
Future Challenges for Work-Related Health Promotion in Europe: A Data-Based Theoretical Reflection

{kind=link}
{kind=link}
Abstract
:1. Background and Conditions of Origin of Workplace Health Promotion
2. Health Management as a Response to the Implementation Deficits of Health Promotion
3. Health Promotion in the Area of Conflict between Opposing Claims
4. Current Changes in the World of Work
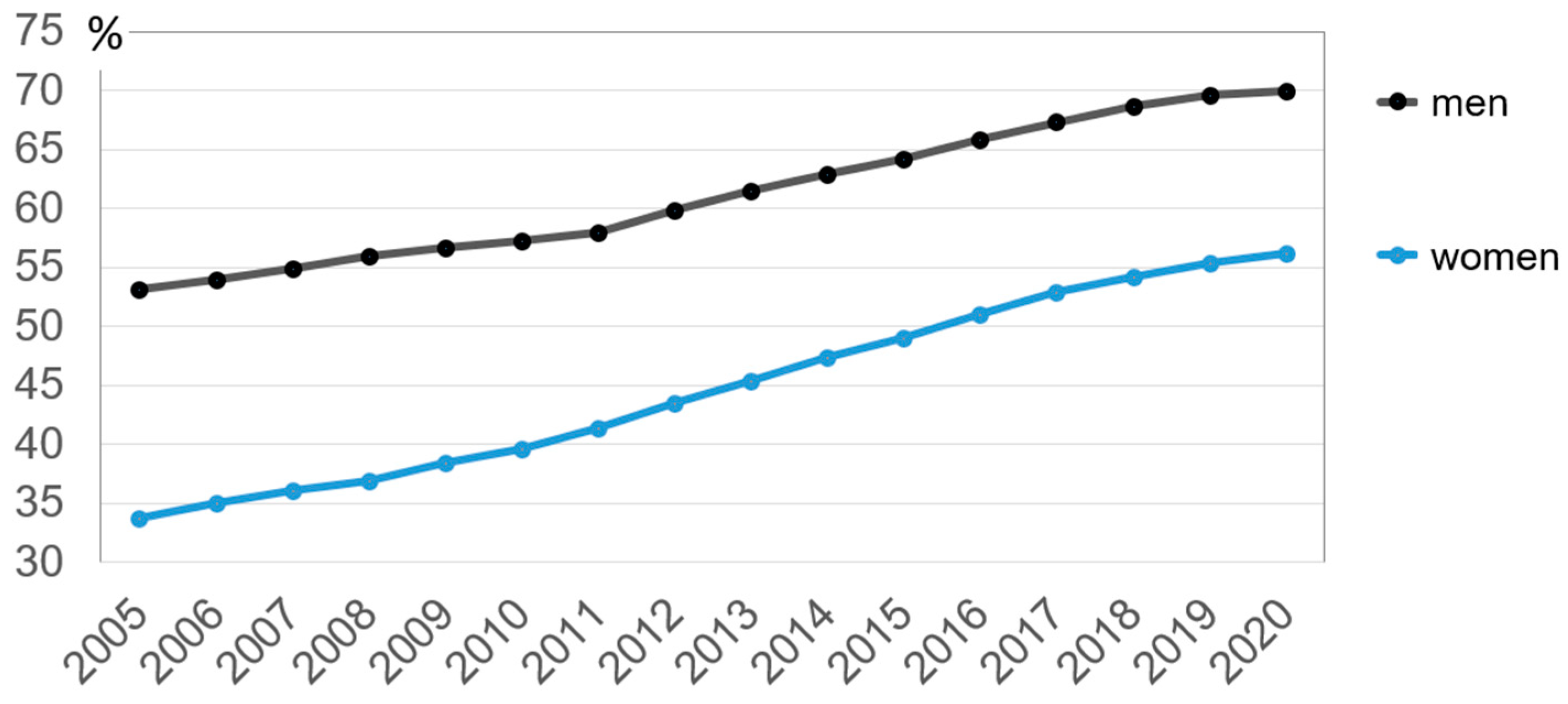
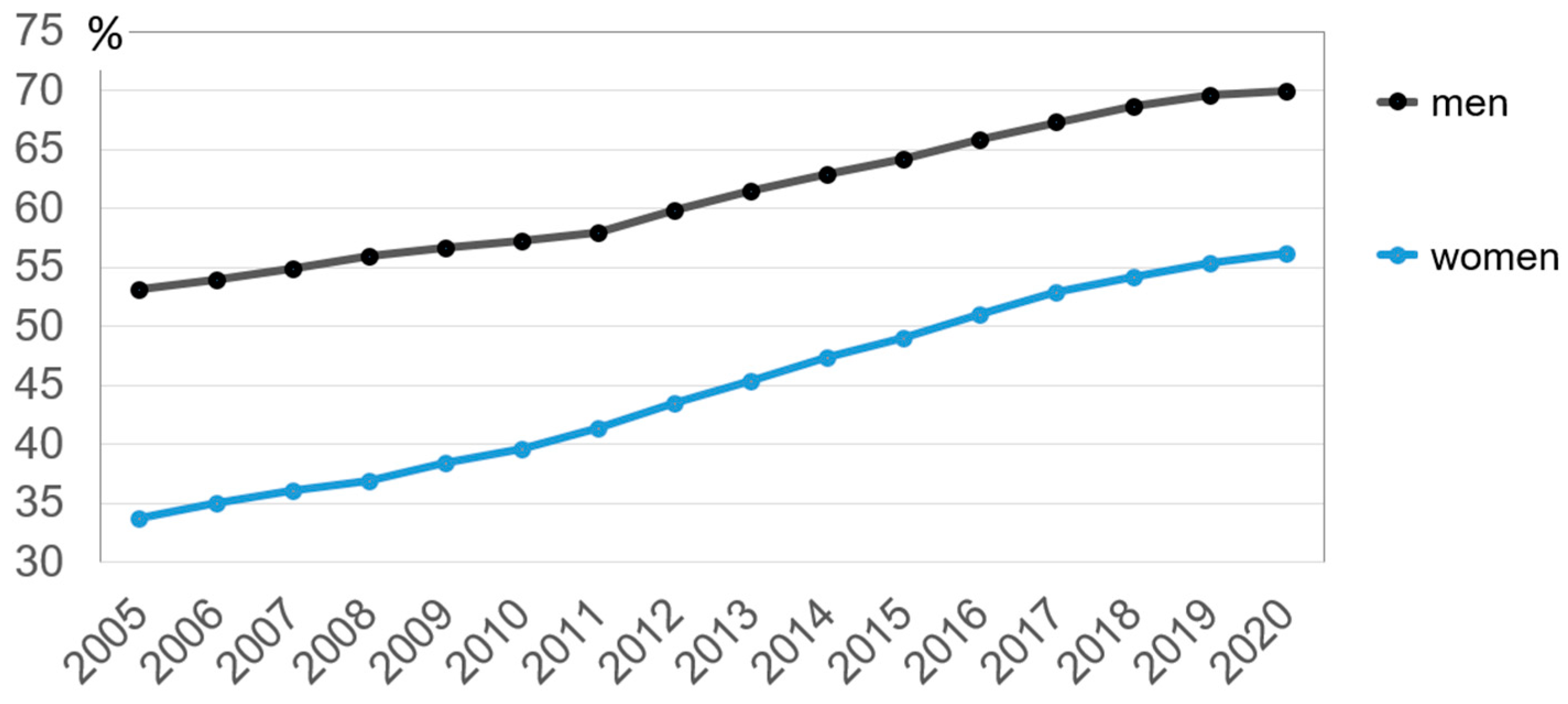
4.1. Demographic Change
4.2. Migration
- fostering an organizational culture characterized by open-mindedness and appreciation of diversity;
- offers to acquire/improve (job-related) language skills;
- the creation and implementation of an induction plan;
- practical day-to-day support;
- the use of mentors;
- the formation of tandems between immigrant and experienced employees to promote informal exchange.
4.3. Digitization, Flexibilization and Subjectivization
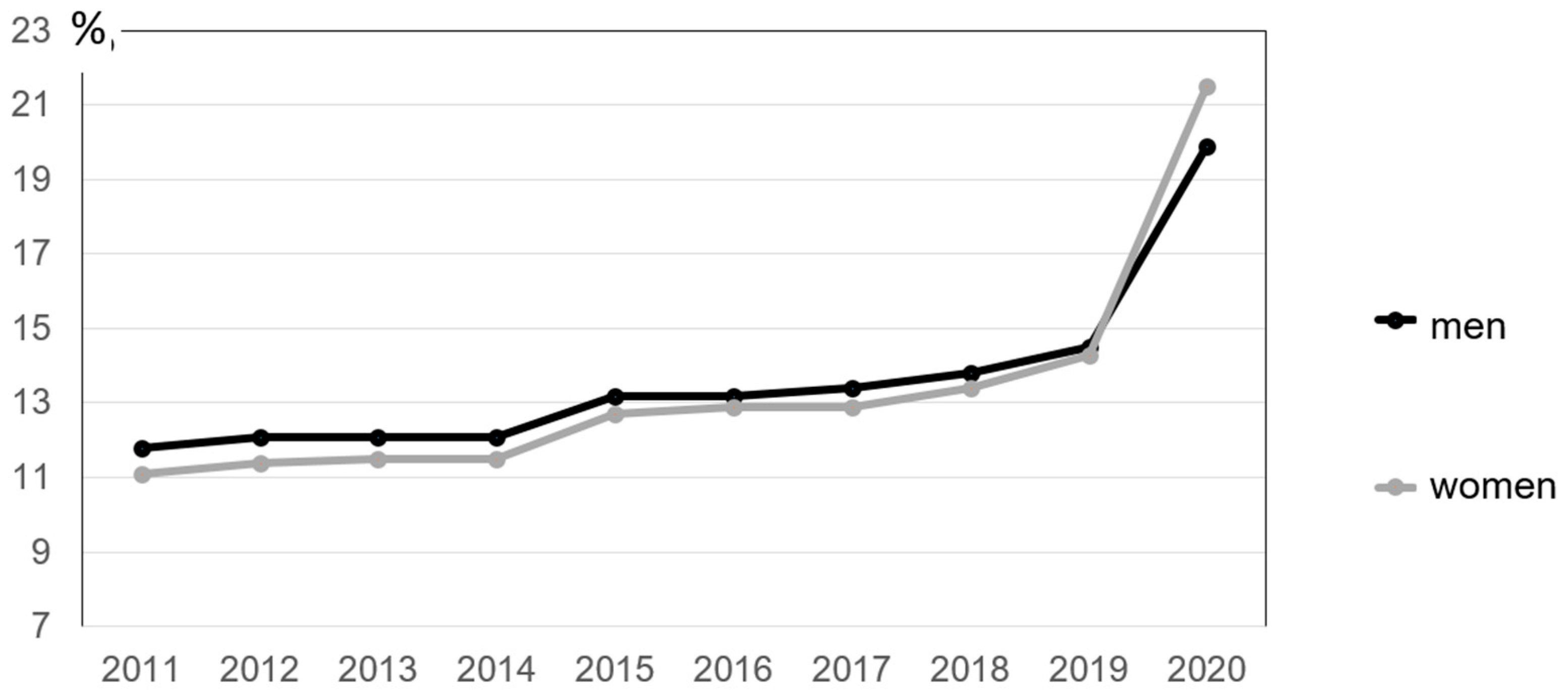
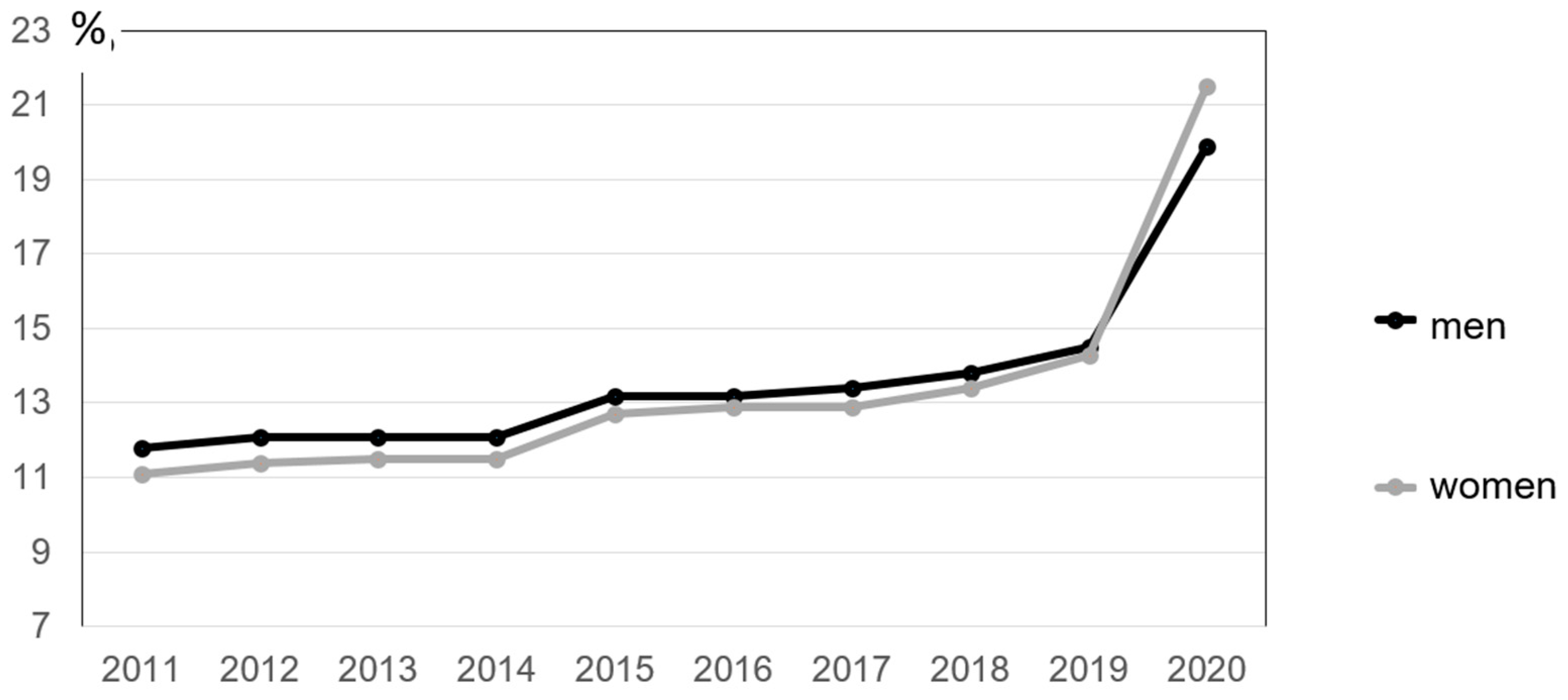
4.4. Work in the “Home Office“
5. Conclusions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- WHO—World Health Organisation. Ottawa Charter for Health Promotion. 1986. Available online: https://www.euro.who.int/de/publications/policy-documents/ottawa-charter-for-health-promotion,-1986 (accessed on 25 August 2021).
- Ashton, J.; Grey, P.; Barnard, K. Healthy Cities. WHO’s New Public Health Initiative. Health Promot. 1986, 1, 319–324. [Google Scholar] [CrossRef]
- Böhme, C.; Stender, K.-P. Gesundheitsförderung und Gesunde‒Soziale Stadt ‒Kommunalpolitische Perspektive (Health Promotion and Healthy-Socially Integrative City-Municipal Policy Perspective); BzgA–Bundeszentrale für Gesundheitliche Aufklärung: Cologne, Germany, 2020. [Google Scholar] [CrossRef]
- Kaba-Schönstein, L. Gesundheitsförderung 2: Entwicklung vor Ottawa 1986. Health Promotion 2: Development before Ottawa 1986; BzgA—Bundeszentrale für Gesundheitliche Aufklärung: Köln, Germany, 2018. [Google Scholar] [CrossRef]
- Dietrich, A.; Hahn, D. Partizipative Strategien zwischen Chancengleichheit, Individualisierung und Verantwortung (Participative strategies between equal opportunities, individualization and responsibility). In Handbuch Partizipation und Gesundheit (Handbook Participation and Health); Hartung, S., Rosenbrock, R., Eds.; Hans Huber: Bern, Switzerland, 2012; pp. 114–126. [Google Scholar]
- Pieper, R. Das Arbeitsschutzrecht in der deutschen und europäischen Arbeits-und Sozialordnung. Grundlagen, Bestandsaufnahme und Bewertung der Reform (Occupational Health and Safety Law in the German and European Labor and Social Order. Fundamentals, Stocktaking and Evaluation of the Reform); Wirtschaftsverlag NW: Bremerhaven, Germany, 1998. [Google Scholar]
- Müller, R. Arbeitsbedingte Gesundheitsgefahren und arbeitsbedingte Erkrankungen als Aufgaben des Arbeitsschutzes (Work-Related Health Hazards and Work-Related Diseases as Occupational Health and Safety Tasks); Wirtschaftsverlag NW: Bremerhaven, Germany, 2001. [Google Scholar]
- Kleinöder, N.; Müller, S.; Uhl, K. Humanisierung der Arbeit: Aufbrüche und Konflikte in der Rationalisierten Arbeitswelt des 20. Jahrhunderts (Humanization of Work: Awakenings and Conflicts in the Rationalized World of Work in the 20th Century); Transcript—Verlag für Kommunikation, Kultur und Soziale Praxis: Bielefeld, Germany, 2019. [Google Scholar]
- Lange, D. Eine neue Art, Autos zu produzieren? Arbeitskämpfe und betriebliche Gewerkschaftsinitiativen bei FIAT-Mirafiori zu Beginn der 1970er Jahre (A new way of producing cars? Labor Struggles and Company Trade Union Initiatives at FIAT-Mirafiori at the Beginning of the 1970 Janre). In Humanisierung der Arbeit: Aufbrüche und Konflikte in der Rationalisierten Arbeitswelt des 20. Jahrhunderts (Humanization of Work: Awakenings and Conflicts in the Rationalized World of Work in the 20th Century); Kleinöder, N., Müller, S., Uhl, K., Eds.; Transcript: Bielefeld, Germany, 2019; pp. 279–304. [Google Scholar]
- Wintersberger, H. Arbeitermedizin in Italien (Workers’ Medicine in Italy); Edition Sigma: Berlin, Germany, 1988. [Google Scholar]
- Isacson, M. Humanization of Work in Scandinavia 1960–1990. In Humanisierung der Arbeit: Aufbrüche und Konflikte in der rationalisierten Arbeitswelt des 20. Jahrhunderts (Humanization of Work. Awakenings and Conflicts in the Rationalized World of Work in the 20th Century); Kleinöder, N., Müller, S., Uhl, K., Eds.; Transcript: Bielefeld, Germany, 2019; pp. 305–327. [Google Scholar]
- Slesina, W. Gesundheitszirkel—Der “Düsseldorfer Ansatz” (Health circles—The “Düsseldorf approach”). In Betriebliche Gesundheitszirkel (Company Health Circles); Westermayer, G., Bähr, B., Eds.; Verlag für Angewandte Psychologie: Göttingen, Germany, 1984; pp. 25–34. [Google Scholar]
- Friczewski, F. Gesundheitszirkel als Organisations-und Personalentwicklung: Der Berliner Ansatz (Health Circles as Organizational and Personnel Development: The Berlin Approach). In Betriebliche Gesundheitszirkel (Company Health Circles); Westermayer, G., Bähr, B., Eds.; Verlag für Angewandte Psychologie: Göttingen, Germany, 1984; pp. 14–24. [Google Scholar]
- Rosenbrock, R. Die Umsetzung der Ottawa Charta in Deutschland: Prävention und Gesundheitsförderung im gesellschaftlichen Umgang mit Gesundheit und Krankheit (The Implementation of the Ottawa Charter in Germany: Prevention and Health Promotion in Society’s Approach to Health and Disease); WZB Discussion Paper, No. P 98-201; Wissenschaftszentrum Berlin für Sozialforschung (WZB): Berlin, Germany, 1998. [Google Scholar]
- WHO—World Health Organisation. Bangkok Charter for Health Promotion in a Globalized World 2005. Available online: https://www.who.int/healthpromotion/conferences/6gchp/hpr_050829_%20BCHP.pdf?ua=1 (accessed on 25 August 2021).
- Lutz, N.; Taeymans, J.; Ballmer, C.; Verhaeghe, N.; Clarys, P.; Deliens, T. Cost-effectiveness and cost-benefit of worksite health promotion programs in Europe: A systematic review. Eur. J. Public Health 2019, 29, 540–546. [Google Scholar] [CrossRef] [PubMed]
- Pelletier, K.R. A Review and Analysis of the Clinical and Cost-Effectiveness Studies of Comprehensive Health Promotion and Disease Management Programs at the Worksite: Update VII 2004–2008. In Database of Abstracts of Reviews of Effects (DARE): Quality-Assessed Reviews; Centre for Reviews and Dissemination (UK): York, UK, 2009. Available online: https://www.ncbi.nlm.nih.gov/books/NBK71763/ (accessed on 25 August 2021).
- Müller, S. Das Forschungs- und Aktionsprogramm Humanisierung des Arbeitslebens (1974–1989) (The Research and Action Program Humanization of Working Life (1974–1989)). In Humanisierung der Arbeit: Aufbrüche und Konflikte in der rationalisierten Arbeitswelt des 20. Jahrhunderts (Humanization of Work: Awakenings and Conflicts in the Rationalized World of Work in the 20th Century); Kleinöder, N., Müller, S., Uhl, K., Eds.; Transcript: Bielefeld, Germany, 2019; pp. 59–88. [Google Scholar]
- Badura, B.; Ritter, W.; Scherf, M. Betriebliches Gesundheits management (Workplace Health Management); Edition Sigma: Berlin, Germany, 1999. [Google Scholar]
- Steinke, M.; Badura, B. Präsentismus: Ein Review zum Stand der Forschung (Presenteeism: A Review of The State of the Research); Bundesanstalt für Arbeitsschutz und Arbeitsmedizin: Dortmund, Germany; Berlin, Germany; Dresden, Germany, 2011. [Google Scholar]
- Faller, G. Was ist eigentlich Betriebliche Gesundheitsförderung (What actually is workplace health promotion)? In Lehrbuch Betriebliche Gesundheitsförderung (Textbook Workplace Health Promotion); Faller, G., Ed.; Hogrefe: Bern, Switzerland, 2017; pp. 25–38. [Google Scholar]
- Petersen, A.; Lupton, D. The New Public Health: Health and Self in the Age of Risk; Sage Publications, Inc.: Thousand Oaks, CA, USA, 1996. [Google Scholar]
- Institute of Medicine. Future of Public Health; Committee for the Study of the Future of Public Health: Washington, DC, USA, 1988. [Google Scholar]
- Wachtler, B.; Rakowitz, N. Public Health in Zeiten von Ökonomisierung und zunehmender sozialer Ungleichheit (Public Health in Times of Economization and Increasing Social Inequality). In Public Health: Sozialwissenschaftliche Gesundheitsforschung; Schmidt-Semisch, H., Schorb, F., Eds.; Springer VS: Wiesbaden, Germany, 2021. [Google Scholar] [CrossRef]
- European Commission. Zukunft der Arbeit gestalten (Shaping the Future of Work) 2021. Available online: https://ec.europa.eu/germany/news/arbeit20190410_de (accessed on 25 August 2021).
- European Commission. Bericht der Kommission an das Europäische Parlament, den Rat, den Europäischen Wirtschafts-Und Sozialausschuss und den Ausschuss der Regionen über die Auswirkungen des Demografischen Wandels (Report from the Commission to the European Parliament, the Council, the European Economic and Social Committee and the Committee of the Regions on the Impact of Demographic Change); European Commission: Brussel, Belgium, 2020. [Google Scholar]
- Hasselhorn, M.; Apt, W. Understanding Employment Participation of Older Workers: Creating a Knowledge Base for Future Labour Market Challenges; Federal Ministry of Labour and Social Affairs/Federal Institute for Occupational Safety and Health: Berlin, Germany; Dortmund, Germany, 2015.
- Cedefop–Europäisches Zentrum für die Förderung der Berufsbildung (European Centre for the Development of Vocational Training). Fachkräftemangel und–Überschuss in Europa: Kurzbericht (Skills Shortages and Surpluses in Europe: Brief Report); November 2016; Cedefop: Thessaloniki, Greece, 2016; Available online: https://www.cedefop.europa.eu (accessed on 25 August 2021).
- Ybema, J.F.; Giesen, F. Older Workers. OSHA-Wiki n.d. Available online: https://oshwiki.eu/wiki/Older_workers (accessed on 25 August 2021).
- Eurostat. Employees and Labor Force by Age and Gender—Annual Data 2021. Available online: https://ec.europa.eu/eurostat/databrowser/view/LFSI_EMP_A__custom_1116266/default/table?lang=de (accessed on 25 August 2021).
- EU-OSHA—European Agency for Safety and Health at Work. Sicherheits-und Gesundheitsschutzmanagement im Kontext Einer Alternden Arbeitnehmerschaft 2021 (Safety and Health Management in the Context of an Aging Workforce 2021). Available online: https://osha.europa.eu/de/themes/osh-management-context-ageing-workforce (accessed on 25 August 2021).
- Van den Berg, T.I.; Elders, L.A.; de Zwart, B.C.; Burdorf, A. The effects of work-related and individual factors on the Work Ability Index: A systematic review. J. Occup. Environ. Med. 2009, 66, 211–220. [Google Scholar]
- Geuskens, G.A.; Oude Hengel, K.M.; Koppes, L.L.J.; Ybema, J.F. Predictors of the willingness and ability to continue working until the age of 65 years. J. Occup. Environ. Med. 2012, 54, 572–578. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rimser, M. Generation Resource Managament; Springer-Gabler: Wiesbaden, Germany, 2014. [Google Scholar]
- Klaffke, M. Generation Diversity—Mehr-Generationen-Belegschaften erfolgreich führen (Generation Diversity—Successfully Managing Multi-generational Workforces). In Diversity Kompetenz (Diversity Competence), 2nd ed.; Genkova, P., Ringeisen, T., Eds.; Springer: Wiesbaden, Germany, 2016. [Google Scholar]
- Geiger, M.; Hanewinkel, V. Politik der Arbeitsmigration: Aktuelle Entwicklungen und Diskurse in Deutschland und Europa. In Räumliche Auswirkungen der Internationalen Migration (Politics of Labor Migration: Current Developments and Discourses in Germany and Europe); Gans, P., Ed.; Akademie für Raumforschung und Landesplanung: Hannover, Germany, 2014; pp. 162–177. [Google Scholar]
- Schmid-Drüner, M. Einwanderungspolitik (Immigration Policy). 2021. Available online: https://www.europarl.europa.eu/factsheets/de/sheet/152/einwanderungspolitik (accessed on 25 August 2021).
- European Commission. Mitteilung der Kommission an das Europäische Parlament, den Rat, den Europäischen Wirtschafts- und Sozialausschuss und den Ausschuss der Regionen: Die Europäische Migrationsagenda 2015 (Communication from the Commission to the European Parliament, the Council, the European Economic and Social Committee and the Committee of the Regions: The European Agenda on Migration 2015). Available online: https://eur-lex.europa.eu/legal-content/DE/TXT/PDF/?uri=CELEX:52015DC0240&from=de (accessed on 25 August 2021).
- Baas, T. Unionsbürgerinnen und -bürger in Deutschland: Eine Übersichtsstudie zu Vorteilen und Herausforderungen bei der Inanspruchnahme der Arbeitnehmerfreizügigkeit 2019. (Union Citizens in Germany: An Overview Study on the Benefits and Challenges of Taking Advantage of the Free Movement of Workers 2019). Available online: https://www.eu-gleichbehandlungsstelle.de/resource/blob/207132/1583340/86fca213057490855bfb1ae1e2b64911/studie-2019-data.pdf (accessed on 25 August 2021).
- Dernbach, A. Europa Braucht auch Ungelernte (Europe also Needs Unskilled Workers), Tagesspiegel. 20 November 2019. Available online: https://www.tagesspiegel.de/wirtschaft/studie-zu-arbeitsmigration-europa-braucht-auch-ungelernte/25246838.html (accessed on 25 August 2021).
- Becker, M. Systematisches Diversity Management (Systematic Diversity Management); Schäffer-Poeschel: Stuttgart, Germany, 2015. [Google Scholar]
- Gundert, S.; Kosyakova, Y.; Fendel, T. Migrantinnen und Migranten am deutschen Arbeitsmarkt: Qualität der Arbeitsplätze als wichtiger Gradmesser einer gelungenen Integration (Migrants in the German Labor Market: Job Quality as an Important Measure of Successful Integration); IAB-Kurzbericht, Institut für Arbeitsmarkt- und Berufsforschung (IAB): Nürnberg, Germany, 2020. [Google Scholar]
- Rothe, I.; Wischniewski, S.; Tegtmeier, S.; Tisch, A. Arbeiten in der digitalen Transformation: Chancen und Risiken für die digitale Arbeitsgestaltung (Working in the digital transformation: Opportunities and risks for digital work design). Z. Für Arb. 2019, 73, 246–251. [Google Scholar]
- Staab, P.; Nachtwey, O. Die Digitalisierung der Dienstleistungsarbeit (The digitization of service work). Polit. Und Zeitgesch. 2016, 66, 25–31. [Google Scholar]
- European Commission. First Phase Consultation of Social Partners Under Article 154 TFEU on Possible Action Addressing the Challenges Related to Working Conditions in Platform Work; Consultation Document; European Commission: Brussel, Belgium, 2021. [Google Scholar]
- Rinne, U.; Zimmermann, K.F. Die digitale Arbeitswelt von heute und morgen (The digital working world of today and tomorrow). Aus Polit. Und Zeitgesch. 2016, 66, 3–9. [Google Scholar]
- Waas, B.; Liebman, W.B.; Lyubarsky, A.; Kezuka, K. Crowdwork—A Comparative Law Perspective; HSI-Schriftenreihe Band 22; Bund-Verlag: Frankfurt, Germany, 2017. [Google Scholar]
- Eurofound—European Foundation for the Improvement of Living and Working Conditions. Atypical Work 2017. Available online: https://www.eurofound.europa.eu/observatories/eurwork/industrial-relations-dictionary/atypical-work (accessed on 25 August 2021).
- Hünefeld, L. Atypische Beschäftigung und psychische Gesundheit (Atypical employment and mental health). Arb. Soz. Umw. 2018, 53, 32–37. [Google Scholar]
- Schulze-Buschoff, K. Atypische Beschäftigung wird normal, Aber haben die Rentensysteme bereits reagiert? Ein Vergleich von sechs europäischen Ländern (Atypical Employment is Becoming Normal, but Have Pension Systems Already Responded? A Comparison of Six European Countries); Friedrich Ebert Stiftung: Berlin, Germany, 2015. [Google Scholar]
- Kyzlinková, R. Industrial Relations and Social Dialogue: Working Life during the COVID-19 Pandemic as Observed through National Research Data; European Foundation for the Improvement of Living and Working Conditions (Eurofound): Dublin, Ireland, 2021. [Google Scholar]
- Rat der Arbeitswelt. Vielfältige Ressourcen Stärken—Zukunft Gestalten (Strengthening Diverse Resources—Shaping the Future); Geschäftsstelle für die Arbeitsweltberichterstattung in Deutschland: Berlin, Germany, 2021. [Google Scholar]
- Seiler, K.; Splittgerber, B. Ein strukturelles Problem? Herausfoderungen der Gesundheitsförderung für prekär Beschäftigte (A structural problem? Challenges of health promotion for precarious employees). In Lehrbuch Betriebliche Gesundheitsförderung (Textbook Workplace Health Promotion); Faller, G., Ed.; Hogrefe: Bern, Switzerland, 2017; pp. 413–424. [Google Scholar]
- Pröll, U.; Ertel, M.; Haake, G. Für alles ständig selbst verantwortlich? Belastungen, Gesundheitsressourcen und Prävention bei selbstständiger Erwerbsarbeit (Responsible for everything all the time? Stresses, Health Resources and Prevention in Self-Employed Gainful Employment). In Lehrbuch Betriebliche Gesundheitsförderung (Textbook Workplace Health Promotion); Faller, G., Ed.; Hogrefe: Bern, Switzerland, 2017; pp. 403–412. [Google Scholar]
- Milasi, S.; González-Vázquez, I.; Fernández-Macías, E. Telework in the EU before and after the COVID-19: Where We Were, Where We Head to; European Commission: Brussels, Belgium, 2020. [Google Scholar]
- Urban, H.-J. Heilsversprechen Homeoffice: Zu den Schattenseiten eines arbeitspolitischen Shootingstars (The promise of a home office: The dark side of a shooting star in labor policy). Blätter Für Dtsch. Und Int. Polit. 2021, 2, 103–113. [Google Scholar]
- Angelucci, M.; Angrisani, M.; Bennett, D.; Kapteyn, A.; Schaner, S. Remote Work and the Heterogeneous Impact of COVID-19 on Employment and Health; IZA Discussion Paper, No. 13620; IZA: Bonn, Germany, 2020. [Google Scholar]
- European Commission. 2021 Report on Gender Equality in the EU; Publications Office of the European Union: Luxembourg, 2021; Available online: https://ec.europa.eu/info/sites/default/files/aid_development_cooperation_fundamental_rights/annual_report_ge_2021_printable_en_0.pdf (accessed on 25 August 2021).
- Eurostat. Employed Persons Working from Home as a Percentage of the Total Employment, by Sex, Age and Professional Status (%) 2021. Available online: https://appsso.eurostat.ec.europa.eu/nui/show.do?dataset=lfsa_ehomp (accessed on 25 August 2021).
- Faller, G. Wearable und App: Was kommt auf uns zu (Wearable and app: What’s in store for us)? Gute Arb. 2020, 32, 25–30. [Google Scholar]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Faller, G. Future Challenges for Work-Related Health Promotion in Europe: A Data-Based Theoretical Reflection. Int. J. Environ. Res. Public Health 2021, 18, 10996. https://doi.org/10.3390/ijerph182010996
Faller G. Future Challenges for Work-Related Health Promotion in Europe: A Data-Based Theoretical Reflection. International Journal of Environmental Research and Public Health. 2021; 18(20):10996. https://doi.org/10.3390/ijerph182010996
Chicago/Turabian StyleFaller, Gudrun. 2021. "Future Challenges for Work-Related Health Promotion in Europe: A Data-Based Theoretical Reflection" International Journal of Environmental Research and Public Health 18, no. 20: 10996. https://doi.org/10.3390/ijerph182010996
APA StyleFaller, G. (2021). Future Challenges for Work-Related Health Promotion in Europe: A Data-Based Theoretical Reflection. International Journal of Environmental Research and Public Health, 18(20), 10996. https://doi.org/10.3390/ijerph182010996