
One Health in Indigenous Communities: A Critical Review of the Evidence

 , , ,
, , ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Indigenous Approach
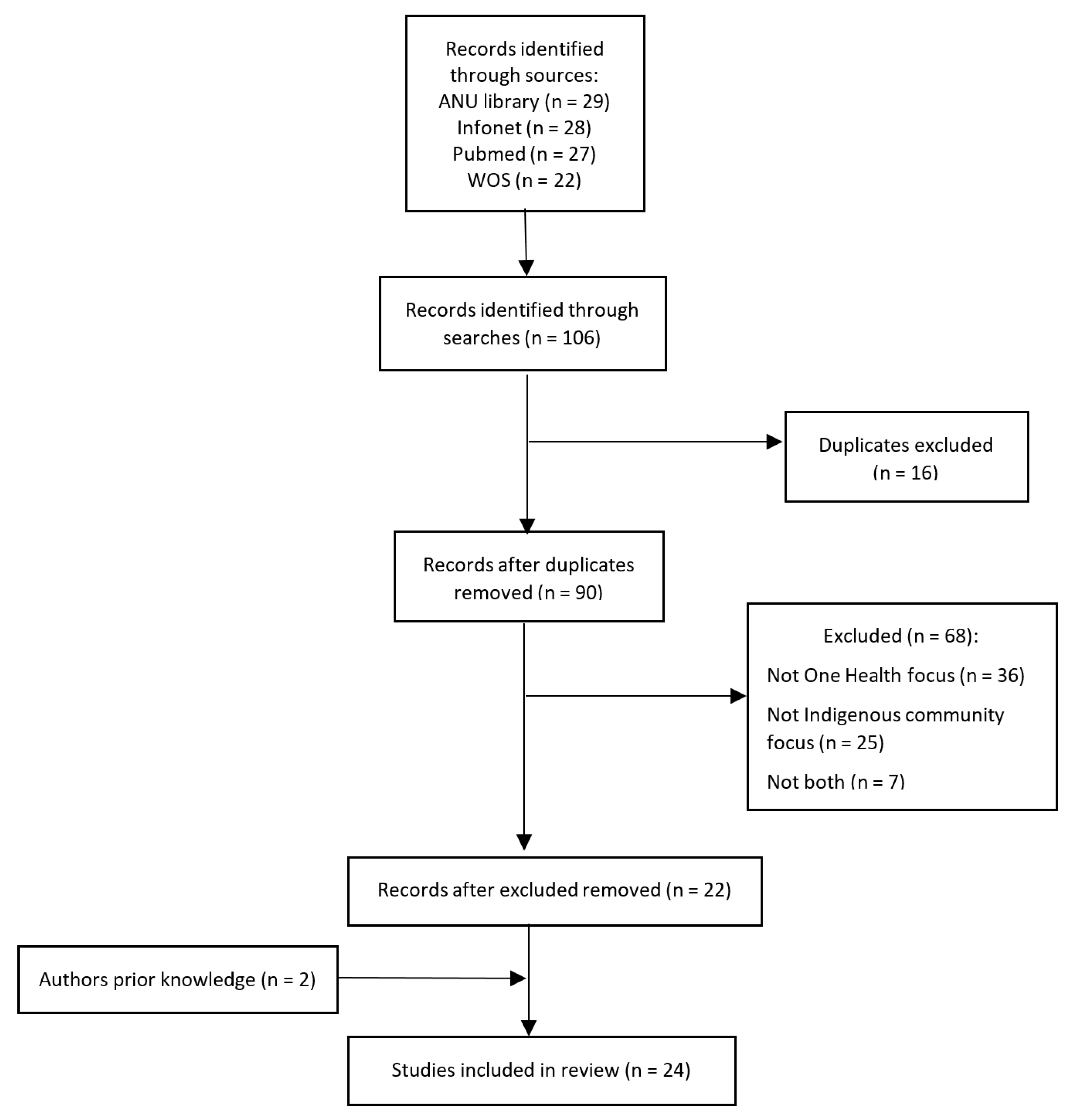
2.2. Search Strategy
- Ecohealth: ‘Ecohealth is committed to fostering the health of humans, animals, and ecosystems and to conducting research which recognizes the inextricable linkages between the health of all species and their environments’ [9] (p. 3);
- One Health: ‘One Health is the collaborative effort of multiple health science professions, together with their related disciplines, and institutions—working locally, nationally, and globally—to attain optimal health for people, domestic animals, wildlife, plants, and our environment’ [9] (p. 2–3);
- One Welfare: ‘One Welfare describes the inter-relationship between animal welfare, human wellbeing and the physical and social environment’ [7] (p. 1);
- Planetary Health: ‘The achievement of the highest attainable standard of health, well-being, and equity worldwide through judicious attention to the human systems—political, economic, and social—that shape the future of humanity and the Earth’s natural systems that define the safe environmental limits within which humanity can flourish’ [9] (p. 4).
2.3. Literature Sources and Search Terms
2.4. Selection of Studies
- Original research;
- Written in English;
- Published between 2010 and 2020;
- Full text available;
- One Health, Ecohealth, Planetary Health, or One Welfare focus;
- Animal, human, and/or environmental health component (at least two of these);
- An indigenous group as the main human population of interest.
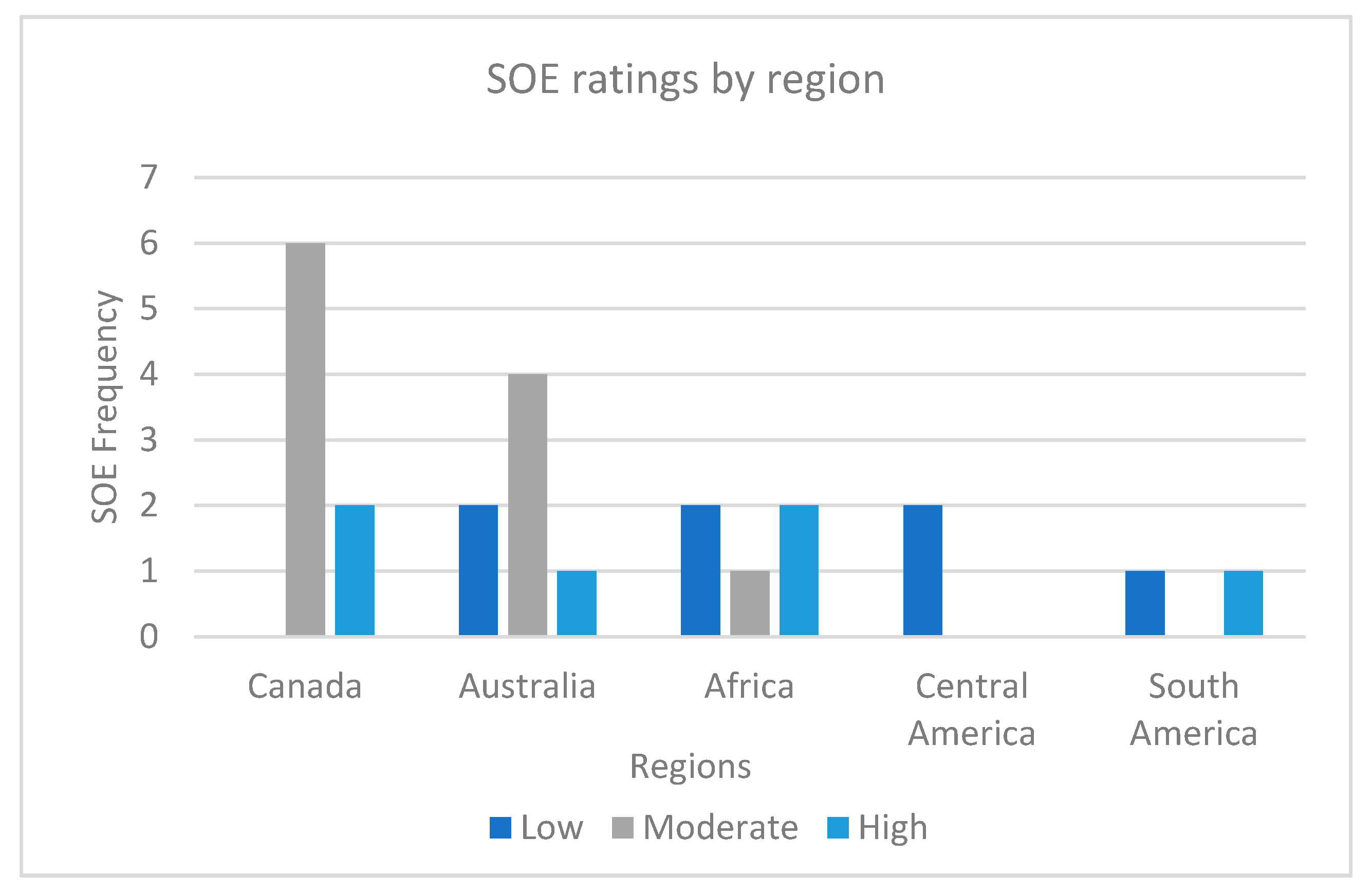
2.5. Summarising and Assessing the Strength of Evidence (SOE)
- 0 domains met = insufficient SOE;
- 1–2 domains met = low SOE;
- 3–4 domains met = moderate SOE;
- 5–6 domains met = high SOE.
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Roncada, P.; Modesti, A.; Timperio, A.M.; Bini, L.; Castagnola, M.; Fasano, M.; Urbani, A. One Medicine–One Health–one biology and many proteins: Proteomics on the verge of the One Health approach. Mol. Biosyst. 2014, 10, 1226–1227. [Google Scholar] [CrossRef]
- Dudgeon, P.; Milroy, H.; Walker, R. Working Together: Aboriginal and Torres Strait Islander Mental Health and Wellbeing Principles and Practice; Commonwealth of Australia: Canberra, Australia, 2014. [Google Scholar]
- World Health Organization. Health Promotion Glossary; World Health Organization: Geneva, Switzerland, 1998. [Google Scholar]
- Lerner, H. The philosophical roots of the “One Medicine” movement: An analysis of some relevant ideas by Rudolf Virchow and Calvin Schwabe with their modern implications. J. Studia Philos. Est. 2013, 6, 97–109. [Google Scholar] [CrossRef]
- Zinsstag, J.; Mackenzie, J.; Jeggo, M.; Heymann, D.; Patz, J.; Daszak, P. Mainstreaming One Health. Ecohealth 2012, 9, 107–110. [Google Scholar] [CrossRef]
- One Health Commission. What Is One Health? Available online: https://www.onehealthcommission.org/en/why_one_health/what_is_one_health/] (accessed on 19 October 2021).
- Pinillos, R.G. One Welfare, companion animals and their vets. J. Companion Anim. 2018, 23, 598. [Google Scholar] [CrossRef]
- Zinsstag, J.; Schelling, E.; Waltner-Toews, D.; Tanner, M. From “One Medicine” to “One Health” and systemic approaches to health and well-being. Prev. Vet. Med. 2011, 101, 148–156. [Google Scholar] [CrossRef] [PubMed]
- Lerner, H.; Berg, C. A comparison of three holistic approaches to health: One Health, Ecohealth, and Planetary Health. Front. Vet. Sci. 2017, 4, 163–170. [Google Scholar] [CrossRef]
- World Health Organization; Food and Agriculture Organization of the United Nations; World Organisation for Animal Health. Taking a Multisectoral One Health Approach: A Tripartite Guide to Addressing Zoonotic Diseases in Countries; World Health Organization, Food and Agriculture Organization of the United Nations, World Organisation for Animal Health: Paris, France, 2019. [Google Scholar]
- United Nations Environment Programme and International Livestock Research Institute. Preventing the Next Pandemic: Zoonotic Diseases and How to Break the Chain of Transmission; United Nations Environment Programme: Nairobi, Kenya, 2020. [Google Scholar]
- Harrison, S.; Baker, M.G.; Benschop, J.; Death, R.G.; French, N.P.; Harmsworth, G.; Lake, R.J.; Lamont, I.L.; Priest, P.C.; Ussher, J.E.; et al. One Health Aotearoa: A transdisciplinary initiative to improve human, animal and environmental health in New Zealand. One Health Outlook 2020, 2, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Harper, S.L.; Edge, V.L.; Ford, J.; Willox, A.C.; Wood, M.; McEwen, S.A.; IHACC Research Team; RICG. Climate-sensitive health priorities in Nunatsiavut, Canada. BMC Public Health 2015, 15, 605–623. [Google Scholar] [CrossRef]
- Dudley, J.P.; Hoberg, E.P.; Jenkins, E.J.; Parkinson, A.J. Climate change in the North American Arctic: A One Health perspective. Ecohealth 2015, 12, 713–725. [Google Scholar] [CrossRef]
- Degeling, C.; Brookes, V.; Lea, T.; Ward, M. Rabies response, One Health and more-than-human considerations in Indigenous communities in Northern Australia. Soc. Sci. Med. 2018, 212, 60–67. [Google Scholar] [CrossRef]
- World Health Organization. The Control of Neglected Zoonotic Diseases: A Route to Poverty Alleviation: Report of a Joint WHO; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Smout, F.; Schrieber, L.; Speare, R.; Skerratt, L.F. More bark than bite: Comparative studies are needed to determine the importance of canine zoonoses in Aboriginal communities. A critical review of published research. Zoonoses Public Health 2017, 64, 495–504. [Google Scholar] [CrossRef]
- Molyneux, D.; Hallaj, Z.; Keusch, G.T.; McManus, D.P.; Ngowi, H.; Cleaveland, S.; Ramos-Jimenez, P.; Gotuzzo, E.; Kar, K.; Sanchez, A. Zoonoses and marginalised infectious diseases of poverty: Where do we stand? Parasites Vectors 2011, 4, 106–112. [Google Scholar] [CrossRef] [PubMed]
- Johnson, I.; Hansen, A.; Bi, P. The challenges of implementing an integrated One Health surveillance system in Australia. Zoonoses Public Health 2018, 65, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Baker, T.; Rock, M.; Brook, R.; van der Meer, F.; Kutz, S. Indigenous community perspectives on dogs in Northern Canada after 10 years of veterinary services indicated improved animal and human welfare. Prev. Vet. Med. 2020, 181, 105061. [Google Scholar] [CrossRef]
- Galaz, V.; Leach, M.; Scoones, I.; Stein, C. The political economy of One Health research and policy. In STEPS Working Paper 81; STEPS Centre: Brighton, UK, 2015. [Google Scholar]
- Hillier, S.A.; Taleb, A.; Chaccour, E.; Aenishaenslin, C. Examining the concept of One Health for Indigenous communities: A systematic review. One Health 2021, 12, 100248. [Google Scholar] [CrossRef] [PubMed]
- Senior, K.; Chenhall, R.; McRae-Williams, E.; Daniels, D.; Rogers, K. Dogs and people in Aboriginal communities: Exploring the relationship within the context of the social determinants of health. J. Environ. Health 2006, 6, 39–46. [Google Scholar]
- Constable, S.; Dixon, R.; Dixon, R. For the love of dog: The human–dog bond in rural and remote Australian Indigenous communities. Anthrozoös 2010, 23, 337–349. [Google Scholar] [CrossRef]
- Ma, G.C.; Ford, J.; Lucas, L.; Norris, J.M.; Spencer, J.; Withers, A.-M.; Ward, M.P. “They reckon they’re man’s best friend and I believe that.” Understanding relationships with dogs in Australian Aboriginal communities to inform effective dog population management. Animals 2020, 10, 810. [Google Scholar] [CrossRef]
- Rabinowitz, P.; Conti, L. Human-Animal Medicine: Clinical Approaches to Zoonoses, Toxicants and Other Shared Health Risks; Saunders Elsevier: Philadelphia, PA, USA, 2010. [Google Scholar]
- Ma, G.C.; Withers, A.-M.; Spencer, J.; Norris, J.M.; Ward, M.P. Evaluation of a dog population management intervention: Measuring indicators of impact. Animals 2020, 10, 1061. [Google Scholar] [CrossRef]
- Dhillon, J.; Favel, D.; Delorme, D.; Ratt, A.; Epp, T. Finding pathways for bite prevention and decreasing dog populations: The process of animal control for Indigenous communities in Canada. J. Indig. Wellbeing 2016, 2, 82–92. [Google Scholar]
- Grant, M.J.; Booth, A. A typology of reviews: An analysis of 14 review types and associated methodologies. Health Inf. Libr. J. 2009, 26, 91–108. [Google Scholar] [CrossRef]
- Rigney, L.-I. Internationalization of an Indigenous anticolonial cultural critique of research methodologies: A guide to Indigenist research methodology and its principles. Wicazo Sa Rev. 1999, 14, 109–121. [Google Scholar] [CrossRef]
- Huria, T.; Palmer, S.C.; Pitama, S.; Beckert, L.; Lacey, C.; Ewen, S.; Smith, L.T. Consolidated criteria for strengthening reporting of health research involving indigenous peoples: The CONSIDER statement. BMC Med Res. Methodol. 2019, 19, 173. [Google Scholar] [CrossRef]
- Berkman, N.D.; Lohr, K.N.; Ansari, M.; McDonagh, M.; Balk, E.; Whitlock, E.; Reston, J.; Bass, E.; Butler, M.; Gartlehner, G. Grading the strength of a body of evidence when assessing health care interventions for the effective health care program of the Agency for Healthcare Research and Quality: An update. In Methods Guide for Effectiveness and Comparative Effectiveness Reviews [Internet]; Agency for Healthcare Research and Quality: Rockville, MD, USA, 2013. [Google Scholar]
- Berkman, N.D.; Lohr, K.N.; Ansari, M.T.; Balk, E.M.; Kane, R.; McDonagh, M.; Morton, S.C.; Viswanathan, M.; Bass, E.B.; Butler, M.; et al. Grading the strength of a body of evidence when assessing health care interventions: An EPC update. J. Clin. Epidemiol. 2015, 68, 1312–1324. [Google Scholar] [CrossRef]
- Goldet, G.; Howick, J. Understanding GRADE: An introduction. J. Evid.-Based Med. 2013, 6, 50–54. [Google Scholar] [CrossRef]
- Olsen, A.; Lovett, R. Existing knowledge, practice and responses to violence against women in Australian Indigenous communities. In Landscapes State of Knowledge Paper; ANROWS: Sydney, Australia, 2016. [Google Scholar]
- Anthonj, C.; Diekkrüger, B.; Borgemeister, C.; Thomas, K. Health risk perceptions and local knowledge of water-related infectious disease exposure among Kenyan wetland communities. Int. J. Hyg. Environ. Health 2019, 222, 34–48. [Google Scholar] [CrossRef] [PubMed]
- Bardosh, K.; Sambo, M.; Sikana, L.; Hampson, K.; Welburn, S.C. Eliminating rabies in Tanzania? Local understandings and responses to mass dog vaccination in Kilombero and Ulanga districts. PLOS Negl. Trop. Dis. 2014, 8, e2935. [Google Scholar] [CrossRef] [PubMed]
- Bevilacqua, M.; Rubio-Palis, Y.; Medina, D.A.; Cárdenas, L. Malaria control in Amerindian communities of Venezuela. Ecohealth 2015, 12, 253–266. [Google Scholar] [CrossRef] [PubMed]
- Riley, T.; Lovett, R.; Thandrayen, J.; Cumming, B.; Thurber, K.A. Evaluating impacts of a One Health approach to companion animal health and management in a remote Aboriginal community in the Northern Territory, Australia. Animals 2020, 10, 1790. [Google Scholar] [CrossRef] [PubMed]
- Schurer, J.M.; Ndao, M.; Skinner, S.; Irvine, J.; Elmore, S.A.; Epp, T.; Jenkins, E.J. Parasitic zoonoses: One Health surveillance in Northern Saskatchewan. PLOS Negl. Trop. Dis. 2013, 7, e2141. [Google Scholar] [CrossRef]
- Schurer, J.M.; Phipps, K.; Okemow, C.; Beatch, H.; Jenkins, E. Stabilizing dog populations and improving animal and public health through a participatory approach in Indigenous communities. Zoonoses Public Health 2015, 62, 445–455. [Google Scholar] [CrossRef] [PubMed]
- Aenishaenslin, C.; Brunet, P.; Lévesque, F.; Gouin, G.; Simon, A.; Saint-Charles, J.; Leighton, P.; Bastian, S.; Ravel, A. Understanding the Connections Between Dogs, Health and Inuit Through a Mixed-Methods Study. Ecohealth 2019, 16, 151–160. [Google Scholar] [CrossRef]
- Aenishaenslin, C.; Simon, A.; Forde, T.; Ravel, A.; Proulx, J.; Fehlner-Gardiner, C.; Picard, I.; Bélanger, D. Characterizing rabies epidemiology in remote Inuit communities in Québec, Canada: A “One Health” approach. EcoHealth 2014, 11, 343–355. [Google Scholar] [CrossRef] [PubMed]
- Cott, P.A.; Amos, A.L.; Guzzo, M.M.; Chavarie, L.; Goater, C.P.; Muir, D.C.G.; Evans, M.S. Can traditional methods of selecting food accurately assess fish health? Arct. Sci. 2018, 4, 205–222. [Google Scholar] [CrossRef]
- Gabriele-Rivet, V.; Brookes, V.; Arsenault, J.; Ward, M. Hunting practices in Northern Australia and their implication for disease transmission between community dogs and wild dogs. Aust. Vet. J. 2019, 97, 268–276. [Google Scholar] [CrossRef]
- Kansiime, C.; Atuyambe, L.M.; Asiimwe, B.B.; Mugisha, A.; Mugisha, S.; Guma, V.; Rwego, I.B.; Rutebemberwa, E. Community perceptions on integrating animal vaccination and health education by veterinary and public health workers in the prevention of brucellosis among pastoral communities of South Western Uganda. PLoS ONE 2015, 10, e0132206. [Google Scholar] [CrossRef]
- Schurer, J.M.; McKenzie, C.; Okemow, C.; Viveros-Guzmán, A.; Beatch, H.; Jenkins, E.J. Who let the dogs out? Communicating First Nations perspectives on a canine veterinary intervention through digital storytelling. Ecohealth 2015, 12, 592–601. [Google Scholar] [CrossRef] [PubMed]
- Smout, F.A.; Skerratt, L.F.; Butler, J.R.; Johnson, C.N.; Congdon, B.C.; Thompson, R.A. The hookworm Ancylostoma ceylanicum: An emerging public health risk in Australian tropical rainforests and Indigenous communities. One Health 2017, 3, 66–69. [Google Scholar] [CrossRef]
- Tsou, C.; Green, C.; Gray, G.; Thompson, S.C. Using the Healthy Community Assessment Tool: Applicability and adaptation in the midwest of Western Australia. Int. J. Environ. Res. Public Health 2018, 15, 1159. [Google Scholar] [CrossRef]
- Beknazarova, M.; Whiley, H.; Traub, R.; Ross, K. Opportunistic mapping of strongyloides stercoralis and hookworm in dogs in remote Australian communities. Pathogens 2020, 9, 398. [Google Scholar] [CrossRef] [PubMed]
- Blaizot, R.; Nabet, C.; Laghoe, L.; Faivre, B.; Escotte-Binet, S.; Djossou, F.; Mosnier, E.; Henaff, F.; Blanchet, D.; Mercier, A. Outbreak of Amazonian Toxoplasmosis: A One Health investigation in a remote Amerindian community. Front. Cell. Infect. Microbiol. 2020, 10, 401. [Google Scholar] [CrossRef] [PubMed]
- Brookes, V.J.; Ward, M.P.; Rock, M.; Degeling, C. One Health promotion and the politics of dog management in remote, Northern Australian communities. Sci. Rep. 2020, 10, 12451. [Google Scholar] [CrossRef] [PubMed]
- Fiorello, C.V.; Straub, M.H.; Schwartz, L.M.; Liu, J.; Campbell, A.; Kownacki, A.K.; Foley, J.E. Multiple-host pathogens in domestic hunting dogs in Nicaragua’s Bosawás Biosphere Reserve. Acta Trop. 2017, 167, 183–190. [Google Scholar] [CrossRef]
- Hampson, K.; Lembo, T.; Bessell, P.; Auty, H.; Packer, C.; Halliday, J.; Beesley, C.A.; Fyumagwa, R.; Hoare, R.; Ernest, E.; et al. Predictability of anthrax infection in the Serengeti, Tanzania. J. Appl. Ecol. 2011, 48, 1333–1344. [Google Scholar] [CrossRef] [PubMed]
- Queenan, K.; Mangesho, P.; Ole-Neselle, M.; Karimuribo, E.; Rweyemamu, M.; Kock, R.; Häsler, B. Using local language syndromic terminology in participatory epidemiology: Lessons for One Health practitioners among the Maasai of Ngorongoro, Tanzania. Prev. Vet. Med. 2017, 139, 42–49. [Google Scholar] [CrossRef]
- Roegner, A.F.; Daniels, M.E.; Smith, W.A.; Gottdenker, N.; Schwartz, L.M.; Liu, J.; Campbell, A.; Fiorello, C.V. Giardia infection and trypanosoma cruzi exposure in dogs in the Bosawás Biosphere Reserve, Nicaragua. Ecohealth 2019, 16, 512–522. [Google Scholar] [CrossRef]
- Davis, M.F.; Rankin, S.C.; Schurer, J.M.; Cole, S.; Conti, L.; Rabinowitz, P.; Gray, G.; Kahn, L.; Machalaba, C.; Mazet, J.J.O.H. Checklist for one health epidemiological reporting of evidence (COHERE). One Health 2017, 4, 14–21. [Google Scholar] [CrossRef]
- Lebov, J.; Grieger, K.; Womack, D.; Zaccaro, D.; Whitehead, N.; Kowalcyk, B.; MacDonald, P. A framework for One Health research. One Health 2017, 3, 44–50. [Google Scholar] [CrossRef]
- Harfield, S.; Pearson, O.; Morey, K.; Kite, E.; Canuto, K.; Glover, K.; Gomersall, J.S.; Carter, D.; Davy, C.; Aromataris, E. Assessing the quality of health research from an Indigenous perspective: The Aboriginal and Torres Strait Islander quality appraisal tool. BMC Med. Res. Methodol. 2020, 20, 79. [Google Scholar] [CrossRef]
- Australian Institute of Aboriginal and Torres Strait Islander Studies. AIATSIS Code of Ethics for Aboriginal and Torres Strait Islander research; Australian Institute of Aboriginal and Torres Strait Islander Studies (AIATSIS): Canberra, Australia, 2020.
- Walter, M.; Suina, M. Indigenous data, indigenous methodologies and indigenous data sovereignty. Int. J. Soc. Res. Methodol. 2019, 22, 233–243. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Domain | Search Terms |
|---|---|
| Indigenous groups | Indigenous OR “First Nations” OR “First People” OR Aboriginal OR “Torres Strait Islander” OR “Native American” OR Inuit OR Maori OR Sami OR “Local tribe” OR “African tribe” OR Amazonian |
| One Health | “One Health” OR “One Welfare” OR Ecohealth OR “Planetary Health” |
| Animals | Animal * |
| Humans | Human * OR People * OR Person |
| Environment | Environment* OR Ecosystem* |
| SOE | One Health Sectors N (%) | Indigenous Viewpoint N (%) | Total Studies N (%) | Corresponding Literature | |||
|---|---|---|---|---|---|---|---|
| Human and Animal | Human and Environment | Human, Animal, and Environment | Yes | No | |||
| High | 2 (33) | 1 (17) | 3 (50) | 6 (100) | 0 (0) | 6 (25) | [36,37,38,39,40,41] |
| Moderate | 4 (36) | 2 (18) | 5 (45) | 10 (91) | 1 (9) | 11 (46) | [13,15,20,42,43,44,45,46,47,48,49] |
| Low | 2 (29) | 0 (0) | 5 (71) | 3 (43) | 4 (57) | 7 (29) | [50,51,52,53,54,55,56] |
| Insufficient | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | 0 (0) | |
| Total | 8 (33) | 3 (13) | 13 (54) | 19 (79) | 5 (21) | 24 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Riley, T.; Anderson, N.E.; Lovett, R.; Meredith, A.; Cumming, B.; Thandrayen, J. One Health in Indigenous Communities: A Critical Review of the Evidence. Int. J. Environ. Res. Public Health 2021, 18, 11303. https://doi.org/10.3390/ijerph182111303
Riley T, Anderson NE, Lovett R, Meredith A, Cumming B, Thandrayen J. One Health in Indigenous Communities: A Critical Review of the Evidence. International Journal of Environmental Research and Public Health. 2021; 18(21):11303. https://doi.org/10.3390/ijerph182111303
Chicago/Turabian StyleRiley, Tamara, Neil E. Anderson, Raymond Lovett, Anna Meredith, Bonny Cumming, and Joanne Thandrayen. 2021. "One Health in Indigenous Communities: A Critical Review of the Evidence" International Journal of Environmental Research and Public Health 18, no. 21: 11303. https://doi.org/10.3390/ijerph182111303
APA StyleRiley, T., Anderson, N. E., Lovett, R., Meredith, A., Cumming, B., & Thandrayen, J. (2021). One Health in Indigenous Communities: A Critical Review of the Evidence. International Journal of Environmental Research and Public Health, 18(21), 11303. https://doi.org/10.3390/ijerph182111303