
The Effectiveness of Intervening on Social Isolation to Reduce Mortality during Heat Waves in Aged Population: A Retrospective Ecological Study



 ,
,
Abstract
:1. Introduction
2. Methods
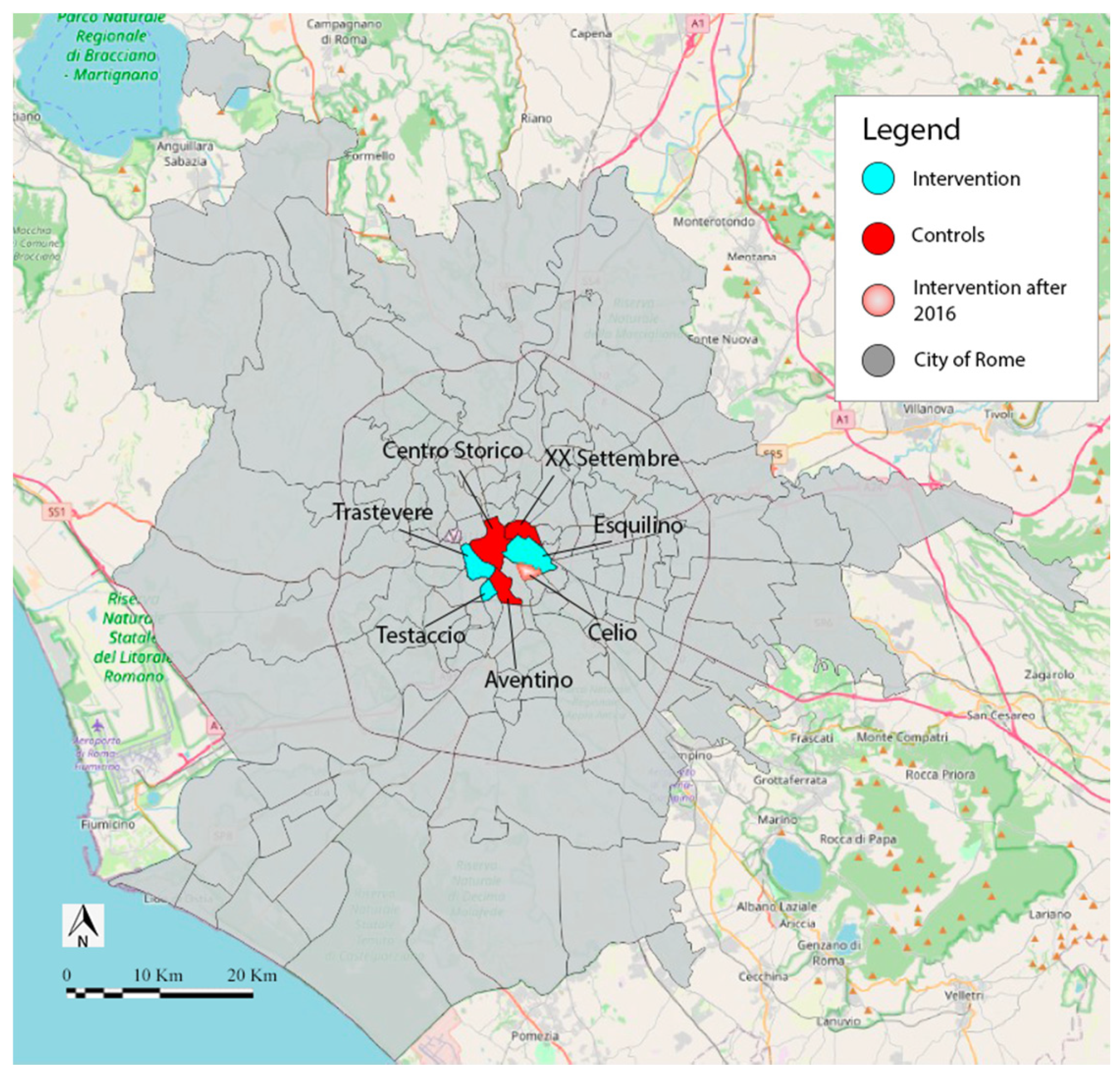
2.1. The Intervention
2.2. Population
2.3. Measures or Variables
2.4. Statistical Analyses
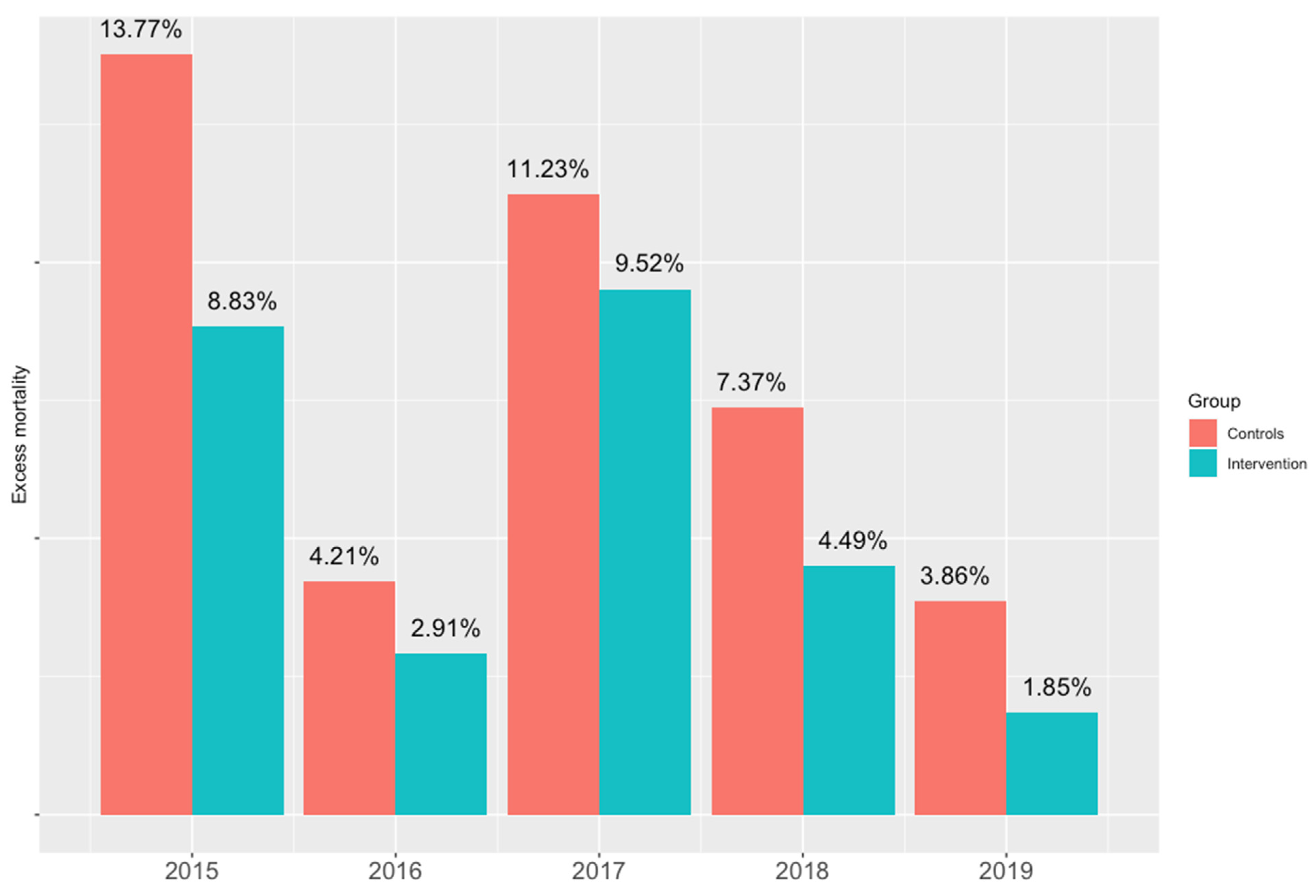
3. Results
4. Discussion
- Possible confounders not included in the analysis
- Population level mitigation measures
- Regional health systems’ capacities
- Number of phone calls from friends or neighbors in the general population
- Number of visits from friends or neighbors in the general population
- Frequency and duration of the above visits/calls
- Action performed by the visitors (bring food or medication, drive the partici-pants to medical appointments and/or to pharmacies to collect medications, drive respondents to go shopping)
- Illness distribution in the two populations
- Drug consumption in the two populations
- Causes of deaths in the two populations
- Impact of these factors on nursing home residents included in the study
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Benmarhnia, T.; Deguen, S.; Kaufman, J.S.; Smargiassi, A. Vulnerability to heat-related mortality: A systematic review, meta-analysis, and meta-regression analysis. Epidemiology 2015, 26, 781–793. [Google Scholar] [PubMed]
- Oudin Åström, D.; Bertil, F.; Joacim, R. Heat wave impact on morbidity and mortality in the elderly population: A review of recent studies. Maturitas 2011, 69, 99–105. [Google Scholar] [CrossRef] [PubMed]
- Barriopedro, D.; Fischer, E.M.; Luterbacher, J.; Trigo, R.M.; García-Herrera, R. The Hot Summer of 2010: Redrawing the Temperature Record Map of Europe. Science 2011, 332, 220–224. Available online: https://www.science.org/doi/abs/10.1126/science.1201224 (accessed on 26 October 2021). [CrossRef] [PubMed] [Green Version]
- Han, J.; Liu, S.; Zhang, J.; Zhou, L.; Fang, Q.; Zhang, J.; Zhang, Y. The impact of temperature extremes on mortality: A time-series study in Jinan, China. BMJ Open 2017, 7, e014741. Available online: http://bmjopen.bmj.com/content/7/4/e014741.abstract (accessed on 30 June 2021). [CrossRef] [PubMed]
- Xu, X.; Chen, Z.; Huo, X.; Wang, C.; Li, N.; Meng, X.; Wang, Q.; Liu, Q.; Bi, P.; Li, J. The effects of temperature on human mortality in a Chinese city: Burden of disease calculation, attributable risk exploration, and vulnerability identification. Int. J. Biometeorol. 2019, 63, 1319–1329. [Google Scholar] [CrossRef] [PubMed]
- Ellena, M.; Ballester, J.; Mercogliano, P.; Ferracin, E.; Barbato, G.; Costa, G.; Ingole, V. Social inequalities in heat-attributable mortality in the city of Turin, northwest of Italy: A time series analysis from 1982 to 2018. Environ. Health 2020, 19, 116. [Google Scholar] [CrossRef] [PubMed]
- Marí-Dell’Olmo, M.; Tobías, A.; Gómez-Gutiérrez, A.; Rodríguez-Sanz, M.; De Olalla, P.G.; Camprubí, E.; Gasparrini, A.; Borrell, C. Social inequalities in the association between temperature and mortality in a South European context. Int. J. Public Health 2018, 64, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Ministry of Health of Italy. Ondate di Calore (Heat Waves). 2021. Available online: https://www.salute.gov.it/portale/caldo/homeCaldo.jsp (accessed on 30 June 2021).
- Martínez-Solanas, È.; Basagaña, X. Temporal changes in temperature-related mortality in Spain and effect of the implementation of a Heat Health Prevention Plan. Environ. Res. 2018, 169, 102–113. Available online: https://www.sciencedirect.com/science/article/pii/S0013935118305759 (accessed on 30 June 2021). [CrossRef] [PubMed]
- Gardiner, C.; Geldenhuys, G.; Gott, M. Interventions to reduce social isolation and loneliness among older people: An integrative review. Health Soc. Care Community 2016, 26, 147–157. [Google Scholar] [CrossRef] [PubMed]
- Weiss, R.S. Loneliness: The Experience of Emotional and Social Isolation; The MIT Press: Cambridge, MA, USA, 1973; p. 236. [Google Scholar]
- Ernst, J.M.; Cacioppo, J.T. Lonely hearts: Psychological perspectives on loneliness. Appl. Prev. Psychol. 2000, 8, 1–22. Available online: https://www.sciencedirect.com/science/article/pii/S0962184999800080 (accessed on 30 June 2021). [CrossRef]
- Courtin, E.; Knapp, M. Social isolation, loneliness and health in old age: A Scoping Review. Health Soc. Care Community 2017, 25, 799–8121. Available online: https://pubmed.ncbi.nlm.nih.gov/26712585/ (accessed on 3 September 2021). [CrossRef] [PubMed]
- Co, L.; Ba, L. Loneliness and the health of older people. Int. J. Geriatr. Psychiatry 2008, 23, 1213–1221. Available online: https://pubmed.ncbi.nlm.nih.gov/18537197/ (accessed on 3 September 2021).
- Bouchama, A.; Dehbi, M.; Mohamed, G.; Matthies, F.; Shoukri, M.; Menne, B. Prognostic Factors in Heat Wave–Related DeathsA Meta-analysis. Arch. Intern. Med. 2007, 167, 2170–2176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liotta, G.; Gilardi, F.; Scarcella, P.; Orlando, S.; Mancinelli, S.; Buonomo, E. Trend and determinants of acute inpatient care for the elderly in italy from 2001 to 2011. Ann Ig 2016, 28, 5. [Google Scholar]
- Comune di Roma. I Numeri di Roma Capitale-Municipio I. 2019. Available online: https://www.comune.roma.it/web/it/i-numeri-di-roma-capitale-municipio-i.page (accessed on 30 October 2021).
- Liotta, G.; Inzerilli, M.C.; Palombi, L.; Madaro, O.; Orlando, S.; Scarcella, P.; Betti, D.; Marazzi, M.C. Social Interventions to Prevent Heat-Related Mortality in the Older Adult in Rome, Italy: A Quasi-Experimental Study. Int. J. Environ. Res. Public Health 2018, 15, 715. Available online: https://pubmed.ncbi.nlm.nih.gov/29641436 (accessed on 30 June 2021). [CrossRef] [Green Version]
- Ministry of Health of Italy. Domande e Risposte-FAQ Ondate di Calore. 2021. Available online: https://www.salute.gov.it/portale/caldo/dettaglioFaqCaldo.jsp?lingua=italiano&id=98#:~:text=Le%ondate%di%caloresono,rischio%per%la%salute%della (accessed on 30 October 2021).
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2021. [Google Scholar]
- Aragon, T.J. Epitools: Epidemiology Tools. R Package; Version 0.5-10.1. Available online: https://cran.r-project.org/web/packages/epitools/index.html (accessed on 3 November 2021).
- Athens, J. A Toolbox for Public Health and Epidemiology. Available online: https://cran.r-project.org/web/packages/pubh/pubh.pdf (accessed on 3 November 2021).
- Lüdecke, D. sjPlot: Data Visualization for Statistics in Social Science; R Package Version 2.8.9. 2021. Available online: https://strengejacke.github.io/sjPlot/ (accessed on 3 November 2021).
- Consul, P.; Famoye, F. Generalized poisson regression model. Commun. Stat.-Theory Methods 1992, 21, 89–109. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Independent Variables | Controls | Intervention | Total | p | Distribution |
|---|---|---|---|---|---|
| (n = 20) | (n = 22) | (n = 42) | |||
| Average population over 80 (2015–2019) | 720.2 [650.5; 1479.8] | 760.8 [602.4; 2146.7] | 720.2 [602.4; 1479.8] | 1.000 | non-normal |
| Average age | 48.1 [47.6; 49.2] | 47.1 [47.0; 48.4] | 48.1 [47.1; 48.4] | 0.034 * | non-normal |
| Percentage of population over 75 | 13.6 [12.3; 15.2] | 11.6 [10.9; 14.0] | 13.3 [11.6; 14.0] | 0.006 ** | non-normal |
| Percentage of population over 90 | 11.2 [9.6; 11.7] | 8.8 [7.4; 11.4] | 9.6 [8.8; 11.4] | 0.001 | non-normal |
| Ageing index × 100 (population > 65/population < 15) | 255.2 [240.6; 273.9] | 228.2 [219.0; 245.8] | 240.6 [228.2; 255.2] | 0.000 *** | non-normal |
| Dependency index × 100 (population > 65 + population < 15 over total) | 55.7 [53.7; 56.6] | 52.6 [52.1; 57.3] | 55.7 [52.6; 57.3] | 0.366 | non-normal |
| Masculinity index (man/women × 100) | 94.5 [87.3; 100.0] | 94.5 [83.0; 97.3] | 94.5 [84.8; 97.3] | 0.093 | non-normal |
| Cadastral income (100 sq-meters) | 17.9 [16.4; 19.8] | 16.7 [13.7; 17.3] | 16.7 [16.4; 17.9] | 0.015 * | non-normal |
| Winter mortality | 34.0 ± 10.9 | 36.4 ± 8.2 | 35.3 ± 9.5 | 0.464 | normal |
| Variables | IRR | IRR | IRR | IRR | IRR |
|---|---|---|---|---|---|
| (Intercept) | 0.01 *** (0.01–0.01) | 0.01 *** (0.00–0.01) | 0.00 *** (0.00–0.01) | 0.10 *** (0.02–0.38) | 0.02 *** (0.01–0.04) |
| group: Intervention | 0.76 * (0.59–0.98) | ||||
| High heat wave level | 1.49 ** (1.11–2.03) | ||||
| Winter mortality | 1.02 * (1.00–1.04) | ||||
| Cadastral income (100 sq-meters) | 0.87 *** (0.80–0.94) | ||||
| Proportion of people over 90 | 0.94 (0.85–1.03) | ||||
| Observations | 30 | 30 | 30 | 30 | 30 |
| R2 Nagelkerke | 0.141 | 0.220 | 0.165 | 0.325 | 0.053 |
| Variables | Excess Mortality Rate | |
|---|---|---|
| Incidence Rate Ratios | CI | |
| (Intercept) | 1.82 | 0.21–14.55 |
| group: Intervention | 0.44 *** | 0.32–0.60 |
| High heat wave level | 1.57 ** | 1.16–2.17 |
| Cadestral income | 0.77 *** | 0.70–0.85 |
| Winter mortality | 1 | 0.98–1.02 |
| Proportion of people over 90 | 0.92 | 0.84–1.01 |
| Observations | 30 | |
| R2 Nagelkerke | 0.802 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Orlando, S.; Mosconi, C.; De Santo, C.; Emberti Gialloreti, L.; Inzerilli, M.C.; Madaro, O.; Mancinelli, S.; Ciccacci, F.; Marazzi, M.C.; Palombi, L.; et al. The Effectiveness of Intervening on Social Isolation to Reduce Mortality during Heat Waves in Aged Population: A Retrospective Ecological Study. Int. J. Environ. Res. Public Health 2021, 18, 11587. https://doi.org/10.3390/ijerph182111587
Orlando S, Mosconi C, De Santo C, Emberti Gialloreti L, Inzerilli MC, Madaro O, Mancinelli S, Ciccacci F, Marazzi MC, Palombi L, et al. The Effectiveness of Intervening on Social Isolation to Reduce Mortality during Heat Waves in Aged Population: A Retrospective Ecological Study. International Journal of Environmental Research and Public Health. 2021; 18(21):11587. https://doi.org/10.3390/ijerph182111587
Chicago/Turabian StyleOrlando, Stefano, Claudia Mosconi, Carolina De Santo, Leonardo Emberti Gialloreti, Maria Chiara Inzerilli, Olga Madaro, Sandro Mancinelli, Fausto Ciccacci, Maria Cristina Marazzi, Leonardo Palombi, and et al. 2021. "The Effectiveness of Intervening on Social Isolation to Reduce Mortality during Heat Waves in Aged Population: A Retrospective Ecological Study" International Journal of Environmental Research and Public Health 18, no. 21: 11587. https://doi.org/10.3390/ijerph182111587
APA StyleOrlando, S., Mosconi, C., De Santo, C., Emberti Gialloreti, L., Inzerilli, M. C., Madaro, O., Mancinelli, S., Ciccacci, F., Marazzi, M. C., Palombi, L., & Liotta, G. (2021). The Effectiveness of Intervening on Social Isolation to Reduce Mortality during Heat Waves in Aged Population: A Retrospective Ecological Study. International Journal of Environmental Research and Public Health, 18(21), 11587. https://doi.org/10.3390/ijerph182111587