
Medical, Health and Wellness Tourism Research—A Review of the Literature (1970–2020) and Research Agenda

 ,
, 
 and
and
Abstract
1. Introduction
2. Scholarly Reviews and Meta-Analyses of Medical, Health and Wellness Tourism
3. Methods
3.1. Data Collection
3.2. Data Analysis
4. Results
4.1. Overview of Articles Published
4.2. Source Journals
4.3. Author Productivity and Authorship Analysis
4.4. Author Regions and Affiliations
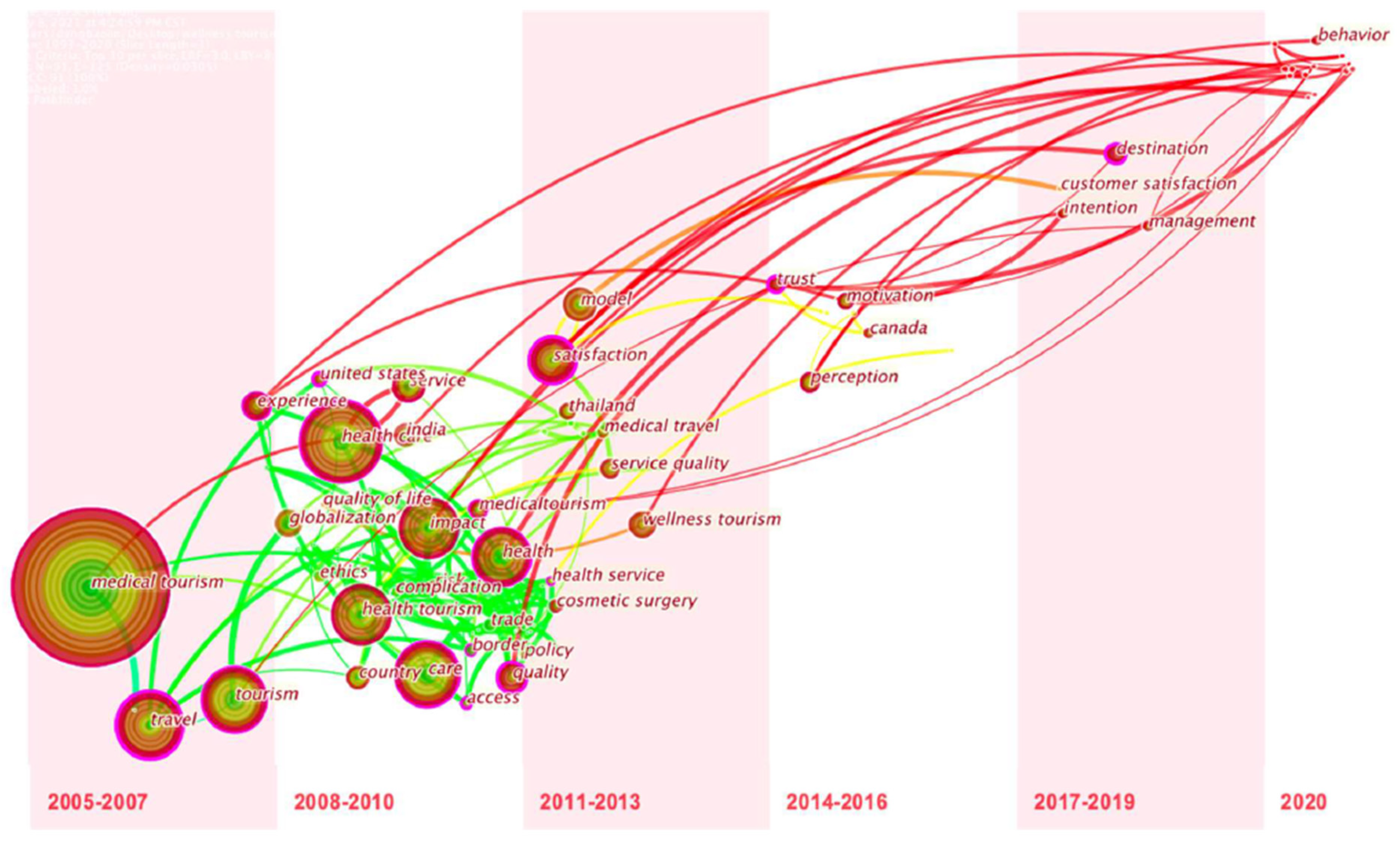
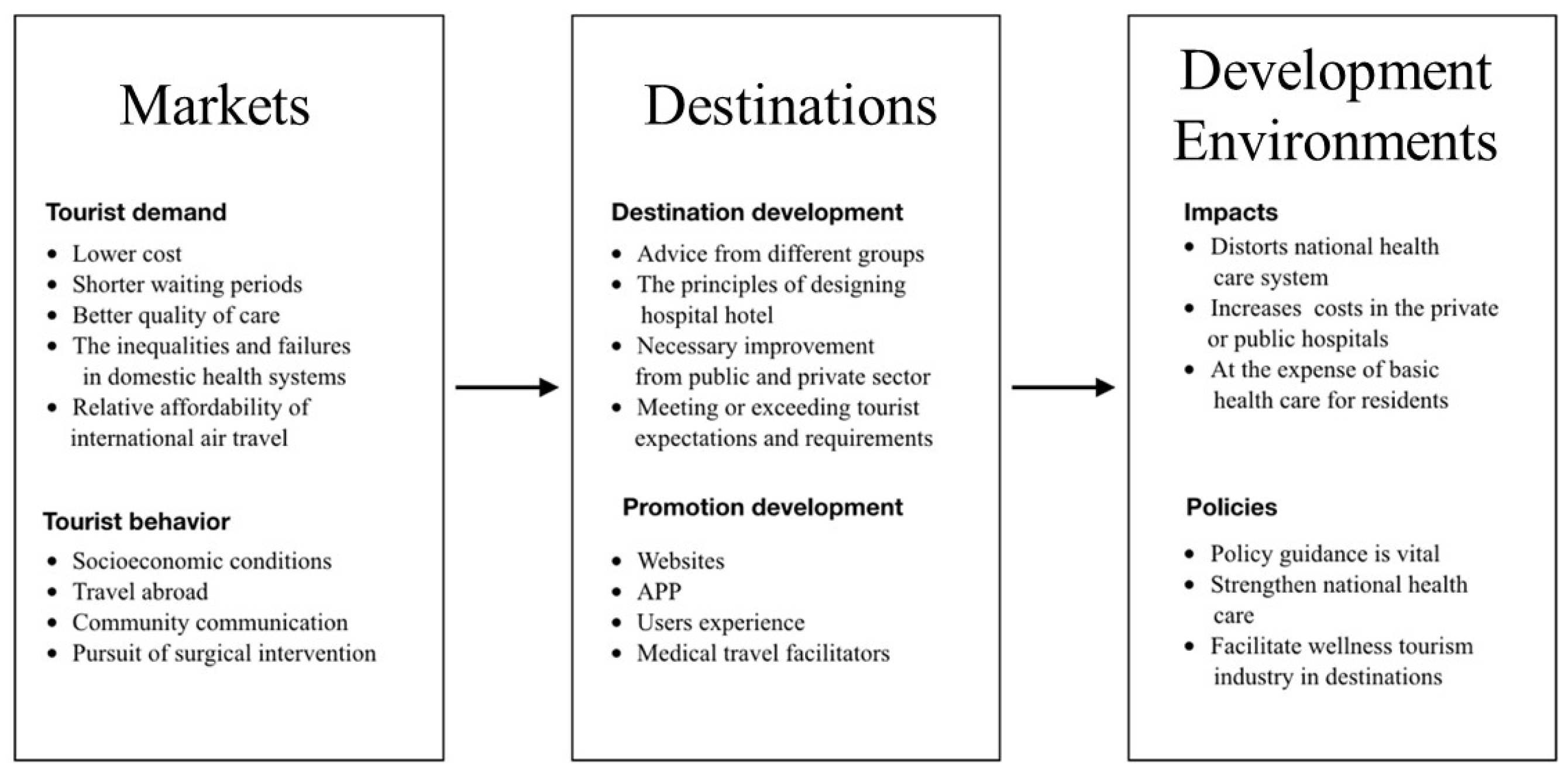
4.5. Thematic Analysis of Research
4.6. Markets: Demand and Behavior
4.7. Destinations: Development and Promotion
4.8. Development Environments: Policies and Impacts
5. Discussion and Conclusions
5.1. Generation Discussion
5.2. Future Research Trends
5.2.1. Industrial Perspective
5.2.2. Destination Development Perspectives
5.2.3. Tourist Perspectives
5.3. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Enzensberger, H.M. A theory of tourism. New Ger. Crit. 1996, 68, 117–135. [Google Scholar] [CrossRef]
- Tabish, S.A. Healthcare: From good to exceptional governance. JIMSA 2012, 25, 147–150. [Google Scholar]
- Koncul, N. Wellness: A New Mode of tourism. Econ. Res. -Ekon. Istraživanja 2012, 25, 525–534. [Google Scholar] [CrossRef]
- Mueller, H.; Kaufmann, E.L. Wellness tourism: Market analysis of a special health tourism segment and implications for the hotel industry. J. Vacat. Mark. 2001, 7, 5–17. [Google Scholar] [CrossRef]
- Pereira, R.T.; Malone, C.M.; Flaherty, G.T. Corrigendum to: Aesthetic journeys: A review of cosmetic surgery tourism. J. Travel Med. 2018, 25, tay051. [Google Scholar] [CrossRef] [PubMed]
- Yaman, H. Travel Medicine in Turkey: Current State and Implications for the Future. J. Travel Med. 2006, 10, 68–69. [Google Scholar] [CrossRef]
- Bauer, I.L. Looking over the fence—How travel medicine can benefit from tourism research. J. Travel Med. 2015, 22, 206–207. [Google Scholar] [CrossRef]
- Jones, C.A.; Keith, L.G. Medical tourism and reproductive outsourcing: The dawning of a new paradigm for healthcare. Int. J. Fertil. Women’s Med. 2006, 51, 251–255. [Google Scholar]
- Leggat, P.; Kedjarune, U. Dental health, ‘dental tourism’ and travellers. Travel Med. Infect. Dis. 2016, 7, 123–124. [Google Scholar] [CrossRef]
- Crozier, G.K.D.; Thomsen, K. Stem cell tourism and the role of health professional organizations. Am. J. Bioeth. 2010, 10, 36–38. [Google Scholar] [CrossRef]
- Nikezic, S.; Djordjevic, M.; Bataveljic, D. Improvement of spa tourism in the Republic of Serbia as a pattern of positive impact on ecology and regional development. Tech. Technol. Educ. Manag.-TTEM 2012, 7, 920–925. [Google Scholar]
- Sayili, M.; Akca, H.; Duman, T.; Esengun, K. Psoriasis treatment via doctor fishes as part of health tourism: A case study of Kangal Fish Spring, Turkey. Tour. Manag. 2007, 28, 625–629. [Google Scholar] [CrossRef]
- Lunt, N.; Carrera, P. Medical tourism: Assessing the evidence on treatment abroad. Maturitas 2010, 66, 27–32. [Google Scholar] [CrossRef]
- Turner, L. “Medical Tourism” and the Global Marketplace in Health Services: U.S. Patients, International Hospitals, and the Search for Affordable Health Care. Int. J. Health Serv. 2010, 40, 443–467. [Google Scholar] [CrossRef] [PubMed]
- Chaulagain, S.; Pizam, A.; Wang, Y. An integrated behavioral model for medical tourism: An American perspective. J. Travel Res. 2021, 60, 761–778. [Google Scholar] [CrossRef]
- Jaramillo, J.; Goyal, D.; Lung, C. Birth Tourism among Chinese Women. MCN Am. J. Matern. Nurs. 2019, 44, 94–99. [Google Scholar] [CrossRef] [PubMed]
- Li, E.P.H.; Min, H.J.; Lee, S. Soft power and nation rebranding the transformation of Korean national identity through cosmetic surgery tourism. Int. Mark. Rev. 2021, 38, 141–162. [Google Scholar] [CrossRef]
- Xie, L.; Guan, X.; He, Y.; Huan, T.-C. Wellness tourism: Customer-perceived value on customer engagement. Tour. Rev. 2021. [Google Scholar] [CrossRef]
- Lwin, H.N.N.; Punnakitikashem, P.; Thananusak, T. The level and determinants of international patient satisfaction with dental tourism in Bangkok, Thailand. Cogent Bus. Manag. 2021, 8, 1898316. [Google Scholar] [CrossRef]
- Zhang, Q.; Zhang, H.; Xu, H. Health tourism destinations as therapeutic landscapes: Understanding the health perceptions of senior seasonal migrants. Soc. Sci. Med. 2021, 279, 113951. [Google Scholar] [CrossRef]
- Lee, H.K.; Fernando, Y. The antecedents and outcomes of the medical tourism supply chain. Tour. Manag. 2015, 46, 148–157. [Google Scholar] [CrossRef]
- Wang, K.; Xu, H.; Huang, L. Wellness tourism and spatial stigma: A case study of Bama, China. Tour. Manag. 2020, 78, 104039. [Google Scholar] [CrossRef]
- Rokni, L.; Park, S.-H. Medical Tourism in Iran, Reevaluation on the New Trends: A Narrative Review. Iran. J. Public Health 2020, 48, 1191–1202. [Google Scholar] [CrossRef]
- Rouland, B.; Jarraya, M. From medical tourism to regionalism from the bottom up: Emerging transnational spaces of care between Libya and Tunisia. J. Ethn. Migr. Stud. 2020, 46, 4248–4263. [Google Scholar] [CrossRef]
- Hanefeld, J.; Smith, R.; Horsfall, D.; Lunt, N. What Do We Know About Medical Tourism? A Review of the Literature With Discussion of Its Implications for the UK National Health Service as an Example of a Public Health Care System. J. Travel Med. 2014, 21, 410–417. [Google Scholar] [CrossRef] [PubMed]
- Hanefeld, J.; Lunt, N.; Smith, R.; Horsfall, D. Why do medical tourists travel to where they do? The role of networks in determining medical travel. Soc. Sci. Med. 2015, 124, 356–363. [Google Scholar] [CrossRef] [PubMed]
- Hopkins, L.; Labonté, R.; Runnels, V.; Packer, C. Medical tourism today: What is the state of existing knowledge? J. Public Health Policy 2010, 31, 185–198. [Google Scholar] [CrossRef] [PubMed]
- Hall, C.M.; James, M. Medical tourism: Emerging biosecurity and nosocomial issues. Tour. Rev. 2011, 66, 118–126. [Google Scholar] [CrossRef]
- Imison, M.; Schweinsberg, S. Australian news media framing of medical tourism in low-And middle income countries: A content review. BMC Public Health 2013, 13, 109. [Google Scholar] [CrossRef]
- Yu, J.; Lee, T.J.; Noh, H. Characteristics of a Medical Tourism Industry: The Case of South Korea. J. Travel Tour. Mark. 2011, 28, 856–872. [Google Scholar] [CrossRef]
- Crooks, V.A.; Kingsbury, P.; Snyder, J.; Johnston, R. What is known about the patient’s experience of medical tourism? A scoping review. BMC Health Serv. Res. 2010, 10, 266. [Google Scholar] [CrossRef]
- Pessot, E.; Spoladore, D.; Zangiacomi, A.; Sacco, M. Natural Resources in Health Tourism: A Systematic Literature Review. Sustainability 2021, 13, 2661. [Google Scholar] [CrossRef]
- Salehi-Esfahani, S.; Ridderstaat, J.; Ozturk, A.B. Health tourism in a developed country with a dominant tourism market: The case of the United States’ travellers to Canada. Curr. Issues Tour. 2021, 24, 536–553. [Google Scholar] [CrossRef]
- Chi, C.G.-Q.; Chi, O.H.; Ouyang, Z. Wellness hotel: Conceptualization, scale development, and validation. Int. J. Hosp. Manag. 2020, 89, 102404. [Google Scholar] [CrossRef]
- Stará, J.; Peterson, C. Understanding the concept of wellness for the future of the tourism industry: A literature review. J. Tour. Serv. 2017, 8, 18–29. [Google Scholar]
- Kazakov, S.; Oyner, O. Wellness tourism: A perspective article. Tour. Rev. 2021, 76, 58–63. [Google Scholar] [CrossRef]
- Chen, C.; Ibekwe-SanJuan, F.; Hou, J. The structure and dynamics of cocitation clusters: A multiple-perspective co-citation analysis. J. Am. Soc. Inf. Sci. Technol. 2010, 61, 1386–1409. [Google Scholar] [CrossRef]
- Chen, C. CiteSpace II: Detecting and visualizing emerging trends and transient patterns in scientific literature. J. Am. Soc. Inf. Sci. Technol. 2006, 57, 359–377. [Google Scholar] [CrossRef]
- Miles, M.B.; Huberman, A.M.; Huberman, M.A.; Huberman, M. Qualitative Data Analysis: An Expanded Sourcebook; SAGE: Thousand Oaks, CA, USA, 1994. [Google Scholar]
- Uçak, H. The relationship between the growth in the health sector and inbound health tourism: The case of Turkey. SpringerPlus 2016, 5, 1685. [Google Scholar] [CrossRef] [PubMed]
- Whittaker, A.; Manderson, L.; Cartwright, E. Patients without borders: Understanding medical travel. Med. Anthropol. 2010, 29, 336–343. [Google Scholar] [CrossRef]
- Singh, N. Exploring the factors influencing the travel motivations of US medical tourists. Curr. Issues Tour. 2013, 16, 436–454. [Google Scholar] [CrossRef]
- Snyder, J.; A Crooks, V.; Turner, L.; Johnston, R. Understanding the impacts of medical tourism on health human resources in Barbados: A prospective, qualitative study of stakeholder perceptions. Int. J. Equity Health 2013, 12, 2. [Google Scholar] [CrossRef] [PubMed]
- Runnels, V.; Carrera, P. Why do patients engage in medical tourism? Maturitas 2012, 73, 300–304. [Google Scholar] [CrossRef] [PubMed]
- Han, H.; Kiatkawsin, K.; Koo, B.; Kim, W. Thai wellness tourism and quality: Comparison between Chinese and American visitors’ behaviors. Asia Pac. J. Tour. Res. 2020, 25, 424–440. [Google Scholar] [CrossRef]
- Fetscherin, M.; Stephano, R.-M. The medical tourism index: Scale development and validation. Tour. Manag. 2016, 52, 539–556. [Google Scholar] [CrossRef]
- Hartwell, H. Medical Tourism: The Ethics, Regulation and Marketing of Health Mobility. Tour. Manag. 2014, 45, 1–2. [Google Scholar] [CrossRef]
- Moghimehfar, F.; Nasr-Esfahani, M.H. Decisive factors in medical tourism destination choice: A case study of Isfahan, Iran and fertility treatments. Tour. Manag. 2011, 32, 1431–1434. [Google Scholar] [CrossRef]
- Ormond, M.; Sulianti, D. More than medical tourism: Lessons from Indonesia and Malaysia on South–South intra-regional medical travel. Curr. Issues Tour. 2017, 20, 94–110. [Google Scholar] [CrossRef]
- Wang, H. Value as a medical tourism driver. Manag. Serv. Qual. Int. J. 2012, 22, 465–491. [Google Scholar] [CrossRef]
- Han, H.; Hyun, S.S. Customer retention in the medical tourism industry: Impact of quality, satisfaction, trust, and price reasonableness. Tour. Manag. 2015, 46, 20–29. [Google Scholar] [CrossRef]
- Han, H.; Hyun, S.S. Medical Hotel in the Growth of Global Medical Tourism. J. Travel Tour. Mark. 2014, 31, 366–380. [Google Scholar] [CrossRef]
- Abubakar, A.M.; Ilkan, M. Impact of online WOM on destination trust and intention to travel: A medical tourism perspective. J. Destin. Mark. Manag. 2016, 5, 192–201. [Google Scholar] [CrossRef]
- Crooks, V.; Cameron, K.; Chouinard, V.; Johnston, R.; Snyder, J.; Casey, V. Use of medical tourism for hip and knee surgery in osteoarthritis: A qualitative examination of distinctive attitudinal characteristics among Canadian patients. BMC Health Serv. Res. 2012, 12, 417. [Google Scholar] [CrossRef] [PubMed]
- Kingsbury, P.; Crooks, V.A.; Snyder, J.; Johnston, R.; Adams, K. Narratives of emotion and anxiety in medical tourism: On State of the Heart and Larry’s Kidney. Soc. Cult. Geogr. 2012, 13, 361–378. [Google Scholar] [CrossRef]
- Margolis, R.; Ludi, E.; Pao, M.; Wiener, L. International adaptation: Psychosocial and parenting experiences of caregivers who travel to the United States to obtain acute medical care for their seriously ill child. Soc. Work Health Care 2013, 52, 669–683. [Google Scholar] [CrossRef] [PubMed][Green Version]
- An, D. Understanding Medical Tourists in Korea: Cross-Cultural Perceptions of Medical Tourism among Patients from the USA, Russia, Japan, and China. Asia Pac. J. Tour. Res. 2013, 19, 1141–1169. [Google Scholar] [CrossRef]
- Yu, J.Y.; Ko, T.G. A cross-cultural study of perceptions of medical tourism among Chinese, Japanese and Korean tourists in Korea. Tour. Manag. 2012, 33, 80–88. [Google Scholar] [CrossRef]
- Altın, U.; Bektaş, G.; Antep, Z.; İrban, A. The international patient’s portfolio and marketing of Turkish health tourism. Procedia-Soc. Behav. Sci. 2012, 58, 1004–1007. [Google Scholar] [CrossRef]
- Connell, J. Contemporary medical tourism: Conceptualisation, culture and commodification. Tour. Manag. 2013, 34, 1–13. [Google Scholar] [CrossRef]
- Johnston, R.; Crooks, V.A.; Snyder, J.; Whitmore, R. “The major forces that need to back medical tour-ism were… in alignment” Championing development of Barbados’s medical tourism sector. Int. J.-Health Serv. 2015, 45, 334–352. [Google Scholar] [CrossRef] [PubMed]
- Chinai, R.; Goswami, R. Medical visas mark growth of Indian medical tourism. Bull. World Health Organ. 2007, 85, 164–165. [Google Scholar] [CrossRef]
- Gupta, V.; Das, P. Medical Tourism in India. Clin. Lab. Med. 2012, 32, 321–325. [Google Scholar] [CrossRef]
- Snyder, J.; Johnston, R.; Crooks, V.A.; Morgan, J.; Adams, K. How Medical Tourism Enables Preferential access to Care: Four Patterns from the Canadian Context. Health Care Anal. 2017, 25, 138–150. [Google Scholar] [CrossRef]
- Gambarov, V.; Gjinika, H. Thermal Spring Health Tourism in Albania: Challenges and Perspectives. In Strategic Innovative Marketing and Tourism; Springer: Cham, Switzerland, 2017; pp. 455–465. [Google Scholar]
- Kumar, S.; Breuing, R.; Chahal, R. Globalization of Health Care Delivery in the United States through Medical Tourism. J. Health Commun. 2012, 17, 177–198. [Google Scholar] [CrossRef]
- Besciu, C.D. The impact of corruption on the performance management of European Health Systems. Manag. Res. Pract. 2016, 8, 5–22. [Google Scholar]
- Qadeer, I.; Reddy, S. Medical tourism in india: Perceptions of physicians in tertiary care hospitals. Philos. Ethic-Humanit. Med. 2013, 8, 20. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Kazemha, A.S.; Dehkordi, K.S. The Principles of Designing Hospital Hotel with the Approach of Health Tourism in Kish Island. J. Hist. Cult. Art Res. 2017, 6, 515. [Google Scholar] [CrossRef]
- Ghosh, T.; Mandal, S. Medical Tourism Experience: Conceptualization, Scale Development, and Validation. J. Travel Res. 2018, 58, 1288–1301. [Google Scholar] [CrossRef]
- Crooks, V.A.; Turner, L.; Snyder, J.; Johnston, R.; Kingsbury, P. Promoting medical tourism to India: Messages, images, and the marketing of international patient travel. Soc. Sci. Med. 2011, 72, 726–732. [Google Scholar] [CrossRef] [PubMed]
- Farahmand, A.A.; Merati, E. It Strategies for Development of Health Tourism. Turk. Online J. Des. ART Commun. 2016, 6, 1086–1092. [Google Scholar] [CrossRef]
- Moghavvemi, S.; Ormond, M.; Musa, G.; Isa, C.R.M.; Thirumoorthi, T.; Mustapha, M.Z.B.; Chandy, J.J.C. Connecting with prospective medical tourists online: A cross-sectional analysis of private hospital websites promoting medical tourism in India, Malaysia and Thailand. Tour. Manag. 2017, 58, 154–163. [Google Scholar] [CrossRef]
- Chang, I.-C.; Chou, P.-C.; Yeh, R.K.-J.; Tseng, H.-T. Factors influencing Chinese tourists’ intentions to use the Taiwan Medical Travel App. Telemat. Inform. 2016, 33, 401–409. [Google Scholar] [CrossRef]
- Turner, L. Beyond “medical tourism”: Canadian companies marketing medical travel. Glob. Health 2012, 8, 16. [Google Scholar] [CrossRef]
- Mohamad, W.N.; Omar, A.; Haron, M.S. The moderating effect of medical travel facilitators in medical tourism. Procedia-Soc. Behav. Sci. 2012, 65, 358–363. [Google Scholar] [CrossRef]
- Cormany, D.; Baloglu, S. Medical travel facilitator websites: An exploratory study of web page contents and services offered to the prospective medical tourist. Tour. Manag. 2011, 32, 709–716. [Google Scholar] [CrossRef]
- Dalstrom, M. Medical travel facilitators: Connecting patients and providers in a globalized world. Anthr. Med. 2013, 20, 24–35. [Google Scholar] [CrossRef] [PubMed]
- Smith, M. Baltic Health Tourism: Uniqueness and Commonalities. Scand. J. Hosp. Tour. 2015, 15, 357–379. [Google Scholar] [CrossRef]
- Bjerke, R.; Polegato, R. How well do advertising images of health and beauty travel across cultures? A self-concept perspective. Psychol. Mark. 2006, 23, 865–884. [Google Scholar] [CrossRef]
- Lee, H.; Wright, K.B.; O’Connor, M.; Wombacher, K. Framing medical tourism: An analysis of persuasive appeals, risks and benefits, and new media features of medical tourism broker websites. Health Commun.-Cation 2014, 29, 637–645. [Google Scholar] [CrossRef]
- Connell, J. Medical tourism: Sea, sun, sand and …. surgery. Tour. Manag. 2006, 27, 1093–1100. [Google Scholar] [CrossRef]
- Connell, J. A new inequality? Privatisation, urban bias, migration and medical tourism. Asia Pac. Viewp. 2011, 52, 260–271. [Google Scholar] [CrossRef]
- Perfetto, R.; Dholakia, N. Exploring the cultural contradictions of medical tourism. Consum. Mark. Cult. 2010, 13, 399–417. [Google Scholar] [CrossRef]
- Smith, K. The Problematization of Medical tourism: A Critique of Neoliberalism. Dev. World Bioeth. 2012, 12, 1–8. [Google Scholar] [CrossRef]
- De Arellano, A.B.R. Patients without borders: The emergence of medical tourism. Int. J. Health Serv. 2007, 37, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Johnston, R.; Adams, K.; Bishop, L.; A Crooks, V.; Snyder, J. “Best care on home ground” versus “elitist healthcare”: Concerns and competing expectations for medical tourism development in Barbados. Int. J. Equity Health 2015, 14, 15. [Google Scholar] [CrossRef] [PubMed]
- NaRanong, A.; NaRanong, V. The effects of medical tourism: Thailand’s experience. Bull. World Health Organ. 2011, 89, 336–344. [Google Scholar] [CrossRef]
- Vijaya, R.M. Medical Tourism: Revenue Generation or International Transfer of Healthcare Problems? J. Econ. Issues 2010, 44, 53–70. [Google Scholar] [CrossRef]
- Adler, A.; Shklyar, M.; Schwaber, M.J.; Navon-Venezia, S.; Dhaher, Y.; Edgar, R.; Solter, E.; Benenson, S.; Masarwa, S.; Carmeli, Y. Introduction of OXA-48-producing Enterobacteriaceae to Israeli hospitals by medical tourism. J. Antimicrob. Chemother. 2011, 66, 2763–2766. [Google Scholar] [CrossRef]
- Green, S.T. Medical tourism–a potential growth factor in infection medicine and public health. J. Infect. 2008, 57, 429. [Google Scholar] [CrossRef]
- Chen, L.H.; Wilson, M.E. The globalization of healthcare: Implications of medical tourism for the infectious disease clinician. Clin. Infect. Dis. 2013, 57, 1752–1759. [Google Scholar] [CrossRef]
- Turner, L. News media reports of patient deaths following ‘medical tourism’ for cosmetic surgery and bariatric surgery. Dev. World Bioeth. 2012, 12, 21–34. [Google Scholar] [CrossRef] [PubMed]
- Barclay, E. Stem-cell experts raise concerns about medical tourism. Lancet 2009, 373, 883–884. [Google Scholar] [CrossRef]
- Lindvall, O.; Hyun, I. Medical Innovation Versus Stem Cell Tourism. Science 2009, 324, 1664–1665. [Google Scholar] [CrossRef]
- Penney, K.; Snyder, J.; A Crooks, V.; Johnston, R. Risk communication and informed consent in the medical tourism industry: A thematic content analysis of canadian broker websites. BMC Med. Ethic. 2011, 12, 17. [Google Scholar] [CrossRef] [PubMed]
- Evans, R.W. Ethnocentrism Is an Unacceptable Rationale for Health Care Policy: A Critique of Transplant Tourism Position Statements. Arab. Archaeol. Epigr. 2008, 8, 1089–1095. [Google Scholar] [CrossRef] [PubMed]
- Johnston, R.; Crooks, V.A.; Ormond, M. Policy implications of medical tourism development in desti-nation countries: Revisiting and revising an existing framework by examining the case of Jamaica. Glob. Health 2015, 11, 29. [Google Scholar] [CrossRef] [PubMed]
- Pocock, N.S.; Phua, K.H. Medical tourism and policy implications for health systems: A conceptual framework from a comparative study of Thailand, Singapore and Malaysia. Glob. Health 2011, 7, 12. [Google Scholar] [CrossRef] [PubMed]
- Maguire, Á.; Bussmann, S.; zu Köcker, C.M.; Verra, S.E.; Giurgi, L.A.; Ruggeri, K. Raising concern about the information provided on medical travel agency websites: A place for policy. Health Policy Technol. 2016, 5, 414–422. [Google Scholar] [CrossRef]
- Álvarez, M.M.; Chanda, R.; Smith, R.D. The potential for bilateral agreements in medical tourism: A qualitative study of stakeholder perspectives from the UK and India. Glob. Health 2011, 7, 11. [Google Scholar] [CrossRef] [PubMed]
- Exworthy, M.; Peckham, S. Access, Choice and Travel: Implications for Health Policy. Soc. Policy Adm. 2006, 40, 267–287. [Google Scholar] [CrossRef]
- Cohen, I.G. How To Regulate Medical Tourism (And Why It Matters for Bioethics). Dev. World Bioeth. 2012, 12, 9–20. [Google Scholar] [CrossRef] [PubMed]
- Lunt, N.; Horsfall, D.; Smith, R.; Exworthy, M.; Hanefeld, J.; Mannion, R. Market size, market share and market strategy: Three myths of medical tourism. Policy Politics 2014, 42, 597–614. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Names of Journals (Top 10) | Number | Percentage |
|---|---|---|
| Tourism Management | 38 | 24.67% |
| Journal of Travel & Tourism Marketing | 26 | 16.88% |
| Asia Pacific Journal of Tourism Research | 22 | 14.28% |
| Current Issues in Tourism | 18 | 11.68% |
| International Journal of Tourism Research | 13 | 8.44% |
| Annals of Tourism Research | 9 | 5.84% |
| Journal of Destination Marketing & Management | 9 | 5.84% |
| Tourism Review | 7 | 4.55% |
| Journal of Travel Medicine | 6 | 3.90% |
| Tourism Management Perspectives | 6 | 3.90% |
| Total | 154 | 100% |
| Names of Journals (Top 10) | Number | Percentage |
|---|---|---|
| Social Science & Medicine | 24 | 16.11% |
| Iranian Journal of Public Health | 24 | 16.11% |
| Globalization and Health | 22 | 14.77% |
| Sustainability | 22 | 14.77% |
| Plastic and Reconstructive Surgery | 13 | 8.72% |
| BMC Health Services Research | 12 | 8.05% |
| Canadian Family Physician | 9 | 6.04% |
| BMJ–British Medical Journal | 8 | 5.37% |
| Developing World Bioethics | 8 | 5.37% |
| Journal of Medical Ethics | 7 | 4.70% |
| Total | 149 | 100% |
| Destination | Frequency | Rank |
|---|---|---|
| Canada | 13 | 1 |
| India | 13 | 2 |
| Malaysia | 9 | 3 |
| South Korea | 9 | 4 |
| Thailand | 8 | 5 |
| China | 7 | 6 |
| Iran | 5 | 7 |
| Russia | 4 | 8 |
| Singapore | 4 | 9 |
| Taiwan | 4 | 10 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zhong, L.; Deng, B.; Morrison, A.M.; Coca-Stefaniak, J.A.; Yang, L. Medical, Health and Wellness Tourism Research—A Review of the Literature (1970–2020) and Research Agenda. Int. J. Environ. Res. Public Health 2021, 18, 10875. https://doi.org/10.3390/ijerph182010875
Zhong L, Deng B, Morrison AM, Coca-Stefaniak JA, Yang L. Medical, Health and Wellness Tourism Research—A Review of the Literature (1970–2020) and Research Agenda. International Journal of Environmental Research and Public Health. 2021; 18(20):10875. https://doi.org/10.3390/ijerph182010875
Chicago/Turabian StyleZhong, Lina, Baolin Deng, Alastair M. Morrison, J. Andres Coca-Stefaniak, and Liyu Yang. 2021. "Medical, Health and Wellness Tourism Research—A Review of the Literature (1970–2020) and Research Agenda" International Journal of Environmental Research and Public Health 18, no. 20: 10875. https://doi.org/10.3390/ijerph182010875
APA StyleZhong, L., Deng, B., Morrison, A. M., Coca-Stefaniak, J. A., & Yang, L. (2021). Medical, Health and Wellness Tourism Research—A Review of the Literature (1970–2020) and Research Agenda. International Journal of Environmental Research and Public Health, 18(20), 10875. https://doi.org/10.3390/ijerph182010875