
Social Participation and Survival in Widowed Persons: Results of the Taiwan Longitudinal Study on Aging

 ,
,  , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Data Source
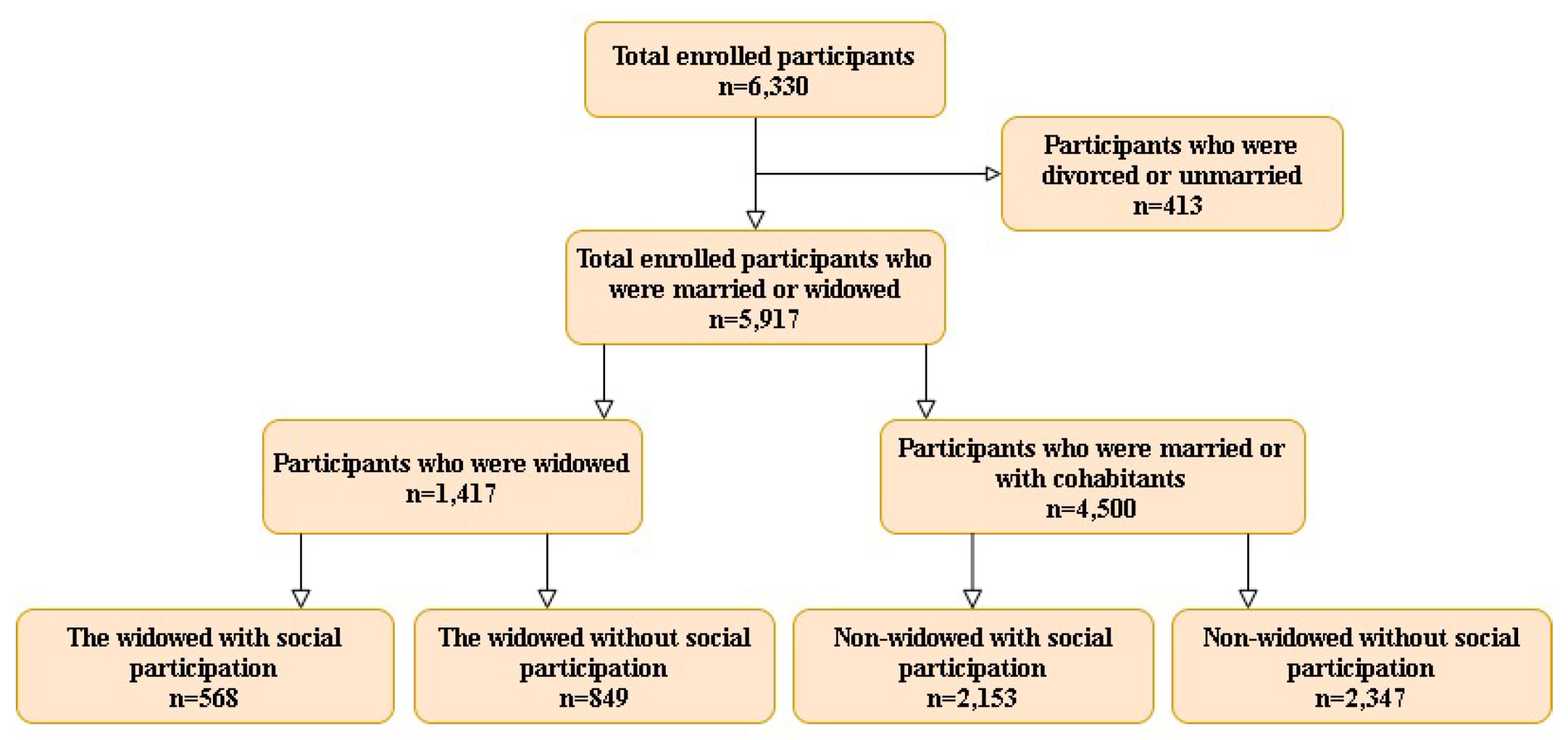
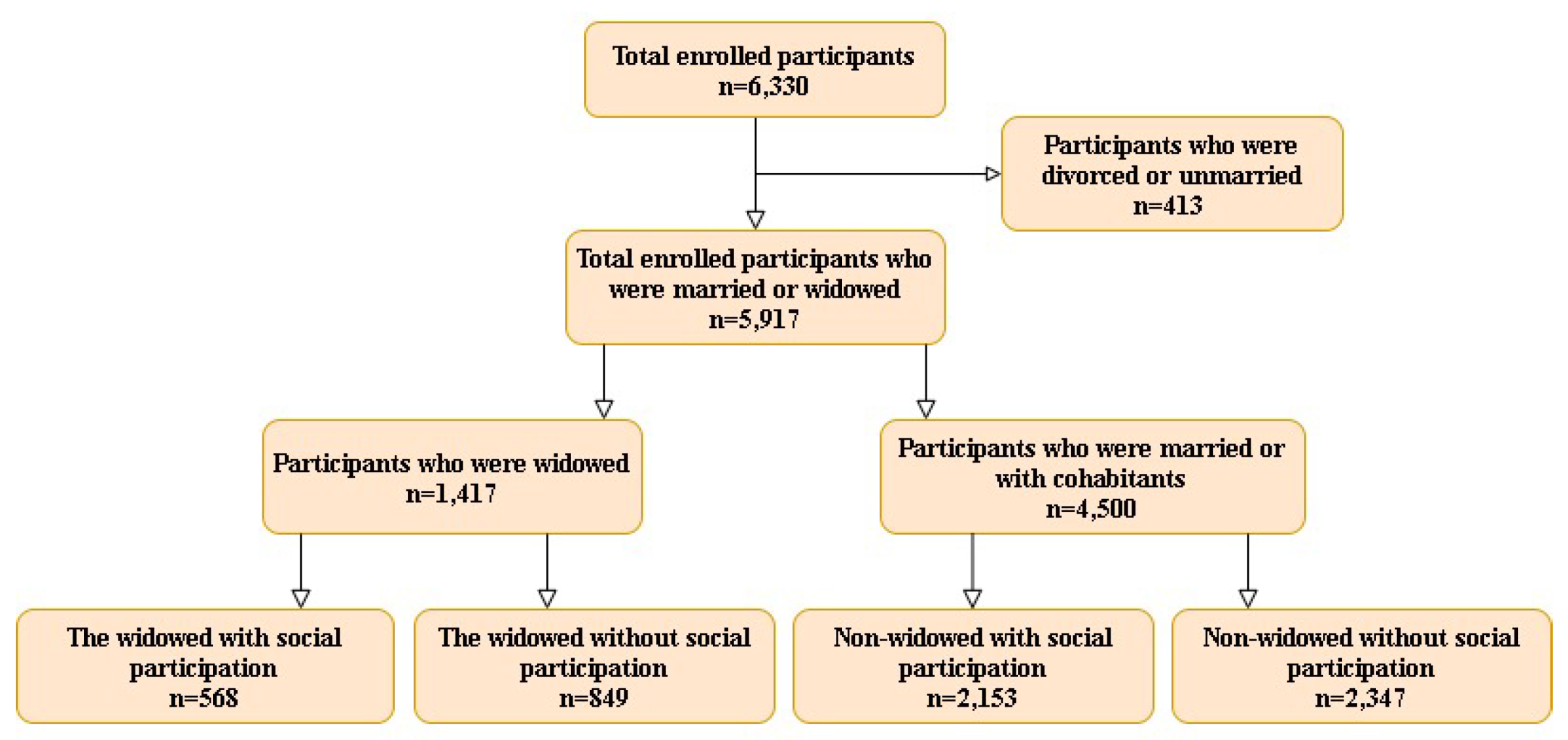
2.2. Study Group Identification, Study Design, and Ethical Approval
2.3. Research Variables
2.3.1. Independent Variable: Social Participation
2.3.2. Dependent Variable: Mortality
2.3.3. Covariates
2.4. Measures
Statistical Methods
3. Results
3.1. Demography
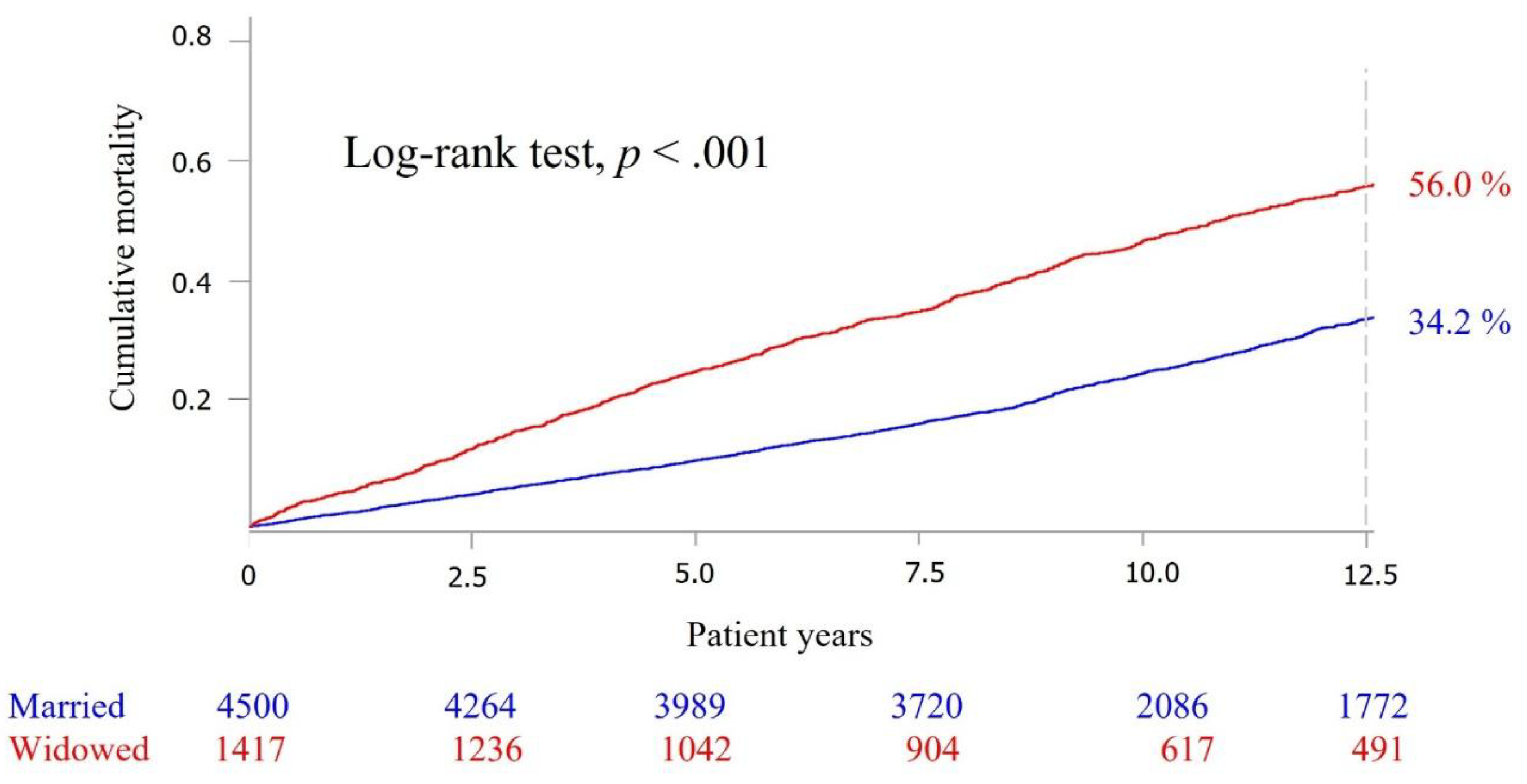
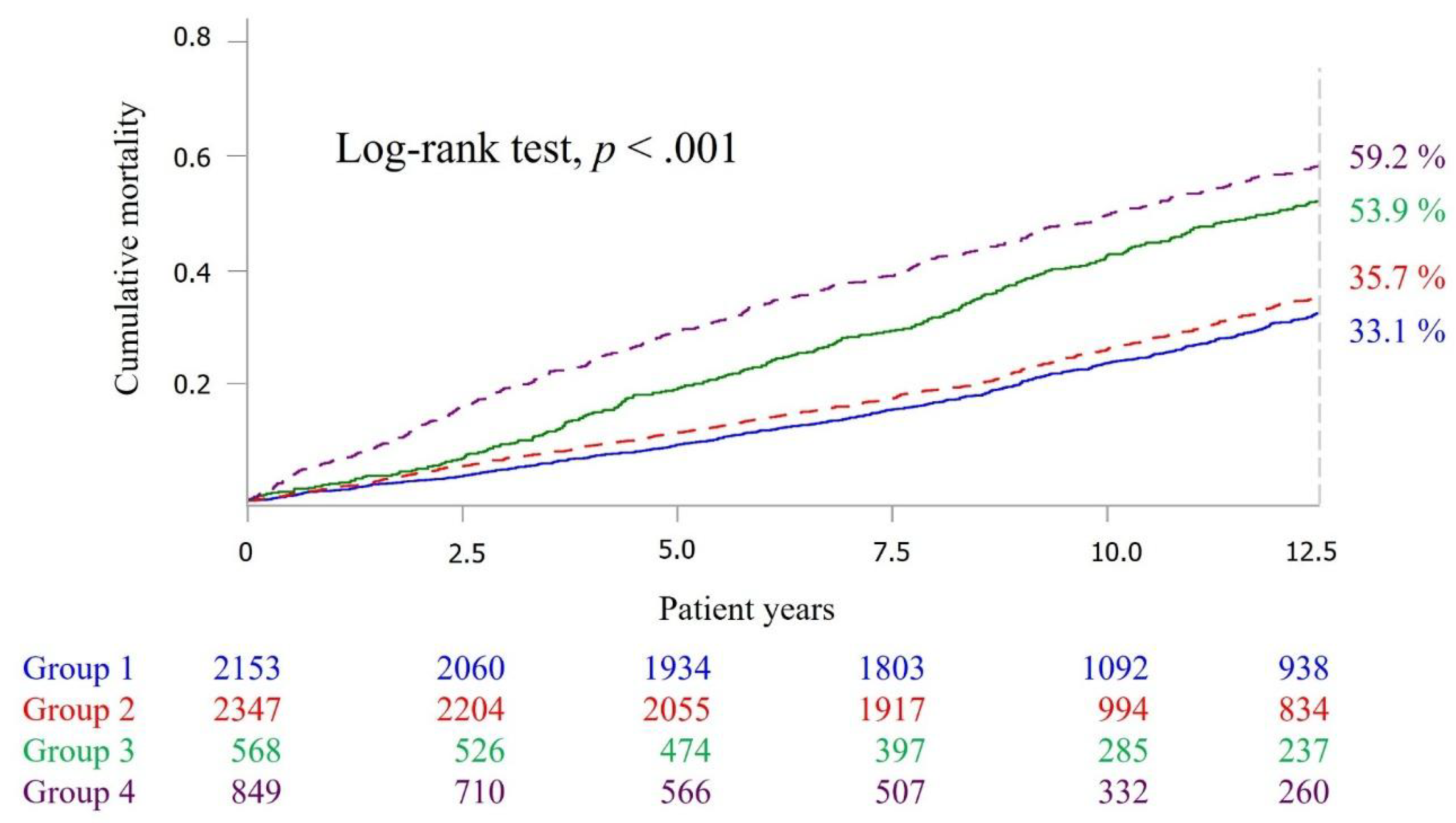
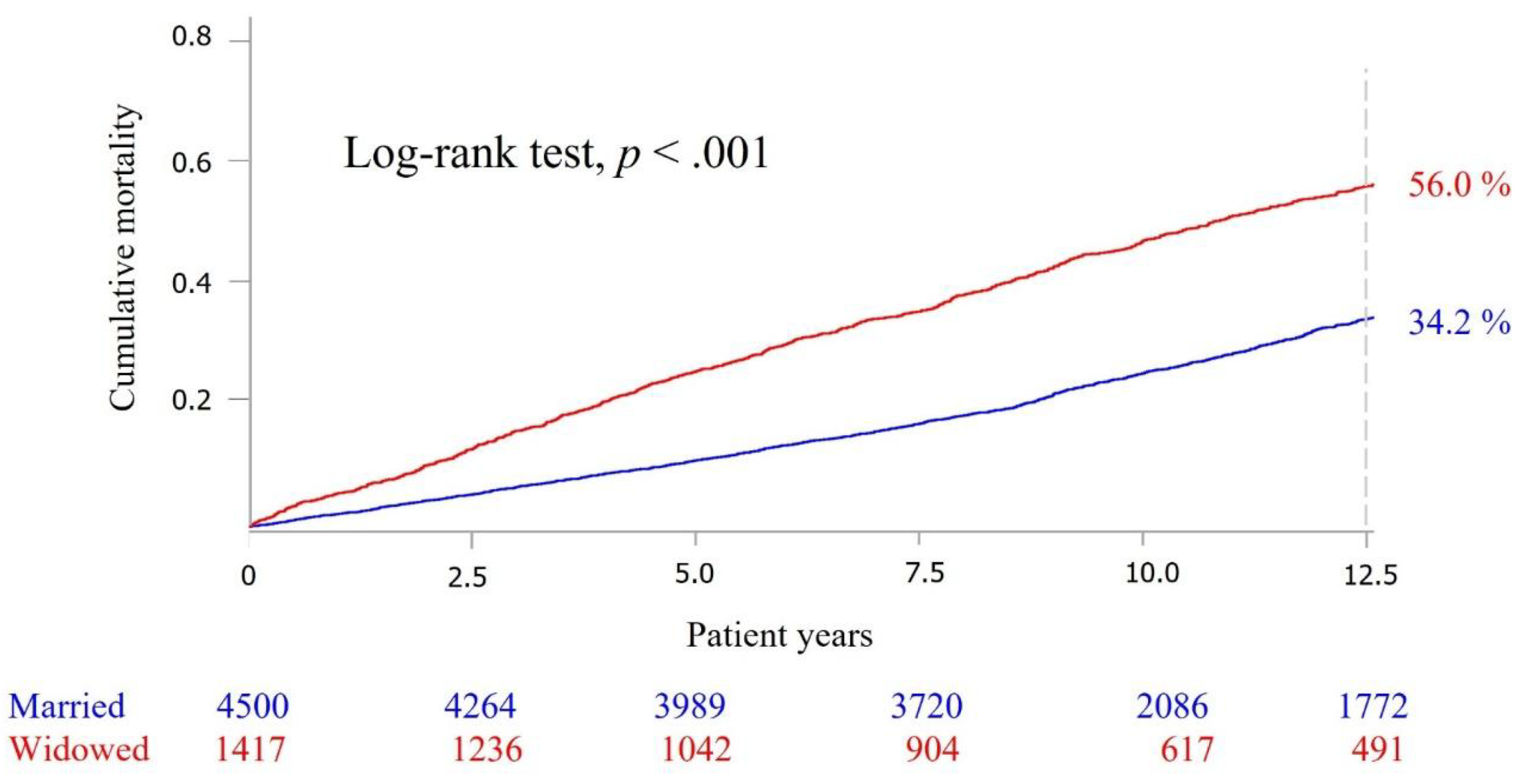
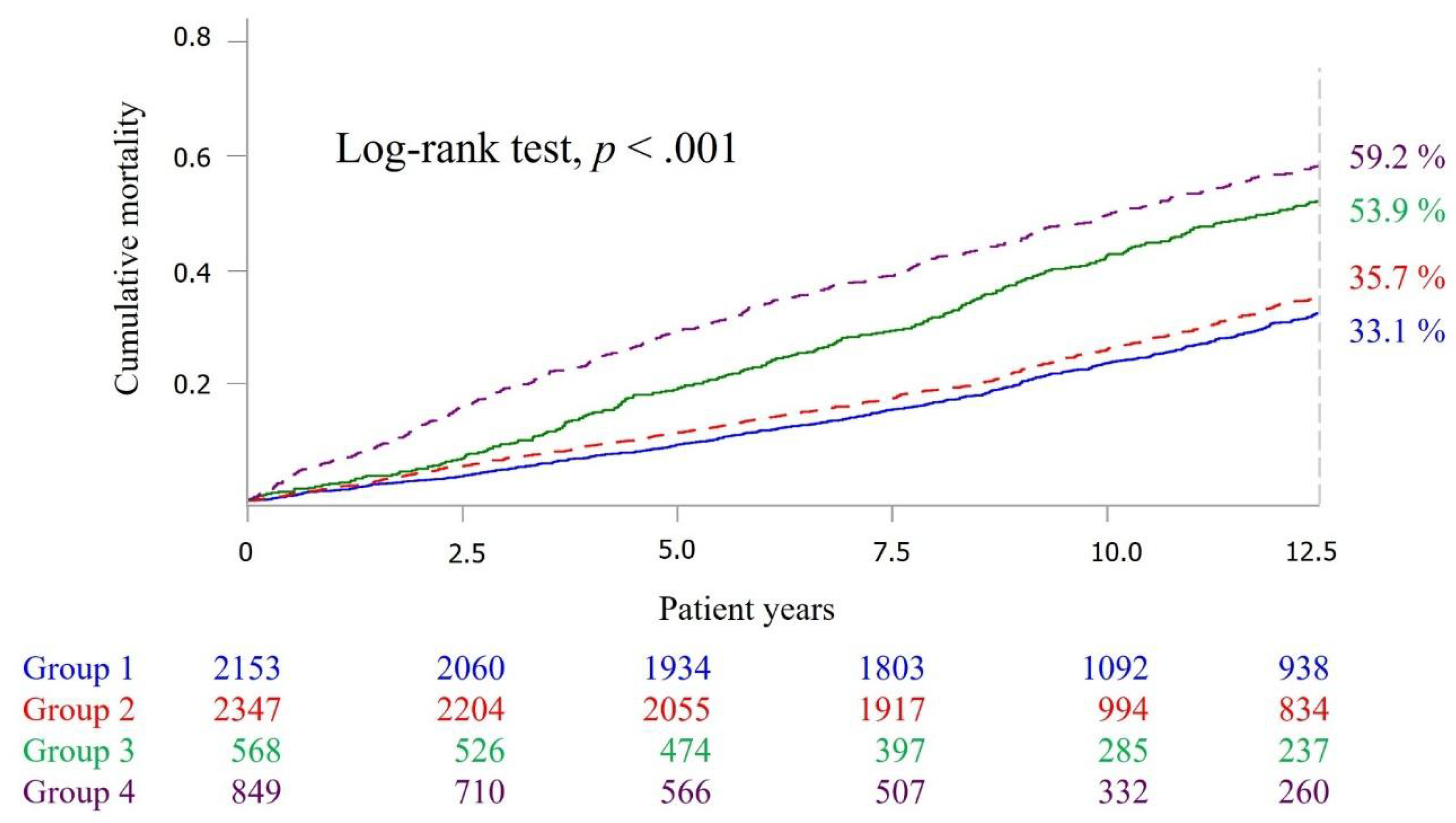
3.2. Mortality
3.3. Matching Analysis in the Widowed
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Jiang, D.; Hou, Y.; Hao, J.; Zhou, J.; Jiang, J.; Wang, Q. Association between personal social capital and loneliness among widowed older people. Int. J. Environ. Res. Public Health 2020, 17, 5799. [Google Scholar] [CrossRef]
- Chamie, J. Widowhood: Stressful and Unprepared. Available online: http://www.ipsnews.net/2020/02/widowhood-stressful-unprepared/ (accessed on 18 June 2021).
- Department of household administration, Taiwan Ministry of Health and Welfare. Available online: https://ws.moi.gov.tw/001/Upload/OldFile/site_stuff/321/2/year/year.html (accessed on 18 June 2021).
- Schaan, B. Widowhood and depression among older Europeans—The role of gender, caregiving, marital quality, and regional context. J. Gerontol. Ser. B 2013, 68, 431–442. [Google Scholar] [CrossRef]
- Hahn, E.A.; Cichy, K.E.; Small, B.J.; Almeida, D.M. Daily emotional and physical reactivity to stressors among widowed and married older adults. J. Gerontol. Ser. B 2013, 69B, 19–28. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wood, N.; McMunn, A.; Webb, E.; Stafford, M. Marriage and physical capability at mid to later life in England and the USA. PLoS ONE 2019, 14, e0209388. [Google Scholar] [CrossRef]
- Subramanian, S.; Elwert, F.; Christakis, N. Widowhood and mortality among the elderly: The modifying role of neighborhood concentration of widowed individuals. Soc. Sci. Med. 2008, 66, 873–884. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chang, W.H.; Tung, H.J. The Effect of social participation on mortality among the elderly in Taiwan: A comparison between the widowed and the non-widowed. Taiwan J. Gerontol. Health Res. 2012, 8, 92–109. [Google Scholar]
- Lund, R.; Holstein, B.E.; Osler, M. Marital history from age 15 to 40 years and subsequent 10-year mortality: A longitudinal study of Danish males born in 1953. Int. J. Epidemiol. 2004, 33, 389–397. [Google Scholar] [CrossRef] [Green Version]
- Brenn, T.; Ytterstad, E. Increased risk of death immediately after losing a spouse: Cause-specific mortality following widowhood in Norway. Prev. Med. 2016, 89, 251–256. [Google Scholar] [CrossRef] [PubMed]
- Elwert, F.; Christakis, N.A. The effect of widowhood on mortality by the causes of death of both spouses. Am. J. Public Health 2008, 98, 2092–2098. [Google Scholar] [CrossRef] [PubMed]
- Morina, N.; Emmelkamp, P.M.G. Health care utilization, somatic and mental health distress, and well-being among widowed and non-widowed female survivors of war. BMC Psychiatry 2012, 12, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Umberson, D.; Wortman, C.B.; Kessler, R.C. Widowhood and depression: Explaining long-term gender differences in vulnerability. J. Health Soc. Behav. 1992, 33, 10–24. [Google Scholar] [CrossRef] [PubMed]
- Jeon, G.-S.; Choi, K.; Cho, S.-I. Impact of living alone on depressive symptoms in older korean widows. Int. J. Environ. Res. Public Health 2017, 14, 1191. [Google Scholar] [CrossRef] [Green Version]
- Ho, S.-H.; Hung, W.-S. The Impacts of widowhood, chronic disease, and physical function on mortality among older people. J. Nurs. Res. 2013, 21, 110–119. [Google Scholar] [CrossRef]
- Aroogh, M.D.; Shahboulaghi, F.M. Social participation of older adults: A concept analysis. Int. J. Community Based Nurs. Midwifery 2020, 8, 55–72. [Google Scholar]
- Schormans, A.F. Social participation. In Encyclopedia of Quality of Life and Well-Being Research; Michalos, A.C., Ed.; Springer: Dordrecht, The Netherlands, 2014; pp. 6135–6140. [Google Scholar]
- Carr, D.C.; Kail, B.L.; Matz-Costa, C.; Shavit, Y.Z. Does becoming a volunteer attenuate loneliness among recently widowed older adults? J. Gerontol. B Psychol. Sci. Soc. Sci. 2018, 73, 501–510. [Google Scholar] [CrossRef] [PubMed]
- Donnelly, E.A.; Hinterlong, J.E. Changes in social participation and volunteer activity among recently widowed older adults. Gerontol. 2009, 50, 158–169. [Google Scholar] [CrossRef] [Green Version]
- Xiang, N.; Liu, E.; Li, H.; Qin, X.; Liang, H.; Yue, Z. The association between widowhood and cognitive function among chinese elderly people: Do gender and widowhood duration make a difference? Healthcare 2021, 9, 991. [Google Scholar] [CrossRef] [PubMed]
- Di Giacomo, M.; Davidson, P.M.; Byles, J.; Nolan, M.T. An integrative and socio-cultural perspective of health, wealth, and adjustment in widowhood. Health Care Women Int. 2013, 34, 1067–1083. [Google Scholar] [CrossRef] [Green Version]
- Onrust, S.A.; Cuijpers, P. Mood and anxiety disorders in widowhood: A systematic review. Aging Ment. Health 2006, 10, 327–334. [Google Scholar] [CrossRef]
- Planning, T.P. 1989 Survey of Health and Living Status of the Elderly in Taiwan: Questionnaire and Survey Design; Population Studies Center and Institute of Gerontology; University of Michigan: Ann Arbor, MI, USA, 1989. [Google Scholar]
- Liang, J.; Wang, C.-N.; Xu, X.; Hsu, H.-C.; Lin, H.-S.; Lin, Y.-H. Trajectory of functional status among older Taiwanese: Gender and age variations. Soc. Sci. Med. 2010, 71, 1208–1217. [Google Scholar] [CrossRef] [Green Version]
- Hsu, H.-C.; Chang, W.-C. Social connections and happiness among the elder population of Taiwan. Aging Ment. Health 2015, 19, 1–7. [Google Scholar] [CrossRef]
- Katz, S.; Ford, A.B.; Moskowitz, R.W.; Jackson, B.A.; Jaffe, M.W. Studies of illness in the aged. The index of adl: A standardized measure of biological and psychosocial function. JAMA 1963, 185, 914–919. [Google Scholar] [CrossRef]
- Hsu, H.-C.; Chang, W.-C. Trajectories of frailty and related factors of the older people in Taiwan. Exp. Aging Res. 2014, 41, 104–114. [Google Scholar] [CrossRef]
- Pfeiffer, E. A Short portable mental status questionnaire for the assessment of organic brain deficit in elderly patients. J. Am. Geriatr. Soc. 1975, 23, 433–441. [Google Scholar] [CrossRef]
- Chiu, C.-J.; Hu, S.C.; Wray, L.A.; Wu, S.-T. The short- and long-term effects of psychobehavioral correlates in buffering diabetes-related cognitive decline. Ann. Behav. Med. 2016, 50, 436–444. [Google Scholar] [CrossRef]
- Yen, C.-H.; Yeh, C.-J.; Wang, C.-C.; Liao, W.-C.; Chen, S.-C.; Chen, C.-C.; Liang, J.; Lai, T.-J.; Lin, H.-S.; Lee, S.-H.; et al. Determinants of cognitive impairment over time among the elderly in Taiwan: Results of the national longitudinal study. Arch. Gerontol. Geriatr. 2010, 50, S53–S57. [Google Scholar] [CrossRef]
- Hsu, H.-C.; Chang, W.-C. Reducing the risks of morbidity, disability, and mortality using successful aging strategies. J. Am. Geriatr. Soc. 2015, 63, 2426–2428. [Google Scholar] [CrossRef] [PubMed]
- Christensen, E. Multivariate survival analysis using Cox’s regression model. Hepatology 1987, 7, 1346–1358. [Google Scholar] [CrossRef] [PubMed]
- Bowling, A. Predictors of mortality among a national sample of elderly widowed people: Analysis of 28-year mortality rates. Age Ageing 2009, 38, 527–530. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, G.R.; DeMaris, A.; Bavin, S.; Sullivan, R. Gender differences in the depressive effect of widowhood in later life. J. Gerontol. Ser. B 2001, 56, S56–S61. [Google Scholar] [CrossRef] [PubMed]
- Liao, C.-C.; Li, C.-R.; Lee, S.-H.; Liao, W.-C.; Liao, M.-Y.; Lin, J.; Yeh, C.-J.; Lee, M.-C. Social support and mortality among the aged people with major diseases or ADL disabilities in Taiwan: A national study. Arch. Gerontol. Geriatr. 2015, 60, 317–321. [Google Scholar] [CrossRef]
- Guillén, L.; Coromina, L.; Saris, W.E. Measurement of social participation and its place in social capital theory. Soc. Indic. Res. 2010, 100, 331–350. [Google Scholar] [CrossRef]
- Nakagomi, A.; Shiba, K.; Kondo, K.; Kawachi, I. Can social capital moderate the impact of widowhood on depressive symptoms? A fixed-effects longitudinal analysis. Aging Ment. Health 2020, 25, 1811–1820. [Google Scholar] [CrossRef] [PubMed]
- Cai, S. Does social participation improve cognitive abilities of the elderly? J. Popul. Econ. 2021, 34, 1–29. [Google Scholar]
- Sorensen, L.V.; Waldorff, F.B.; Waldemara, G. Social participation in home-living patients with mild Alzheimer’s disease. Arch. Gerontol. Geriatr. 2008, 47, 291–301. [Google Scholar] [CrossRef] [PubMed]
- Ponce, M.S.H.; Rosas, R.P.E.; Lorca, M.B.F. Social capital, social participation and life satisfaction among Chilean older adults. Rev. de Saude Publica 2014, 48, 739–749. [Google Scholar] [CrossRef] [PubMed]
- Gilmour, H. Social participation and the health and well-being of Canadian seniors. Health Rep. 2012, 23, 23–32. [Google Scholar]
- Hosokawa, R.; Kondo, K.; Ito, M.; Miyaguni, Y.; Mizutani, S.; Goto, F.; Abe, Y.; Tsuge, Y.; Handa, Y.; Ojima, T. The effectiveness of Japan’s community centers in facilitating social participation and maintaining the functional capacity of older people. Res. Aging 2019, 41, 315–335. [Google Scholar] [CrossRef]
- The Ministry of Health and Welfare. Project Report of Long-term Care 2.0 Implementation Status and Review; Ministry of Health and Welfare: Taipei, Taiwan, 2020. [Google Scholar]
- Chu, W.; Ho, H.; Yeh, C.; Tsan, Y.; Lee, S.; Lee, M. Late-career unemployment and risk of frailty among older adults in Taiwan: An 8-year population-based cohort study. Geriatr. Gerontol. Int. 2021, 21, 353–358. [Google Scholar] [CrossRef]
- Gottlieb, B.H. Social networks and social support: An overview of research, practice, and policy implications. Health Educ. Q. 1985, 12, 5–22. [Google Scholar] [CrossRef]
- Glick, P.C.; Miller, H.P. Educational level and potential income. Am. Sociol. Rev. 1956, 21, 307–312. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Widowed n = 1417 | Nonwidowed n = 4500 | p Value | |||
|---|---|---|---|---|---|
| N | % | N | % | ||
| Age, years | 69.5 ± 10.7 | 60.3 ± 8.0 | <0.001 † | ||
| Male | 382 | 27.0 | 2640 | 58.7 | <0.001 * |
| Social participation | <0.001 * | ||||
| No | 849 | 60.0% | 2347 | 52.2% | |
| Yes | 568 | 40.0% | 2153 | 47.8% | |
| Age group | <0.001 * | ||||
| 50 ≤ age < 65 | 933 | 65.8 | 3642 | 80.9 | |
| 65 ≤ age < 70 | 116 | 8.2 | 455 | 10.1 | |
| 70 ≤ age < 75 | 90 | 6.4 | 180 | 4.0 | |
| Age ≥ 75 | 278 | 19.6 | 223 | 5.0 | |
| Education level | <0.001 * | ||||
| Illiterate | 635 | 44.8 | 847 | 18.8 | |
| Elementary school | 596 | 42.0 | 2130 | 47.3 | |
| Junior high school | 90 | 6.4 | 555 | 12.3 | |
| Senior high school | 66 | 4.7 | 521 | 11.6 | |
| College or above | 30 | 2.1 | 447 | 9.9 | |
| Urbanization of residence | <0.001 * | ||||
| Nonrural areas and offshore islands | 1355 | 95.6 | 4375 | 97.2 | |
| Rural areas and offshore islands | 62 | 4.4 | 125 | 2.8 | |
| Self-rated health | <0.001 * | ||||
| Good or very good | 377 | 26.6 | 1997 | 44.4 | |
| Okay | 467 | 33.0 | 1418 | 31.5 | |
| Bad or very bad | 573 | 40.4 | 1085 | 24.1 | |
| Self-reported economic pressure | <0.001 * | ||||
| No | 822 | 58.0 | 2736 | 60.8 | |
| Mild | 437 | 30.8 | 1582 | 35.1 | |
| Severe | 158 | 11.2 | 182 | 4.1 | |
| Healthy and unhealthy behaviors | |||||
| Exercise | 724 | 51.1 | 2499 | 55.5 | <0.001 * |
| Smoking | 203 | 14.3 | 1195 | 26.6 | <0.001 * |
| Alcohol | 216 | 15.2 | 1416 | 31.5 | <0.001 * |
| Comorbidities | |||||
| Hypertension | 519 | 36.6 | 1283 | 28.5 | <0.001 * |
| Diabetes mellitus | 214 | 15.1 | 550 | 12.2 | <0.001 * |
| Heart diseases | 318 | 22.4 | 584 | 13.0 | <0.001 * |
| Stroke | 112 | 7.9 | 193 | 4.3 | <0.001 * |
| Cancer | 46 | 3.3 | 122 | 2.7 | <0.001 * |
| Bronchitis | 186 | 13.1 | 465 | 10.3 | <0.001 * |
| Physical and psychological function tests a | |||||
| ADL disability | 223 | 15.7 | 227 | 5.0 | <0.001 * |
| Cognitive impairment by SPMSQ | 201 | 14.2 | 304 | 6.8 | <0.001 * |
| Depression by CES-D | 478 | 33.7 | 731 | 16.2 | <0.001 * |
| Mortality | HR | 95% CI | p Value | p for Trend | |
|---|---|---|---|---|---|
| Group 1 | 651 (30.2%) | 1.00 | - | - | p < 0.001 * |
| Group 2 | 740 (31.5%) | 1.11 | 0.99–1.23 | 0.05 | |
| Group 3 | 307 (54.1%) | 1.92 | 1.67–2.20 | <0.001 * | |
| Group 4 | 491 (57.8%) | 2.35 | 2.09–2.64 | <0.001 * |
| Widowed with Social Participation n = 529 | Widowed without Social Participation n = 529 | p Value | |||
|---|---|---|---|---|---|
| N | % | N | % | ||
| Age, years | 68.4 ± 10.0 | 68.0 ± 11.2 | 0.649 | ||
| Male | 157 | 29.7% | 157 | 29.7% | 1.000 |
| Age group | 1.000 | ||||
| 50 ≤ age <65 | 368 | 69.6% | 368 | 69.6% | |
| 65 ≤ age <70 | 50 | 9.5% | 50 | 9.5% | |
| 70 ≤ age <75 | 34 | 6.4% | 34 | 6.4% | |
| Age ≥ 75 | 77 | 14.6% | 77 | 14.6% | |
| Education level | 0.648 | ||||
| Illiterate | 222 | 42.0% | 227 | 42.9% | |
| Elementary school | 221 | 41.8% | 232 | 43.9% | |
| Junior high school | 38 | 7.2% | 35 | 6.6% | |
| Senior high school | 33 | 6.2% | 24 | 4.5% | |
| College or above | 15 | 2.8% | 11 | 2.1% | |
| Urbanization of residence | 0.466 | ||||
| Nonrural areas and offshore islands | 502 | 94.9% | 507 | 95.8% | |
| Rural areas and offshore islands | 27 | 5.1% | 22 | 4.2% | |
| Self-rated health | 0.043 * | ||||
| Good or very good | 156 | 29.5% | 130 | 24.6% | |
| Okay | 189 | 35.7% | 177 | 33.5% | |
| Bad or very bad | 184 | 34.8% | 222 | 42.0% | |
| Self-reported economic pressure | <0.001 * | ||||
| No | 357 | 67.6% | 281 | 53.1% | |
| Mild | 148 | 28.0% | 169 | 32.0% | |
| Severe | 24 | 4.5% | 79 | 14.9% | |
| Healthy and unhealthy behaviors | |||||
| Exercise | 318 | 60.1% | 244 | 46.2% | <0.001 * |
| Smoking | 80 | 15.1% | 87 | 16.5% | 0.555 |
| Alcohol | 83 | 15.7% | 86 | 16.3% | 0.791 |
| Comorbidities | |||||
| Hypertension | 185 | 35.0% | 195 | 36.5% | 0.506 |
| Diabetes mellitus | 68 | 12.9% | 75 | 14.2% | 0.529 |
| Heart diseases | 131 | 24.8% | 106 | 20.0% | 0.070 |
| Stroke | 27 | 5.1% | 47 | 8.9% | 0.016 * |
| Cancer | 11 | 2.1% | 21 | 4.0% | 0.073 |
| Bronchitis | 81 | 15.3% | 64 | 12.1% | 0.132 |
| Physical and psychological function tests a | |||||
| ADL disability | 45 | 8.5% | 97 | 18.3% | <0.001 * |
| Cognitive impairment by SPMSQ | 64 | 12.1% | 67 | 12.7% | 0.298 |
| Depression by CES-D | 153 | 30.5% | 185 | 41.6% | 0.035 * |
| Mortality N (%) | Adjusted HR # | 95% CI | p-Value | |
|---|---|---|---|---|
| Widowed without social participation (n = 529) | 295 (55.6%) | 1.00 | - | - |
| Widowed with social participation (n = 529) | 286 (54.1%) | 0.83 | 0.71–0.98 | 0.04 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hsiao, Y.-H.; Lee, M.-C.; Yeh, C.-J.; Tai, C.-J.; Lee, S.-S. Social Participation and Survival in Widowed Persons: Results of the Taiwan Longitudinal Study on Aging. Int. J. Environ. Res. Public Health 2021, 18, 10974. https://doi.org/10.3390/ijerph182010974
Hsiao Y-H, Lee M-C, Yeh C-J, Tai C-J, Lee S-S. Social Participation and Survival in Widowed Persons: Results of the Taiwan Longitudinal Study on Aging. International Journal of Environmental Research and Public Health. 2021; 18(20):10974. https://doi.org/10.3390/ijerph182010974
Chicago/Turabian StyleHsiao, Yu-Han, Meng-Chih Lee, Chih-Jung Yeh, Chi-Jung Tai, and Shiuan-Shinn Lee. 2021. "Social Participation and Survival in Widowed Persons: Results of the Taiwan Longitudinal Study on Aging" International Journal of Environmental Research and Public Health 18, no. 20: 10974. https://doi.org/10.3390/ijerph182010974
APA StyleHsiao, Y.-H., Lee, M.-C., Yeh, C.-J., Tai, C.-J., & Lee, S.-S. (2021). Social Participation and Survival in Widowed Persons: Results of the Taiwan Longitudinal Study on Aging. International Journal of Environmental Research and Public Health, 18(20), 10974. https://doi.org/10.3390/ijerph182010974