
Association between Weight Loss and Food Form in Older Individuals Residing in Long-Term Care Facilities: 1-Year Multicenter Longitudinal Study

 , , , , , , , , ,
, , , , , , , , ,
Abstract
1. Introduction
2. Materials and Methods
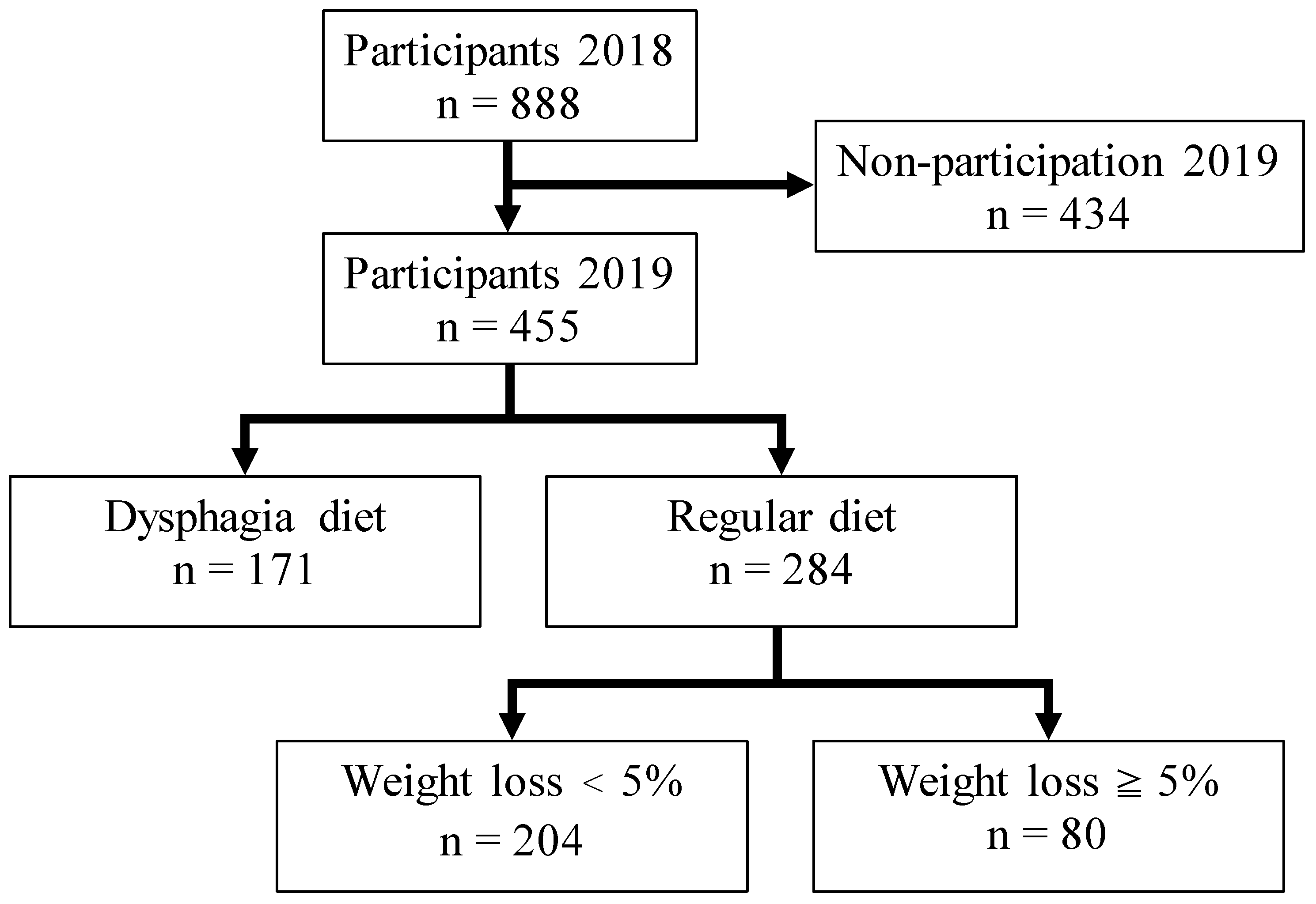
2.1. Study Population
2.2. Survey Items
2.3. Survey Contents in the Questionnaire
2.3.1. Basic Information
2.3.2. Total Energy Intake and Food Form
2.4. Oral Survey
Evaluation of Oral Condition
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wirth, R.; Streicher, M.; Smoliner, C.; Kolb, C.; Hiesmayr, M.; Thiem, U.; Sieber, C.C.; Volkert, D. The impact of weight loss and low BMI on mortality of nursing home residents—Results from the nutritionDay in nursing homes. Clin. Nutr. 2016, 35, 900–906. [Google Scholar] [CrossRef]
- He, W.; Goodkind, D.; Kowal, P. An Aging World 2015; International Population Reports; U.S. Government Publishing Office: Washington, DC, USA, 2016; p. 12.
- Arai, H.; Ouchi, Y.; Yokode, M.; Ito, H.; Uematsu, H.; Eto, F.; Oshima, S.; Ota, K.; Saito, Y.; Sasaki, H.; et al. Toward the realization of a better aged society: Messages from gerontology and geriatrics. Geriatr. Gerontol. Int. 2012, 12, 16–22. [Google Scholar] [CrossRef] [PubMed]
- Health and Welfare Bureau for the Elderly Ministry of Health, Labour and Welfare. Long-Term Care Insurance System of Japan. Available online: https://www.mhlw.go.jp/english/policy/care-welfare/care-welfare-elderly/dl/ltcisj_e.pdf (accessed on 17 September 2021).
- Flynn, E.; Smith, C.H.; Walsh, C.D.; Walshe, M. Modifying the consistency of food and fluids for swallowing difficulties in dementia. Cochrane Database Syst. Rev. 2018, 9, Cd011077. [Google Scholar] [CrossRef]
- Edahiro, A.; Hirano, H.; Yamada, R.; Chiba, Y.; Watanabe, Y. Comparative study of eating behavior in elderly patients with Alzheimer’s disease and vascular dementia: A first report—Comparison of disturbed eating behavior. Nihon Ronen Igakkai Zasshi Jpn. J. Geriatr. 2013, 50, 651–660. [Google Scholar] [CrossRef] [PubMed]
- Kuzuya, M. Nutritional assessment and nutritional management for the elderly. Nippon Ronen Igakkai Zasshi. Jpn. J. Geriatr. 2003, 40, 199–203. [Google Scholar] [CrossRef]
- Robbins, J.; Gensler, G.; Hind, J.; Logemann, J.A.; Lindblad, A.S.; Brandt, D.; Baum, H.; Lilienfeld, D.; Kosek, S.; Lundy, D.; et al. Comparison of 2 interventions for liquid aspiration on pneumonia incidence: A randomized trial. Ann. Intern. Med. 2008, 148, 509–518. [Google Scholar] [CrossRef] [PubMed]
- Painter, V.; Le Couteur, D.; Waite, L. Texture-modified food and fluids in dementia and residential aged care facilities. Clin. Interv. Aging 2017, 12, 1193–1203. [Google Scholar] [CrossRef]
- Keller, H.; Chambers, L.; Niezgoda, H.; Duizer, L. Issues associated with the use of modified texture foods. J. Nutr. Health Aging 2012, 16, 195–200. [Google Scholar] [CrossRef] [PubMed]
- Germain, I.; Dufresne, T.; Gray-Donald, K. A novel dysphagia diet improves the nutrient intake of institutionalized elders. J. Am. Diet Assoc. 2006, 106, 1614–1623. [Google Scholar] [CrossRef]
- Dietitians Association of Australia; The Speech Pathology Association of Australia Limited. Texture-modified foods and thickened fluids as used for individuals with dysphagia: Australian standardised labels and definitions. Nutr. Diet 2007, 64, S53–S76. [Google Scholar] [CrossRef]
- Mahoney, F.I.; Barthel, D.W. Functional Evaluation: The Barthel Index. Md. State Med. J. 1965, 14, 61–65. [Google Scholar]
- Morris, J.C. The Clinical Dementia Rating (CDR): Current version and scoring rules. Neurology 1993, 43, 2412–2414. [Google Scholar] [CrossRef]
- Matsuo, K.; Fujishima, I. Textural changes by mastication and proper food texture for patients with oropharyngeal dysphagia. Nutrients 2020, 12, 1613. [Google Scholar] [CrossRef] [PubMed]
- Fujitani, J.; Uyama, R.; Oogosi, H. Japanese Dysphagia Diet 2013 by the JSDR dysphagia diet committee (JDD2013). Dysphagia Rehabil. 2013, 17, 255–267. [Google Scholar]
- Ohkuma, R.; Fjishima, I.; Kojima, C.; Hojo, K.; Takedhara, I.; Motohashi, Y. Development of a questionnaire to screen dysphagia. Jpn. J. Dysphagia Rehabil. 2002, 6, 3–8. [Google Scholar]
- Ohkuma, R.; Fjishima, I. Development of a The Relationship between the Seirei Questionnaire of Swallowing and 30 ml Water Swallowing Test. Jpn. J. Dysphagia Rehabil. 2012, 16, 192–197. [Google Scholar]
- Kawashima, K.; Motohashi, Y.; Fujishima, I. Prevalence of dysphagia among community-dwelling elderly individuals as estimated using a questionnaire for dysphagia screening. Dysphagia 2004, 19, 266–271. [Google Scholar] [CrossRef] [PubMed]
- Wallace, J.I.; Schwartz, R.S.; LaCroix, A.Z.; Uhlmann, R.F.; Pearlman, R.A. Involuntary weight loss in older outpatients: Incidence and clinical significance. J. Am. Geriatr. Soc. 1995, 43, 329–337. [Google Scholar] [CrossRef]
- De Stefani, F.D.C.; Pietraroia, P.S.; Fernandes-Silva, M.M.; Faria-Neto, J.; Baena, C.P. Observational evidence for unintentional weight loss in all-cause mortality and major cardiovascular events: A systematic review and meta-analysis. Sci. Rep. 2018, 8, 154. [Google Scholar] [CrossRef]
- Gazewood, J.D.; Mehr, D.R. Diagnosis and management of weight loss in the elderly. J. Fam. Pract. 1998, 47, 19–25. [Google Scholar]
- Nishida, Y.; Tanaka, S.; Nakae, S.; Yamada, Y.; Shirato, H.; Hirano, H.; Sasaki, S.; Katsukawa, F. Energy Gap between Doubly Labeled Water-Based Energy Expenditure and Calculated Energy Intake from Recipes and Plate Waste, and Subsequent Weight Changes in Elderly Residents in Japanese Long-Term Care Facilities: CLEVER Study. Nutrients 2020, 12, 2677. [Google Scholar] [CrossRef] [PubMed]
- Valentini, L.; Schindler, K.; Schlaffer, R.; Bucher, H.; Mouhieddine, M.; Steininger, K.; Tripamer, J.; Handschuh, M.; Schuh, C.; Volkert, D.; et al. The first nutritionDay in nursing homes: Participation may improve malnutrition awareness. Clin. Nutr. 2009, 28, 109–116. [Google Scholar] [CrossRef]
- Watanabe, I. Masticatory function and life style in aged. Nihon Ronen Igakkai Zasshi Jpn. J. Geriatr. 1998, 35, 194–200. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Saka, B.; Kaya, O.; Ozturk, G.B.; Erten, N.; Karan, M.A. Malnutrition in the elderly and its relationship with other geriatric syndromes. Clin. Nutr. 2010, 29, 745–748. [Google Scholar] [CrossRef] [PubMed]
- McKendry, J.; Currier, B.S.; Lim, C.; McLeod, J.C.; Thomas, A.C.Q.; Phillips, S.M. Nutritional supplements to support resistance exercise in countering the sarcopenia of aging. Nutrients 2020, 12, 2057. [Google Scholar] [CrossRef]
- Azzolino, D.; Passarelli, P.C.; De Angelis, P.; Piccirillo, G.B.; D’Addona, A.; Cesari, M. Poor Oral Health as a Determinant of Malnutrition and Sarcopenia. Nutrients 2019, 11, 2898. [Google Scholar] [CrossRef]
- Motokawa, K.; Yasuda, J.; Mikami, Y.; Edahiro, A.; Morishita, S.; Shirobe, M.; Ohara, Y.; Nohara, K.; Hirano, H.; Watanabe, Y. The Mini Nutritional Assessment-Short Form as a predictor of nursing home mortality in Japan: A 30-month longitudinal study. Arch. Gerontol. Geriatr. 2020, 86, 103954. [Google Scholar] [CrossRef]
- Park, M.; Song, J.A.; Lee, M.; Jeong, H.; Lim, S.; Lee, H.; Kim, C.G.; Kim, J.S.; Kim, K.S.; Lee, Y.W.; et al. National study of the nutritional status of Korean older adults with dementia who are living in long-term care settings. Jpn. J. Nurs. Sci. 2018, 15, 318–329. [Google Scholar] [CrossRef]
- Chiesi, F.; Grazzini, M.; Innocenti, M.; Giammarco, B.; Simoncini, E.; Garamella, G.; Zanobini, P.; Perra, C.; Baggiani, L.; Lorini, C.; et al. Older people living in nursing homes: An oral health screening survey in Florence, Italy. Int. J. Environ. Res. Public Health 2019, 16, 3492. [Google Scholar] [CrossRef]


{kind=link}
| Variable | Overall (n = 455) | Dysphagia Diet (n = 171) | Regular Diet (n = 284) | p Value | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Median (Q1, Q3) | Mean ± SD | Median (Q1, Q3) | Mean ± SD | Median (Q1, Q3) | ||||||||
| n (%) | n (%) | n (%) | |||||||||||
| Age (years) | 86.5 | ± | 7.8 | 87.0 (82.0, 93.0) | 87.5 | ± | 7.7 | 88.0 (83.0, 93.0) | 85.9 | ± | 7.9 | 87.0 (81.0, 92.0) | 0.035 |
| Sex (female) | 370 | (81.3) | 139 | (81.3) | 231 | (81.3) | 1.000 | ||||||
| Weight (kg) | 46.1 | ± | 8.7 | 45.2 (40.1, 51.9) | 42.7 | ± | 6.8 | 42.7 (38.0, 47.7) | 48.1 | ± | 7.9 | 47.4 (41.7, 53.4) | <0.001 |
| Weight loss ≥5% | 130 | (28.6) | 50 | (29.4) | 80 | (28.2) | 0.830 | ||||||
| Barthel Index | 33.7 | ± | 26.2 | 30.0 (10.0, 50.0) | 16.5 | ± | 19.0 | 10.0 (00.0, 25.0) | 44.0 | ± | 24.4 | 45.0 (25.0, 60.0) | <0.001 |
| Clinical Dementia Rating | |||||||||||||
| 0 | 9 | (2.0) | 2 | (1.1) | 7 | (2.7) | <0.001 | ||||||
| 0.5 | 37 | (8.2) | 20 | (2.1) | 33 | (12.7) | |||||||
| 1 | 93 | (20.7) | 33 | (10.0) | 74 | (28.6) | |||||||
| 2 | 133 | (29.6) | 37 | (25.3) | 85 | (32.8) | |||||||
| 3 | 177 | (39.4) | 65 | (61.6) | 60 | (23.2) | |||||||
| Total energy intake (kcal/day) | 1261.0 | ± | 215.9 | 1254.0 (1108.3, 1400.0) | 1250.0 | ± | 233.0 | 1230.0 (1100.0, 1400.0) | 1268.4 | ± | 204.1 | 1270.0 (1134.0, 1400.0) | 0.271 |
| Oral conditions | |||||||||||||
| Dysphagia screening rating | |||||||||||||
| No dysphagia | 97 | (21.3) | 17 | (9.9) | 79 | (27.8) | <0.001 | ||||||
| At risk of dysphagia | 175 | (38.5) | 43 | (25.1) | 129 | (45.4) | |||||||
| Possibility of dysphagia | 183 | (40.2) | 111 | (46.9) | 76 | (26.8) | |||||||
| Present teeth | 8.3 | ± | 8.9 | 5.0 (0.0, 16.0) | 5.8 | ± | 7.5 | 3.0 (0.0, 10.25) | 9.9 | ± | 9.4 | 7.0 (0.0, 18.0) | <0.001 |
| Functional teeth | 20.1 | ± | 10.2 | 26.0 (13.0, 28.0) | 15.3 | ± | 11.7 | 16.5 (2.0, 28.0) | 23.0 | ± | 7.9 | 27.5 (20.8, 28.0) | <0.001 |
| Edentulous | 155 | (34.3) | 75 | (44.1) | 80 | (28.4) | 0.001 | ||||||
| Prosthesis use | 243 | (53.8) | 71 | (41.8) | 172 | (61.0) | <0.001 | ||||||
| Medical history | |||||||||||||
| Pneumonia | 32 | (7.0) | 24 | (14.0) | 8 | (2.8) | <0.001 | ||||||
| Stroke | 154 | (33.9) | 53 | (31.0) | 101 | (35.7) | 0.357 | ||||||
| Diabetes mellitus | 66 | (14.5) | 26 | (15.2) | 40 | (14.1) | 0.784 | ||||||
| Depression | 33 | (7.3) | 9 | (5.3) | 24 | (8.5) | 0.263 | ||||||
| Variable | Regular Diet 2018 (n = 284) | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| Weight Loss <5% (n = 204) | Weight Loss ≥5% (n = 80) | p Value | |||||||
| Mean ± SD | Median, (Q1, Q3) | Mean ± SD | Median (Q1, Q3) | ||||||
| n (%) | n (%) | ||||||||
| Age (years) | 85.6 | ± | 7.9 | 86.0 (80.0, 92.0) | 86.7 | ± | 7.8 | 87.0 (82.5, 92.8) | 0.335 |
| Sex (female) | 167 | (81.9) | 64 | (80.0) | 0.736 | ||||
| Weight (kg) | 47.7 | ± | 6.2 | 47.1 (40.9, 53.4) | 49.1 | ± | 8.7 | 48.1 (42.4, 54.6) | 0.214 |
| Barthel Index | 44.6 | ± | 25.3 | 45.0 (25.0, 65.0) | 42.6 | ± | 22.2 | 45.0 (25.0, 60.0) | 0.583 |
| Clinical Dementia Rating | |||||||||
| 0 | 8 | (3.9) | 0 | (0.0) | |||||
| 0.5 | 30 | (14.7) | 4 | (5.1) | 0.058 | ||||
| 1 | 54 | (26.5) | 25 | (31.6) | |||||
| 2 | 64 | (31.4) | 31 | (39.2) | |||||
| 3 | 48 | (23.5) | 19 | (24.1) | |||||
| Total energy intake (kcal/day) | 1269.8 | ± | 199.5 | 1254.5 (1136.8, 1400.0) | 1264.7 | ± | 216.8 | 1302.0 (1100.0, 1400.0) | 0.938 |
| Oral conditions | |||||||||
| Dysphagia screening rating | |||||||||
| No dysphagia | 58 | (28.4) | 21 | (26.3) | 0.564 | ||||
| At risk of dysphagia | 95 | (46.6) | 34 | (42.5) | |||||
| Possibility of dysphagia | 51 | (25.0) | 25 | (31.3) | |||||
| Present teeth | 9.6 | ± | 9.3 | 7.0 (0.0, 18.0) | 10.5 | ± | 9.6 | 7.5 (0.0, 20.0) | 0.497 |
| Functional teeth | 23.2 | ± | 7.7 | 28.0 (21.8, 28.0) | 22.3 | ± | 8.4 | 27.0 (20.0, 28.0) | 0.274 |
| Edentulous | 58 | (28.7) | 22 | (27.5) | 0.884 | ||||
| Prosthesis use | 128 | (63.4) | 44 | (55.0) | 0.223 | ||||
| Medical History | |||||||||
| Pneumonia | 4 | (2.0) | 4 | (5.0) | 0.228 | ||||
| Stroke | 72 | (35.5) | 29 | (36.3) | 0.891 | ||||
| Diabetes mellitus | 30 | (14.8) | 10 | (12.5) | 0.707 | ||||
| Depression | 19 | (9.49) | 5 | (6.3) | 0.484 | ||||
| Variable (Change/Year) | Overall (n = 284) | Weight Loss <5% (n = 204) | Weight Loss ≥5% (n = 80) | p Value | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | Median (Q1, Q3) | Mean ± SD | Median (Q1, Q3) | Mean ± SD | Median (Q1, Q3) | ||||||||
| n (%) | n (%) | n (%) | |||||||||||
| Barthel Index | −5.2 | ± | 15.8 | −5.0 (−15.0, 5.0) | −3.3 | ± | 15.5 | 0.0 (−10.0, 5.0) | −10.0 | ± | 15.6 | −5.0 (−20.0, 0.0) | 0.003 |
| Clinical Dementia Rating deterioration | +86 | (+30.3) | +56 | (+27.5) | +30 | (+37.5) | 0.114 | ||||||
| Total energy intake (kcal/day) | +13.1 | ± | 203.1 | 0.0 (−100.0, 100.0) | +28.6 | ± | 183.8 | 0.0 (−75.0, 107.0) | −23.5 | ± | 240.2 | 0.0 (−187.8, 79.0) | 0.095 |
| Dysphagia screening rating deterioration | +91 | (+32.0) | +61 | (+29.9) | +30 | (+37.5) | 0.258 | ||||||
| Functional teeth | −1.1 | ± | 5.8 | 0.0 (0.0, 0.0) | −1.0 | ± | 5.9 | 0.0 (0.0, 0.0) | −1.4 | ± | 5.4 | 0.0 (−2.0, 0.0) | 0.151 |
| Food form (Dysphagia diet) | +55 | (+19.4) | +27 | (+13.2) | +28 | (+35.0) | <0.001 | ||||||
| OR | 95% CI | p Value | |||
|---|---|---|---|---|---|
| Age (years) | 1.03 | 0.98 | – | 1.07 | 0.232 |
| Sex (female) | 1.21 | 0.49 | – | 2.95 | 0.683 |
| Weight (kg) Baseline | 1.04 | 1.00 | – | 1.08 | 0.031 |
| Barthel Index change | 0.97 | 0.95 | – | 0.99 | 0.009 |
| Clinical Dementia Rating deterioration | 1.07 | 0.54 | – | 2.10 | 0.852 |
| Total energy intake change (kcal/day) | 1.00 | 1.00 | 1.00 | 0.407 | |
| Food form change (to dysphagia diet) | 3.02 | 1.41 | – | 6.46 | 0.004 |
| Dysphagia screening rating deterioration | 1.02 | 0.52 | – | 1.97 | 0.962 |
| Functional teeth change | 0.99 | 0.94 | – | 1.04 | 0.680 |
| Pneumonia | 2.42 | 0.46 | – | 12.83 | 0.299 |
| Stroke | 1.13 | 0.59 | – | 2.15 | 0.711 |
| Diabetes mellitus | 0.78 | 0.30 | – | 2.04 | 0.612 |
| Depression | 1.11 | 0.34 | – | 3.64 | 0.863 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Endo, A.; Watanabe, Y.; Matsushita, T.; Okada, K.; Ohara, Y.; Iwasaki, M.; Ito, K.; Nakajima, J.; Iwasa, Y.; Itoda, M.; et al. Association between Weight Loss and Food Form in Older Individuals Residing in Long-Term Care Facilities: 1-Year Multicenter Longitudinal Study. Int. J. Environ. Res. Public Health 2021, 18, 10776. https://doi.org/10.3390/ijerph182010776
Endo A, Watanabe Y, Matsushita T, Okada K, Ohara Y, Iwasaki M, Ito K, Nakajima J, Iwasa Y, Itoda M, et al. Association between Weight Loss and Food Form in Older Individuals Residing in Long-Term Care Facilities: 1-Year Multicenter Longitudinal Study. International Journal of Environmental Research and Public Health. 2021; 18(20):10776. https://doi.org/10.3390/ijerph182010776
Chicago/Turabian StyleEndo, Akemi, Yutaka Watanabe, Takae Matsushita, Kazutaka Okada, Yuki Ohara, Masanori Iwasaki, Kayoko Ito, Junko Nakajima, Yasuyuki Iwasa, Masataka Itoda, and et al. 2021. "Association between Weight Loss and Food Form in Older Individuals Residing in Long-Term Care Facilities: 1-Year Multicenter Longitudinal Study" International Journal of Environmental Research and Public Health 18, no. 20: 10776. https://doi.org/10.3390/ijerph182010776
APA StyleEndo, A., Watanabe, Y., Matsushita, T., Okada, K., Ohara, Y., Iwasaki, M., Ito, K., Nakajima, J., Iwasa, Y., Itoda, M., Sasaki, R., Nishi, Y., Furuya, J., Watanabe, Y., Umemoto, G., Kishima, M., Hirano, H., Sato, Y., Yoshida, M., & Yamazaki, Y. (2021). Association between Weight Loss and Food Form in Older Individuals Residing in Long-Term Care Facilities: 1-Year Multicenter Longitudinal Study. International Journal of Environmental Research and Public Health, 18(20), 10776. https://doi.org/10.3390/ijerph182010776