
SARC-F and the Risk of Falling in Middle-Aged and Older Community-Dwelling Postmenopausal Women


 ,
,  , , ,
, , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
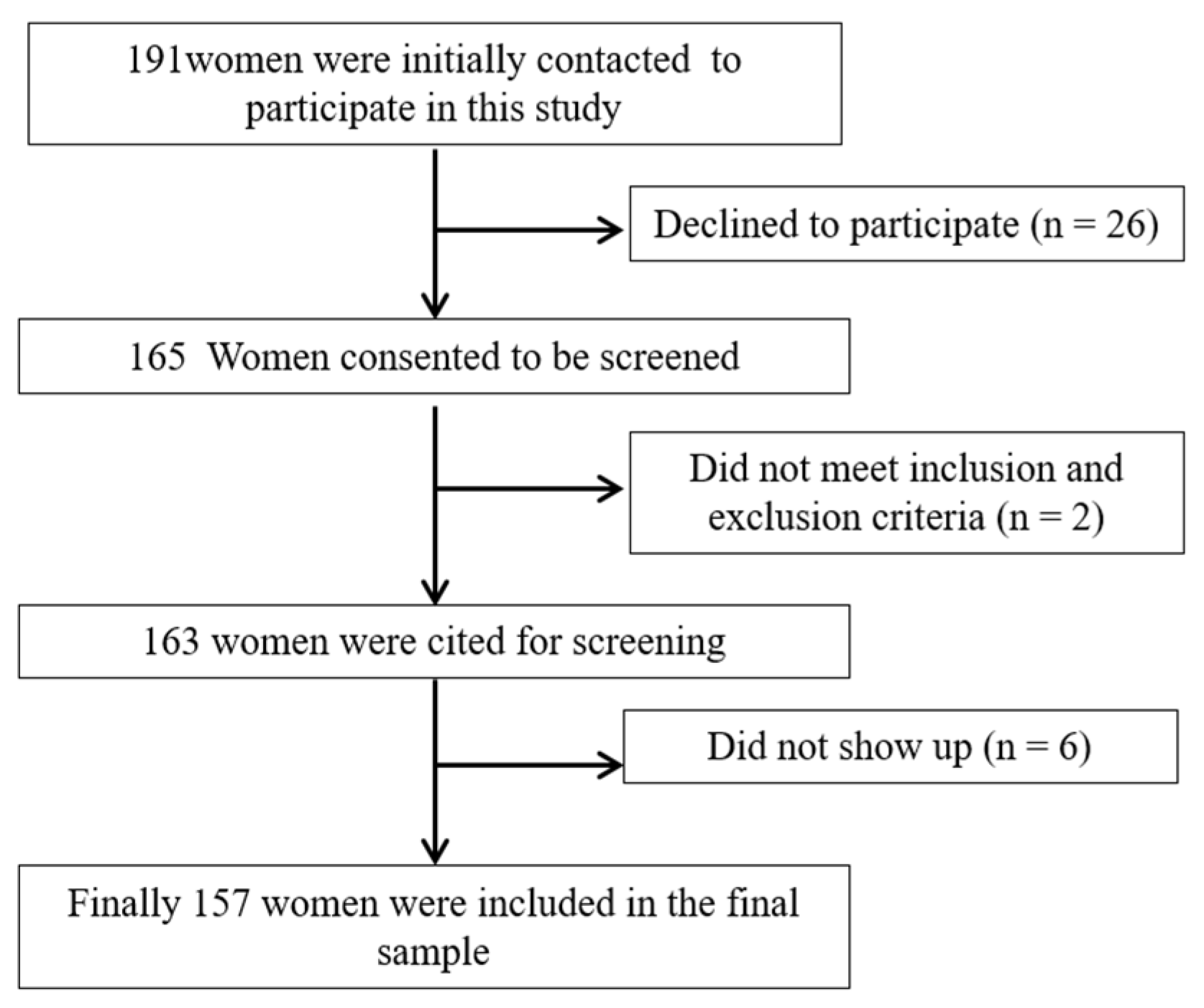
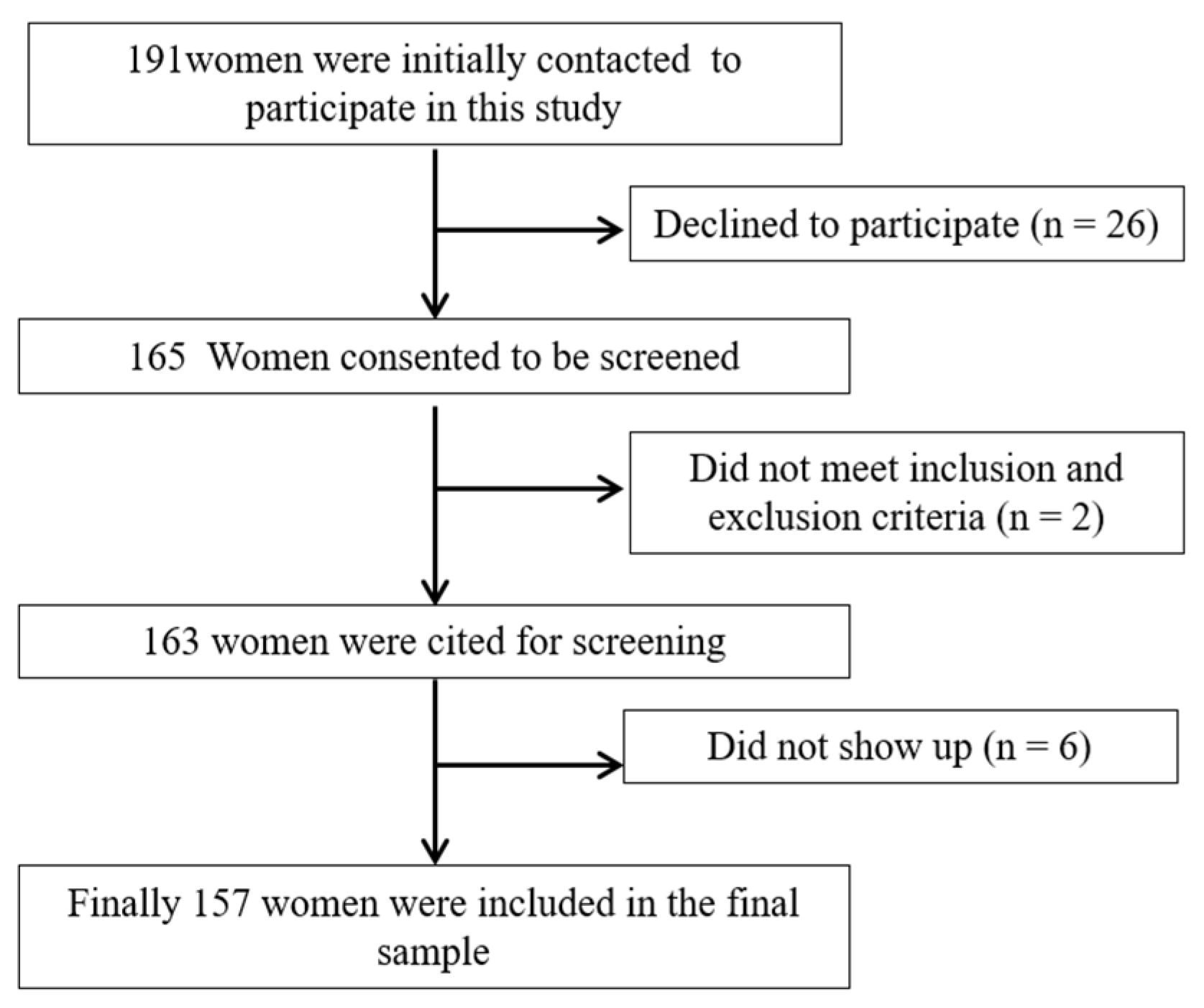
2.1. Study Design and Participants
2.2. Outcomes
2.2.1. Risk of Sarcopenia
2.2.2. Fear of Falling
2.2.3. Balance Confidence
2.2.4. Anxiety and Depression
2.2.5. Fatigue Severity
2.3. Sample Size Calculation
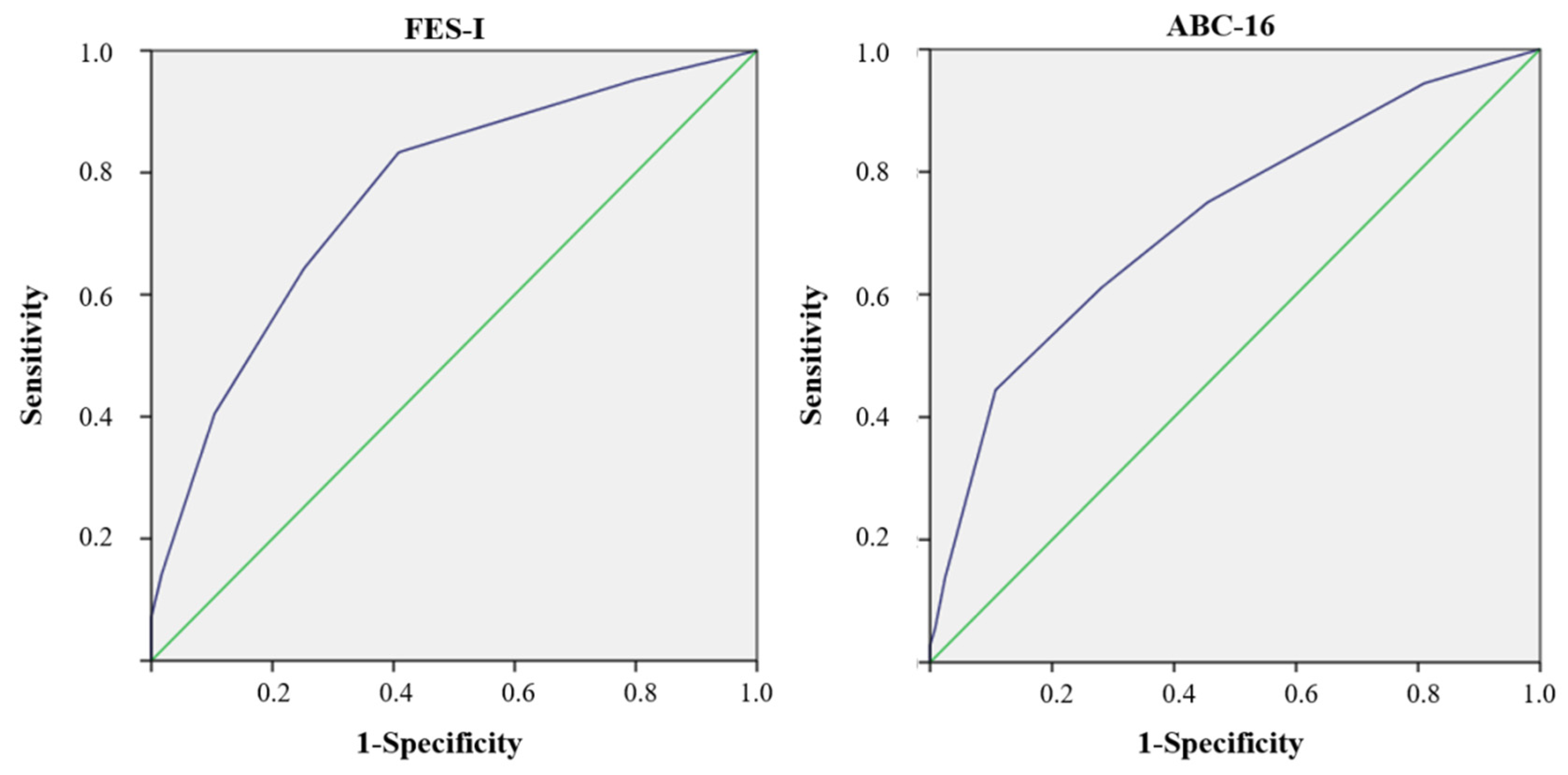
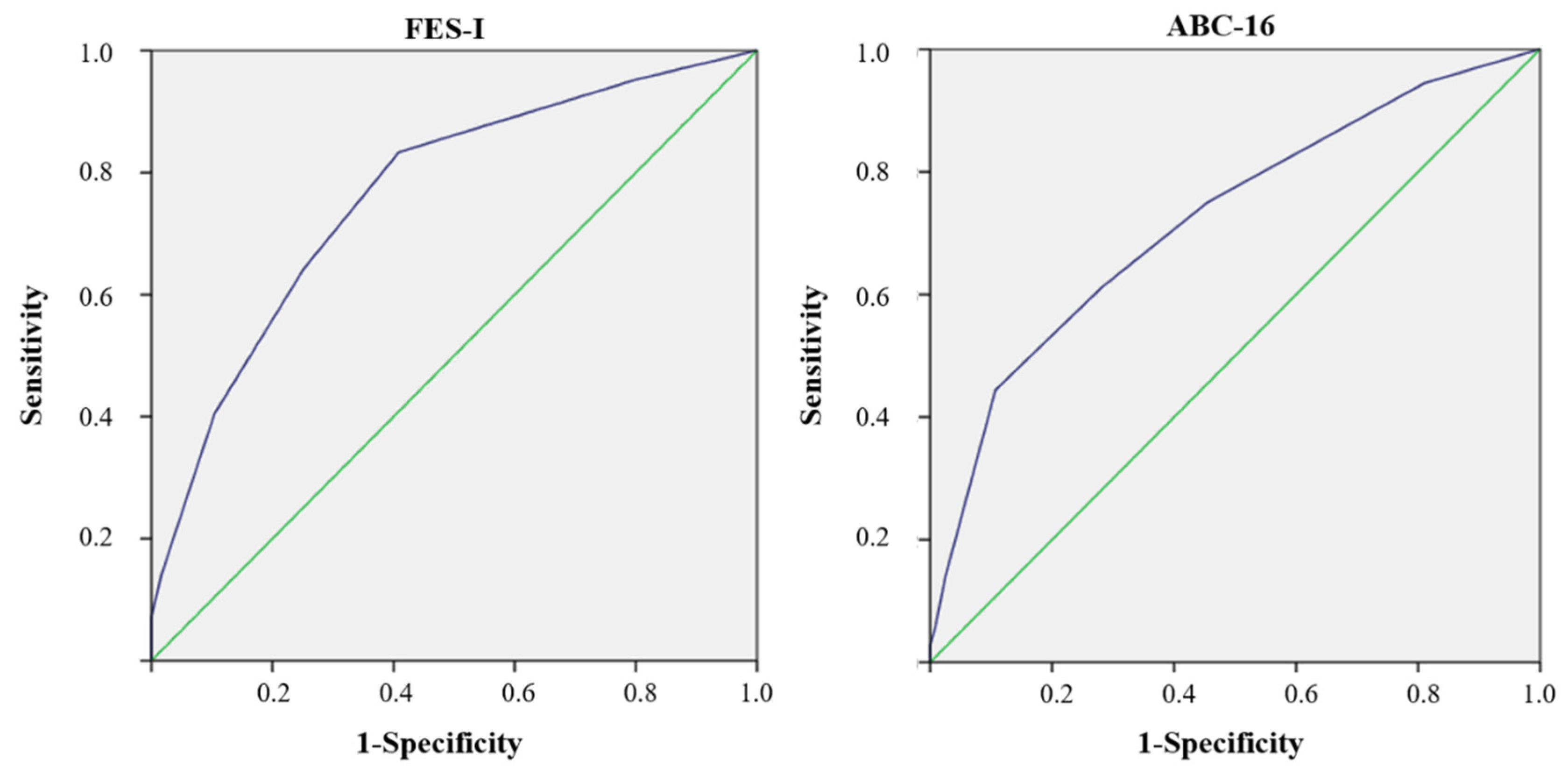
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Peel, N.M. Epidemiology of falls in older age. Can. J. Aging 2011, 30, 7–19. [Google Scholar] [CrossRef]
- James, S.L.; Lucchesi, L.R.; Bisignano, C.; Castle, C.D.; Dingels, Z.V.; Fox, J.T.; Hamilton, E.B.; Henry, N.J.; Krohn, K.J.; Liu, Z.; et al. The global burden of falls: Global, regional and national estimates of morbidity and mortality from the Global Burden of Disease Study 2017. Inj. Prev. 2020, 26, i3–i11. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. A Global Report on Falls Prevention. Epidemiology of Falls; WHO: Geneva, Switzerland, 2007; Available online: https://extranet.who.int/agefriendlyworld/wp-content/uploads/2014/06/WHo-Global-report-on-falls-prevention-in-older-age.pdf (accessed on 12 September 2021).
- Do, M.T.; Chang, V.C.; Kuran, N.; Thompson, W. Fall-related injuries among Canadian seniors, 2005-2013: An analysis of the Canadian Community Health Survey. Health Promot. Chronic Dis. Prev. Can. 2015, 35, 99–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sayyah, M.; Khosravi, G.; Bigdeli, M. Frequency of fall-related injuries of female patients referred to the trauma center in the city of Kashan from years 2005 to 2008. Chin. J. Traumatol. 2013, 16, 46–50. [Google Scholar] [PubMed]
- Hita-Contreras, F.; Martínez-Amat, A.; Cruz-Díaz, D.; Pérez-López, F.R. Osteosarcopenic obesity and fall prevention strategies. Maturitas 2015, 80, 126–132. [Google Scholar] [CrossRef] [PubMed]
- Landers, M.R.; Oscar, S.; Sasaoka, J.; Vaughn, K. Balance Confidence and Fear of Falling Avoidance Behavior Are Most Predictive of Falling in Older Adults: Prospective Analysis. Phys. Ther. 2016, 96, 433–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tinetti, M.E.; Powell, L. Fear of falling and low self-efficacy: A case of dependence in elderly persons. J. Gerontol. 1993, 48, 35–38. [Google Scholar] [CrossRef] [PubMed]
- Powell, L.E.; Myers, A.M. The Activities-specific Balance Confidence (ABC) Scale. J. Gerontol. A Biol. Sci. Med. Sci. 1995, 50, M28–M34. [Google Scholar] [CrossRef]
- Hita-Contreras, F.; Martínez-Amat, A.; Lomas-Vega, R.; Álvarez, P.; Mendoza, N.; Romero-Franco, N.; Aránega, A. Relationship of body mass index and body fat distribution with postural balance and risk of falls in Spanish postmenopausal women. Menopause 2013, 20, 202–208. [Google Scholar] [CrossRef]
- Cheng, M.H.; Wang, S.J.; Yang, F.Y.; Wang, P.H.; Fuh, J.L. Menopause and physical performance--a community-based cross-sectional study. Menopause 2009, 16, 892–896. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Beaudart, C.; Zaaria, M.; Pasleau, F.; Reginster, J.Y.; Bruyère, O. Health outcomes of sarcopenia: A systematic review and meta-analysis. PLoS ONE 2017, 12, e0169548. [Google Scholar] [CrossRef] [Green Version]
- Malmstrom, T.K.; Miller, D.K.; Simonsick, E.M.; Ferrucci, L.; Morley, J.E. SARC-F: A symptom score to predict persons with sarcopenia at risk for poor functional outcomes. J. Cachexia Sarcopenia Muscle 2016, 7, 28–36. [Google Scholar] [CrossRef]
- Yeung, S.S.Y.; Reijnierse, E.M.; Pham, V.K.; Trappenburg, M.C.; Lim, W.K.; Meskers, C.G.M.; Maier, A.B. Sarcopenia and its association with falls and fractures in older adults: A systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 2019, 10, 485–500. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, X.; Huang, P.; Dou, Q.; Wang, C.; Zhang, W.; Yang, Y.; Wang, J.; Xie, X.; Zhou, J.; Zeng, Y. Falls among older adults with sarcopenia dwelling in nursing home or community: A meta-analysis. Clin. Nutr. 2020, 39, 33–39. [Google Scholar] [CrossRef] [Green Version]
- Veronese, N.; Smith, L.; Barbagallo, M.; Yang, L.; Zou, L.; Haro, J.M.; Koyanagi, A. Sarcopenia and fall-related injury among older adults in five low- and middle-income countries. Exp. Gerontol. 2021, 147, 111262. [Google Scholar] [CrossRef]
- Lamb, S.E.; Jørstad-Stein, E.C.; Hauer, K.; Becker, C. Prevention of Falls Network Europe and Outcomes Consensus Group Development of a common outcomedata set for fall injury prevention trials: The Prevention of Falls Network Europeconsensus. J. Am. Geriatr. Soc. 2005, 53, 1618–1622. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Obesity: Preventing and Management of the Global Epidemic; Report of the WHO Consultation: Technical Report Series. No. 894; World Health Organization: Geneva, Switzerland, 2000. [Google Scholar]
- Presta, E.; Leibel, R.L.; Hirsch, J. Regional changes in adrenergic receptor status during hypocaloric intake do not predict changes in adipocyte size or body shape. Metabolism 1990, 39, 307–315. [Google Scholar] [CrossRef]
- Sánchez-Rodríguez, D.; Marco, E.; Dávalos-Yerovi, V.; López-Escobar, J.; Messaggi-Sartor, M.; Barrera, C.; Ronquillo-Moreno, N.; Vázquez-Ibar, O.; Calle, A.; Inzitari, M.; et al. Translation and Validation of the Spanish Version of the SARC-F Questionnaire to Assess Sarcopenia in Older People. J. Nutr. Health Aging 2019, 23, 518–524. [Google Scholar] [CrossRef]
- Yardley, L.; Beyer, N.; Hauer, K.; Kempen, G.; Piot-Ziegler, C.; Todd, C. Development and initial validation of the Falls Efficacy Scale-International (FES-I). Age Ageing 2005, 34, 614–619. [Google Scholar] [CrossRef] [Green Version]
- Lomas-Vega, R.; Hita-Contreras, F.; Mendoza, N.; Martínez-Amat, A. Cross-cultural adaptation and validation of the Falls Efficacy Scale International in Spanish postmenopausal women. Menopause 2012, 19, 904–908. [Google Scholar] [CrossRef]
- Ersoy, Y.; MacWalter, R.S.; Durmus, B.; Altay, Z.E.; Baysal, O. Predictive effects of different clinical balance measures and the fear of falling on falls in postmenopausal women aged 50 years and over. Gerontology 2009, 55, 660–665. [Google Scholar] [CrossRef]
- Montilla-Ibáñez, A.; Martínez-Amat, A.; Lomas-Vega, R.; Cruz-Díaz, D.; Torre-Cruz, M.J.; Casuso-Pérez, R.; Hita-Contreras, F. The Activities-specific Balance Confidence scale: Reliability and validity in Spanish patients with vestibular disorders. Disabil. Rehabil. 2017, 39, 697–703. [Google Scholar] [CrossRef]
- Lajoie, Y.; Gallagher, S.P. Predicting falls within the elderly community: Comparison of postural sway, reaction time, the Berg balance scale and the Activities-specific Balance Confidence (ABC) scale for comparinfallers and non-fallers. Arch. Gerontol. Geriatr. 2004, 38, 11–26. [Google Scholar] [CrossRef]
- Zigmond, A.S.; Snaith, P.R. The Hospital Anxiety and Depression Scale. Acta Psychiatr. Scand 1983, 67, 361–370. [Google Scholar] [CrossRef] [Green Version]
- Herrero, M.J.; Blanch, J.; Peri, J.M.; De Pablo, J.; Pintor, L.; Bulbena, A. A validation study of the Hospital Anxiety and Depression Scale (HADS) in a Spanish population. Gen. Hosp. Psychiatry 2003, 25, 277–283. [Google Scholar] [CrossRef]
- Krupp, L.B.; LaRocca, N.G.; Muir-Nash, J.; Steinberg, A.D. The fatigue severity scale. Application to patients with multiplsclerosis and systemic lupus erythematosus. Arch. Neurol. 1989, 46, 1121–1123. [Google Scholar] [CrossRef] [PubMed]
- Ortega Calvo, M.; Cayuela Domínguez, A. Unconditioned logistic regression and sample size: A bibliographic review. Rev. Esp. Salud Publica 2002, 76, 85–93. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zweig, M.H.; Campbell, G. Receiver-operating characteristic (ROC) plots: A fundamental evaluation tool in clinical medicine. Clin. Chem. 1993, 39, 561–577. [Google Scholar] [CrossRef]
- Yang, M.; Liu, Y.; Zuo, Y.; Tang, H. Sarcopenia for predicting falls and hospitalization in community-dwelling older adults: EWGSOP versus EWGSOP2. Sci. Rep. 2019, 9, 17636. [Google Scholar] [CrossRef] [PubMed]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Marincolo, J.C.S.; Aprahamian, I.; Corona, L.P.; Neri, A.L.; Yassuda, M.S.; Borim, F.S.A. Three definitions of probable sarcopenia and associations with falls and functional disability among community-dwelling older adults. Osteoporos Sarcopenia 2021, 7, 69–74. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.X.; Yeo, A.; Tan, C.N.; Yew, S.; Tay, L.; Ding, Y.Y.; Lim, W.S. Combined Impact of Positive Screen for Sarcopenia and Frailty on Physical Function, Cognition and Nutrition in the Community Dwelling Older Adult. Ann. Geriatr Med. Res. 2021, 25, 210. [Google Scholar]
- Scheffer, A.C.; Schuurmans, M.J.; van Dijk, N.; van der Hooft, T.; de Rooij, S.E. Fear of Falling: Measurement Strategy, Prevalence, Risk Factors and Consequences Among Older Persons. Age Ageing 2008, 37, 19–24. [Google Scholar] [CrossRef] [Green Version]
- Lavedán, A.; Viladrosa, M.; Jürschik, P.; Botigué, T.; Nuín, C.; Masot, O.; Lavedán, R. Fear of falling in community-dwelling older adults: A cause of falls, a consequence, or both? PLoS ONE 2018, 13, e0194967. [Google Scholar] [CrossRef]
- Oh, J.; Choi, C.K.; Kim, S.A.; Kweon, S.S.; Lee, Y.H.; Nam, H.S.; Park, K.S.; Ryu, S.Y.; Choi, S.W.; Shin, M.H. Association of Falls and Fear of Falling with Mortality in Korean Adults: The Dong-gu Study. Chonnam Med. J. 2019, 55, 104–108. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cao, L.; Chen, S.; Zou, C.; Ding, X.; Gao, L.; Liao, Z.; Liu, G.; Malmstrom, T.K.; Morley, J.E.; Flaherty, J.H.; et al. A pilot study of the SARC-F scale on screening sarcopenia and physical disability in the Chinese older people. J. Nutr. Health Aging 2014, 18, 277–283. [Google Scholar] [CrossRef] [PubMed]
- Gadelha, A.B.; Neri, S.G.R.; Oliveira, R.J.; Bottaro, M.; David, A.C.; Vainshelboim, B.; Lima, R.M. Severity of sarcopenia is associated with postural balance and risk of falls in community-dwelling older women. Exp. Aging Res. 2018, 44, 258–269. [Google Scholar] [CrossRef]
- Bahat Öztürk, G.; Kılıç, C.; Bozkurt, M.E.; Karan, M.A. Prevalence and Associates of Fear of Falling among Community-Dwelling Older Adults. J. Nutr. Health Aging 2021, 25, 433–439. [Google Scholar] [CrossRef] [PubMed]
- Kirk, B.; Zanker, J.; Bani Hassan, E.; Bird, S.; Brennan-Olsen, S.; Duque, G. Sarcopenia Definitions and Outcomes Consortium (SDOC) Criteria are Strongly Associated With Malnutrition, Depression, Falls, and Fractures in High-Risk Older Persons. J. Am. Med. Dir. Assoc. 2021, 22, 741–745. [Google Scholar] [CrossRef]
- Aibar-Almazán, A.; Martínez-Amat, A.; Cruz-Díaz, D.; Jiménez-García, J.D.; Achalandabaso, A.; Sánchez-Montesinos, I.; de la Torre-Cruz, M.; Hita-Contreras, F. Sarcopenia and sarcopenic obesity in Spanish community-dwelling middle-aged and older women: Association with balance confidence, fear of falling and fall risk. Maturitas 2018, 107, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Park, J.I.; Yang, J.C.; Chung, S. Risk Factors Associated with the Fear of Falling in Community-Living Elderly People in Korea: Role of Psychological Factors. Psychiatry Investig. 2017, 14, 894–899. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dierking, L.; Markides, K.; Al Snih, S.; Kristen Peek, M. Fear of Falling in Older Mexican Americans: A Longitudinal Study of Incidence and Predictive Factors. J. Am. Geriatr. Soc. 2016, 64, 2560–2565. [Google Scholar] [CrossRef] [Green Version]
- Payette, M.C.; Bélanger, C.; Léveillé, V.; Grenier, S. Fall-Related Psychological Concerns and Anxiety among Community-Dwelling Older Adults: Systematic Review and Meta-Analysis. PLoS ONE 2016, 11, e0152848. [Google Scholar] [CrossRef] [Green Version]
- Rivasi, G.; Kenny, R.A.; Ungar, A.; Romero-Ortuno, R. Predictors of Incident Fear of Falling in Community-Dwelling Older Adults. J. Am. Med. Dir. Assoc. 2020, 21, 615–620. [Google Scholar] [CrossRef]
- Tyagi, S.; Perera, S.; Brach, J.S. Balance and Mobility in Community-Dwelling Older Adults: Effect of Daytime Sleepiness. J. Am. Geriatr. Soc. 2017, 65, 1019–1025. [Google Scholar] [CrossRef] [PubMed]
- Fábrega-Cuadros, R.; Aibar-Almazán, A.; Martínez-Amat, A.; Hita-Contreras, F. Impact of Psychological Distress and Sleep Quality on Balance Confidence, Muscle Strength, and Functional Balance in Community-Dwelling Middle-Aged and Older People. J. Clin. Med. 2020, 22, 3059. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Study Sample = 157 | |||
|---|---|---|---|
| Mean | SD | ||
| Age (Years) | 70.80 | 8.37 | |
| Years in menopause | 21.41 | 8.91 | |
| BMI | 29.28 | 4.33 | |
| WHR | 0.86 | 0.09 | |
| SARC-F | 1.98 | 1.53 | |
| HADS- anxiety | 6.05 | 4.11 | |
| HADS-depression | 4.90 | 3.50 | |
| Sleep duration (hours) | 6.57 | 1.45 | |
| Self-perceived fatigue | 22.19 | 15.28 | |
| FES-I | 23.54 | 7.34 | |
| ABC-16 | 76.28 | 17.71 | |
| Frequency | Percentage | ||
| Occupational status | Retired | 98 | 62.42 |
| Working | 30 | 19.11 | |
| Unemployed | 29 | 18.47 | |
| Marital status | Single | 6 | 3.82 |
| Married/cohabiting | 76 | 48.41 | |
| Separated/divorced/ Widowed | 75 | 47.77 | |
| Educational level | No formal education | 27 | 17.20 |
| Primary | 75 | 47.77 | |
| Secondary | 41 | 26.11 | |
| University | 14 | 8.92 | |
| History of falls | No | 101 | 64.33 |
| Yes | 56 | 35.67 | |
| Osteoporosis | No | 98 | 62.42 |
| Yes | 59 | 37.58 | |
| Risk of Falling (FES-I) | ||||||
|---|---|---|---|---|---|---|
| No (n = 115) | Yes (n = 42) | |||||
| Mean | SD | Mean | SD | p-Value | ||
| SARC-F | 1.58 | 1.30 | 3.07 | 1.58 | <0.001 | |
| Age | 69.39 | 7.71 | 74.64 | 8.96 | <0.001 | |
| BMI | 29.09 | 4.01 | 29.83 | 5.10 | 0.342 | |
| WHR | 0.85 | 0.10 | 0.87 | 0.06 | 0.262 | |
| Self-perceived fatigue | 19.66 | 14.94 | 29.12 | 14.17 | <0.001 | |
| Anxiety | 5.30 | 4.08 | 8.10 | 3.48 | <0.001 | |
| Depression | 4.23 | 3.25 | 6.74 | 3.54 | <0.001 | |
| Sleep Duration | 6.70 | 1.44 | 6.19 | 1.45 | 0.050 | |
| Frequency | Percentage | Frequency | Percentage | |||
| History of falls | No (n = 101) | 79 | 68.70% | 22 | 520.38% | 0.059 |
| Yes (n = 56) | 36 | 31.30% | 20 | 470.62% | ||
| Osteoporosis | No (n = 98) | 78 | 67.8% | 20 | 470.6% | 0.021 |
| Yes (n = 59) | 37 | 32.2% | 22 | 520.4% | ||
| Risk of Falling (ABC-16) | ||||||
|---|---|---|---|---|---|---|
| No (n = 115) | Yes (n = 42) | |||||
| Mean | SD | Mean | SD | p-Value | ||
| SARC-F | 1.69 | 1.35 | 2.97 | 1.68 | <0.001 | |
| Age | 70.31 | 8.14 | 72.44 | 9.01 | 0.179 | |
| BMI | 29.09 | 4.01 | 29.94 | 5.28 | 0.302 | |
| WHR | 0.86 | 0.10 | 0.87 | 0.07 | 0.445 | |
| Self-perceived fatigue | 19.23 | 13.82 | 32.14 | 15.93 | <0.001 | |
| Anxiety | 5.64 | 4.11 | 7.42 | 3.82 | 0.023 | |
| Depression | 4.58 | 3.32 | 6.00 | 3.89 | 0.032 | |
| Sleep Duration | 6.71 | 1.40 | 6.07 | 1.53 | 0.019 | |
| Frequency | Percentage | Frequency | Percentage | |||
| History of falls | No (n = 101) | 83 | 68.60 | 18 | 50.00 | 0.041 |
| Yes (n = 56) | 38 | 31.40 | 18 | 50.00 | ||
| Osteoporosis | No (n = 98) | 78 | 64.46 | 20 | 55.56 | 0.333 |
| Yes (n = 59) | 43 | 35.54 | 16 | 44.44 | ||
| Exp (B) | 95 CI | p-Value | |||
|---|---|---|---|---|---|
| Inferior | Superior | ||||
| FES-I | SARC-F | 1.656 | 1.212 | 2.263 | 0.002 |
| Anxiety | 1.147 | 1.031 | 1.276 | 0.012 | |
| Age | 1.060 | 1.005 | 1.118 | 0.031 | |
| ABC-16 | SARC-F | 1.612 | 1.201 | 2.165 | 0.001 |
| Self-perceived fatigue | 1.044 | 1.017 | 1.072 | 0.001 | |
| Sleep duration | 0.745 | 0.553 | 1.004 | 0.053 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alzar-Teruel, M.; Hita-Contreras, F.; Martínez-Amat, A.; Lavilla-Lerma, M.L.; Fábrega-Cuadros, R.; Jiménez-García, J.D.; Aibar-Almazán, A. SARC-F and the Risk of Falling in Middle-Aged and Older Community-Dwelling Postmenopausal Women. Int. J. Environ. Res. Public Health 2021, 18, 11570. https://doi.org/10.3390/ijerph182111570
Alzar-Teruel M, Hita-Contreras F, Martínez-Amat A, Lavilla-Lerma ML, Fábrega-Cuadros R, Jiménez-García JD, Aibar-Almazán A. SARC-F and the Risk of Falling in Middle-Aged and Older Community-Dwelling Postmenopausal Women. International Journal of Environmental Research and Public Health. 2021; 18(21):11570. https://doi.org/10.3390/ijerph182111570
Chicago/Turabian StyleAlzar-Teruel, María, Fidel Hita-Contreras, Antonio Martínez-Amat, María Leyre Lavilla-Lerma, Raquel Fábrega-Cuadros, José Daniel Jiménez-García, and Agustín Aibar-Almazán. 2021. "SARC-F and the Risk of Falling in Middle-Aged and Older Community-Dwelling Postmenopausal Women" International Journal of Environmental Research and Public Health 18, no. 21: 11570. https://doi.org/10.3390/ijerph182111570
APA StyleAlzar-Teruel, M., Hita-Contreras, F., Martínez-Amat, A., Lavilla-Lerma, M. L., Fábrega-Cuadros, R., Jiménez-García, J. D., & Aibar-Almazán, A. (2021). SARC-F and the Risk of Falling in Middle-Aged and Older Community-Dwelling Postmenopausal Women. International Journal of Environmental Research and Public Health, 18(21), 11570. https://doi.org/10.3390/ijerph182111570