Series D–Variable Descriptions and Coding; DIW Berlin/SOEP: Berlin, Germany, 2019. [Google Scholar]
- United Nations Statistics Division Standard Country or Area Codes for Statistical Use (M49); United Nations: New York, NY, USA, 2020.
- Rabe-Hesketh, S.; Skrondal, A. Multilevel and Longitudinal Modeling Using Stata; Stata Press Publication: College Station, TX, USA, 2012. [Google Scholar]
- Hilbe, J.M. Modeling Count Data; Cambridge University Press: New York, NY, USA, 2014. [Google Scholar]
- Bermejo, I.; Holzel, L.P.; Kriston, L.; Harter, M. Barriers in the attendance of health care interventions by immigrants. Bundesgesundheitsblatt Gesundheitsforschung Gesundh. 2012, 55, 944–953. [Google Scholar] [CrossRef] [PubMed]
- Ciupitu, C.C.; Babitsch, B. Why is it not working? Identifying barriers to the therapy of paediatric obesity in an intercultural setting. J. Child Health Care 2011, 15, 140–150. [Google Scholar] [CrossRef] [PubMed]
- Rechel, B.; Mladovsky, P.; Ingleby, D.; Mackenbach, J.P.; McKee, M. Migration and health in an increasingly diverse Europe. Lancet 2013, 381, 1235–1245. [Google Scholar] [CrossRef]
- Babitsch, B.; Gohl, D.; von Lengerke, T. Re-revisiting Andersen’s Behavioral Model of Health Services Use: A systematic review of studies from 1998-2011. Psychosoc. Med. 2012, 9, Doc11. [Google Scholar] [CrossRef]
- Thode, N.; Bergmann, E.; Kamtsiuris, P.; Kurth, B.M. Predictors for ambulatory medical care utilization in Germany. Bundesgesundheitsblatt Gesundheitsforschung Gesundh. 2005, 48, 296–306. [Google Scholar] [CrossRef] [Green Version]
- Alemi, Q.; Stempel, C.; Koga, P.M.; Smith, V.; Danis, D.; Baek, K.; Montgomery, S. Determinants of Health Care Services Utilization among First Generation Afghan Migrants in Istanbul. Int. J. Environ. Res. Public Health 2017, 14, 201. [Google Scholar] [CrossRef] [Green Version]
- Baykara-Krumme, H.; Milewski, N. Fertility Patterns Among Turkish Women in Turkey and Abroad: The Effects of International Mobility, Migrant Generation, and Family Background. Eur. J. Popul. 2017, 33, 409–436. [Google Scholar] [CrossRef]
- Pötsch, O. Fertility in Germany before and after the 2011 census: Still no trend reversal in sight. Comp. Popul. Stud. 2016, 41, 87–118. [Google Scholar] [CrossRef]
- Kaus, W.; Mundil-Schwarz, R. Die Ermittlung der Einwohnerzahlen und der demografischen Strukturen nach dem Zensus 2011. WISTA Wirtsch. Stat. 2015, 4, 18–38. [Google Scholar]


{kind=link}
{kind=link}
| Sociodemographic Characteristic | Persons without Migration Background (n = 32,535) | Persons with Direct Migration Background (n = 8080) | Persons with Indirect Migration Background (n = 3306) |
|---|---|---|---|
| Age: Mean (SD) | 47.16 (17.98) | 42.00 (14.16) *** | 30.17 (12.07) *** |
| Grouped age: n (%) | |||
| 18–24 | 4641 (14.26) | 773 (9.57) *** | 1465 (44.31) *** |
| 25–34 | 4038 (12.41) | 1864 (23.07) | 729 (22.05) |
| 35–44 | 5573 (17.13) | 2364 (29.26) | 678 (20.51) |
| 45–54 | 7123 (21.89) | 1555 (19.25) | 289 (8.74) |
| 55–64 | 5002 (15.37) | 905 (11.20) | 113 (3.42) |
| ≥65 | 6158 (18.93) | 619 (7.66) | 32 (0.97) |
| Sex: n (%) | |||
| Female | 16,892 (51.92) | 4338 (53.69) ** | 1713 (51.81) |
| Male | 15,643 (48.08) | 3742 (46.31) | 1593 (48.19) |
| Marital status: n (%) | |||
| Never married/single | 9754 (29.98) | 1661 (20.56) *** | 1990 (60.19) *** |
| Married/in partnership | 17,364 (53.37) | 5386 (66.66) | 1085 (32.82) |
| Separated/divorced | 3779 (11.62) | 838 (10.37) | 211 (6.38) |
| Widowed | 1638 (5.03) | 195 (2.41) | 20 (0.60) |
| Employment status: n (%) | |||
| Employed fulltime | 12,691 (39.01) | 3171 (39.25) *** | 1106 (33.45) *** |
| Employed part-time | 4635 (14.25) | 1075 (13.30) | 346 (10.47) |
| Apprenticeship | 1110 (3.41) | 191 (2.36) | 297 (8.98) |
| Marginally employed | 1952 (6.00) | 656 (8.12) | 289 (8.74) |
| Other employment 1 | 290 (0.89) | 21 (0.26) | 33 (1.00) |
| Unemployed | 11,857 (36.44) | 2966 (36.71) | 1235 (37.36) |
| Nationality: n (%) | |||
| German | 32,535 (100.00) | 3573 (44.22) *** | 2573 (77.83) *** |
| East European | - | 1419 (17.56) | 10 (0.30) |
| South European | - | 1260 (15.59) | 376 (11.37) |
| West and North European 2 | - | 382 (4.73) | 43 (1.30) |
| African | - | 178 (2.20) | 9 (0.27) |
| Asian | - | 1123 (13.90) | 286 (8.65) |
| American/Oceanian | - | 128 (1.58) | 8 (0.24) |
| Stateless/ethnic minority | - | 17 (0.21) | 1 (0.03) |
| Independent Variables | Without Migration Background vs. with Direct Migration Background | Without Migration Background vs. with Indirect Migration Background | ||
|---|---|---|---|---|
| OR (SE) † | Exp(β) (SE) ‡ | OR (SE) † | Exp(β) (SE) ‡ | |
| Migration background (Ref. without migration background) | ||||
| With direct migration background | 0.73 (0.05) *** | 0.94 (0.02) * | ||
| With indirect migration background | 0.99 (0.09) | 0.99 (0.04) | ||
| Age | 1.03 (0.00) *** | 1.00 (0.00) *** | 1.03 (0.00) *** | 1.00 (0.00) *** |
| Sex (Ref. male) | ||||
| Female | 1.60 (0.04) *** | 1.08 (0.01) *** | 1.60 (0.04) *** | 1.08 (0.01) *** |
| Marital status (Ref. married/in partnership) | ||||
| Never married/single | 1.16 (0.03) *** | 0.98 (0.01) | 1.18 (0.04) *** | 0.97 (0.01) * |
| Separated/divorced | 1.03 (0.03) | 1.08 (0.01) *** | 1.00 (0.04) | 1.08 (0.01) *** |
| Widowed | 1.02 (0.06) | 1.00 (0.02) | 1.04 (0.06) | 0.99 (0.02) |
| Employment status (Ref. employed fulltime) | ||||
| Employed part-time | 1.14 (0.03) *** | 1.00 (0.01) | 1.15 (0.03) *** | 1.00 (0.01) |
| Apprenticeship | 1.99 (0.11) *** | 1.07 (0.02) *** | 1.94 (0.10) *** | 1.05 (0.02) ** |
| Marginally employed | 1.25 (0.04) *** | 1.06 (0.01) *** | 1.26 (0.05) *** | 1.06 (0.01) *** |
| Other employment 1 | 1.88 (0.20) *** | 1.12 (0.04) *** | 1.78 (0.19) *** | 1.10 (0.04) ** |
| Unemployed | 1.70 (0.04) *** | 1.24 (0.01) *** | 1.65 (0.04) *** | 1.22 (0.01) *** |
| Migration background * Sex (Ref. no migration background * male) | ||||
| Direct migration background * Female | 1.21 (0.06) *** | 1.01 (0.02) | ||
| Indirect migration background * Female | 1.32 (0.10) *** | 1.08 (0.03) ** | ||
| Survey year | Yes | Yes | Yes | Yes |
| Migration background * Survey year | Yes | Yes | Yes | Yes |
| Constant | 0.48 (0.02) *** | 2.24 (0.04) *** | 0.49 (0.03) *** | 2.27 (0.04) *** |
| Random effect: Person-ID | ||||
| Variance (Constant) | 2.12 (0.04) | 0.24 (0.00) | 2.16 (0.04) | 0.24 (0.00) |
| Independent Variables | Without Migration Background vs. with Direct Migration Background | Without Migration Background vs. with Indirect Migration Background | ||
|---|---|---|---|---|
| OR (SE) † | Exp(β) (SE) ‡ | OR (SE) † | Exp(β) (SE) ‡ | |
| Migration background (Ref. without migration background) | ||||
| With direct migration background | 0.79 (0.06) ** | 0.93 (0.06) | ||
| With indirect migration background | 0.82 (0.10) | 1.16 (0.15) | ||
| Age | 1.01 (0.00) *** | 1.01 (0.00) *** | 1.01 (0.00) *** | 1.01 (0.00) *** |
| Sex (Ref. male) | ||||
| Female | 1.05 (0.03) * | 0.95 (0.02) * | 1.05 (0.03) | 0.95 (0.02) * |
| Marital status (Ref. married/in partnership) | ||||
| Never married/single | 0.79 (0.03) *** | 1.06 (0.03) * | 0.77 (0.03) *** | 1.05 (0.03) |
| Separated/divorced | 1.23 (0.04) *** | 1.17 (0.03) * | 1.19 (0.04) *** | 1.19 (0.03) |
| Widowed | 1.17 (0.05) *** | 1.09 (0.03) *** | 1.16 (0.05) *** | 1.06 (0.03) *** |
| Employment status (Ref. employed fulltime) | ||||
| Employed part-time | 1.03 (0.04) | 1.02 (0.03) | 1.06 (0.04) | 1.02 (0.03) |
| Apprenticeship | 1.54 (0.11) *** | 1.15 (0.09) | 1.64 (0.11) *** | 1.24 (0.09) ** |
| Marginally employed | 1.33 (0.06) *** | 1.08 (0.04) | 1.38 (0.07) *** | 1.06 (0.05) |
| Other employment 1 | 1.90 (0.22) *** | 1.15 (0.12) | 1.83 (0.22) *** | 1.09 (0.11) |
| Unemployed | 2.73 (0.07) *** | 1.34 (0.03) *** | 2.68 (0.08) *** | 1.33 (0.03) *** |
| Migration background * Sex (Ref. no migration background * male) | ||||
| Direct migration background * Female | 1.21 (0.07) *** | 1.00 (0.05) | 1.40 (0.13) *** | 1.03 (0.09) |
| Survey year | Yes | Yes | Yes | Yes |
| Migration background * Survey year | Yes | Yes | Yes | Yes |
| Constant | 0.04 (0.00) *** | 3.53 (0.15) *** | 0.04 (0.00) *** | 3.58 (0.16) *** |
| Random effect: Person-ID | ||||
| Variance(Constant) | 1.32 (0.04) | 0.46 (0.01) | 1.35 (0.04) | 0.47 (0.01) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Grochtdreis, T.; König, H.-H.; Dams, J. Health Care Services Utilization of Persons with Direct, Indirect and without Migration Background in Germany: A Longitudinal Study Based on the German Socio-Economic Panel (SOEP). Int. J. Environ. Res. Public Health 2021, 18, 11640. https://doi.org/10.3390/ijerph182111640
Grochtdreis T, König H-H, Dams J. Health Care Services Utilization of Persons with Direct, Indirect and without Migration Background in Germany: A Longitudinal Study Based on the German Socio-Economic Panel (SOEP). International Journal of Environmental Research and Public Health. 2021; 18(21):11640. https://doi.org/10.3390/ijerph182111640
Chicago/Turabian StyleGrochtdreis, Thomas, Hans-Helmut König, and Judith Dams. 2021. "Health Care Services Utilization of Persons with Direct, Indirect and without Migration Background in Germany: A Longitudinal Study Based on the German Socio-Economic Panel (SOEP)" International Journal of Environmental Research and Public Health 18, no. 21: 11640. https://doi.org/10.3390/ijerph182111640
APA StyleGrochtdreis, T., König, H.-H., & Dams, J. (2021). Health Care Services Utilization of Persons with Direct, Indirect and without Migration Background in Germany: A Longitudinal Study Based on the German Socio-Economic Panel (SOEP). International Journal of Environmental Research and Public Health, 18(21), 11640. https://doi.org/10.3390/ijerph182111640