
Early Implementation and Evaluation of StepUp for Dementia Research: An Australia-Wide Dementia Research Participation and Public Engagement Platform

 , , , ,
, , , ,
Abstract
:1. Introduction
2. Materials and Methods
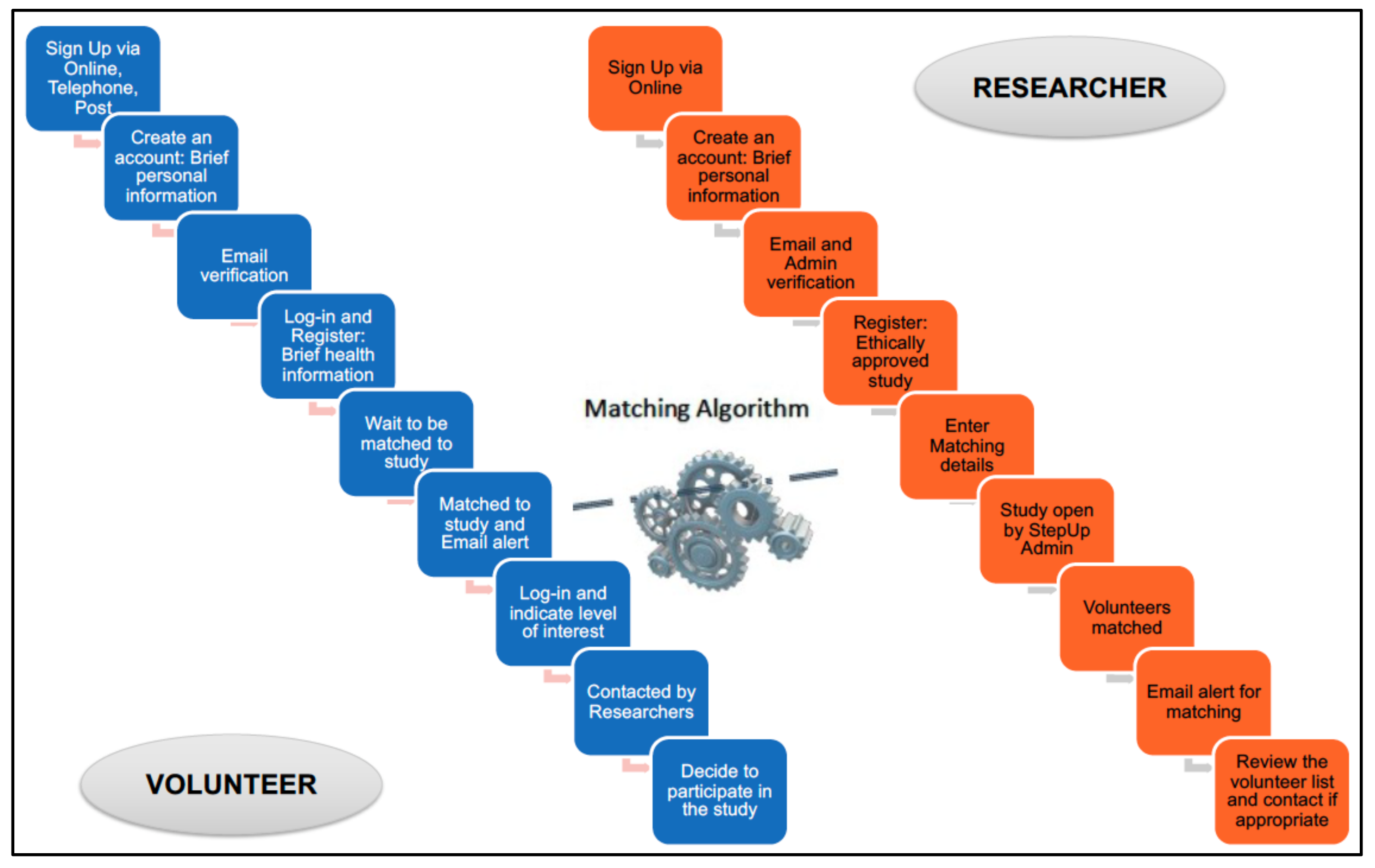
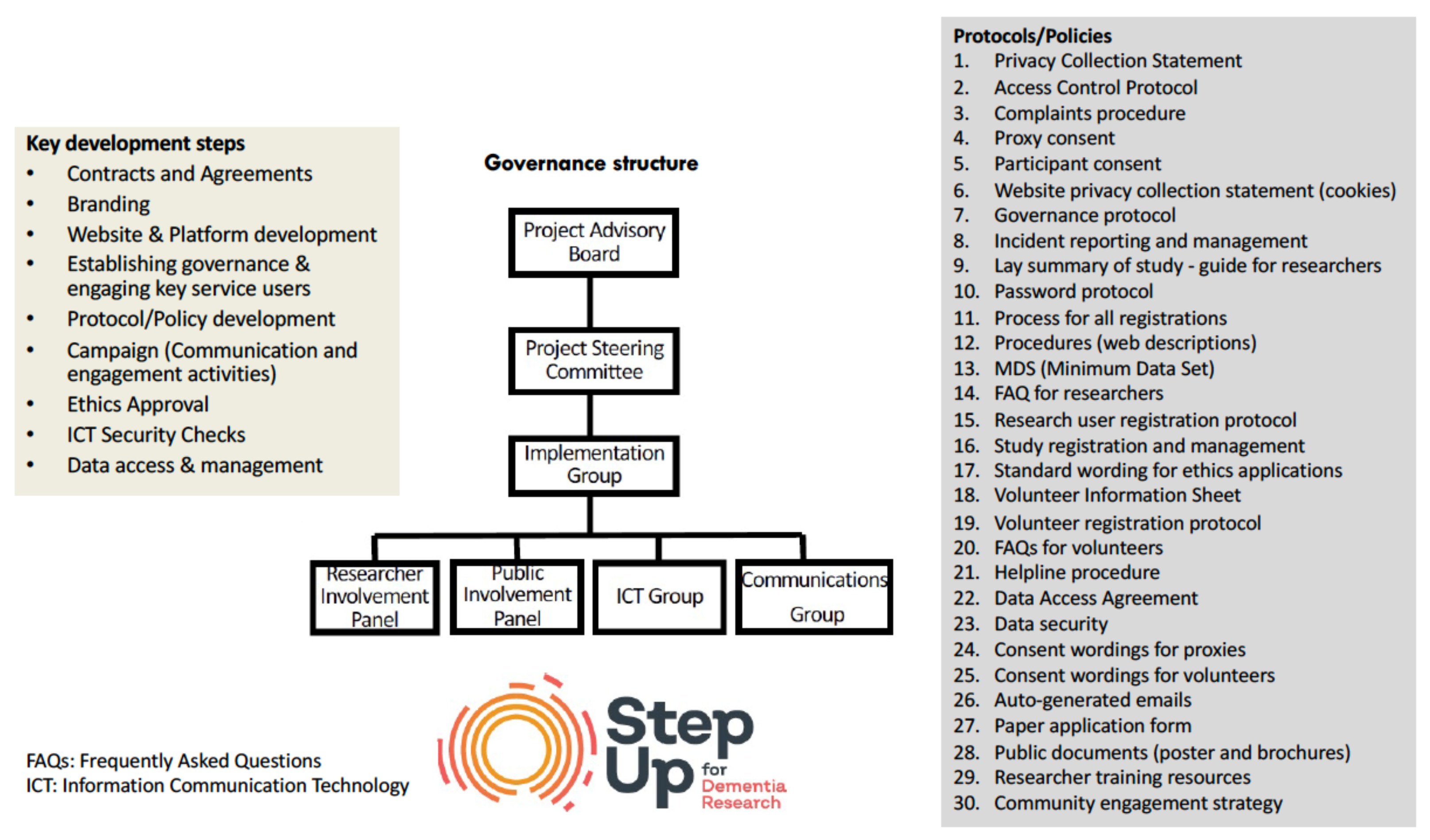
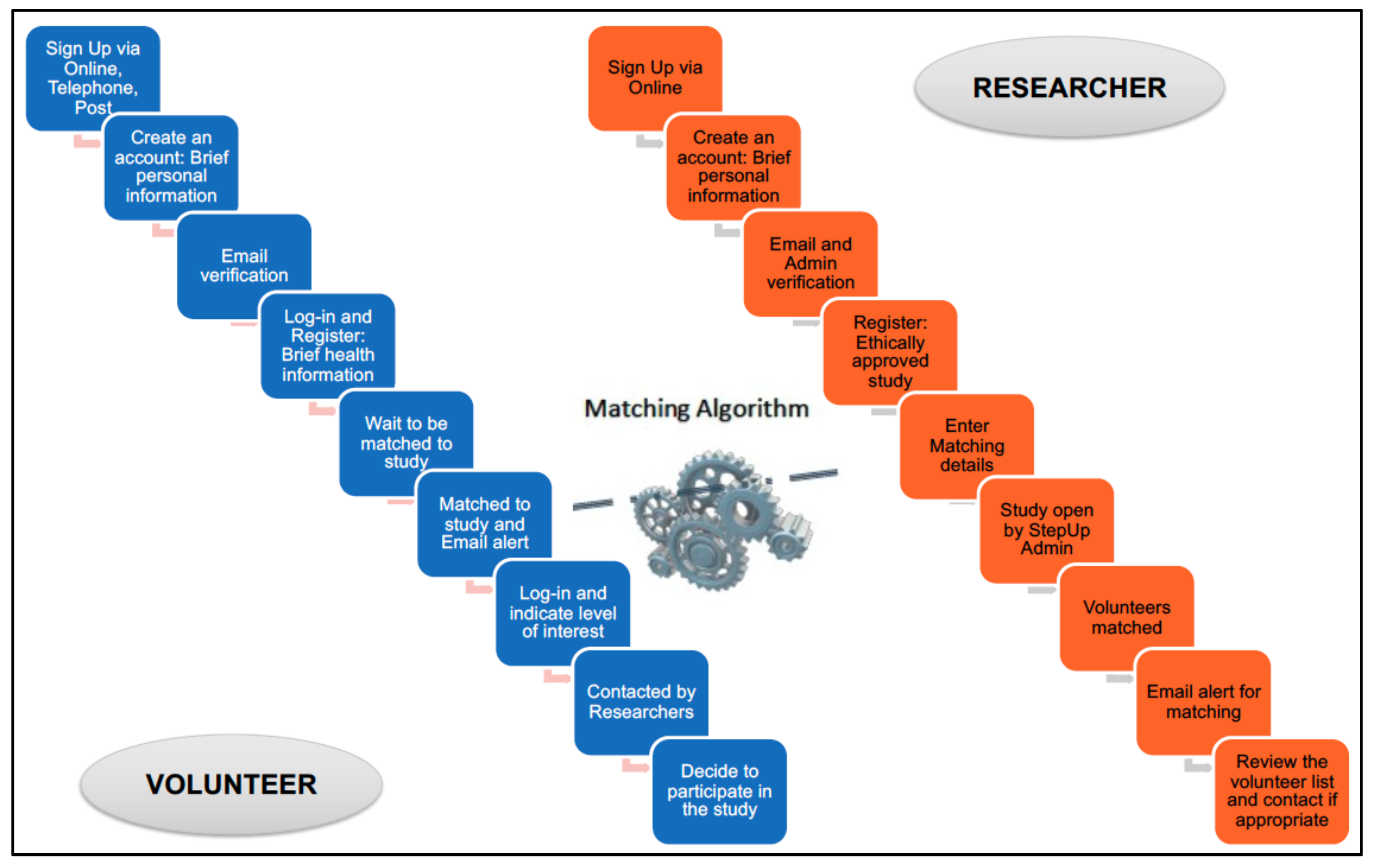
What Is StepUp for Dementia Research and How does it Work?
- (1)
- platform functionality and feasibility (i.e., effective website and registration processes via online, helpdesk and post, and deliverables including ethics approval, data management and cybersecurity);
- (2)
- registration reach (with initial focus on NSW and WA, followed by a national rollout) and the number of volunteers, researchers and studies; and
- (3)
- user experience (i.e., support for volunteers, researcher training and support, and institutional agreements).
3. Results
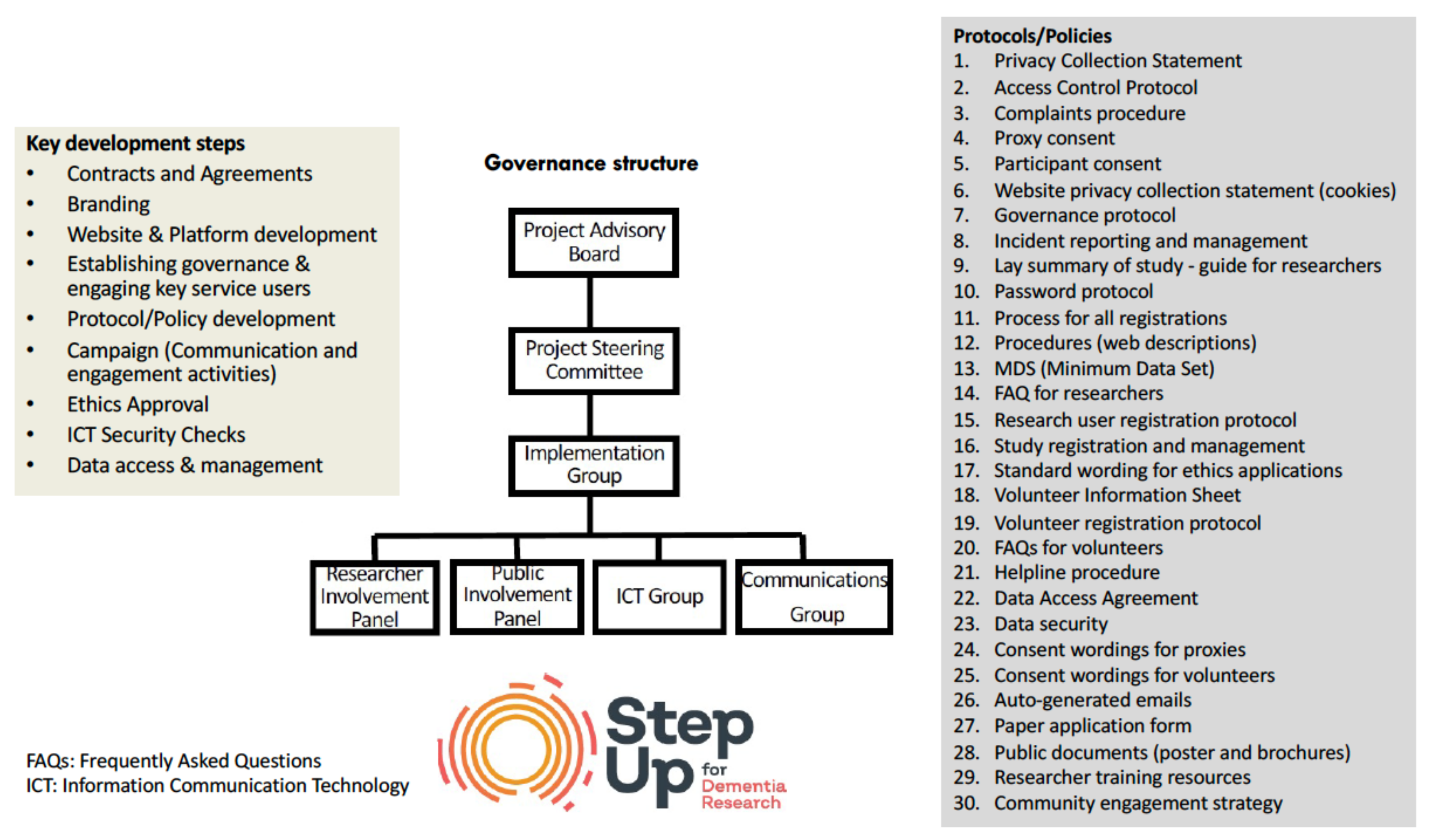
3.1. Platform Functionality and Feasibility
3.2. Reach and Characteristics of Volunteers and Researchers Registered in StepUp
3.3. Key Milestones for Volunteers and Registered Studies in StepUp for Dementia Research
3.4. The Experience of Volunteers and Researchers Registered in StepUp for Dementia Research
3.4.1. Characteristics of Volunteers who Responded to the Surveys
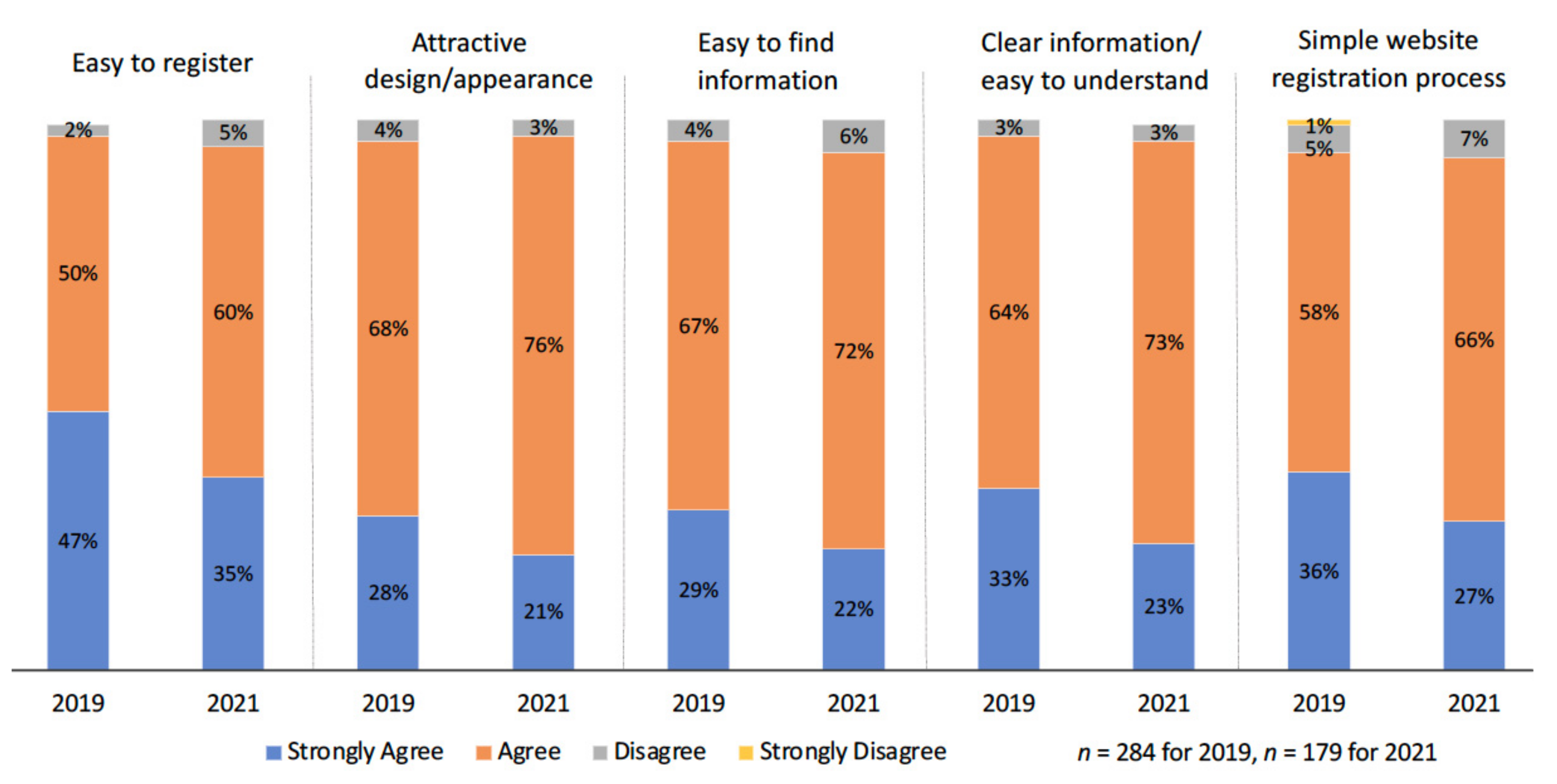
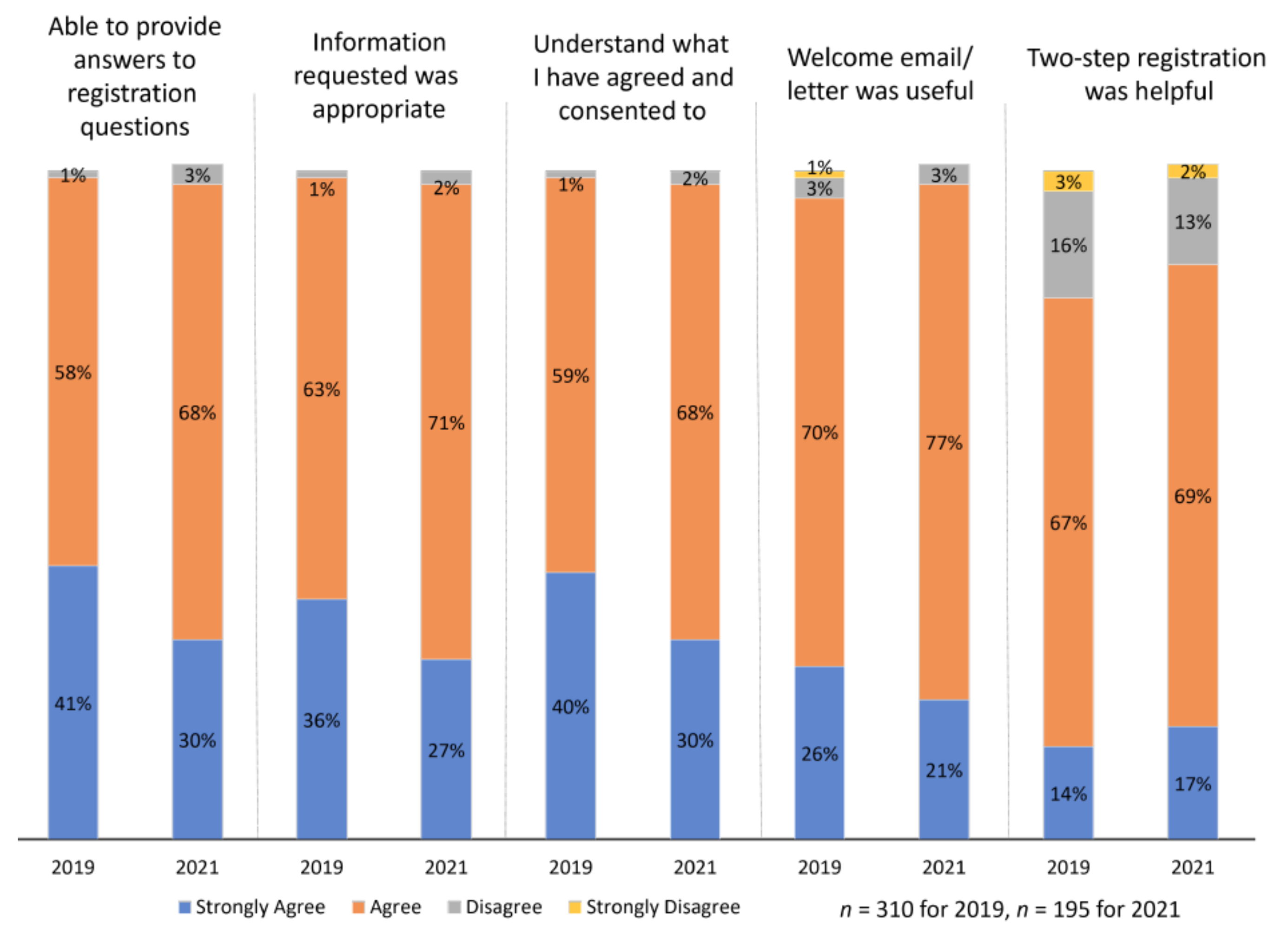
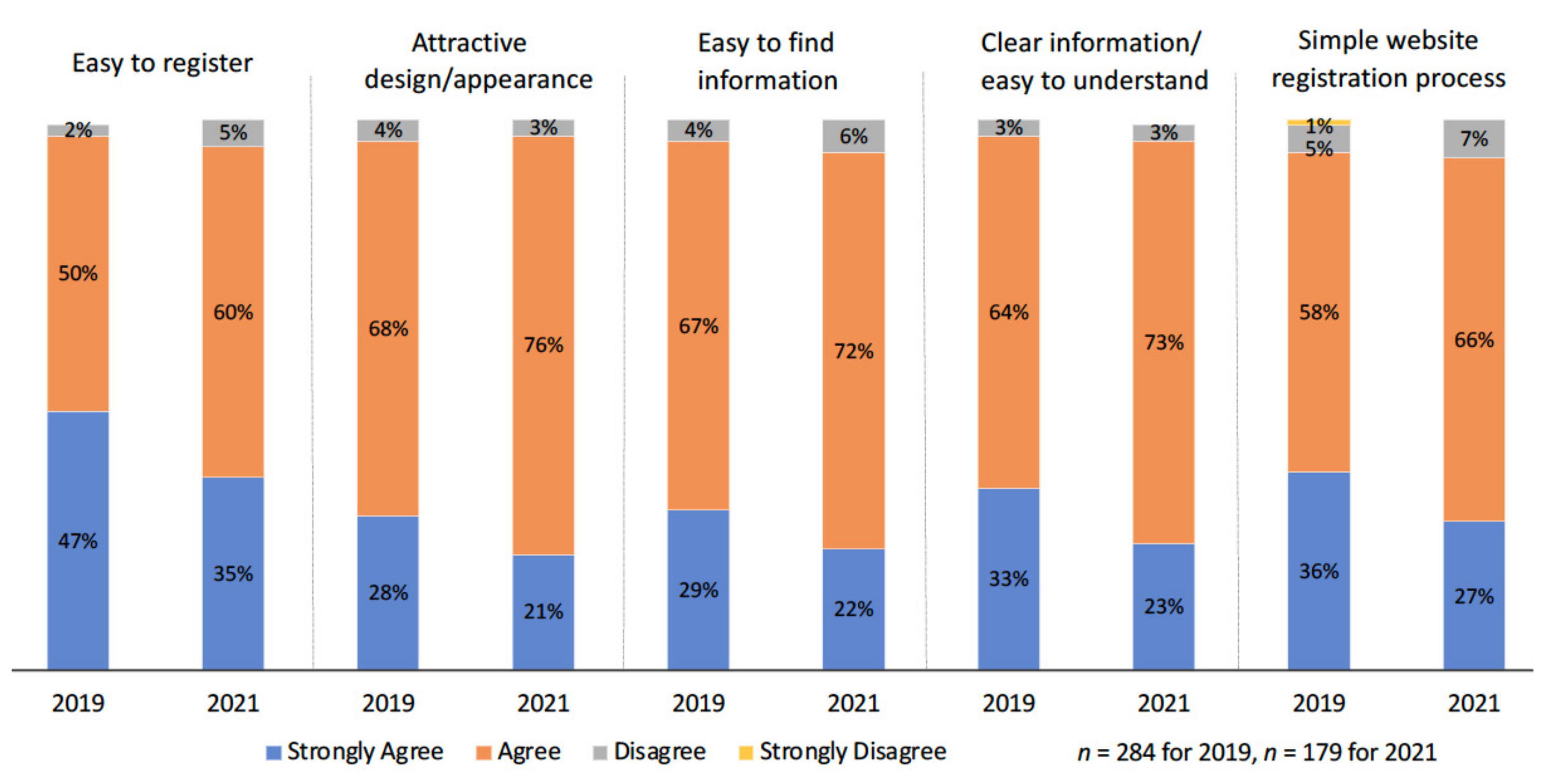
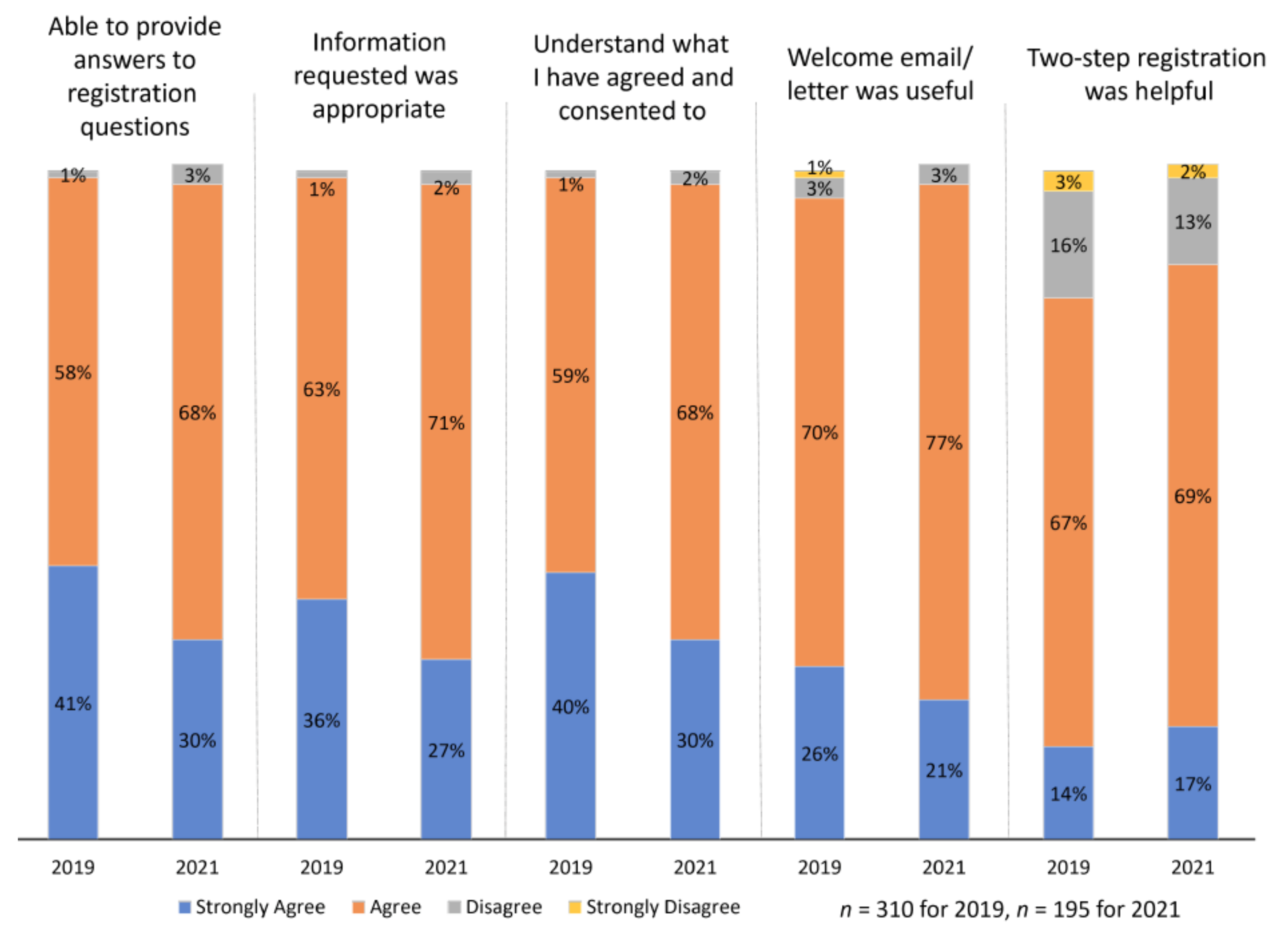
3.4.2. Volunteers’ Experience with StepUp Registration: Online, Helpdesk and Post
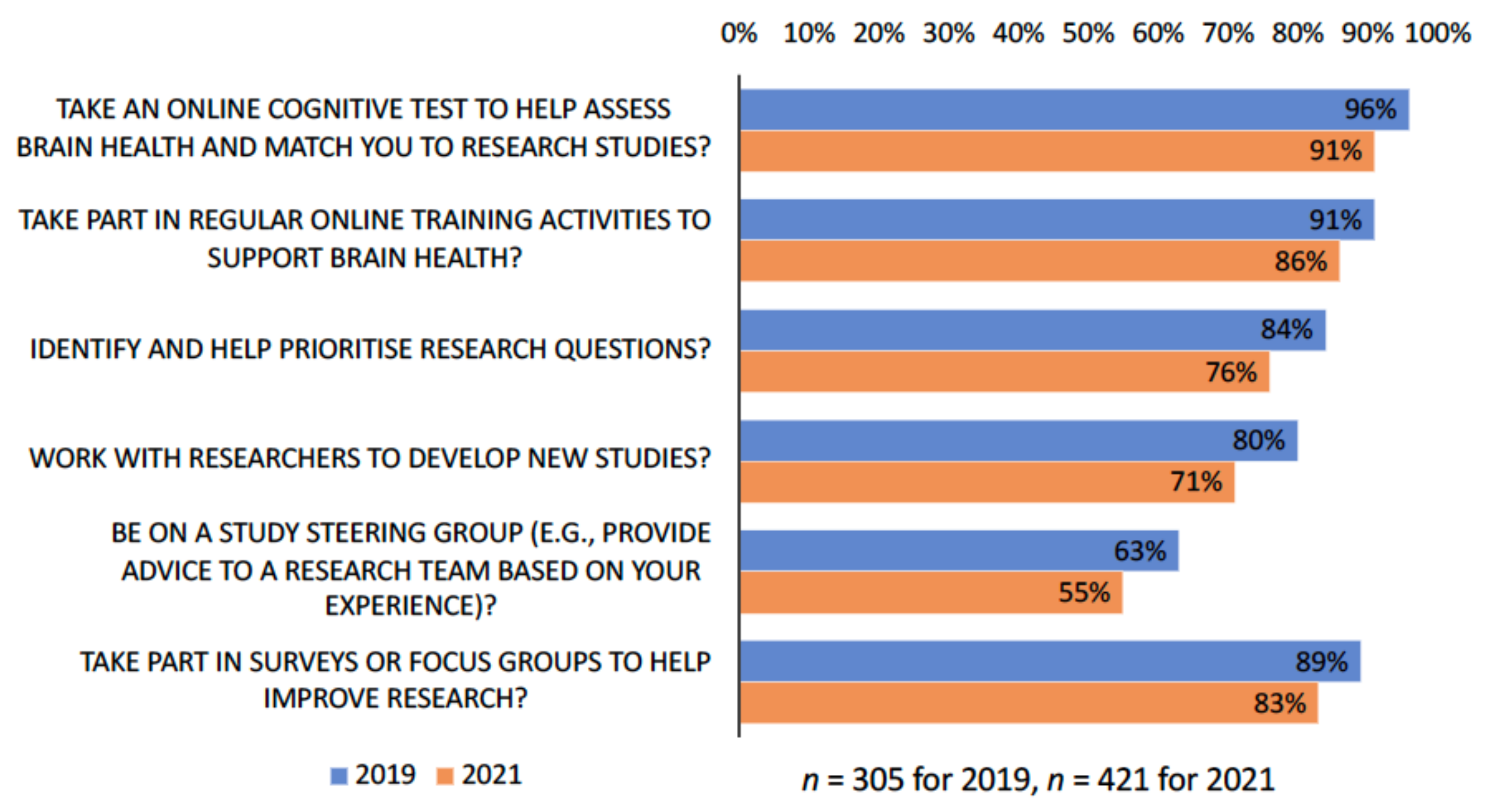
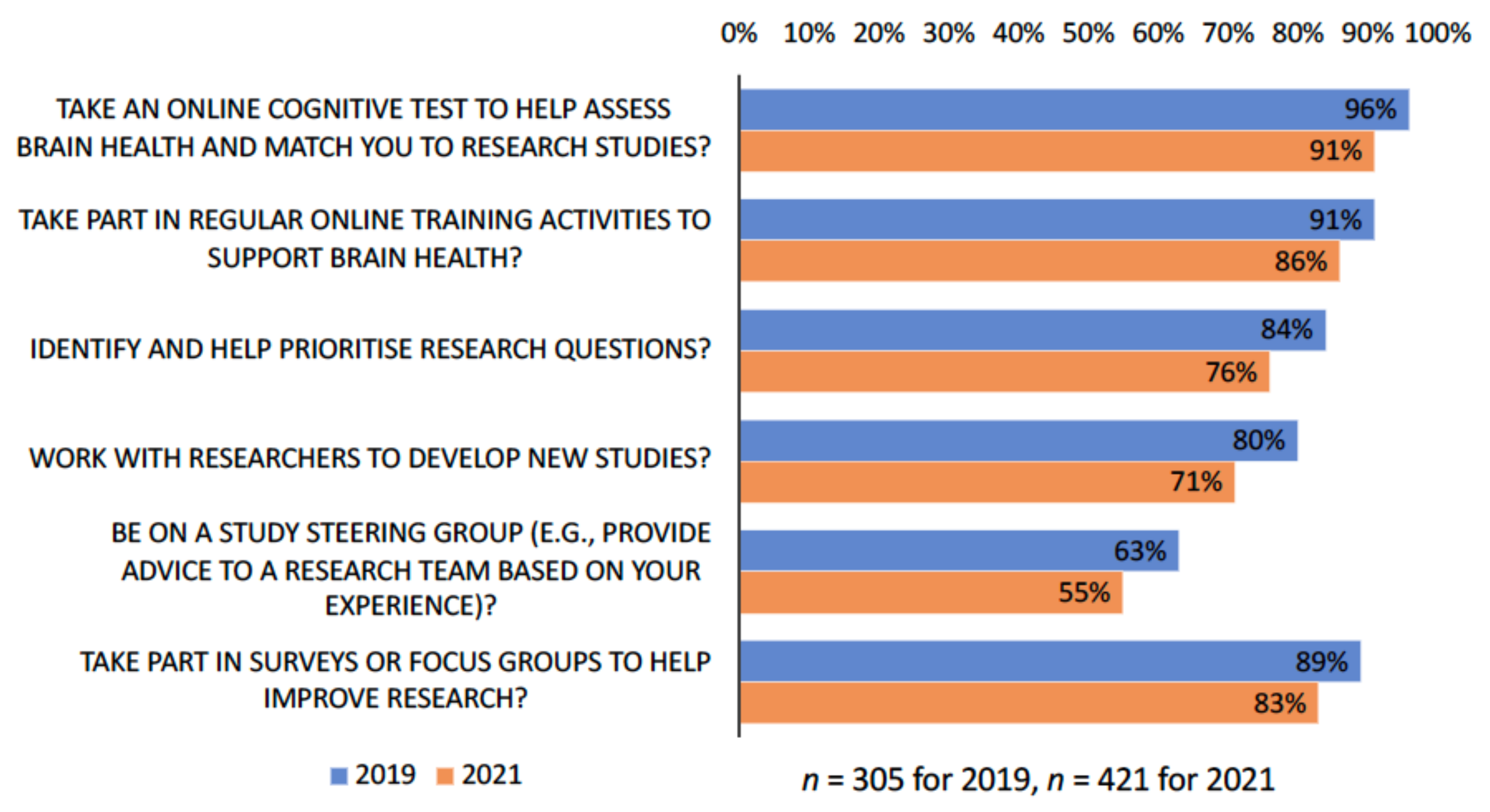
3.4.3. Volunteers’ Motivation to Join StepUp and Interest in Broad Research Activities
3.4.4. Volunteers’ Experience with Research Participation through StepUp
3.4.5. Researcher Experience with StepUp
“StepUp contributed more than half of our responses! We were thrilled by the number of responses we received though StepUp.”
“The survey has done really well since being on Step-up—it’s such a brilliant resource for age-related research!”
I think what influenced our relatively low number of StepUp volunteers is that we began recruitment in November and conducted this research over Dec/Jan so it might have corresponded with holiday time when many people might not have been available to participate in research. The platform was easy to use and to navigate. Volunteers were often responsive to invites for participation and all volunteers were interested in the topic of our research and provided some great feedback which was helpful.
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Dementia. Available online: https://www.who.int/news-room/fact-sheets/detail/dementia (accessed on 2 September 2021).
- World Health Organization. Global Action Plan on the Public Health Response to Dementia 2017–2025; World Health Organization: Geneva, Switzerland, 2017. [Google Scholar]
- Cote, D.N. Minimizing Trial Costs by Accelerating and Improving Enrollment and Retention. In Global Clinical Trials for Alzheimer’s Disease: Design, Implementation, and Standardization; Elsevier Inc.: Amsterdam, The Netherlands, 2013; pp. 197–215. [Google Scholar]
- Aisen, P.; Touchon, J.; Andrieu, S.; Boada, M.; Doody, R.; Nosheny, R.; Langbaum, J.; Schneider, L.; Hendrix, S.; Wilcock, G. Registries and Cohorts to Accelerate Early Phase Alzheimer’s Trials. A Report from the EU/US Clinical Trials in Alzheimer’s Disease Task Force. J. Prev. Alzheimer’s Dis. 2016, 3, 68–74. [Google Scholar]
- Fargo, K.N.; Carrillo, M.C.; Weiner, M.W.; Potter, W.Z.; Khachaturian, Z. The crisis in recruitment for clinical trials in Alzheimer’s and dementia: An action plan for solutions. Alzheimer’s Dement. 2016, 12, 1113–1115. [Google Scholar] [CrossRef]
- Grill, J.D. Recruiting to preclinical Alzheimer’s disease clinical trials through registries. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2017, 3, 205–212. [Google Scholar] [CrossRef] [PubMed]
- Watson, J.L.; Ryan, L.; Silverberg, N.; Cahan, V.; Bernard, M.A. Obstacles and opportunities in Alzheimer’s clinical trial recruitment. Health Aff. 2014, 33, 574–579. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Health Organization. Risk Reduction of Cognitive Decline and Dementia: WHO Guidelines; World Health Organization: Geneva, Switzerland, 2019. [Google Scholar]
- Livingston, G.; Sommerlad, A.; Orgeta, V.; Costafreda, S.G.; Huntley, J.; Ames, D.; Ballard, C.; Banerjee, S.; Burns, A.; Cohen-Mansfield, J. Dementia prevention, intervention, and care. Lancet 2017, 390, 2673–2734. [Google Scholar] [CrossRef] [Green Version]
- Livingston, G.; Huntley, J.; Sommerlad, A.; Ames, D.; Ballard, C.; Banerjee, S.; Brayne, C.; Burns, A.; Cohen-Mansfield, J.; Cooper, C. Dementia prevention, intervention, and care: 2020 report of the Lancet Commission. Lancet 2020, 396, 413–446. [Google Scholar] [CrossRef]
- Cahill, S.; Pierce, M.; Werner, P.; Darley, A.; Bobersky, A. A systematic review of the public’s knowledge and understanding of Alzheimer’s disease and dementia. Alzheimer Dis. Assoc. Disord. 2015, 29, 255–275. [Google Scholar] [CrossRef] [PubMed]
- Cations, M.; Radisic, G.; Crotty, M.; Laver, K.E. What does the general public understand about prevention and treatment of dementia? A systematic review of population-based surveys. PLoS ONE 2018, 13, e0196085. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Grill, J.D.; Galvin, J.E. Facilitating Alzheimer’s Disease research recruitment. Alzheimer Dis. Assoc. Disord. 2014, 28, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- World Dementia Council. Defeating Dementia: The Road to 2025; Wellcome Trust: London, UK, 2013. [Google Scholar]
- Kotting, P.; Smith, A.; Rossor, M. Harnessing Consumer Technologies and Clinical Data to Improve Recruitment to Clinical Studies: A Review of the First 12 Months of the Join Dementia Research Service in the United Kingdom. Alzheimer’s Dement. 2016, 12, P153. [Google Scholar] [CrossRef]
- Krysinska, K.; Sachdev, P.; Breitner, J.; Kivipelto, M.; Kukull, W.; Brodaty, H. Dementia registries around the globe and their applications: A systematic review. Alzheimer’s Dement. 2017, 13, 1031–1047. [Google Scholar] [CrossRef] [PubMed]
- Petersen, R.C.; Nixon, R.A.; Thies, W.; Taylor, A.; Geiger, A.T.; Cordell, C. Alzheimer’s Association® TrialMatch™: A next-generation resource for matching patients to clinical trials in Alzheimer’s disease and related disorders. Neurodegener. Dis. Manag. 2012, 2, 107–115. [Google Scholar] [CrossRef]
- Langbaum, J.B.; High, N.; Nichols, J.; Kettenhoven, C.; Reiman, E.M.; Tariot, P.N. The Alzheimer’s Prevention Registry: A Large Internet-Based Participant Recruitment Registry to Accelerate Referrals to Alzheimer’s-Focused Studies. J. Prev. Alzheimer’s Dis. 2020, 7, 242–250. [Google Scholar] [CrossRef]
- Langbaum, J.B.; Karlawish, J.; Roberts, J.S.; Wood, E.M.; Bradbury, A.; High, N.; Walsh, T.L.; Gordon, D.; Aggarwal, R.; Davis, P.; et al. GeneMatch: A novel recruitment registry using at-home APOE genotyping to enhance referrals to Alzheimer’s prevention studies. Alzheimer’s Dement. 2019, 15, 515–524. [Google Scholar] [CrossRef]
- Zwan, M.D.; van der Flier, W.M.; Cleutjens, S.; Schouten, T.C.; Vermunt, L.; Jutten, R.J.; van Maurik, I.S.; Sikkes, S.A.M.; Flenniken, D.; Howell, T.; et al. Dutch Brain Research Registry for study participant recruitment: Design and first results. Alzheimer’s Dement. Transl. Res. Clin. Interv. 2021, 7, e12132. [Google Scholar]
- Dementia Australia. Dementia Key Facts and Statistics; Dementia Australia: Melbourne, Australia, 2018. [Google Scholar]
- Dementia Australia. Dementia in Australia Prevalence Estimates 2021–2058; Dementia Australia: Melbourne, Australia, 2021. [Google Scholar]
- Juaristi, G.E.A.; Dening, K.H. Promoting participation of people with dementia in research. Nurs. Stand. 2016, 30, 38–43. [Google Scholar] [CrossRef]
- Join Dementia Research. JDR Newsletter May 2021. Available online: https://mailchi.mp/a42c7af3818f/jdr-newsletter-may-2652712 (accessed on 13 September 2021).
- Weiner, M.W.; Nosheny, R.; Camacho, M.; Truran-Sacrey, D.; Mackin, R.S.; Flenniken, D.; Ulbricht, A.; Insel, P.; Finley, S.; Fockler, J. The Brain Health Registry: An internet-based platform for recruitment, assessment, and longitudinal monitoring of participants for neuroscience studies. Alzheimer’s Dement. 2018, 14, 1063–1076. [Google Scholar] [CrossRef]
- Smith, A.M.; Kotting, P.M.; Rossor, M.N. Encouraging public participation in dementia research: Analysis of take-up and costs following mail out to 10,000 patients within general practice. Alzheimer’s Dement. 2017, 13, P861. [Google Scholar] [CrossRef]
- Join Dementia Research. Data and Statistics. Available online: https://nhs.joindementiaresearch.nihr.ac.uk/data-and-statistics (accessed on 13 September 2021).
- Einolf, C.J. Gender differences in the correlates of volunteering and charitable giving. Nonprofit Volunt. Sect. Q. 2011, 40, 1092–1112. [Google Scholar] [CrossRef]
- Smith, A.; Kotting, P.; Rossor, M. Join dementia research improving public access to research in the UK. In Proceedings of the 32nd International Conference of Alzheimer’s Disease International, Kyoto, Japan, 26–29 April 2017. [Google Scholar]
- Australian Bureau of Statistics. Census of Population and Housing: Cultural Diversity Data Cube ABS cat. no. 2071.0; Australian Bureau of Statistics (ABS): Canberra, Australia, 2017. [Google Scholar]
- Low, L.F.; Barcenilla-Wong, A.L.; Brijnath, B. Including ethnic and cultural diversity in dementia research. Med. J. Aust. 2019, 211, 345–346. [Google Scholar] [CrossRef]
- Cooper, C.; Tandy, A.R.; Balamurali, T.B.; Livingston, G. A systematic review and meta-analysis of ethnic differences in use of dementia treatment, care, and research. Am. J. Geriatr. Psychiatry 2010, 18, 193–203. [Google Scholar] [CrossRef] [PubMed]
- Berisic, M.; Nesvadba, N. Perceptions of Dementia in Ethnic Communities. Alzheimer’s Australia. October 2008. Available online: https://www.dementia.org.au/sites/default/files/Perceptions_of_dementia_in_ethnic_communities_-_project_report.pdf (accessed on 13 September 2021).
- Australian Institute of Health and Welfare. Older Australia at a Glance; AIHW: Canberra, Australia, 2018. [Google Scholar]
- Australian Institute of Health and Welfare. Australia’s Health 2018; AIHW: Canberra, Australia, 2018. [Google Scholar]
- Flicker, L.; Holdsworth, K. Aboriginal and Torres Strait Islander People and Dementia: A Review of the Research; Alzheimer’s Australia: Melbourne, Australia, 2014. [Google Scholar]
- Connell, C.M.; Shaw, B.A.; Holmes, S.B.; Foster, N.L. Caregivers’ attitudes toward their family members’ participation in Alzheimer disease research: Implications for recruitment and retention. Alzheimer Dis. Assoc. Disord. 2001, 15, 137–145. [Google Scholar] [CrossRef]
- Hughes, T.B.; Varma, V.R.; Pettigrew, C.; Albert, M.S.; Bowers, B.J. African Americans and clinical research: Evidence concerning barriers and facilitators to participation and recruitment recommendations. Gerontologist 2017, 57, 348–358. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Neugroschl, J.; Sewell, M.; De La Fuente, A.; Umpierre, M.; Luo, X.; Sano, M. Attitudes and Perceptions of Research in Aging and Dementia in an Urban Minority Population. J. Alzheimer’s Dis. 2016, 53, 69–72. [Google Scholar] [CrossRef] [Green Version]
- Hinton, L.; Guo, Z.; Hillygus, J.; Levkoff, S. Working with culture: A qualitative analysis of barriers to the recruitment of Chinese–American family caregivers for dementia research. J. Cross-Cult. Gerontol. 2000, 15, 119–137. [Google Scholar] [CrossRef]
- Greenhalgh, T.; Hinton, L.; Finlay, T.; Macfarlane, A.; Fahy, N.; Clyde, B.; Chant, A. Frameworks for supporting patient and public involvement in research: Systematic review and co-design pilot. Health Expect. 2019, 22, 785–801. [Google Scholar] [CrossRef]
- Flavin, T.; Sinclair, C. Reflections on involving people living with dementia in research in the Australian context. Australas. J. Ageing 2019, 38, 6–8. [Google Scholar] [CrossRef]
- Iliffe, S.; McGrath, T.; Mitchell, D. The impact of patient and public involvement in the work of the Dementias & Neurodegenerative Diseases Research Network (DeNDRoN): Case studies. Health Expect. 2013, 16, 351–361. [Google Scholar] [PubMed] [Green Version]
- World Health Organization. Global Status Report on the Public Health Response to Dementia; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Design | Study Description | Sites | Mat’d (Scr’d) | Ineligible/ Declined | Enrolled Numbers | Duration (Days) | Overall Numbers |
|---|---|---|---|---|---|---|---|
| Online survey (n = 14) | * Research volunteers’ motivation, needs, wellbeing and experiences | Nationwide | 692 (N/A) | N/A | 301 | N/A | 301 |
| * The role of habit in maintaining physical activity | Nationwide | 229 (N/A) | N/A | 60 | N/A | 126 | |
| * Healthy ageing, memory and technology | Nationwide | 757 (N/A) | N/A | 170 | N/A | 254 | |
| * Impact of COVID-19 on wellbeing and access to support | Nationwide | 264 (N/A) | N/A | 71 | N/A | 137 | |
| * Dementia, stigma and factors that affect self-disclosure | Nationwide | 802 (N/A) | N/A | 182 | N/A | 304 | |
| * Impact of COVID-19 on people with dementia/carers | Nationwide | 272 (N/A) | N/A | 16 | N/A | 46 | |
| * Needs assessment of technology in aged care | Nationwide | 590 (N/A) | N/A | 63 | N/A | 188 | |
| * Quality use of medicines in people with dementia | Nationwide | 866 (N/A) | N/A | 96 | N/A | 151 | |
| * The evidence-practice gap in young onset dementia care | Nationwide | 275 (N/A) | N/A | N/A | N/A | 214 | |
| * Beliefs and attitudes towards dementia | Nationwide | 1085 (N/A) | N/A | 165 | N/A | 185 | |
| Online healthy brain ageing psychoeducation and cognitive training | Nationwide | 113 (N/A) | N/A | In progress | N/A | In progress | |
| Experiences of adult children carer for parent with dementia | Nationwide | 252 (N/A) | N/A | In progress | N/A | ||
| Benefits of gardens and plants to caregiver’s wellbeing | Nationwide | 252 (N/A) | N/A | In progress | N/A | In progress | |
| Use of therapy-informed music in dementia care | Nationwide | 369 (N/A) | N/A | In progress | N/A | In progress | |
| Observational study (n = 17) | * Carers’ experiences of medication advice for people with dementia | Nationwide | 182 (155) | 65/1 | 22 | 15 | 30 |
| * Changed behaviors with memory and cognitive decline | Nationwide | 311 (60) | 6/3 | 51 | 61 | 52 | |
| * Impact of COVID-19 on the lives of people with dementia and carers | Nationwide | 214 (N/A) | 0/0 | 16 | N/A | 18 | |
| * Patient decision aid for deprescribing cholinesterase inhibitors | Nationwide | 333 (7) | 0/0 | 6 | 99 | 17 | |
| * Carer’s experiences during COVID-19 | Nationwide | 196 (Uk) | 0/0 | 29 | Uk | 29 | |
| Computerized cognitive tests | NSW | 158 (17) | 0/1 | In progress | 52 | In progress | |
| Early biological markers in familial non-AD | Nationwide | 346 (342) | 90/11 | 20 | 215 | In progress | |
| Financial skills in ageing and cognitive impairment | Nationwide | 766 (42) | 15/18 | 6 | 79 | In progress | |
| Gait and cognition study | NSW | 55 (0) | 0/0 | 0 | In progress | In progress | |
| Making an advance research directive | Nationwide | 85 (10) | 3/0 | 5 | 17 | In progress | |
| Validation of the Montreal Cognitive Assessment | NSW | 103 (0) | 0/0 | 0 | In progress | In progress | |
| Social health and reserve in people with dementia | Nationwide | 34 (28) | 17/5 | 1 | 13 | In progress | |
| Effect of hearing loss on cognitive impairment | NSW | 124 (123) | 45/27 | 12 | 205 | In progress | |
| Optic nerve decline and cognitive change | NSW | 275 (260) | 153/2 | 2 | 2 | In progress | |
| Habits on physical activity in people with MCI or memory concern | NSW | 33 (29) | 13/10 | 0 | In progress | In progress | |
| Safety for people with memory problems or dementia | Nationwide | 65 (0) | 0/0 | 0 | In progress | In progress | |
| Benefits of physical activity and brain health | Nationwide | 155 (0) | 0/0 | 0 | In progress | In progress | |
| Experimental study (n = 9) | * Exercise intervention in people with MCI (RCT) | NSW | 45 (45) | 41/4 | 0 | N/A | 68 |
| ** Effects of intranasal oxytocin on emotions | NSW | 14 (1) | 0/0 | 0 | N/A | 5 | |
| Sailuotong for VD or AD mixed with CVD | NSW, SA | 23 (12) | 3/4 | 1 | 262 | In progress | |
| Melatonin supplementation in MCI (RCT) | NSW | 19 (19) | 10/6 | 2 | 119 | In progress | |
| Online training and support for people with early-stage dementia and carers | NSW, QLD, VIC | 118 (57) | 0/21 | 1 | 17 | In progress | |
| Driving cessation and mobility in people with dementia (RCT) | NSW, QLD, VIC, WA | 364 (24) | 3/13 | 3 | 198 | In progress | |
| Telehealth psychotherapy for anxiety in people with cognitive impairment | Nationwide | 105 (50) | 4/7 | 1 | 71 | In progress | |
| Music and reading for people with Dementia (RCT) | Nationwide | 382 (327) | 68/24 | 25 | 175 | In progress | |
| Polypharmacy and reduction for general practice patients with dementia | WA | 36 (35) | 18/10 | 6 | 138 | In progress |
| Characteristics | 2019 Survey (n = 319) | 2021 Survey (n = 450) | |
|---|---|---|---|
| Gender | Female | 80% | 78% |
| Male | 20% | 22% | |
| Age | 18–44 | 8% | 9% |
| 45–64 | 42% | 40% | |
| 65+ | 51% | 51% | |
| Country of birth | Australia | 67% | 70% |
| Other (UK, NZ, etc.) | 33% | 30% | |
| Preferred language | English | 99% | 99% |
| Education | Year 11 or below | 12% | 11% |
| Year 12 or Diploma | 24% | 26% | |
| Bachelor’s Degree | 28% | 27% | |
| Graduate Diploma/Certificate | 13% | 11% | |
| Postgraduate Degree | 23% | 26% | |
| Marital Status | Single | 9% | 12% |
| Married/in de-facto | 66% | 67% | |
| Separated or divorced | 14% | 11% | |
| Widowed | 10% | 9% | |
| Unwilling to answer | 1% | 1% | |
| Employment Status * | Full-time | 18% | 21% |
| Part-time | 24% | 20% | |
| Student | 4% | 2% | |
| Home duties/carer | 5% | 6% | |
| Retired | 51% | 47% | |
| Unemployed | 1% | 2% | |
| Pension/Allowance | 11% | 12% | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeon, Y.-H.; Shin, M.; Smith, A.; Beattie, E.; Brodaty, H.; Frost, D.; Hobbs, A.; Kotting, P.; Petrie, G.; Rossor, M.; et al. Early Implementation and Evaluation of StepUp for Dementia Research: An Australia-Wide Dementia Research Participation and Public Engagement Platform. Int. J. Environ. Res. Public Health 2021, 18, 11353. https://doi.org/10.3390/ijerph182111353
Jeon Y-H, Shin M, Smith A, Beattie E, Brodaty H, Frost D, Hobbs A, Kotting P, Petrie G, Rossor M, et al. Early Implementation and Evaluation of StepUp for Dementia Research: An Australia-Wide Dementia Research Participation and Public Engagement Platform. International Journal of Environmental Research and Public Health. 2021; 18(21):11353. https://doi.org/10.3390/ijerph182111353
Chicago/Turabian StyleJeon, Yun-Hee, Mirim Shin, Adam Smith, Elizabeth Beattie, Henry Brodaty, Dennis Frost, Anthony Hobbs, Piers Kotting, Glenys Petrie, Martin Rossor, and et al. 2021. "Early Implementation and Evaluation of StepUp for Dementia Research: An Australia-Wide Dementia Research Participation and Public Engagement Platform" International Journal of Environmental Research and Public Health 18, no. 21: 11353. https://doi.org/10.3390/ijerph182111353
APA StyleJeon, Y.-H., Shin, M., Smith, A., Beattie, E., Brodaty, H., Frost, D., Hobbs, A., Kotting, P., Petrie, G., Rossor, M., Thompson, J., Vickers, J., & Waters, D. (2021). Early Implementation and Evaluation of StepUp for Dementia Research: An Australia-Wide Dementia Research Participation and Public Engagement Platform. International Journal of Environmental Research and Public Health, 18(21), 11353. https://doi.org/10.3390/ijerph182111353