
Functional and Anthropometrical Screening Test among High Performance Female Football Players: A Descriptive Study with Injury Incidence Analysis, the Basque Female Football Cohort (BFFC) Study


 , , ,
, , ,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Data Collection
2.2.1. Anthropometrics
2.2.2. Range of Motion (ROM) Measurements
2.2.3. Hand-Held Dynamometry (HHD)
2.2.4. Core Musculature Functional Evaluation
2.2.5. Jumping Biomechanics Assessment
2.3. Injury Surveillance Assessment
2.4. Statistical Analysis
3. Results
3.1. Anthropometrics
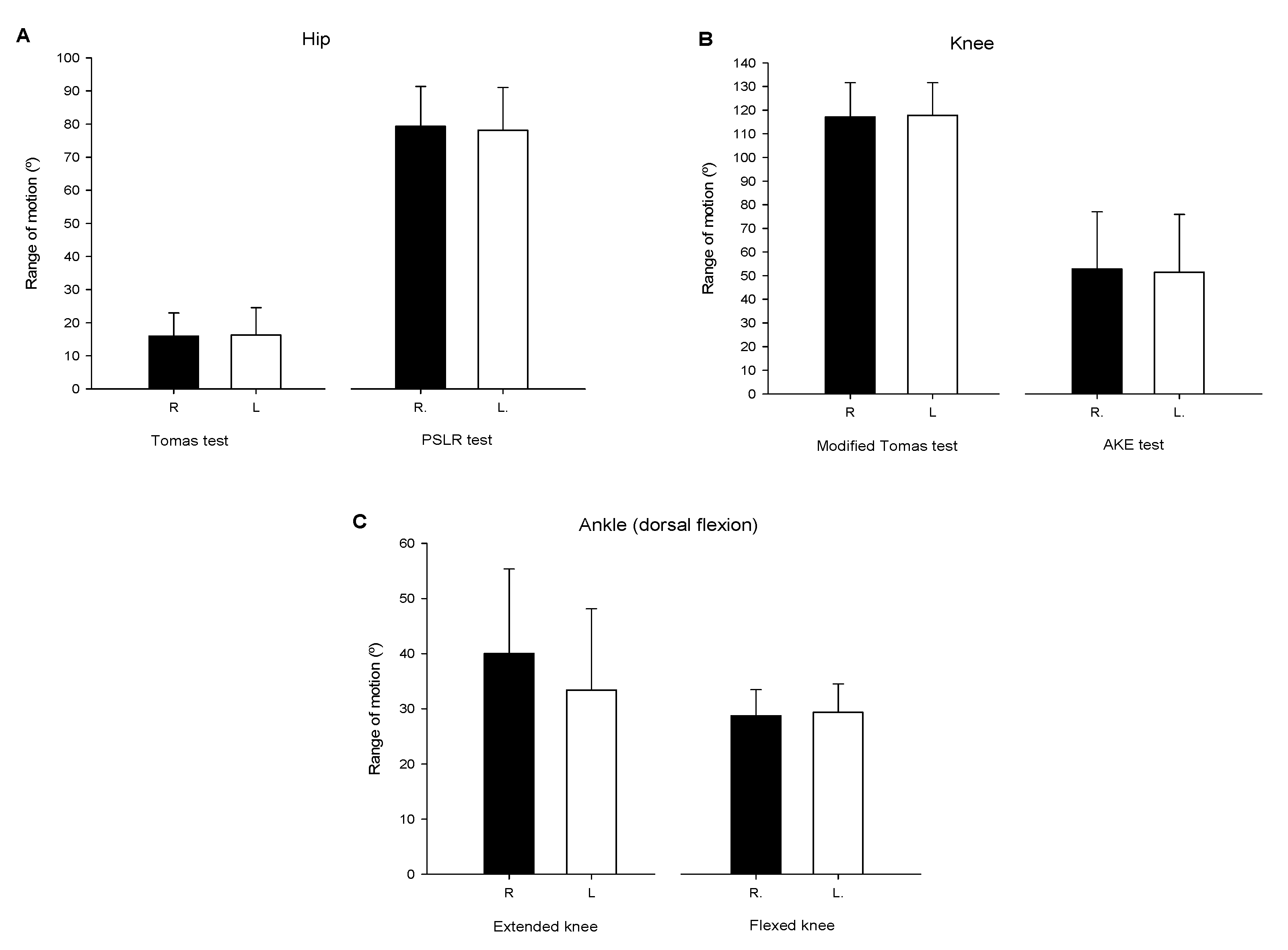
3.2. ROM Measurements
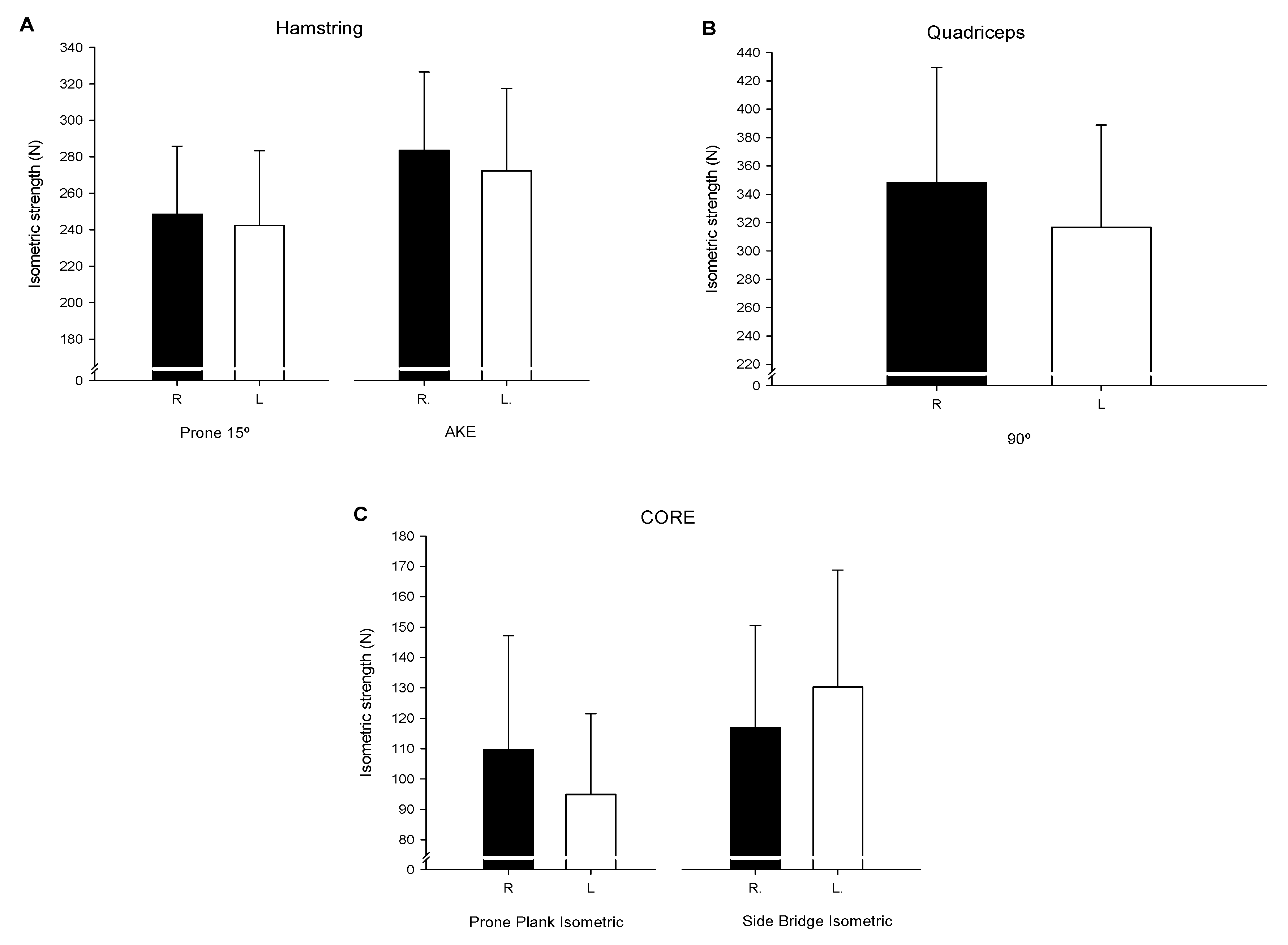
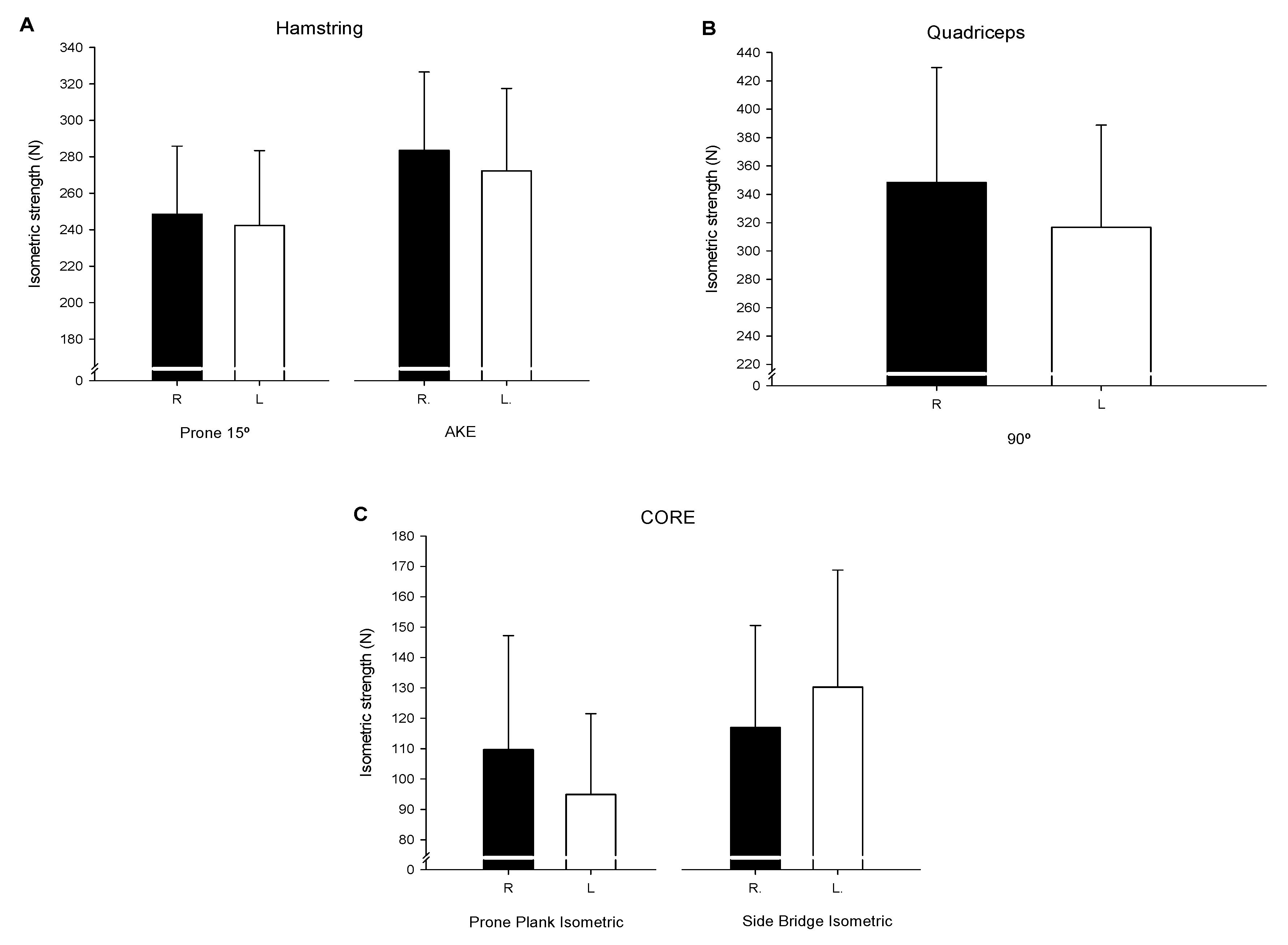
3.3. HHD Strength Evaluations
3.4. Jumping Biomechanics
3.4.1. Vertical Bilateral Drop Jump (VBDJ) & Vertical Unilateral Drop Jump (VUDJ)
3.4.2. Cross over Hop for Distance (COHD)
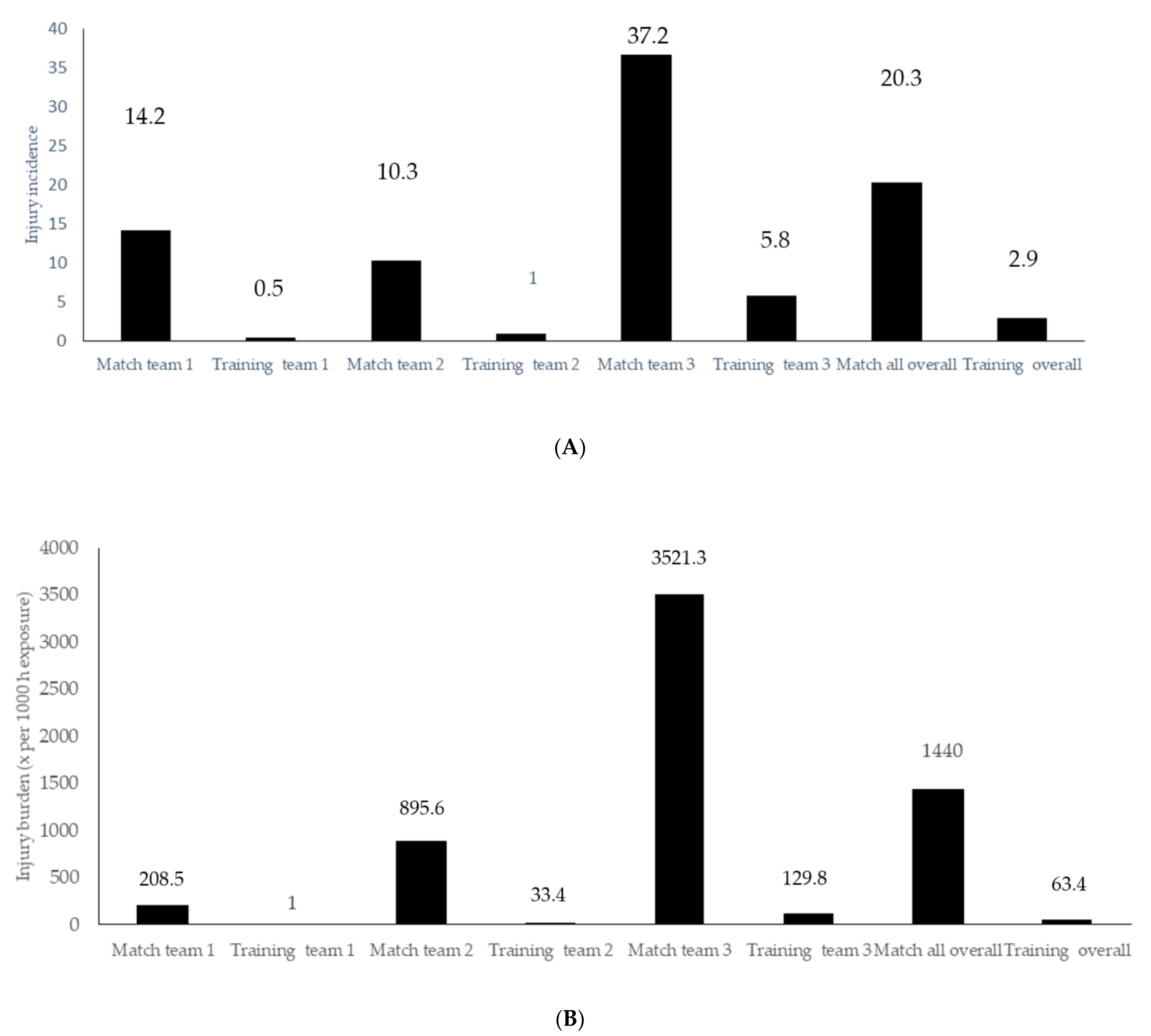
3.5. Injury Surveillance Assessment
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Alahmad, T.A.; Kearney, P.; Cahalan, R. Injury in elite women’s soccer: A systematic review. Phys. Sportsmed. 2020, 48, 259–265. [Google Scholar] [CrossRef] [PubMed]
- Mercieca, F.; Cumbo, R.K.; Seychell, D. An Overview of Injuries in Senior Women’s Football in Malta. MCAST J. Appl. Res. Pract. 2020, 4, 180–201. [Google Scholar] [CrossRef]
- Woods, C.; Hawkins, R.; Hulse, M.; Hodson, A. The Football Association Medical Research Programme—Analysis of preseaon injuries. Br. J. Sports Med. 2002, 36, 436–441. [Google Scholar] [CrossRef] [Green Version]
- Biedert, R.M.; Bachmann, M. Frauenfußball. Verletzungen, risiken und prävention. Orthopade 2005, 34, 448–453. [Google Scholar] [CrossRef]
- Mark, A. Science and Soccer: Developing Elite Performers. Angew. Chem. Int. Ed. 1967, 6, 951–952. [Google Scholar]
- Martínez-Lagunas, V.; Niessen, M.; Hartmann, U. Women’s football: Player characteristics and demands of the game. J. Sport Health Sci. 2014, 3, 258–272. [Google Scholar] [CrossRef] [Green Version]
- Järvinen, T.A.H.; Järvinen, T.L.N.; Kääriäinen, M.; Äärimaa, V.; Vaittinen, S.; Kalimo, H.; Järvinen, M. Muscle injuries: Optimising recovery. Best Pract. Res. Clin. Rheumatol. 2007, 21, 317–331. [Google Scholar] [CrossRef]
- Barber-Westin, S.D.; Noyes, F.R.; Smith, S.T.; Campbell, T.M. Reducing the risk of noncontact anterior cruciate ligament injuries in the female athlete. Phys. Sportsmed. 2009, 37, 49–61. [Google Scholar] [CrossRef]
- Iaia, M.F.; Rampinini, E.; Bangsbo, J. High-intensity training in football. Int. J. Sports Physiol. Perform. 2009, 4, 291–306. [Google Scholar] [CrossRef] [Green Version]
- Agustín, R.M.S.; Medina-Mirapeix, F.; Esteban-Catalán, A.; Escriche-Escuder, A.; Sánchez-Barbadora, M.; Benítez-Martínez, J.C. Epidemiology of injuries in first division Spanish women’s soccer players. Int. J. Environ. Res. Public Health 2021, 18, 3009. [Google Scholar] [CrossRef]
- Faude, O.; Junge, A.; Kindermann, W.; Dvorak, J. Risk factors for injuries in elite female soccer players. Br. J. Sports Med. 2006, 40, 785–790. [Google Scholar] [CrossRef] [Green Version]
- Lewis, T. GradDipPhys MCSP is a clinical physiotherapy specialist (musculoskeletal service) in the physiotherapy department at The Royal. Physiother. Sept. 2000, 86, 464–472. [Google Scholar] [CrossRef]
- Griffin, J.; Horan, S.; Keogh, J.; Dodd, K.; Andreatta, M.; Minahan, C. Contextual factors influencing the characteristics of female football players. J. Sports Med. Phys. Fit. 2021, 61, 218–232. [Google Scholar] [CrossRef]
- Nilstad, A.; Andersen, T.E.; Bahr, R.; Holme, I.; Steffen, K. Risk factors for lower extremity injuries in elite female soccer players. Am. J. Sports Med. 2014, 42, 940–948. [Google Scholar] [CrossRef]
- Östenberg, A.; Roos, H. Injury risk factors in female European football. A prospective study of 123 players during one season. Scand. J. Med. Sci. Sports 2000, 10, 279–285. [Google Scholar] [CrossRef]
- Söderman, K.; Alfredson, H.; Pietilä, T.; Werner, S. Risk factors for leg injuries in female soccer players: A prospective investigation during one out-door season. Knee Surg. Sports Traumatol. Arthrosc. 2001, 9, 313–321. [Google Scholar] [CrossRef]
- Nilstad, A.; Krosshaug, T.; Mok, K.M.; Bahr, R.; Andersen, T.E. Association between anatomical characteristics, knee laxity, muscle strength, and peak knee valgus during vertical drop-jump landings. J. Orthop. Sports Phys. Ther. 2015, 45, 998–1005. [Google Scholar] [CrossRef]
- Ekstrand, J. Epidemiology of football injuries. Sci. Sports 2008, 23, 73–77. [Google Scholar] [CrossRef] [Green Version]
- Pedersen, A.V.; Aksdal, I.M.; Stalsberg, R. Scaling demands of soccer according to anthropometric and physiological sex differences: A fairer comparison of men’s and women’s soccer. Front. Psychol. 2019, 10, 762. [Google Scholar] [CrossRef] [Green Version]
- Kammoun, M.M.; Trabelsi, O.; Gharbi, A.; Masmoudi, L.; Ghorbel, S.; Tabka, Z.; Chamari, K. Anthropometric and physical fitness profiles of tunisian female soccer players: Associations with field position. Acta Gymnica 2020, 50, 130–137. [Google Scholar] [CrossRef]
- Steffen, K.; Nilstad, A.; Krosshaug, T.; Pasanen, K.; Killingmo, A.; Bahr, R. No association between static and dynamic postural control and ACL injury risk among female elite handball and football players: A prospective study of 838 players. Br. J. Sports Med. 2017, 51, 253–259. [Google Scholar] [CrossRef]
- Villaseca-Vicuña, R.; Molina-Sotomayor, E.; Zabaloy, S.; Gonzalez-Jurado, J.A. Anthropometric profile and physical fitness performance comparison by game position in the Chile women’s senior national football team. Appl. Sci. 2021, 11, 2004. [Google Scholar] [CrossRef]
- Marfell-Jones, M.; Stewart, A.; Olds, T. Kinanthropometry IXnull; Taylor & Francis: Abingdon-on-Thames, UK, 2006. [Google Scholar]
- Grazioli, R.; Lopez, P.; Machado, C.L.F.; Farinha, J.B.; Fagundes, A.O.; Voser, R.; Reischak-Oliveira, Á.; Setuain, I.; Izquierdo, M.; Pinto, R.S.; et al. Moderate volume of sprint bouts does not induce muscle damage in well-trained athletes. J. Bodyw. Mov. Ther. 2020, 24, 206–211. [Google Scholar] [CrossRef]
- Casajus, J.; Aragones, M. Estudio morfologico del futbolista de alto nivel. Composicion corporal y somatotipo. Arch. Med. Deport. 1991, 8, 00147–00152. [Google Scholar]
- Jackson, A.S.; Pollock, M.L. Generalized equations for predicting body density of men. Br. J. Nutr. 1978, 40, 497–504. [Google Scholar] [CrossRef] [Green Version]
- Setuain, I.; Izquierdo, M.; Idoate, F.; Bikandi, E.; Gorostiaga, E.M.; Aagaard, P.; Cadore, E.L.; Alfaro-Adrián, J. Differential effects of 2 rehabilitation programs following anterior cruciate ligament reconstruction. J. Sport Rehabil. 2017, 26, 544–555. [Google Scholar] [CrossRef]
- Bohannon, R.W. Hand-held compared with isokinetic dynamometry for measurement of static knee extension torque (parallel reliability of dynamometers). Clin. Phys. Physiol. Meas. 1990, 11, 217–222. [Google Scholar] [CrossRef]
- Harvey, D. Assessment of the flexibility of elite athletes using the modified Thomas test. Br. J. Sports Med. 1998, 32, 68–70. [Google Scholar] [CrossRef] [Green Version]
- Konor, M.M.; Morton, S.; Eckerson, J.M.; Grindstaff, T.L. Reliability of Three Measures of Ankle. Int. J. Sports Phys. Ther. 2012, 7, 279–287. [Google Scholar]
- Whiteley, R.; Jacobsen, P.; Prior, S.; Skazalski, C.; Otten, R.; Johnson, A. Correlation of isokinetic and novel hand-held dynamometry measures of knee flexion and extension strength testing. J. Sci. Med. Sport 2012, 15, 444–450. [Google Scholar] [CrossRef]
- Toonstra, J.; Mattacola, C.G. Test-retest reliability and validity of isometric knee-flexion and -extension measurement using 3 methods of assessing muscle strength. J. Sport Rehabil. 2013, 22, 1–5. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Etxaleku, S.; Izquierdo, M.; Bikandi, E.; Arroyo, J.G.; Sarriegi, I.; Sesma, I.; Setuain, I. Validation and application of two new core stability tests in professional football. Appl. Sci. 2020, 10, 5495. [Google Scholar] [CrossRef]
- Setuain, I.; Martinikorena, J.; Gonzalez-Izal, M.; Martinez-Ramirez, A.; Gómez, M.; Alfaro-Adrián, J.; Izquierdo, M. Vertical jumping biomechanical evaluation through the use of an inertial sensor-based technology. J. Sports Sci. 2016, 34, 843–851. [Google Scholar] [CrossRef] [PubMed]
- Noyes, F.R.; Barber, S.D.; Mangine, R.E. Abnormal lower limb symmetry determined by function hop tests after anterior cruciate ligament rupture. Am. J. Sports Med. 1991, 19, 513–518. [Google Scholar] [CrossRef]
- Di Stasi, S.; Myer, G.D.; Hewett, T.E. Neuromuscular training to target deficits associated with second anterior cruciate ligament injury. J. Orthop. Sports Phys. Ther. 2013, 43, 777–792. [Google Scholar] [CrossRef] [Green Version]
- Setuain, I.; Bikandi, E.; Amú Ruiz, F.A.; Urtasun, F.; Izquierdo, M. Horizontal jumping biomechanics among elite female handball players with and without anterior cruciate ligament reconstruction: An ISU based study. BMC Sports Sci. Med. Rehabil. 2019, 11, 30. [Google Scholar] [CrossRef]
- Clarsen, B.; Rønsen, O.; Myklebust, G.; Flørenes, T.W.; Bahr, R. The Oslo sports trauma research center questionnaire on health problems: A new approach to prospective monitoring of illness and injury in elite athletes. Br. J. Sports Med. 2014, 48, 754–760. [Google Scholar] [CrossRef] [Green Version]
- Hägglund, M.; Waldén, M.; Bahr, R.; Ekstrand, J. Methods for epidemiological study of injuries to professional football players: Developing the UEFA model. Br. J. Sports Med. 2005, 39, 340–346. [Google Scholar] [CrossRef] [Green Version]
- Fuller, C.W.; Ekstrand, J.; Junge, A.; Andersen, T.E.; Bahr, R.; Dvorak, J.; Hägglund, M.; McCrory, P.; Meeuwisse, W.H. Consensus statement on injury definitions and data collection procedures in studies of football (soccer) injuries. Scand. J. Med. Sci. Sport. 2006, 16, 83–92. [Google Scholar] [CrossRef]
- Ingebrigtsen, J.; Dillem, T.; Shalfawi, S.A. Aerobic capacities and anthropometric characteristics of elite female soccer players. J. Strength Cond. Res. 2011, 25, 3352–3357. [Google Scholar] [CrossRef]
- López-Valenciano, A.; Ayala, F.; De Ste Croix, M.; Barbado, D.; Vera-Garcia, F.J. Different neuromuscular parameters influence dynamic balance in male and female football players. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 962–970. [Google Scholar] [CrossRef] [PubMed]
- Sugimoto, D.; Howell, D.R.; Tocci, N.X.; Meehan, W.P. Risk factors associated with self-reported injury history in female youth soccer players. Phys. Sportsmed. 2018, 46, 312–318. [Google Scholar] [CrossRef] [PubMed]
- Slimani, M.; Nikolaidis, P.T. Anthropometric and physiological characteristics of male soccer players according to their competitive level, playing position and age group: A systematic review. J. Sports Med. Phys. Fit. 2019, 141–163. [Google Scholar] [CrossRef] [PubMed]
- Queiroga, M.R.; da Silva, D.F.; Ferreira, S.A.; Weber, V.M.R.; Fernandes, D.Z.; Cavazzotto, T.G.; Portela, B.S.; Tartaruga, M.P.; Nascimento, M.A.; Vieira, E.R. Characterization of Reproductive and Morphological Variables in Female Elite Futsal Players. Front. Psychol. 2021, 12, 625354. [Google Scholar] [CrossRef] [PubMed]
- Nikolaidis, P. Physical Fitness in Female Soccer Players by Player Position: A Focus on Anaerobic Power. Hum. Mov. 2014, 15, 74–79. [Google Scholar] [CrossRef]
- Brooks, K.A.; Clark, S.L.; Dawes, J.J. Isokinetic Strength and Performance in Collegiate Women’s Soccer. J. Nov. Physiother. 2013, s3. [Google Scholar] [CrossRef]
- Garcia-Tabar, I.; Iturricastillo, A.; Castellano, J.; Cadore, E.L.; Izquierdo, M.; Setuain, I. Predicting Cardiorespiratory Fitness in Female Soccer Players. The Basque Female Football Cohort Study. Int. J. Sports Physiol. Perform. 2021, in press. [Google Scholar] [CrossRef]
- Raya-González, J.; Clemente, F.M.; Castillo, D. Analyzing the Magnitude of Interlimb Asymmetries in Young Female Soccer Players: A Preliminary Study. Int. J. Environ. Res. Public Health 2021, 18, 475. [Google Scholar] [CrossRef]
- Farley, J.B.; Keogh, J.W.L.; Woods, C.T.; Milne, N. Physical fitness profiles of female Australian football players across five competition levels. Sci. Med. Football 2021, in press. [Google Scholar] [CrossRef]
- Mentiplay, B.F.; Mosler, A.B.; Crossley, K.M.; Carey, D.L.; Sakadjian, K.; Bodger, R.; Shipperd, B.; Bruder, A.M. Lower limb musculoskeletal screening in elite female Australian football players. Phys. Ther. Sport 2019, 40, 33–43. [Google Scholar] [CrossRef]
- Paul, D.J.; Nassis, G.P.; Whiteley, R.; Marques, J.B.; Kenneally, D.; Chalabi, H. Actue responses of soccer match play on hip stregth and flexibility measures: Potential measure of injury risk. J. Sports Sci. 2014, 32, 1318–1323. [Google Scholar] [CrossRef]
- Andrade, M.D.S.; Mascarin, N.C.; Foster, R.; di Bella, Z.I.d.; Vancini, R.L.; de Lira, C.A.B. Is muscular strength balance influenced by menstrual cycle in female soccer players? J. Sports Med. Phys. Fit. 2017, 57, 859–864. [Google Scholar] [CrossRef]
- Hannon, J.P.; Wang-Price, S.; Garrison, J.C.; Goto, S.; Bothwell, J.M.; Bush, C.A. Normalized Hip and Knee Strength in Two Age Groups of Adolescent Female Soccer Players. J. Strength Cond. Res. 2019, 1–5. [Google Scholar] [CrossRef]
- Parpa, K.; Michaelides, M.A. The Effect of Transition Period on Performance Parameters in Elite Female Soccer Players. Int. J. Sports Med. 2020, 41, 528–532. [Google Scholar] [CrossRef]
- Ruas, C.V.; Minozzo, F.; Pinto, M.D.; Brown, L.E.; Pinto, R.S. Lower-extremity strength ratios of professional soccer players according to field position. J. Strength Cond. Res. 2015, 29, 1220–1226. [Google Scholar] [CrossRef]
- Karsten, B.; Baker, J.; Naclerio, F.; Klose, A.; Antonino, B.; Nimmerichter, A. Association Between the Force-Velocity Profile and Performance Variables Obtained in Jumping and Sprinting in Elite Female Soccer Players. Int. J. Sports Physiol. Perform. 2018, 14, 156–162. Available online: https://www.cochranelibrary.com/central/doi/10.1002/central/CN-01787161/full (accessed on 26 July 2020).
- Mujika, I.; Santisteban, J.; Impellizzeri, F.M.; Castagna, C. Fitness determinants of success in men’s and women’s football. J. Sports Sci. 2009, 27, 107–114. [Google Scholar] [CrossRef] [PubMed]
- Mok, K.M.; Petushek, E.; Krosshaug, T. Reliability of knee biomechanics during a vertical drop jump in elite female athletes. Gait Posture 2016, 46, 173–178. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arcos, A.L.; Yanci, J.; Mendiguchia, J.; Salinero, J.J.; Brughelli, M.; Castagna, C. Short-term training effects of vertically and horizontally oriented exercises on neuromuscular performance in professional soccer players. Int. J. Sports Physiol. Perform. 2014, 9, 480–488. [Google Scholar] [CrossRef] [PubMed]
- Read, P.J.; McAuliffe, S.; Bishop, C.; Oliver, J.L.; Graham-Smith, P.; Farooq, M.A. Asymmetry thresholds for common screening tests and their effects on jump performance in professional soccer players. J. Athl. Train. 2021, 56, 46–53. [Google Scholar] [CrossRef]
- Bishop, C.; Read, P.; McCubbine, J.; Turner, A. Vertical and Horizontal Asymmetries Are Related to Slower Sprinting and Jump Performance in Elite Youth Female Soccer Players. J. Strength Cond. Res. 2021, 35, 56–63. [Google Scholar] [CrossRef] [Green Version]
- Sprouse, B.; Alty, J.; Kemp, S.; Cowie, C.; Mehta, R.; Tang, A.; Morris, J.; Cooper, S.; Varley, I. The Football Association Injury and Illness Surveillance Study: The Incidence, Burden and Severity of Injuries and Illness in Men’s and Women’s International Football. Sports Med. 2020, 1–20. [Google Scholar] [CrossRef]
- Finch, C.F.; Twomey, D.M.; Fortington, L.V.; Doyle, T.L.A.; Elliott, B.C.; Akram, M.; Lloyd, D.G. Preventing australian football injuries with a targeted neuromuscular control exercise programme: Comparative injury rates from a training intervention delivered in a clustered randomised controlled trial. Inj. Prev. 2016, 22, 123–128. [Google Scholar] [CrossRef] [Green Version]
- Milanović, Z.; Sporiš, G.; James, N.; Trajković, N.; Ignjatović, A.; Sarmento, H.; Trecroci, A.; Mendes, B.M.B. Physiological Demands, Morphological Characteristics, Physical Abilities and Injuries of Female Soccer Players. J. Hum. Kinet. 2017, 60, 77–83. [Google Scholar] [CrossRef] [Green Version]
- Mayhew, L.; Johnson, M.I.; Francis, P.; Lutter, C.; Alali, A.; Jones, G. Incidence of injury in adult elite women’s football: A systematic review and meta-analysis. BMJ Open Sport Exerc. Med. 2021, 13, e001094. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Mean | SD | Min. | Max. | |
|---|---|---|---|---|
| Age | 21.9 | 4.9 | 15.3 | 36.6 |
| Body mass (kg) | 60.4 | 8.1 | 45.0 | 78.7 |
| Height (cm) | 163.8 | 6.7 | 152.0 | 183.0 |
| BMI (kg·m−2) | 22.7 | 2.2 | 18.9 | 29.6 |
| TL (cm) | 35.4 | 2.4 | 30.3 | 41.5 |
| FL (cm) | 36.4 | 3.2 | 29.6 | 44.8 |
| TL + FL (cm) | 71.7 | 4.8 | 59.8 | 85.8 |
| Pelvis with (cm) | 23.7 | 2.6 | 19.0 | 29.5 |
| Skinfold’s thickness | ||||
| Subscapularis (mm) | 11.2 | 3.4 | 6.8 | 19.7 |
| Triceps (mm) | 15.5 | 4.2 | 8.3 | 25.5 |
| Iliac Crest (mm) | 14.0 | 6.4 | 6.0 | 32.6 |
| Abdominal (mm) | 19.3 | 7.7 | 7.5 | 37.5 |
| Vastus Cruralis (mm) | 26.9 | 7.2 | 15.2 | 41.4 |
| Gastrocnemius (mm) | 12.8 | 5.8 | 4.0 | 31.0 |
| Ʃ skinfolds (mm) | 99.6 | 29.6 | 55.4 | 170.5 |
| % Body fat | 19.8 | 5.1 | 6.0 | 30.0 |
| Antero-Posterior Knee Laxity | ||||
| KT1000 D (mm) | 4.6 | 1.8 | 1.0 | 9.0 |
| KT1000 I (mm) | 5.3 | 1.8 | 2.0 | 9.5 |
| KT1000 LSI | 0.7 | 0.7 | −5.0 | 4.0 |
| Mean | SD | Min. | Max. | |
|---|---|---|---|---|
| Bilateral | ||||
| Height (cm) | 48 | 3 | 41 | 54 |
| Vf1 (N) | 3370.5 | 1442.0 | 1441.3 | 7630.0 |
| Vf2 (N) | 2644.5 | 1670.2 | 544.8 | 7194.0 |
| Vip (Ns) | 1342.1 | 695.1 | 522.5 | 4093.6 |
| Vf1 (N·kg−1) | 5.5 | 1.9 | 2.5 | 10.0 |
| Vf2 (N·kg−1) | 4.3 | 2.7 | 9.8 | 11.0 |
| Vip (N·kg−1) | 2.3 | 1.2 | 9.6 | 6.8 |
| Unilateral | ||||
| Height R (cm) | 17.6 | 2.4 | 12.3 | 23.0 |
| Height L (cm) | 18.2 | 2.7 | 13.0 | 28.0 |
| Vf1 R (N) | 1796.3 | 780.4 | 831.4 | 4073.5 |
| Vf1 L (N) | 1740.3 | 781.0 | 710.1 | 3723.7 |
| Vf1 R (N·BW−1) | 2.9 | 11.0 | 1.5 | 5.6 |
| Vf1 L (N·BW−1) | 2.8 | 11.5 | 10.4 | 62.6 |
| Vf2 R (N) | 2675.0 | 1030.3 | 1142.8 | 6623.6 |
| Vf2 L (N) | 2574.4 | 1051.4 | 818.3 | 6438.9 |
| Vf2 R (N·BW−1) | 4.4 | 1.5 | 1.8 | 9.0 |
| Vf 2 L (N·BW−1) | 4.2 | 1.4 | 14.2 | 8.8 |
| Vpi R (Ns·BW−1) | 1.7 | 0.2 | 1.3 | 2.1 |
| Vpi L (Ns·BW−1) | 1.7 | 0.2 | 1.2 | 2.2 |
| Mech power D (W·kg−1) | 14.3 | 2.8 | 7.9 | 22.2 |
| Mech power I (W·kg−1) | 14.7 | 2.7 | 9.4 | 22.3 |
| Vertical Bilateral Drop Jump | Mean | SD | Min. | Max. |
|---|---|---|---|---|
| Frontal plane | ||||
| I.C trunk lateral flexion (°) | −0.7 | 4.2 | −13.0 | 7.0 |
| I.C Knee valgus R (°) | 0.1 | 5.0 | −12.5 | 10.0 |
| I.C Knee valgus L (°) | −0.6 | 5.5 | −18.0 | 10.0 |
| Max Flex trunk lateral flexion (°) | −0.1 | 4.3 | −13.0 | 7.5 |
| Max Flex valgus R (°) | −7.8 | 17.4 | −53.0 | 21.5 |
| Max Flex valgus L (°) | −6.5 | 14.6 | −48.0 | 27.5 |
| Sagittal plane | ||||
| C.I trunk Flexion (°) | 42.7 | 10.2 | 24 | 67 |
| C.I knee Flexion (°) | 47.0 | 12.0 | 20.5 | 73 |
| Max Flex. Trunk Flexion (°) | 102.0 | 9.7 | 67.5 | 127.5 |
| Max Flex. Knee Flexion (°) | 102.7 | 20.6 | 61.5 | 176 |
| Mean | SD | Min. | Max. | |
|---|---|---|---|---|
| Vf R (N) | 3207.2 | 1280.2 | 1379.6 | 8007.2 |
| Vf L (N) | 3221.1 | 1141.7 | 1091.4 | 6287.6 |
| Vf R (N·BW−1) | 5.3 | 18.2 | 2.7 | 10.9 |
| Vf L (N·BW−1) | 5.3 | 1.7 | 2.3 | 9.4 |
| Hf R (N) | 184.0 | 49.4 | 105.9 | 306.5 |
| Hf L (N) | 188.7 | 53.5 | 97.7 | 335.1 |
| Hf R (N·BW−1) | 3.0 | 0.7 | 1.9 | 5.5 |
| Hf L (N·BW−1) | 3.1 | 0.8 | 1.9 | 5.4 |
| Distance R (cm) | 357.0 | 44.4 | 235.0 | 468.5 |
| Distance L (cm) | 349.7 | 54.4 | 154.0 | 432.0 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Álvarez-Zafra, M.; Yanci, J.; García-Tabar, I.; Bikandi, E.; Etxaleku, S.; Izquierdo, M.; Krosshaug, T.; Fernandez-Lasa, U.; Setuain, I. Functional and Anthropometrical Screening Test among High Performance Female Football Players: A Descriptive Study with Injury Incidence Analysis, the Basque Female Football Cohort (BFFC) Study. Int. J. Environ. Res. Public Health 2021, 18, 10658. https://doi.org/10.3390/ijerph182010658
Álvarez-Zafra M, Yanci J, García-Tabar I, Bikandi E, Etxaleku S, Izquierdo M, Krosshaug T, Fernandez-Lasa U, Setuain I. Functional and Anthropometrical Screening Test among High Performance Female Football Players: A Descriptive Study with Injury Incidence Analysis, the Basque Female Football Cohort (BFFC) Study. International Journal of Environmental Research and Public Health. 2021; 18(20):10658. https://doi.org/10.3390/ijerph182010658
Chicago/Turabian StyleÁlvarez-Zafra, Marta, Javier Yanci, Ibai García-Tabar, Eder Bikandi, Saioa Etxaleku, Mikel Izquierdo, Tron Krosshaug, Uxue Fernandez-Lasa, and Igor Setuain. 2021. "Functional and Anthropometrical Screening Test among High Performance Female Football Players: A Descriptive Study with Injury Incidence Analysis, the Basque Female Football Cohort (BFFC) Study" International Journal of Environmental Research and Public Health 18, no. 20: 10658. https://doi.org/10.3390/ijerph182010658
APA StyleÁlvarez-Zafra, M., Yanci, J., García-Tabar, I., Bikandi, E., Etxaleku, S., Izquierdo, M., Krosshaug, T., Fernandez-Lasa, U., & Setuain, I. (2021). Functional and Anthropometrical Screening Test among High Performance Female Football Players: A Descriptive Study with Injury Incidence Analysis, the Basque Female Football Cohort (BFFC) Study. International Journal of Environmental Research and Public Health, 18(20), 10658. https://doi.org/10.3390/ijerph182010658