
Multifactorial Programs for Healthy Older Adults to Reduce Falls and Improve Physical Performance: Systematic Review

 ,
,  ,
,  ,
,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Information Sources and Search Strategy
2.2. Inclusion and Exclusion Criteria
2.3. Selection Process and Data Extraction
2.4. Outcomes
2.5. Quality of the Included Studies
3. Results
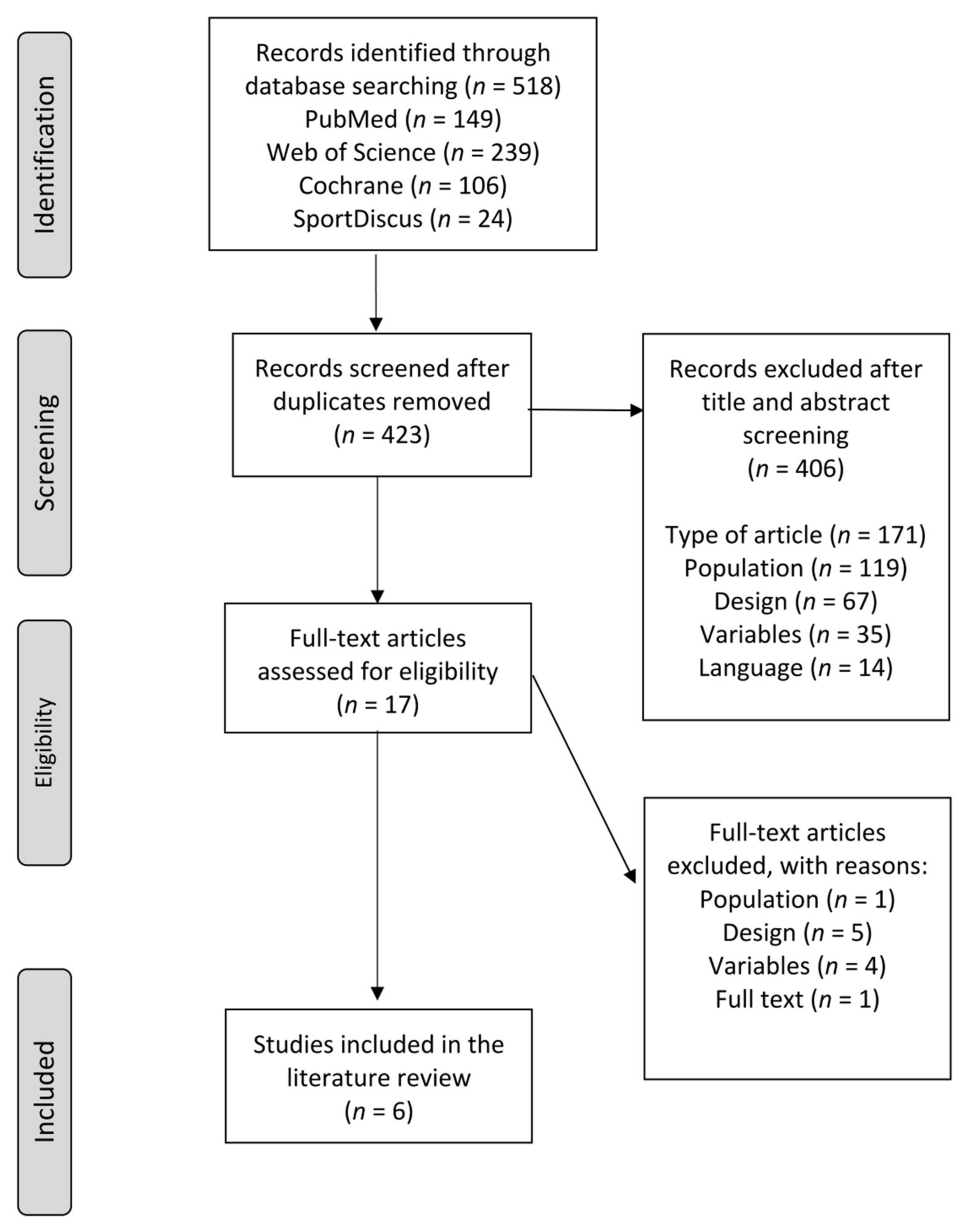
3.1. Inclusion of Studies
3.2. Quality of Studies
3.3. Characteristics of Studies and Participants
3.4. Outcomes
3.4.1. Rate of Falls
3.4.2. Physical Performance
3.4.3. Secondary Outcomes
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- WHO. Global Recommendations on Physical Activity for Health; WHO Press: Geneva, Switzerland, 2010. [Google Scholar]
- United Nations. World Population Prospects: The 2015 Revision, Key Findings and Advance Tables; Working Paper; UN: New York, NY, USA, 2015. [Google Scholar]
- United Nations. World Population Ageing 2017; United Nations, Department of Economic and Social Affairs, Population Division: New York, NY, USA, 2017. [Google Scholar]
- Rechel, B.; Grundy, E.; Robine, J.M.; Cylus, J.; Mackenbach, J.P.; Knai, C.; McKee, M. Ageing in the European Union. Lancet 2013, 381, 1312–1322. [Google Scholar] [CrossRef]
- Deandrea, S.; Lucenteforte, E.; Bravi, F.; Foschi, R.; La Vecchia, C.; Negri, E. Risk Factors for Falls in Community-dwelling Older People. Epidemiology 2010, 21, 658–668. [Google Scholar] [CrossRef]
- Morrison, A.; Fan, T.; Sen, S.S.; Weisenfluh, L. Epidemiology of falls and osteoporotic fractures: A systematic review. Clinicoecon Outcomes Res. 2013, 5, 9–18. [Google Scholar]
- Peeters, G.; van Schoor, N.M.; Lips, P. Fall risk: The clinical relevance of falls and how to integrate fall risk with fracture risk. Best Pract. Res. Clin. Rheumatol. 2009, 23, 797–804. [Google Scholar] [CrossRef]
- Hartholt, K.A.; van Beeck, E.F.; Polinder, S.; van der Velde, N.; van Lieshout, E.M.; Panneman, M.J.; van der Cammen, T.J.; Patka, P. Societal consequences of falls in the older population: Injuries, healthcare costs, and long-term reduced quality of life. J. Trauma. 2011, 71, 748–753. [Google Scholar] [CrossRef] [Green Version]
- WHO. Global Report on Falls Prevention in Older Age. Community Health; WHO: Geneva, Switzerland, 2007. [Google Scholar]
- Franse, C.B.; Rietjens, J.A.; Burdorf, A.; van Grieken, A.; Korfage, I.J.; van der Heide, A.; Mattace-Raso, F.; van Beeck, E.; Raat, H. A prospective study on the variation in falling and fall risk among community-dwelling older citizens in 12 European countries. B.M.J. Open. 2017, 7, e015827. [Google Scholar] [CrossRef] [Green Version]
- Lusardi, M.M.; Fritz, S.; Middleton, A.; Allison, L.; Wingood, M.; Phillips, E.; Cris, M.; Verma, S.; Osborne, J.; Chui, K.K. Determining Risk of Falls in Community Dwelling Older Adults: A Systematic Review and Meta-analysis Using Posttest Probability. J. Geriatr. Phys. 2017, 40, 1–36. [Google Scholar] [CrossRef] [Green Version]
- Skelton, D.A.; Becker, C.; Lamb, S.E.; Close, J.C.T.; Zijlstra, W.; Yardley, L.; Todd, C.J. Prevention of Falls Network Europe: A thematic network aimed at introducing good practice in effective falls prevention across. Eur. J. Ageing 2004, 1, 89–94. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.C.; Chang, K.C.; Tsauo, J.Y.; Hung, J.W.; Huang, Y.C.; Lin, S.I. Effects of a Multifactorial Fall Prevention Program on Fall Incidence and Physical Function in Community-Dwelling Older Adults with Risk of Falls. Arch. Phys. Med. Rehabil. 2013, 94, 606–615.e1. [Google Scholar] [CrossRef]
- Park, S.H. Tools for assessing fall risk in the elderly: A systematic review and meta-analysis. Aging. Clin. Exp. Res. 2018, 30, 1–16. [Google Scholar] [CrossRef]
- Karlsson, M.; Vonschewelov, T.; Karlsson, C.; Cöster, M.; Rosengen, B.E. Prevention of falls in the elderly: A review. Scand. J. Public Health 2013, 41, 442–454. [Google Scholar] [CrossRef]
- Todd, C.; Skelton, D. What are the Main Risk Factors for Falls among Older People and What are the Most Effective Interventions to Prevent These Falls? WHO Regional Office for Europe: Copenhagen, Denmark, 2004; Available online: http://www.euro.who.int/document/E82552.pdf (accessed on 27 July 2021).
- Onder, G.; Penninx, B.W.; Ferrucci, L.; Fried, L.P.; Guralnik, J.M.; Pahor, M. Measures of physical performance and risk for progressive and catastrophic disability: Results from the Women’s Health and Aging Study. J. Gerontol. A. Biol. Sci. Med. Sci. 2005, 60, 74–79. [Google Scholar] [CrossRef] [Green Version]
- Studenski, S.; Perera, S.; Pate, K.; Rosano, C.; Faulkner, K.; Inzitari, M.; Brach, J.; Chandler, J.; Cawthon, P.; Connor, E.B.; et al. Gait speed and survival in older adults. Jama 2011, 305, 50–58. [Google Scholar] [CrossRef] [Green Version]
- Owen, N.; Healy, G.N.; Matthews, C.E.; Dunstan, D.W. Too much sitting: The population health science of sedentary behavior. Exerc Sport Sci Rev. 2010, 38, 105–113. [Google Scholar] [CrossRef]
- Chodzko-Zajko, W.J.; Proctor, D.N.; Singh, M.A.F.; Minson, C.T.; Nigg, C.R.; Salem, G.J.; Skinner, J.S. Exercise and physical activity for older adults. Med. Sci. Sports Exerc. 2016, 11, 9457–9468. [Google Scholar]
- Biswas, A.; Oh, P.I.; Faulkner, G.E.; Bajaj, R.R.; Silver, M.A.; Mitchell, M.S.; Alter, D.A. Sedentary time and its association with risk for disease incidence, mortality, and hospitalization in adults a systematic review and meta-analysis. Ann. Intern. Med. 2015, 162, 123–132. [Google Scholar] [CrossRef]
- De Labra, C.; Guimaraes-Pinheiro, C.; Maseda, A.; Lorenzo, T.; Millán-Calenti, J. Effects of physical exercise interventions in frail older adults: A systematic review of randomized controlled trials Physical functioning, physical health and activity. BMC. Geriatr. 2015, 15, 45. [Google Scholar] [CrossRef] [Green Version]
- Sherrington, C.; Michaleff, Z.A.; Fairhall, N.; Paul, S.S.; Tiedemann, A.; Whitney, J.; Cumming, R.G.; Herbert, R.D.; Close, J.C.T.; Lord, S.R. Exercise to prevent falls in older adults: An updated systematic review and meta-analysis. Br. J. Sports. Med. 2017, 51, 1750–1758. [Google Scholar] [CrossRef]
- Hita-Contreras, F.; Martínez-Amat, A.; Cruz-Díaz, D.; Pérez-López, F.R. Fall prevention in postmenopausal women: The role of Pilates exercise training. Climacteric 2016, 19, 229–233. [Google Scholar] [CrossRef]
- Lomas-Vega, R.; Obrero-Gaitán, E.; Molina-Ortega, F.J.; Del-Pino-Casado, R. Tai Chi for Risk of Falls. A Meta-analysis. J. Am. Geriatr. Soc. 2017, 65, 2037–2043. [Google Scholar] [CrossRef]
- Gillespie, L.D.; Robertson, M.C.; Gillespie, W.J.; Sherrington, C.; Gates, S.; Clemson, L.; Lamb, S.E. Interventions for preventing falls in older people living in the community. Cochrane Database Syst. Rev. 2012, 2012, CD007146. [Google Scholar]
- Delbaere, K.; Close, J.C.T.; Heim, J.; Sachdev, P.S.; Brodaty, H.; Slavin, M.J.; Kochan, N.A.; Lord, S.R. A Multifactorial Approach to Understanding Fall Risk in Older People. J. Am. Geriatr. Soc. 2010, 58, 1679–1685. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Valdés-Badilla, P.A.; Gutiérrez-García, C.; Pérez-Gutiérrez, M.; Vargas-Vitoria, R.; López-Fuenzalida, A. Effects of Physical Activity Governmental Programs on Health Status in Independent Older Adults: A Systematic Review. J. Aging Phys. Act. 2019, 27, 265–275. [Google Scholar] [CrossRef]
- Tinetti, M.; Baker, D.; Dutcher, J.; Vicent, J.; Rozett, R. Reducing the Risk of Falls among Older Adults in the Community; Peaceable Kingdom Press: Berkeley, CA, USA, 1997. [Google Scholar]
- De Morton, N.A. The PEDro scale is a valid measure of the methodological quality of clinical trials: A demographic study. Aust. J. Physiother. 2009, 55, 129–133. [Google Scholar] [CrossRef] [Green Version]
- Foley, N.C.; Bhogal, S.K.; Teasell, R.W.; Bureau, Y.; Speechley, M.R. Estimates of quality and reliability with the physiotherapy evidence-based database scale to assess the methodology of randomized controlled trials of pharmacological and nonpharmacological interventions. Phys. Ther. 2006, 86, 817–824. [Google Scholar] [CrossRef]
- Beling, J.; Roller, M. Multifactorial intervention with balance training as a core component among fall-prone older adults. J. Geriatr. Phys. Ther. 2009, 32, 123–133. [Google Scholar] [CrossRef] [Green Version]
- Pérula, L.A.; Varas-Fabra, F.; Rodríguez, V.; Ruiz-Moral, R.; Fernández, J.A.; González, J.; Pérula, C.J.; Roldán, A.M.; de Dios, C. Effectiveness of a multifactorial intervention program to reduce falls incidence among community-living older adults A randomized controlled trial. Arch. Phys. Med. Rehabil. 2012, 93, 1677–1684. [Google Scholar] [CrossRef]
- Fairhall, N.; Sherrington, C.; Lord, S.R.; Kurrle, S.E.; Langron, C.; Lockwood, K.; Monaghan, N.; Aggar, C.; Cameron, I.D. Effect of a multifactorial, interdisciplinary intervention on risk factors for falls and fall rate in frail older people: A randomised controlled trial. Age Ageing 2013, 43, 616–622. [Google Scholar] [CrossRef] [Green Version]
- Siegrist, M.; Freiberger, E.; Geilhof, B.; Salb, J.; Hentschke, C.; Landendoerfer, P.; Linde, K.; Halle, M.; Blanck, W.A. Fall Prevention in a Primary Care Setting. Dtsch. Arztebl. Int. 2016, 113, 365–372. [Google Scholar] [CrossRef] [Green Version]
- Matchar, D.B.; Duncan, P.W.; Lien, C.T.; Ong, M.E.H.; Lee, M.; Gao, F.; Sim, R.; Eom, K. Randomized Controlled Trial of Screening, Risk Modification, and Physical Therapy to Prevent Falls Among the Elderly Recently Discharged From the Emergency Department to the Community: The Steps to Avoid Falls in the Elderly Study. Arch. Phys. Med. Rehabil. 2017, 98, 1086–1096. [Google Scholar] [CrossRef]
- Panel on Prevention of Falls in Older Persons, American Geriatrics Society and British Geriatrics Society. Summary of the Updated American Geriatrics Society/British Geriatrics Society clinical practice guideline for prevention of falls in older persons. J. Am. Geriat. R. Soc. 2011, 59, 148–157.
- Hopewell, S.; Copsey, B.; Nicolson, P.; Adedire, B.; Boniface, G.; Lamb, S. Multifactorial interventions for preventing falls in older people living in the community: A systematic review and meta-analysis of 41 trials and almost 20,000 participants. Br. J. Sports Med. 2020, 54, 1340–1350. [Google Scholar] [CrossRef] [Green Version]
- Tricco, A.C.; Thomas, S.M.; Veroniki, A.A.; Hamid, J.S.; Cogo, E.; Strifler, L.; Khan, P.A.; Robson, R.; Sibley, K.M.; MacDonald, H.; et al. Comparisons of Interventions for Preventing Falls in Older Adults: A Systematic Review and Meta-analysis. JAMA 2017, 318, 1687–1699. [Google Scholar] [CrossRef]
- Soares Menezes, K.V.R.; Auger, C.; de Souza Menezes, W.R.; Guerra, R.O. Instruments to evaluate mobility capacity of older adults during hospitalization: A systematic review. Arch. Gerontol. Geriatr. 2017, 72, 67–79. [Google Scholar] [CrossRef]
- Shumway-Cook, A.; Brauer, S.; Woollacott, M. Predicting the probability for falls in community-dwelling older adults using the Timed Up & Go Test. Phys. Ther. 2000, 80, 896–903. [Google Scholar]
- Muir, S.W.; Berg, K.; Chesworth, B.M.; Klar, N.; Speechley, M. Modifiable Risk Factors Identify People Who Transition from Non-fallers to Fallers in Community-Dwelling Older Adults: A Prospective Study. Physiother. Can. 2010, 62, 358–367. [Google Scholar] [CrossRef]
- Marques, E.A.; Figueiredo, P.; Harris, T.B.; Wanderley, F.A.; Carvalho, J. Are resistance and aerobic exercise training equally effective at improving knee muscle strength and balance in older women? Arch. Gerontol. Geriatr. 2017, 68, 106–112. [Google Scholar] [CrossRef] [Green Version]
- Vasconcelos Rocha, S.; Souza Dos Santos, S.; Carneiro Vasconcelos, L.R.; Alves Dos Santos, C. Strength and ability to implement the activities of daily living in elderly resident in rural areas. Colomb. Med. 2016, 47, 167–171. [Google Scholar] [CrossRef]
- Neri, S.G.R.; Lima, R.M.; Ribeiro, H.S.; Vainshelboim, B. Poor handgrip strength determined clinically is associated with falls in older women. J. Frailty Sarcopenia Falls 2021, 6, 43–49. [Google Scholar] [CrossRef]
- Lord, S.R.; Menz, H.B.; Tiedemann, A. A physiological profile approach to falls risk assessment and prevention. Phys. Ther. 2003, 83, 237–252. [Google Scholar] [CrossRef] [PubMed]
- Murphy, S.L.; Williams, C.S.; Gill, T.M. Characteristics associated with fear of falling and activity restriction in community-living older persons. J. Am. Geriatr. Soc. 2002, 50, 516–520. [Google Scholar] [CrossRef]
- Aibar-Almazán, A.; Martínez-Amat, A.; Cruz-Díaz, D.; De la Torre-Cruz, M.J.; Jiménez-García, J.D.; Zagalaz-Anula, N.; Pérez-Herrezuelo, I.; Hita-Contreras, F. Effects of Pilates on fall risk factors in community-dwelling elderly women: A randomized, controlled trial. Eur. J. Sport Sci. 2019, 19, 1386–1394. [Google Scholar] [CrossRef] [PubMed]
- Stanghelle, B.; Bentzen, H.; Giangregorio, L.; Pripp, A.H.; Skelton, D.A.; Bergland, A. Effects of a resistance and balance exercise programme on physical fitness, health-related quality of life and fear of falling in older women with osteoporosis and vertebral fracture: A randomized controlled trial. Osteoporos. Int. 2020, 31, 1069–1078. [Google Scholar] [CrossRef] [PubMed]
- Ekelund, U.; Tarp, J.; Steene-Johannessen, J.; Hansen, B.H.; Jefferis, B.; Fagerland, M.W.; Whincup, P.; Diaz, K.M.; Hooker, S.P.; Chernofsky, A.; et al. Dose-response associations between accelerometry measured physical activity and sedentary time and all cause mortality: Systematic review and harmonised meta-analysis. BMJ 2019, 366, l4570. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Studies | (a) | (b) | (c) | (d) | (e) | (f) | (g) | (h) | (i) | (j) | (k) | Score |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Beling and Roller [33] | Yes | Yes | No | Yes | No | No | No | No | No | Yes | Yes | 4/10 |
| Pérula et al. [34] | Yes | Yes | No | No | No | No | Yes | Yes | Yes | Yes | Yes | 6/10 |
| Lee et al. [13] | Yes | Yes | No | Yes | No | No | No | Yes | No | Yes | No | 5/10 |
| Fairhall et al. [35] | Yes | Yes | Yes | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 8/10 |
| Siegrist et al. [36] | Yes | Yes | No | Yes | No | No | No | No | No | Yes | Yes | 4/10 |
| Matchar et al. [37] | Yes | Yes | No | Yes | No | No | Yes | Yes | Yes | Yes | Yes | 7/10 |
| Components | |||||||
|---|---|---|---|---|---|---|---|
| Exercise + FRHA | Exercise + HE | Exercise + FRHA + MM | Exercise + FRHA + HE + MM | ||||
| Beling and Roller [33] | Pérula et al. [34] | Siegrist et al. [36] | Fairhall et al. [35] | Matchar et al. [37] | Lee et al. [13] | ||
| Rate of falls | ✓ * | ✓ * | ✓ * | ✓ | ✓ | ✓ | |
| Physical performance | Mobility and gait | ✓ | ✓ * | ✓ * | ✓ * | ✓ * | ✓ * |
| Balance | ✓ * | ✓ * | ✓ * | ✓ * | ✓ * | ||
| Strength | ✓ * | ✓ | ✓ * | ✓ * | |||
| Physiological functioning | ✓ | ✓ * | |||||
| Fear of falling | ✓ * | ✓ * | ✓ | ||||
| PA level | ✓ | ✓ * | |||||
| Ways of Delivery of Exercise Intervention | |||||||
|---|---|---|---|---|---|---|---|
| Group Activities | Home-Based Program | Group Activities + Home-Based Program | |||||
| Beling and Roller [33] | Siegrist et al. [36] | Fairhall et al. [35] | Pérula et al. [34] | Matchar et al. [37] | Lee et al. [13] | ||
| Rate of falls | ✓ * | ✓ * | ✓ | ✓ * | ✓ | ✓ | |
| Physical performance | Mobility and gait | ✓ | ✓ * | ✓ * | ✓ * | ✓ * | ✓ * |
| Balance | ✓ * | ✓ * | ✓ * | ✓ * | ✓ * | ||
| Strength | ✓ * | ✓ | ✓ * | ✓ * | |||
| Physiological functioning | ✓ | ✓ * | |||||
| Fear of falling | ✓ * | ✓ * | ✓ | ||||
| PA level | ✓ | ✓ * | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Loureiro, V.; Gomes, M.; Loureiro, N.; Aibar-Almazán, A.; Hita-Contreras, F. Multifactorial Programs for Healthy Older Adults to Reduce Falls and Improve Physical Performance: Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 10842. https://doi.org/10.3390/ijerph182010842
Loureiro V, Gomes M, Loureiro N, Aibar-Almazán A, Hita-Contreras F. Multifactorial Programs for Healthy Older Adults to Reduce Falls and Improve Physical Performance: Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(20):10842. https://doi.org/10.3390/ijerph182010842
Chicago/Turabian StyleLoureiro, Vânia, Margarida Gomes, Nuno Loureiro, Agustín Aibar-Almazán, and Fidel Hita-Contreras. 2021. "Multifactorial Programs for Healthy Older Adults to Reduce Falls and Improve Physical Performance: Systematic Review" International Journal of Environmental Research and Public Health 18, no. 20: 10842. https://doi.org/10.3390/ijerph182010842
APA StyleLoureiro, V., Gomes, M., Loureiro, N., Aibar-Almazán, A., & Hita-Contreras, F. (2021). Multifactorial Programs for Healthy Older Adults to Reduce Falls and Improve Physical Performance: Systematic Review. International Journal of Environmental Research and Public Health, 18(20), 10842. https://doi.org/10.3390/ijerph182010842