Abstract
There is a paucity of published literature on the epidemiology of adult attention-deficit/hyperactivity disorder (ADHD). We investigated the time trends of the diagnostic and pharmacotherapy incidence of ADHD, including the first used medication, in the adult population based on a Korean population-based database from 2015 to 2018. The number of diagnosed cases of ADHD significantly increased from 7782 in 2015 to 17,264 in 2018 (p = 0.03), which is 0.02% to 0.04% of the total population. Similarly, the number of pharmacotherapy cases of ADHD significantly increased from 3886 in 2015 to 12,502 in 2018 (p = 0.01), which is 0.01% to 0.03% of total population. The most commonly used medication at the initiation of pharmacotherapy shifted from Penid in 2015 to Concerta in 2018. Furthermore, combination therapy with two or more drugs was the preferred method in 2016–2018. In conclusion, the identified diagnoses and pharmacotherapy incidences were very low, highlighting the need to improve the public’s awareness of adult ADHD.
1. Introduction
Attention-deficit/hyperactivity disorder (ADHD) is a common psychiatric disorder with a chronic course that can lead to negative outcomes without optimal treatment [1,2]. It was previously believed to occur only among children and adolescents. However, the concept of adult ADHD was established due to the reorganization of the Diagnostic and Statistical Manual of Mental Disorders [3], and subsequent research has been actively conducted.
The global prevalence of ADHD in children and adolescents is approximately 2–7% [4,5], and about half of cases are known to persist into adulthood [6]. In the USA, the administrative prevalence based on diagnosis ranged from 0.93 to 11.0% [7,8], while it ranged from 0.6 to 10% [9] based on prescription [10]. In the UK, the prevalence based on prescriptions ranged from 0.03 to 0.92% [11,12]. In studies outside the USA and the UK, such as in Denmark [13], Norway [14], and Australia [15], the administrative prevalence estimates were lower compared to those in the USA. Similarly, studies in Taiwan [16] and Korea [17] reported a lower prevalence. Although it is challenging to ascertain the incidence rate of mental disorders, Hong et al. investigated the diagnosis of ADHD and the transition to pharmacotherapy in children and adolescent populations by taking advantage of the mandatory universal national health insurance system in Korea [17]. They found that the diagnostic incidence was 0.3% and the pharmacotherapy incidence was 0.2%.
However, the epidemiological data of adult ADHD diagnosis and medication are limited compared to those of children and adolescents. In this study, we aimed to investigate the diagnostic and pharmacotherapeutic incidence of ADHD and conducted a trend analysis in the entire adult population (18 and above) using the National Health Insurance Services (NHIS) database.
2. Materials and Methods
2.1. Data Source and Study Population
This retrospective analysis used data from the NHIS claims database from 1 January 2014 to 31 December 2018. The inclusion criteria were as follows: (1) aged 18 and above and (2) the presence of an inpatient or outpatient medical claim containing a code for the diagnosis of ADHD (International Classification of Disease, 10the Revision code F90.0x) between 1 January 2014 and 31 December 2018, with no medication use during the 1 year preceding the claim. This study was approved by the institutional review board of Myongji Hospital (MJH 2019-05-014).
2.2. The Incidence of Adult ADHD Based on Diagnosis and Medication
Subjects diagnosed with ADHD (F90.0x) during a given year, but not the previous year, were defined as incident cases. The annual incidence was calculated from 2015 to 2018 by dividing the number of newly diagnosed cases of ADHD during each year by the number of person-years at risk in the NHIS dataset for the same year. The incidence of ADHD was calculated using the same method. The data on the total population aged 18 and above were obtained from the National Statistical Office (https://kosis.kr/statisticsList/statisticsListIndex.do?menuId=M_01_01&vwcd=MT_ZTITLE&parmTabId=M_01_01&outLink=Y&entrType=#content-group, accessed on 10 May 2021).
2.3. Other Measures
The demographic factors, such as age, sex, type of insurance, clinician specialty, and hospital level, were obtained from the NHIS database. Age was divided into the following six age groups: 18–23, 24–30, 31–40, 41–50, 51–60, and 61 years and over. The types of insurance were classified as national health insurance or medical aid. The clinicians’ specialties were categorized as psychiatry or other. The hospital levels were stratified into hospital and private clinics, and the initial ADHD medication was identified based on the list of medications (Table 1).

Table 1.
The available medication for attention-deficit/hyperactivity disorder in Korea.
2.4. Statistical Analysis
Descriptive statistics (means and frequencies) were used to characterize the medication use and the clinical and demographic variables. To assess the trends in adult ADHD diagnosis and medication use, we examined temporal changes from 2015 to 2018 using a time series linear model. SAS 9.3 (SAS Institute Inc., Cary, NC, USA) was used to link and analyze the data. The significance level was set at p < 0.05.
3. Results
3.1. Diagnostic Incidence of Adult ADHD from 2015 to 2018
The numbers and trends of annual incident cases are shown in Table 2 and Figure 1. The number of annual incident cases significantly increased from 7762 to 17,264 from 2015 to 2018 (p = 0.036). The annual diagnostic incidence during the study period also increased from 0.02% in 2015 to 0.04% in 2018. The diagnostic incidence showed an overall male predominance, though this trend gradually decreased. All the age groups, except the 31–40 year and 61 years and over groups, showed significant linear trends. New diagnoses by psychiatrists showed a statistically significant increase during the four-year period (p = 0.0466).
Table 2.
The diagnostic incidence of attention-deficit/hyperactivity disorder in adults.
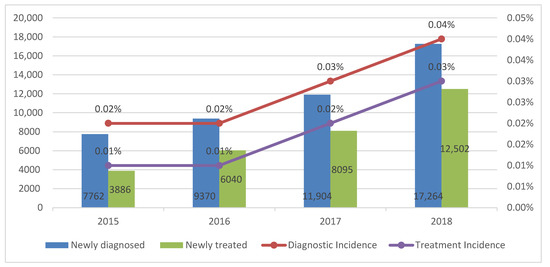
Figure 1.
The trends of number of cases and incidence among adults with attention deficit hyperactivity disorder between 2015 and 2018.
3.2. Medication Rate among Newly Diagnosed Adult ADHD from 2015 to 2018
The number and trends of the annual pharmacotherapy cases are shown in Table 3 and Figure 1. The number of newly diagnosed adult patients with ADHD who initiated medication significantly increased from 3886 to 12,502 from 2015 to 2018 (p = 0.0196). The annual treatment incidence during the study period also increased from 0.01% in 2015 to 0.03% in 2018. The treatment incidence showed an overall male predominance, though this trend gradually decreased. All the age groups, except the 61 years and over group, showed significant linear trends.
Table 3.
The treatment incidence of attention-deficit/hyperactivity disorder in adults.
3.3. First Medication Used for Adult ADHD
Most patients who initiated pharmacotherapy used two or more drugs, and the trends increased significantly (p = 0.02). The commonly used drugs were Penid, followed by Concerta, atomoxetine, and bupropion.
4. Discussion
This was the first nationwide study that investigated the diagnostic and pharmacotherapy incidence among adult patients with ADHD in Korea using nationally representative data from the NHIS.
The diagnostic and pharmacotherapy incidence in the adult population is only one-tenth that of the child and adolescent population in Korea [17]. It is worth noting that the number of diagnosed and medicated ADHD cases in the present study was limited. Thus, it does not support the debate that ADHD may be overdiagnosed and overtreated. It is noteworthy that the transition rate from diagnosis to treatment increased by 50% in 2015 and 2016, 67% in 2017, and 75% in 2018. This finding is consistent with that of the child and adolescent population [17]. The rate of pharmacotherapy in ADHD patients is known to have a wide variation ranging from 12 to 72% due to the differences in regional prescribing practice or different time frames for outcome assessment [18,19,20,21]. In Korea, however, the transition rate from diagnosis to treatment is high in all age groups. That is, once an individual is involved in clinical practice, the transition to treatment goes smoothly.
During the study period, the trends of both diagnosis and pharmacotherapy significantly increased. Although it is not possible to compare directly because of the different methods and periods of various studies, the current study found a significant increase in the trends of both diagnosis and pharmacotherapy among the adult population, consistent with studies in Taiwan [22] and Denmark [23]. However, the extent or absolute figure was remarkably low compared to that in other studies [22,23]. This is most likely due to the cultural differences that affect people’s attitudes towards psychiatric diagnosis and treatment [22], and in part by the fact that the Food and Drug Administration only approved ADHD medication for use in the adult population in September 2016.
In the trend analysis, the 18–23 years group showed a significant decrease in both diagnosis and pharmacotherapy, but the latter significantly increased in the 24–50 years group. We speculate that the 18–23 years age group are given autonomy after high school graduation and will exist outside the treatment boundary because it is a period with few compulsory tasks, such as work or school. Meanwhile, the 24–50 years age group, the period in which productive activities must be performed at work, is considered to be included in the treatment boundary due to their self-awareness of the symptoms or by others. The increase in the diagnosis and pharmacotherapy of the adult population could play a pivotal role in lowering the socioeconomic cost of ADHD [24].
The male predominance decreased during the study period in both the diagnosed (1.83 in 2015; 1.45 in 2018) and treatment population (1.74 in 2015; 1.39 in 2018). This finding is consistent with the published results [22].
Although the current study was outstanding in its analysis of the trend of adult ADHD using nationwide population data, several limitations need to be acknowledged. First, the ADHD diagnoses used in the study were derived from administrative claims data based on the International Classification of Disease 10th edition codes by physicians, rather than from structured clinical interviews. Second, the identified incidence rate in this study may be an underestimation of the actual incidence, as the study included only those who visited a clinic or hospital, that is, they had healthcare-seeking behavior. Third, caution is warranted when generalizing the results to other countries where no mandatory NHI system has been adopted.
5. Conclusions
Despite the above-mentioned limitations, the current study is among the few to date that have investigated the trends in the diagnostic and pharmacotherapy incidence of ADHD in the adult population.
Author Contributions
Conceptualization, S.-M.L. and M.H.; methodology, I.-H.O.; software, I.-H.O.; formal analysis, H.-K.C.; data curation, H.-K.C.; writing—original draft preparation, S.-M.L. and M.H.; writing—review and editing, S.-M.L. and M.H.; visualization, S.-M.L.; supervision, M.H.; funding acquisition, M.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Research Fund of Myongji Hospital, grant number 2001-03-04.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki, and approved by the Institutional Review Board of Myongji Hospital (MJH 2019-05-014).
Informed Consent Statement
Not applicable.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Paik, J.W.; Kim, K.H.; Lee, S.M.; Hong, M. Postdischarge Suicide and Death in South Korean Children and Adolescents Hospitalized for a Psychiatric Illness. J. Am. Acad. Child. Adolesc. Psychiatry 2018, 57, 508.e1–514.e1. [Google Scholar] [CrossRef] [PubMed]
- Barkley, R.A.; Fischer, M.; Smallish, L.; Fletcher, K. Young adult outcome of hyperactive children: Adaptive functioning in major life activities. J. Am. Acad. Child. Adolesc. Psychiatry 2006, 45, 192–202. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. DSM-5 Task Force, Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013; p. 947. [Google Scholar]
- Polanczyk, G.V.; Willcutt, E.; Salum, G.; Kieling, C.; Rohde, L. ADHD prevalence estimates across three decades: An updated systematic review and meta-regression analysis. Int. J. Epidemiol. 2014, 43, 434–442. [Google Scholar] [CrossRef]
- Sayal, K.; Prasad, V.; Daley, D.; Ford, T.; Coghill, C. ADHD in children and young people: Prevalence, care pathways, and service provision. Lancet Psychiatry 2018, 5, 175–186. [Google Scholar] [CrossRef]
- Simon, V.; Czobor, P.; Bálint, S.; Mészáros, A.; Bitter, I. Prevalence and correlates of adult attention-deficit hyperactivity disorder: Meta-analysis. Br. J. Psychiatry 2009, 194, 204–211. [Google Scholar] [CrossRef]
- Fontanella, C.A.; Phillips, G.S.; Bridge, J.A.; Campo, J.V. Trends in psychotropic medication use for Medicaid-enrolled preschool children. J. Child Fam. Stud. 2014, 23, 617–631. [Google Scholar] [CrossRef]
- Visser, S.N.; Danielson, M.; Bitsko, R.; Holbrook, J.; Kogan, M.; Ghandour, R.; Perou, R.; Blumberg, S. Trends in the parent-report of health care provider-diagnosed and medicated attention-deficit/hyperactivity disorder: United States, 2003–2011. J. Am. Acad. Child. Adolesc. Psychiatry 2014, 53, 34.e2–46.e2. [Google Scholar] [CrossRef]
- Olfson, M.; Marcus, S.; Weissman, M.; Jensen, P. National trends in the use of psychotropic medications by children. J. Am. Acad. Child. Adolesc. Psychiatry 2002, 41, 514–521. [Google Scholar] [CrossRef]
- LeFever, G.B.; Morrow, A.L. The extent of drug therapy for attention deficit-hyperactivity disorder among children in public schools. Am. J. Public Health 1999, 89, 1359–1364. [Google Scholar] [CrossRef]
- Hsia, Y.; Maclennan, K. Rise in psychotropic drug prescribing in children and adolescents during 1992–2001: A population-based study in the UK. Eur. J. Epidemiol. 2009, 24, 211–216. [Google Scholar] [CrossRef]
- McCarthy, S.; Wilton, L.; Murray, M.; Hodgkins, P.; Asherson, P.; Wong, I. The epidemiology of pharmacologically treated attention deficit hyperactivity disorder (ADHD) in children, adolescents and adults in UK primary care. BMC Pediatr. 2012, 12, 78. [Google Scholar] [CrossRef]
- Pottegard, A.; Hallas, J.; Diaz, H.; Zoega, H. Children’s relative age in class and use of medication for ADHD: A Danish Nationwide Study. J. Child. Psychol. Psychiatry 2014, 55, 1244–1250. [Google Scholar] [CrossRef] [PubMed]
- Norum, J.; Olse, A.; Horh, F.; Heyd, A.; Totth, A. Medical treatment of children and youths with attention-deficit/hyperactivity disorder (ADHD): A Norwegian Prescription Registry Based Study. Glob. J. Health Sci. 2014, 6, 155–162. [Google Scholar] [CrossRef]
- Prosser, B.; Lambert, L.C.; Reid, R. Psychostimulant prescription for ADHD in new South Wales: A longitudinal perspective. J. Attent. Disord. 2015, 19, 284–292. [Google Scholar] [CrossRef]
- Chien, I.C.; Lin, C.; Chou, Y.; Chou, P. Prevalence, incidence, and stimulant use of attention-deficit hyperactivity disorder in Taiwan, 1996–2005: A national population-based study. Soc. Psychiatry Psychiatr. Epidemiol. 2012, 47, 1885–1890. [Google Scholar] [CrossRef]
- Hong, M.; Kwack, Y.; Joung, Y.; Lee, S.; Kim, B.; Sohn, S.; Chung, U.; Yang, J.; Bhang, S.; Hwang, J.; et al. Nationwide rate of attention-deficit hyperactivity disorder diagnosis and pharmacotherapy in Korea in 2008–2011. Asia Pac. Psychiatry 2014, 6, 379–385. [Google Scholar] [CrossRef] [PubMed]
- Wolraich, M.L.; Hannah, J.; Baumgaertel, A.; Feurer, I. Examination of DSM-IV criteria for attention deficit/hyperactivity disorder in a county-wide sample. J. Dev. Behav. Pediatr. 1998, 19, 162–168. [Google Scholar] [CrossRef]
- Jensen, P.S.; Kettle, L.; Roper, M.T.; Sloan, M.T.; Dulcan, M.K.; Hoven, C.; Bird, H.R.; Bauermeister, J.; Payne, J. Are stimulants overprescribed? Treatment of ADHD in four U.S. communities. J. Am. Acad Child. Adolesc. Psychiatry 1999, 38, 797–804. [Google Scholar] [CrossRef][Green Version]
- Angold, A.; Erkanli, A.; Egger, H.; Costello, E. Stimulant treatment for children: A community perspective. J. Am. Acad. Child Adolesc. Psychiatry 2000, 39, 975–984. [Google Scholar] [CrossRef]
- Froehlich, T.E.; Lanphear, B.; Epstein, J.; Barbaresi, W.; Katusic, S.; Kahn, S. Prevalence, recognition, and treatment of attention-deficit/hyperactivity disorder in a national sample of US children. Arch. Pediatr. Adolesc. Med. 2007, 161, 857–864. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.L.; Wang, J.J.; Ho, C.H. Trends in incidence rates of diagnosed attention-deficit/hyperactivity disorder (ADHD) over 12 years in Taiwan: A nationwide population-based study. Psychiatry Res. 2020, 284, 112792. [Google Scholar] [CrossRef] [PubMed]
- Mohr, J.C.; Steinhausen, H.C. Time trends in incidence rates of diagnosed attention-deficit/hyperactivity disorder across 16 years in a nationwide Danish registry study. J. Clin. Psychiatry 2015, 76, e334–e341. [Google Scholar]
- Hong, M.; Park, B.; Lee, S.; Bahn, G.; Kim, M.; Park, S.; Park, S. Economic Burden and Disability-Adjusted Life Years (DALYs) of Attention Deficit/Hyperactivity Disorder. J. Atten. Disord. 2020, 24, 823–829. [Google Scholar] [CrossRef] [PubMed]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).