
Let’s Walk It: Mobility and the Perceived Quality of Life in Older Adults


Abstract
:1. Introduction
2. Materials and Methods
2.1. The Questionnaire
- -
- Living conditions and socioeconomic environment, social integration and state of health (incl. experiences of falling and hospitalization), perception of living and built environment, mobility, and QOL.
- -
- Assessment of and experiences with technical aids and the willingness to undertake concrete changes in their life or living environment.
- -
- Assessment of how their ageing is perceived (continuum/breaks) in terms of self-image and compared with others. Survey of wishes and ideas concerning the process of getting older (including the perceived significance of AAL—active assisted living).
2.2. Procedure and Sampling
2.3. Conceptual Thoughts
2.4. Mobility
2.5. Quality of Life
2.6. Multivariate Statistics
3. Results
3.1. Descriptive Statistics
3.1.1. The Sample Composition—Description of Main Variables
3.1.2. Social Aspects
3.1.3. Mobility
3.1.4. Quality of Life
3.1.5. Self-Perception
3.2. Inference Statistics
3.2.1. Association of Main Variables
3.2.2. Quality of Life
3.2.3. Mobility
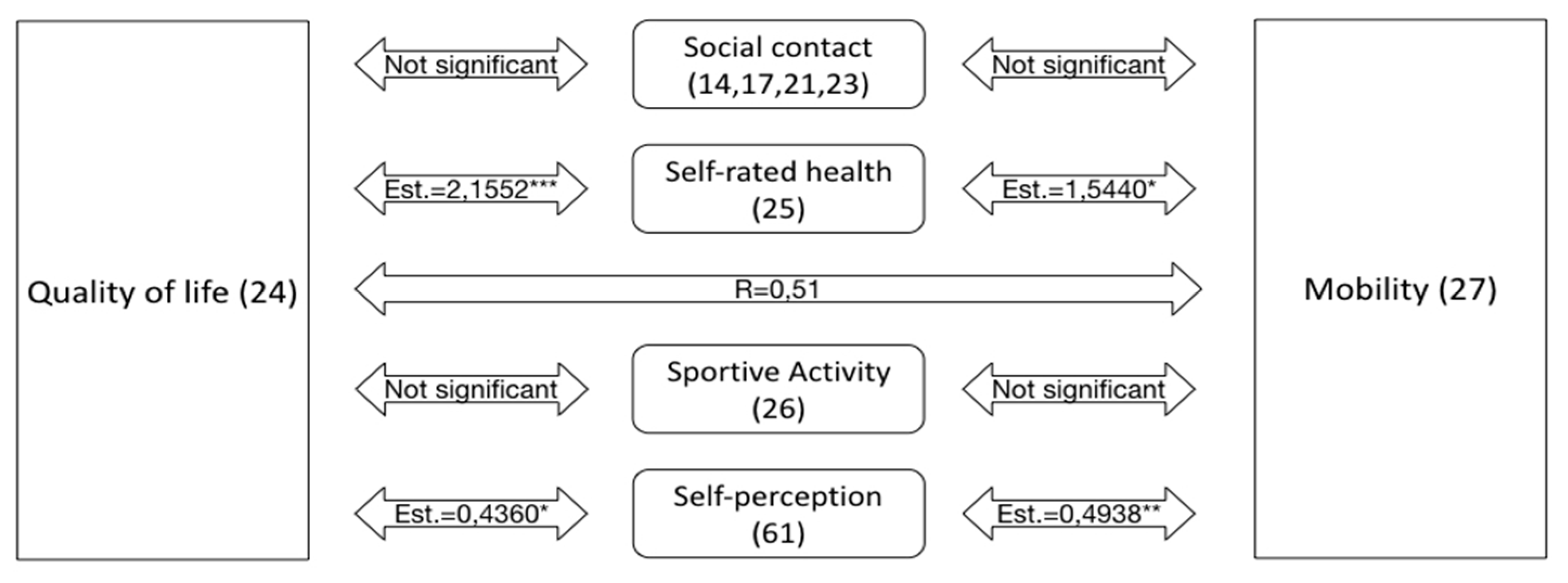
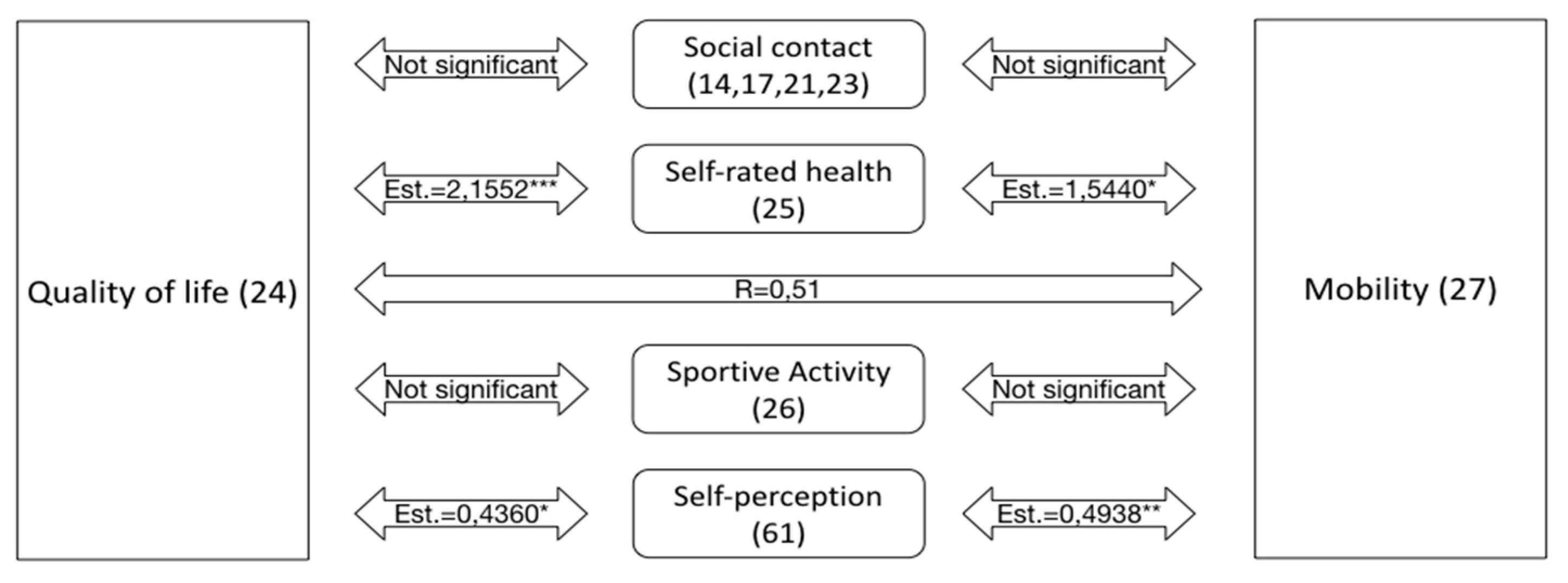
3.2.4. Association of Self-Rated Health, Self-Perception with Certain Conditions
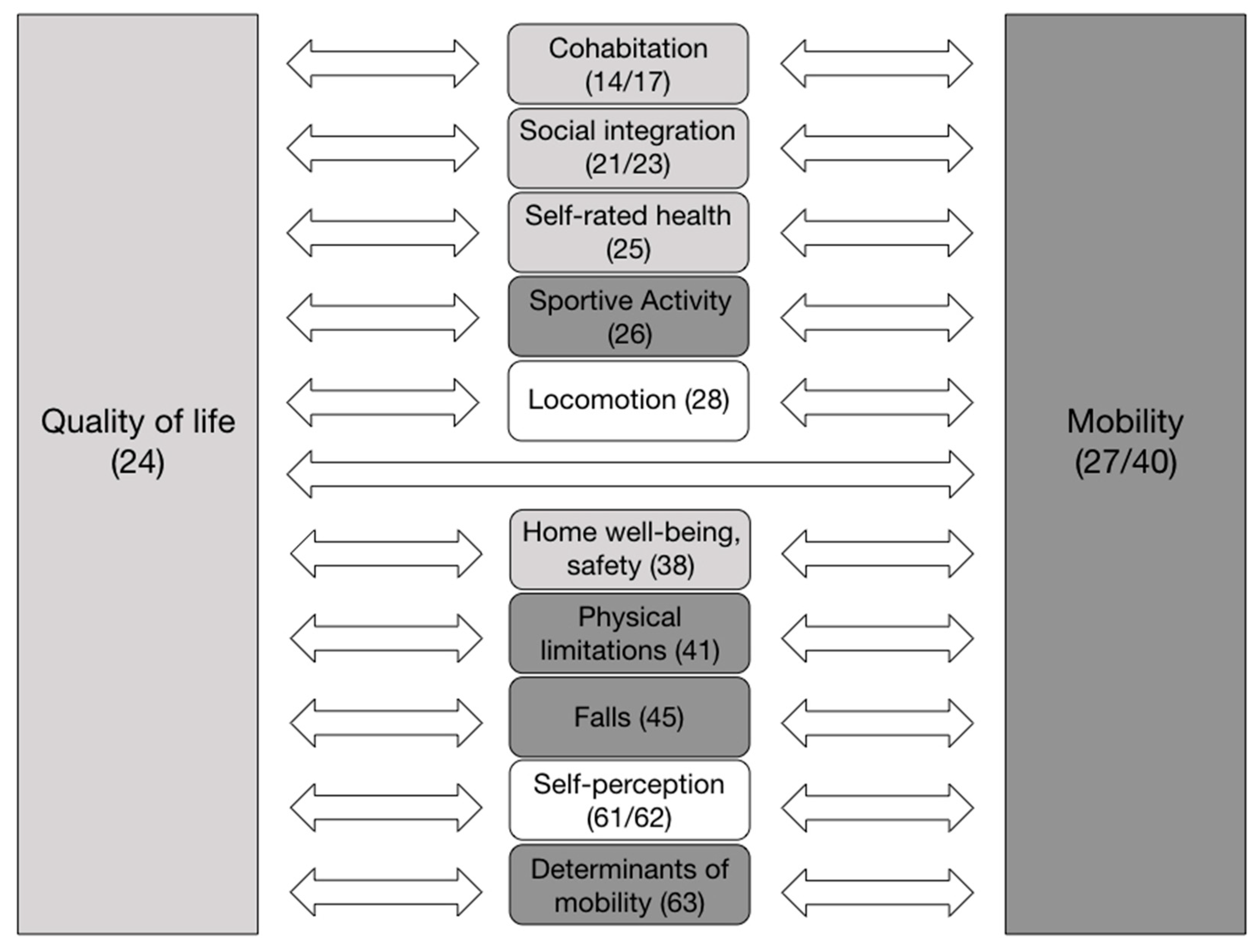
3.2.5. Correlation of Conditions—“Related Conditions”
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Olsberg, D.; Winters, M. Ageing in Place: Intergenerational and Intrafamilial Housing Transfers and Shifts in Later Life; Australian Housing and Urban Research Institute: Melbourne, VIC, Australia, 2013. [Google Scholar]
- Means, R. Safe as houses? Ageing in place and vulnerable older people in the UK. Soc. Policy Adm. 2007, 41, 65–85. [Google Scholar] [CrossRef]
- World Health Organization. 2016 World Report on Ageing and Health; World Health Organization: Geneva, Switzerland, 2016; Available online: https://apps.who.int/iris/handle/10665/186463 (accessed on 18 October 2021).
- Buffel, T.; Handler, S.; Phillipson, C. Age-Friendly Cities and Communities; Policy Press: Bristol, UK, 2018. [Google Scholar]
- Shishehgar, M.; Kerr, D.; Blake, J. A systematic review of research into how robotic technology can help older people. Smart Health 2018, 7-8, 1–18. [Google Scholar] [CrossRef]
- Bechtold, U.; Sotoudeh, M. Assistive technologies: Their development from a technology assessment perspective. Gerontechnology 2013, 11, 521–533. [Google Scholar] [CrossRef]
- Neven, L. By any means? Questioning the link between gerontechnological innovation and older people’s wish to live at home. Technol. Forecast. Soc. Change 2015, 93, 32–43. [Google Scholar] [CrossRef]
- Fletcher-Watson, B.; Crompton, C.J.; Hutchison, M.; Lu, H. Strategies for enhancing success in digital tablet use by older adults: A pilot study. Gerontechnology 2016, 15, 162–170. [Google Scholar] [CrossRef] [Green Version]
- Tinker, A. Some ethical issues in research on the housing of older people. Gerontechnology 2016, 15, 192–197. [Google Scholar] [CrossRef]
- Mollenkopf, H. Societal aspects and individual preconditions of technological development. Gerontechnology 2016, 15, 216–226. [Google Scholar] [CrossRef]
- Bechtold, U. DiaLogbuch AAL Dialoge zu Active and Assisted Living; Austrian Computer Society: Vienna, Austria, 2016; ISBN 9783902580122. [Google Scholar]
- Ottoni, C.A.; Sims-Gould, J.; Winters, M.; Heijnen, M.; McKay, H.A. ‘Benches become like porches’: Built and social environment influences on older adults’ experiences of mobility and well-being. Soc. Sci. Med. 2016, 169, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Van Hees, S.; Horstman, K.; Jansen, M.; Ruwaard, D. Photovoicing the neighbourhood: Understanding the situated meaning of intangible places for ageing-in-place. Health Place 2017, 48, 11–19. [Google Scholar] [CrossRef]
- Webber, S.C.; Porter, M.M.; Menec, V.H. Mobility in older adults: A comprehensive framework. Gerontologist 2010, 50, 443–450. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van der Vorst, A.; Zijlstra, G.A.R.; Witte, N.D.; Duppen, D.; Stuck, A.E.; Kempen, G.I.J.M.; Schols, J.M.G.A. Limitations in activities of daily living in community-dwelling people aged 75 and over: A systematic literature review of risk and protective factors, edited by Ginsberg, S.D. PLoS ONE 2016, 11, e0165127. [Google Scholar] [CrossRef] [Green Version]
- Zeitler, E.; Buys, L.; Aird, R.; Miller, E. Mobility and active ageing in suburban environments: Findings from in-depth interviews and person-based G.P.S. tracking. Curr. Gerontol. Geriatr. Res. 2012, 2012, 1–10. [Google Scholar] [CrossRef] [Green Version]
- McLean, A. Ethical frontiers of ICT and older users: Cultural, pragmatic and ethical issues. Ethics Inf. Technol. 2011, 13, 313–326. [Google Scholar] [CrossRef]
- Oxley, J.; Whelan, M. It cannot be all about safety: The benefits of prolonged mobility. Traffic Inj. Prev. 2008, 9, 367–378. [Google Scholar] [CrossRef]
- Ravulaparthy, S.; Yoon, S.Y.; Goulias, K.G. Linking elderly transport mobility and subjective well-being: A Multivariate latent modeling approach, transportation research record. J. Transp. Res. Board 2013, 2382, 28–36. [Google Scholar] [CrossRef] [Green Version]
- Van Hoven, B.; Meijering, L. Mundane mobilities in later life—Exploring experiences of everyday trip-making by older adults in a Dutch urban neighbourhood. Res. Transp. Bus. Manag. 2019, 30, 100375. [Google Scholar] [CrossRef]
- Baydan, M.; Caliskan, H.; Balam-Yavuz, B.; Aksoy, S.; Böke, B. The Interaction between mild cognitive impairment with vestibulo-ocular reflex, dynamic visual acuity and postural balance in older adults. Exp. Gerontol. 2020, 130, 110785. [Google Scholar] [CrossRef] [PubMed]
- Da Silva Costa, A.A.; Moraes, R.; Hortobágyi, T.; Sawers, A. Older adults reduce the complexity and efficiency of neuromuscular control to preserve walking balance. Exp. Gerontol. 2020, 140, 111050. [Google Scholar] [CrossRef] [PubMed]
- Kahiel, Z.; Grant, A.; Aubin, M.-J.; Buhrmann, R.; Kergoat, M.-J.; Freeman, E.E. Vision, eye disease, and the onset of balance problems: The Canadian longitudinal study on aging. Am. J. Ophthalmol. 2021, 231, 170–178. [Google Scholar] [CrossRef] [PubMed]
- Camporeale, R.; Wretstrand, A.; Andersson, M. How the built environment and the railway network can affect the mobility of older people: Analyses of the southern Swedish region of Scania. Res. Transp. Bus. Manag. 2019, 30, 100368. [Google Scholar] [CrossRef]
- Musselwhite, C. Prioritising transport barriers and enablers to mobility in later life: A case study from Greater Manchester in the United Kingdom. J. Transp. Health 2021, 22, 101085. [Google Scholar] [CrossRef]
- Mollenkopf, H.; Marcellini, F.; Ruoppila, I.; Széman, Z.; Tacken, M.; Wahl, H.-W. Social and behavioural science perspectives on out-of-home mobility in later life: Findings from the European project MOBILATE. Eur. J. Ageing 2004, 1, 45–53. [Google Scholar] [CrossRef] [Green Version]
- Musselwhite, C.; Haddad, H. Mobility, accessibility and quality of later life. Qual. Ageing Older Adults 2010, 11, 25–37. [Google Scholar] [CrossRef] [Green Version]
- Amann, A.; Bischof, C.; Salmhofer, A. Intergenerationelle Lebensqualität: Diversität zwischen Stadt und Land; Verlag des ÖGB GmbH: Vienna, Austria, 2016. [Google Scholar]
- Wang, C.; Pu, R.; Ghose, B.; Tang, S. Chronic musculoskeletal pain, self-reported health and quality of life among older populations in South Africa and Uganda. Int. J. Environ. Res. Public Health 2018, 15, 2806. [Google Scholar] [CrossRef] [Green Version]
- Rowles, G.; Watkins, J. History, habit, heart, and hearth: On making spaces into places. In Aging Independently. Living Arrangements and Mobility; Springer: New York, NY, USA, 2003. [Google Scholar]
- Ruppe, G.; Stückler, A.; Klambauer, E.; Schmidt, A.; Wosko, P.; Pleschberger, S. Austrian Interdisciplinary Study on the Oldest Old. 2013. Available online: http://www.oepia.at/hochaltrigkeit/wp-content/uploads/2015/05/OEIHS_Endbericht_Endfassung1.pdf (accessed on 19 August 2021).
- Campbell, E.; Petermann-Rocha, F.; Welsh, P.; Celis-Morales, C.; Pell, J.P.; Ho, F.K.; Gray, S.R. The effect of exercise on quality of life and activities of daily life in frail older adults: A systematic review of randomised control trials. Exp. Gerontol. 2021, 147, 111287. [Google Scholar] [CrossRef] [PubMed]
- Mendoza-Núñez, V.; Sarmiento-Salmorán, E.; Marín-Cortés, R.; Martínez-Maldonado, M.; Ruiz-Ramos, M. Influence of the self-perception of old age on the effect of a healthy aging program. J. Clin. Med. 2018, 7, 106. [Google Scholar] [CrossRef] [Green Version]
- Wahl, A.K.; Rustøen, T.; Hanestad, B.R.; Lerdal, A.; Moum, T. Quality of life in the general Norwegian Population, measured by the quality of life scale (QOLS-N). Qual. Life Res. 2004, 13, 1001–1009. [Google Scholar] [CrossRef] [PubMed]
- Ward, M.; McGarrigle, C.A.; Kenny, R.A. More than health: Quality of life trajectories among older adults—Findings from The Irish Longitudinal Study of Ageing (TILDA). Qual. Life Res. 2019, 28, 429–439. [Google Scholar] [CrossRef] [PubMed]
- Davis, J.C.; Bryan, S.; McLeod, R.; Rogers, J.; Khan, K.; Liu-Ambrose, T. Exploration of the association between quality of life, assessed by the EQ-5D and ICECAP-O, and falls risk, cognitive function and daily function, in older adults with mobility impairments. BMC Geriatr. 2012, 12, 65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mifsud, D.; Attard, M.; Ison, S. An exploratory study of the psychological determinants of mobility of older people in Malta. Res. Transp. Bus. Manag. 2019, 30, 100373. [Google Scholar]
- Levy, B.R.; Myers, L.M. Preventive health behaviors influenced by self-perceptions of aging. Prev. Med. 2004, 39, 625–629. [Google Scholar] [CrossRef] [PubMed]
- Brown, C.J.; Flood, K.L. Mobility limitation in the older patient: A clinical review. JAMA 2013, 310, 1168. [Google Scholar] [CrossRef] [PubMed]
- Kenny, R.A.; Coen, R.F.; Frewen, J.; Donoghue, O.A.; Cronin, H.; Savva, G.M. Normative values of cognitive and physical function in older adults: Findings from the Irish longitudinal study on ageing. J. Am. Geriatr. Soc. 2013, 61, S279–S290. [Google Scholar] [CrossRef]
- Musich, S.; Wang, S.S.; Ruiz, J.; Hawkins, K.; Wicker, E. The impact of mobility limitations on health outcomes among older adults. Geriatr. Nurs. 2018, 39, 162–169. [Google Scholar] [CrossRef]
- Lahmann, C.; Henningsen, P.; Brandt, T.; Strupp, M.; Jahn, K.; Dieterich, M.; Eckhardt-Henn, A.; Feuerecker, R.; Dinkel, A.; Schmid, G. Psychiatric comorbidity and psychosocial impairment among patients with vertigo and dizziness. J. Neurol. Neurosurg. Psychiatry 2015, 86, 302–308. [Google Scholar] [CrossRef] [Green Version]
- Bigelow, R.T.; Semenov, Y.R.; du Lac, S.; Hoffman, H.J.; Agrawal, Y. Vestibular vertigo and comorbid cognitive and psychiatric impairment: The 2008 National Health Interview Survey. J. Neurol. Neurosurg. Psychiatry 2016, 87, 367–372. [Google Scholar] [CrossRef]
- Ambrose, A.F.; Paul, G.; Hausdorff, J.M. Risk factors for falls among older adults: A review of the literature. Maturitas 2013, 75, 51–61. [Google Scholar] [CrossRef]
- Heiland, E.G.; Welmer, A.-K.; Wang, R.; Santoni, G.; Angleman, S.; Fratiglioni, L.; Qiu, C. Association of mobility limitations with incident disability among older adults: A population-based study. Age Ageing 2016, 45, 812–819. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jalali, M.M.; Gerami, H.; Heidarzadeh, A.; Soleimani, R. Balance performance in older adults and its relationship with falling. Aging Clin. Exp. Res. 2015, 27, 287–296. [Google Scholar] [CrossRef]
- Muir, S.W.; Berg, K.; Chesworth, B.; Klar, N.; Speechley, M. Balance impairment as a risk factor for falls in community-dwelling older adults who are high functioning: A prospective study. Phys. Ther. 2010, 90, 338–347. [Google Scholar] [CrossRef] [Green Version]
- Rivasi, G.; Kenny, R.A.; Ungar, A.; Romero-Ortuno, R. Predictors of incident fear of falling in community-dwelling older adults. J. Am. Med. Dir. Assoc. 2020, 21, 615–620. [Google Scholar] [CrossRef] [PubMed]
- Pothier, K.; Vrinceanu, T.; Intzandt, B.; Bosquet, L.; Karelis, A.D.; Lussier, M.; Vu, T.T.M.; Nigam, A.; Li, K.Z.H.; Berryman, N.; et al. A comparison of physical exercise and cognitive training interventions to improve determinants of functional mobility in healthy older adults. Exp. Gerontol. 2021, 149, 111331. [Google Scholar] [CrossRef] [PubMed]
- Gómez-Bruton, A.; López-Torres, O.; Gómez-Cabello, A.; Rodríguez-Gomez, I.; Pérez-Gómez, J.; Pedrero-Chamizo, R.; Gusi, N.; Ara, I.; Jasaus, J.A.; Gonzalez-Gross, M.; et al. How important is current physical fitness for future quality of life? Results from an 8-year longitudinal study on older adults. Exp. Gerontol. 2021, 149, 111301. [Google Scholar] [CrossRef]
- Langlois, F.; Vu, T.T.M.; Chasse, K.; Dupuis, G.; Kergoat, M.-J.; Bherer, L. Benefits of physical exercise training on cognition and quality of life in frail older adults. J. Gerontol. Ser. B 2013, 68, 400–404. [Google Scholar] [CrossRef] [PubMed]
- Lindsley, O.R. Geriatric behavioral prosthetics. In New Thoughts on Old Age; Kastenbaum, R., Ed.; Springer: Berlin/Heidelberg, Germany, 1964; pp. 41–60. [Google Scholar]
- Peine, A. Socio-Gerontechnology: Interdisciplinary Critical Studies of Ageing and Technology, 1st ed.; Routledge: New York, NY, USA, 2021. [Google Scholar]
- Wanka, A.; Gallistl, V. Age, Actors and Agency—What We Can Learn from Age Studies and STS for the Development of Socio-gerontechnology, Socio-Gerontechnology: Interdisciplinary Critical Studies of Ageing and Technology, 1st ed.; Routledge: New York, NY, USA, 2021. [Google Scholar]
- Neven, L.; Peine, A. From triple win to triple sin: How a Problematic future discourse is shaping the way people age with technology. Societies 2017, 7, 26. [Google Scholar] [CrossRef]
- Bechtold, U.; Capari, L.; Gudowsky, N. Futures of ageing and technology—Comparing different actors’ prospective views. J. Responsible Innov. 2017, 4, 157–176. [Google Scholar] [CrossRef]
- Kahiel, Z.; Aubin, M.-J.; Buhrmann, R.; Kergoat, M.-J.; Freeman, E.E. Incidence of visual impairment in Canada: The Canadian longitudinal study on aging. Can. J. Ophthalmol. 2021, 56, S0008418221000363. [Google Scholar] [CrossRef]
- Maniscalco, L.; Miceli, S.; Bono, F.; Matranga, D. Self-perceived health, objective health, and quality of life among people aged 50 and over: Interrelationship among health indicators in Italy, Spain, and Greece. Int. J. Environ. Res. Public Health 2020, 17, 2414. [Google Scholar] [CrossRef] [Green Version]
- McCreadie, C.; Tinker, A. The acceptability of assistive technology to older people. Ageing Soc. 2005, 25, 91–110. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Estimate | Std. Error | z Values | OR | p | ||
|---|---|---|---|---|---|---|
| (Intercept) | −1.8239 | 2.7647 | −0.6600 | 0.5094 | ||
| Sex female (ref. male) | 0.3235 | 0.5660 | 0.5720 | 1.3819 | 0.5676 | |
| Age | −0.0089 | 0.0354 | −0.2520 | 0.9911 | 0.8009 | |
| Education | 0.5522 | 0.2334 | 2.3660 | 1.7371 | 0.0180 | * |
| Self-rated health intermediate (ref. unsatisfactory) | 1.4695 | 0.6846 | 2.1460 | 4.3471 | 0.0318 | * |
| Self-rated health satisfactory (ref. unsatisfactory) | 2.1552 | 0.6135 | 3.5130 | 8.6296 | 0.0004 | *** |
| Self-perception compared to others | 0.4360 | 0.1817 | 2.4000 | 1.5466 | 0.0164 | * |
| Estimate | Std. Error | z Values | OR | p | ||
|---|---|---|---|---|---|---|
| (Intercept) | 3.6667 | 2.8055 | 1.3070 | 0.1912 | ||
| Sex female (ref. male) | 0.7082 | 0.5475 | 1.2940 | 2.0304 | 0.1958 | |
| Age | −0.0750 | 0.0367 | −2.0430 | 0.9277 | 0.0410 | * |
| Education | 0.3912 | 0.2255 | 1.7350 | 1.4788 | 0.0827 | |
| Self-rated health intermediate (ref.: unsatisfactory) | 0.7535 | 0.6656 | 1.1320 | 2.1245 | 0.2576 | |
| Self-rated health satisfied (ref.: unsatisfactory) | 1.5440 | 0.6260 | 2.4660 | 4.6835 | 0.0137 | * |
| Self-perception compared to others | 0.4938 | 0.1871 | 2.6390 | 1.6385 | 0.0083 | ** |
| Estimate | Std. Error | z Values | p | ||
|---|---|---|---|---|---|
| Memory problems yes (ref: no) | −0.5606 | 0.3380 | −1.6590 | 0.0972 | |
| Walking problems yes (ref: no) | −3.1927 | 0.4903 | −6.5120 | 0.0000 | *** |
| Debility of eyesight yes (ref: no) | −0.1852 | 0.3321 | −0.5580 | 0.5772 | |
| Hardness of hearing yes (ref: no) | −0.0501 | 0.3449 | −0.1450 | 0.8846 | |
| Vertigo yes (ref: no) | −1.7193 | 0.3625 | −4.7430 | 0.0000 | *** |
| Balance problems yes (ref: no) | −1.4844 | 0.3781 | −3.9260 | 0.0001 | *** |
| Orientation problems yes (ref: no) | −1.0608 | 0.4824 | −2.1990 | 0.0279 | * |
| Estimate | Std. Error | z Values | p | ||
|---|---|---|---|---|---|
| Memory problems yes (ref: no) | −0.3954 | 0.2226 | −1.7770 | 0.0777 | |
| Walking problems yes (ref: no) | −1.1458 | 0.2084 | −5.4970 | 0.0000 | *** |
| Debility of eyesight yes (ref: no) | −0.2900 | 0.2253 | −1.2870 | 0.2001 | |
| Hardness of hearing yes (ref: no) | −0.4058 | 0.2273 | −1.7850 | 0.0764 | |
| Vertigo yes (ref: no) | −0.6778 | 0.2526 | −2.6830 | 0.0082 | ** |
| Balance problems yes (ref: no) | −1.1973 | 0.2605 | −4.5970 | 0.0000 | *** |
| Orientation problems yes (ref: no) | −0.7179 | 0.3530 | −2.0340 | 0.0439 | * |
| Walking Problems Yes (Ref: No) | Vertigo Yes (Ref: No) | Balance Problems Yes (Ref: No) | Orientation Problems Yes (Ref: No) | |
|---|---|---|---|---|
| Walking problems yes (ref: no) | 1 | 0.507 | 0.592 | 0.352 |
| Vertigo yes (ref: no) | 1 | 0.86 | 0.5103 | |
| Balance problems yes (ref: no) | 1 | 0.6285 | ||
| Orientation problems yes (ref: no) | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bechtold, U.; Stauder, N.; Fieder, M. Let’s Walk It: Mobility and the Perceived Quality of Life in Older Adults. Int. J. Environ. Res. Public Health 2021, 18, 11515. https://doi.org/10.3390/ijerph182111515
Bechtold U, Stauder N, Fieder M. Let’s Walk It: Mobility and the Perceived Quality of Life in Older Adults. International Journal of Environmental Research and Public Health. 2021; 18(21):11515. https://doi.org/10.3390/ijerph182111515
Chicago/Turabian StyleBechtold, Ulrike, Natalie Stauder, and Martin Fieder. 2021. "Let’s Walk It: Mobility and the Perceived Quality of Life in Older Adults" International Journal of Environmental Research and Public Health 18, no. 21: 11515. https://doi.org/10.3390/ijerph182111515
APA StyleBechtold, U., Stauder, N., & Fieder, M. (2021). Let’s Walk It: Mobility and the Perceived Quality of Life in Older Adults. International Journal of Environmental Research and Public Health, 18(21), 11515. https://doi.org/10.3390/ijerph182111515