An Innovative Approach to Designing Digital Health Solutions Addressing the Unmet Needs of Obese Patients in Europe

 ,
,  ,
,  ,
, 


Abstract
1. Introduction
2. Methodology
- Data analytics for predictive risk stratification and prevention;
- Proactive prevention through empowerment, self-management, monitoring, and coaching;
- Digital solutions for connected health;
- Digital support for integrated care.
3. Results
3.1. Health Policy and Obesity (World Health Organization (WHO), European Commission (EC), National, and Local)
3.2. Innovative Approaches to Address Obesity: A European Vision
3.3. Innovative Approaches to Address Obesity: The Italian Vision
Experiences of Italian Regions: Campania and Sicilia
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- The Lancet Diabetes & Endocrinology Tackling obesity in 2020—With a great resolution comes shared responsibility. Lancet Diabetes Endocrinol. 2020, 8, 89. [CrossRef]
- Han, T.S.; Tijhuis, M.A.; Lean, M.E.; Seidell, J.C. Quality of life in relation to overweight and body fat distribution. Am. J. Public Health 1998, 88, 1814–1820. [Google Scholar] [CrossRef] [PubMed]
- Fontaine, K.R.; Cheskin, L.J.; Barofsky, I. Health-related quality of life in obese persons seeking treatment. J. Fam. Pract. 1996, 43, 265–270. [Google Scholar] [PubMed]
- NHLBI Obesity Education Initiative Expert Panel on the Identification, Evaluation, and Treatment of Obesity in Adults (US). Clinical Guidelines on the Identification, Evaluation, and Treatment of Overweight and Obesity in Adults: The Evidence Report. National Heart, Lung, and Blood Institute, 1998. Available online: https://www.ncbi.nlm.nih.gov/books/NBK1988/ (accessed on 15 October 2020).
- The Global Health Observatory WHO (WHO). Body Mass Index (BMI), World Health Data Platform. Available online: https://www.who.int/data/gho/data/themes/theme-details/GHO/body-mass-index-(bmi) (accessed on 15 October 2020).
- Marques, A.; Peralta, M.; Naia, A.; Loureiro, N.; de Matos, M.G. Prevalence of adult overweight and obesity in 20 European countries, 2014. Eur. J. Public Health 2018, 28, 295–300. [Google Scholar] [CrossRef]
- Wilson, K. Obesity: Understanding Obesity. FP Essent.; 2020. Available online: https://pubmed.ncbi.nlm.nih.gov/32383843/ (accessed on 15 October 2020).
- Bray, G.A.; Kim, K.K.; Wilding, J.P.H. Obesity: A chronic relapsing progressive disease process. A position statement of the World Obesity Federation. Obes. Rev. 2017, 18, 715–723. [Google Scholar] [CrossRef]
- Ramos-Lopez, O.; Milagro, F.I.; Allayee, H.; Chmurzynska, A.; Choi, M.S.; Curi, R.; De Caterina, R.; Ferguson, L.R.; Goni, L.; Kang, J.X.; et al. Guide for Current Nutrigenetic, Nutrigenomic, and Nutriepigenetic Approaches for Precision Nutrition Involving the Prevention and Management of Chronic Diseases Associated with Obesity. J. Nutr. Nutr. 2017, 10, 43–62. [Google Scholar] [CrossRef]
- World Health Organization (WHO). Obesity [Internet]. 2020. Available online: https://www.who.int/health-topics/obesity (accessed on 15 October 2020).
- World Health Organization (WHO). Malnutrition, Factsheet Detail [Internet]. 2020. Available online: https://www.who.int/news-room/fact-sheets/detail/malnutrition (accessed on 15 October 2020).
- Mohapatra, S.; Gangadharan, K.; Pitchumoni, C.S. Malnutrition in obesity before and after bariatric surgery. Dis.-A-Month 2020, 66, 100866. [Google Scholar] [CrossRef]
- Astrup, A.; Bügel, S. Overfed but undernourished: Recognizing nutritional inadequacies/deficiencies in patients with overweight or obesity. Int. J. Obes. 2019, 43, 219–232. [Google Scholar] [CrossRef]
- Mendonça, N.; Granic, A.; Mathers, J.C.; Hill, T.R.; Siervo, M.; Adamson, A.J.; Jagger, C. Prevalence and determinants of low protein intake in very old adults: Insights from the Newcastle 85+ Study. Eur. J. Nutr. 2018, 57, 2713–2722. [Google Scholar] [CrossRef]
- PROMISS. Protein [Internet]. Available online: https://www.promiss-vu.eu/about/protein/?cn-reloaded=1 (accessed on 15 October 2020).
- Aasheim, E.T.; Hofsø, D.; Hjelmesæth, J.; Birkeland, K.I.; Bøhmer, T. Vitamin status in morbidly obese patients: A cross-sectional study. Am. J. Clin. Nutr. 2008, 87, 362–369. [Google Scholar] [CrossRef]
- Castro, A.M.; Macedo-de la Concha, L.E.; Pantoja-Meléndez, C.A. Low-grade inflammation and its relation to obesity and chronic degenerative diseases. Rev. Med. Hosp. Gen. Mex. 2017, 80, 101–105. [Google Scholar] [CrossRef]
- Sandstead, H.H. Zinc nutrition in the United States. Am. J. Clin. Nutr. 1973, 26, 1251–1260. [Google Scholar] [CrossRef] [PubMed]
- Sandstead, H.H. Zinc as an unrecognized limiting nutrient. Am. J. Clin. Nutr. 1973, 26, 790–791. [Google Scholar] [CrossRef] [PubMed]
- El Dib, R.; Gameiro, O.L.; Ogata, M.S.; Módolo, N.S.; Braz, L.G.; Jorge, E.C.; do Nascimento Junior, P.; Beletate, V. Zinc supplementation for the prevention of type 2 diabetes mellitus in adults with insulin resistance. Cochrane Database Syst. Rev. 2015, CD005525. [Google Scholar] [CrossRef]
- Swaminathan, R. Magnesium metabolism and its disorders. Clin. Biochem. Rev. 2003, 24, 47–66. [Google Scholar]
- Huerta, M.G.; Roemmich, J.N.; Kington, M.L.; Bovbjerg, V.E.; Weltman, A.L.; Holmes, V.F.; Patrie, J.T.; Rogol, A.D.; Nadler, J.L. Magnesium Deficiency Is Associated with Insulin Resistance in Obese Children. Diabetes Care 2005, 28, 1175–1181. [Google Scholar] [CrossRef] [PubMed]
- Hassan, S.A.U.; Ahmed, I.; Nasrullah, A.; Haq, S.; Ghazanfar, H.; Sheikh, A.B.; Zafar, R.; Askar, G.; Hamid, Z.; Khushdil, A.; et al. Comparison of Serum Magnesium Levels in Overweight and Obese Children and Normal Weight Children. Cureus 2017, 9, e1607. [Google Scholar] [CrossRef] [PubMed]
- Parrott, J.; Frank, L.; Rabena, R.; Craggs-Dino, L.; Isom, K.A.; Greiman, L. American Society for Metabolic and Bariatric Surgery Integrated Health Nutritional Guidelines for the Surgical Weight Loss Patient 2016 Update: Micronutrients. Surg. Obes. Relat. Dis. 2017, 13, 727–741. [Google Scholar] [CrossRef]
- DeMaeyer, E.; Adiels-Tegman, M. The prevalence of anaemia in the world. World Health Stat. Q. 1985, 38, 302–316. [Google Scholar] [PubMed]
- Cheng, H.L.; Bryant, C.; Cook, R.; O’Connor, H.; Rooney, K.; Steinbeck, K. The relationship between obesity and hypoferraemia in adults: A systematic review. Obes. Rev. 2012, 13, 150–161. [Google Scholar] [CrossRef]
- de Luis, D.A.; Pacheco, D.; Izaola, O.; Terroba, M.C.; Cuellar, L.; Cabezas, G. Micronutrient status in morbidly obese women before bariatric surgery. Surg. Obes. Relat. Dis. 2013, 9, 323–327. [Google Scholar] [CrossRef] [PubMed]
- Sánchez, A.; Rojas, P.; Basfi-fer, K.; Carrasco, F.; Inostroza, J.; Codoceo, J.; Valencia, A.; Papapietro, K.; Csendes, A.; Ruz, M. Micronutrient Deficiencies in Morbidly Obese Women Prior to Bariatric Surgery. Obes. Surg. 2016, 26, 361–368. [Google Scholar] [CrossRef]
- Lefebvre, P.; Letois, F.; Sultan, A.; Nocca, D.; Mura, T.; Galtier, F. Nutrient deficiencies in patients with obesity considering bariatric surgery: A cross-sectional study. Surg. Obes. Relat. Dis. 2014, 10, 540–546. [Google Scholar] [CrossRef] [PubMed]
- van der Valk, E.S.; Savas, M.; van Rossum, E.F.C. Stress and Obesity: Are there More Susceptible Individuals? Curr. Obes. Rep. 2018, 7, 193–203. [Google Scholar] [CrossRef] [PubMed]
- Sikorski, C.; Luppa, M.; Luck, T.; Riedel-Heller, S.G. Weight stigma “gets under the skin”-evidence for an adapted psychological mediation framework—A systematic review. Obesity 2015, 23, 266–276. [Google Scholar] [CrossRef] [PubMed]
- Simon, G.E.; Ludman, E.J.; Linde, J.A.; Operskalski, B.H.; Ichikawa, L.; Rohde, P.; Finch, E.A.; Jeffery, R.W. Association between obesity and depression in middle-aged women. Gen. Hosp. Psychiatry 2008, 30, 32–39. [Google Scholar] [CrossRef]
- Jauch-Chara, K.; Oltmanns, K.M. Obesity—A neuropsychological disease? Systematic review and neuropsychological model. Prog. Neurobiol. 2014, 114, 84–101. [Google Scholar] [CrossRef]
- Taylor, V.H.; McIntyre, R.S.; Remington, G.; Levitan, R.D.; Stonehocker, B.; Sharma, A.M. Beyond Pharmacotherapy: Understanding the Links between Obesity and Chronic Mental Illness. Can. J. Psychiatry 2012, 57, 5–12. [Google Scholar] [CrossRef]
- Assari, S. The link between mental health and obesity: Role of individual and contextual factors. Int. J. Prev. Med. 2014, 5, 247–249. [Google Scholar]
- Bak, M.; Fransen, A.; Janssen, J.; van Os, J.; Drukker, M. Almost all antipsychotics result in weight gain: A meta-analysis. PLoS ONE 2014, 9, e94112. [Google Scholar] [CrossRef]
- Karlsson, J.; Sjöström, L.; Sullivan, M. Swedish obese subjects (SOS)—An intervention study of obesity. Two-year follow-up of health-related quality of life (HRQL) and eating behavior after gastric surgery for severe obesity. Int. J. Obes. Relat. Metab. Disord. 1998, 22, 113–126. [Google Scholar] [CrossRef] [PubMed]
- Dickerson, F.B.; Brown, C.H.; Kreyenbuhl, J.A.; Fang, L.; Goldberg, R.W.; Wohlheiter, K.; Dixon, L.B. Obesity among individuals with serious mental illness. Acta Psychiatr. Scand. 2006, 113, 306–313. [Google Scholar] [CrossRef] [PubMed]
- Sachs-Ericsson, N.; Burns, A.B.; Gordon, K.H.; Eckel, L.A.; Wonderlich, S.A.; Crosby, R.D.; Blazer, D.G. Body Mass Index and Depressive Symptoms in Older Adults: The Moderating Roles of Race, Sex, and Socioeconomic Status. Am. J. Geriatr. Psychiatry 2007, 15, 815–825. [Google Scholar] [CrossRef]
- Sjöberg, R.L.; Nilsson, K.W.; Leppert, J. Obesity, shame, and depression in school-aged children: A population-based study. Pediatrics 2005, 116, e389–e392. [Google Scholar] [CrossRef]
- Falkner, N.H.; Neumark-Sztainer, D.; Story, M.; Jeffery, R.W.; Beuhring, T.; Resnick, M.D. Social, Educational, and Psychological Correlates of Weight Status in Adolescents. Obes. Res. 2001, 9, 32–42. [Google Scholar] [CrossRef]
- Erickson, S.J.; Robinson, T.N.; Haydel, K.F.; Killen, J.D. Are Overweight Children Unhappy? Arch. Pediatr. Adolesc. Med. 2000, 154, 931. [Google Scholar] [CrossRef]
- van der Merwe, M.-T. Psychological correlates of obesity in women. Int. J. Obes. 2007, 31, S14–S18. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Scott, K.M.; Bruffaerts, R.; Simon, G.E.; Alonso, J.; Angermeyer, M.; de Girolamo, G.; Demyttenaere, K.; Gasquet, I.; Haro, J.M.; Karam, E.; et al. Obesity and mental disorders in the general population: Results from the world mental health surveys. Int. J. Obes. 2008, 32, 192–200. [Google Scholar] [CrossRef] [PubMed]
- Francis, H.M.; Stevenson, R.J.; Chambers, J.R.; Gupta, D.; Newey, B.; Lim, C.K. A brief diet intervention can reduce symptoms of depression in young adults—A randomised controlled trial. PLoS ONE 2019, 14, e0222768. [Google Scholar] [CrossRef]
- Schiller, M.R.; Miller, M.; Moore, C.; Davis, E.; Dunn, A.; Mulligan, K.; Zeller, P. Patients Report Positive Nutrition Counseling Outcomes. J. Am. Diet. Assoc. 1998, 98, 977–982. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. U.S. Obesity Trends; Centers for Disease Control and Prevention: Washington, DC, USA, 2011.
- WHO. Healthy Diet [Internet]. Available online: https://www.who.int/behealthy/healthy-diet (accessed on 15 October 2020).
- World Health Organization (WHO) N. Guideline: Sugars Intake for Adults and Children; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- World Health Organization (WHO) N. Guideline: Sodium Intake for Adults and Children; World Health Organization (WHO): Geneva, Switzerland, 2012. [Google Scholar]
- Astrup, A.; Bertram, H.C.; Bonjour, J.-P.; de Groot, L.C.; de Oliveira Otto, M.C.; Feeney, E.L.; Garg, M.L.; Givens, I.; Kok, F.J.; Krauss, R.M.; et al. WHO draft guidelines on dietary saturated and trans fatty acids: Time for a new approach? BMJ 2019, 366, 15683. [Google Scholar] [CrossRef] [PubMed]
- Kalkuz, S.; Demircan, A. Effects of the Mediterranean diet adherence on body composition, blood parameters and quality of life in adults. Postgrad. Med. J. 2020. [Google Scholar] [CrossRef] [PubMed]
- Goulet, J. Effect of a nutritional intervention promoting the Mediterranean food pattern on plasma lipids, lipoproteins and body weight in healthy French-Canadian women. Atherosclerosis 2003, 170, 115–124. [Google Scholar] [CrossRef]
- Trichopoulos, D.; Lagiou, P. Editorial: Mediterranean diet and cardiovascular epidemiology. Eur. J. Epidemiol. 2003, 19, 7–8. [Google Scholar] [CrossRef]
- Estruch, R.; Ros, E.; Salas-Salvadó, J.; Covas, M.-I.; Corella, D.; Arós, F.; Gómez-Gracia, E.; Ruiz-Gutiérrez, V.; Fiol, M.; Lapetra, J.; et al. Primary Prevention of Cardiovascular Disease with a Mediterranean Diet. N. Engl. J. Med. 2013, 368, 1279–1290. [Google Scholar] [CrossRef]
- Grosso, G.; Mistretta, A.; Frigiola, A.; Gruttadauria, S.; Biondi, A.; Basile, F.; Vitaglione, P.; D’Orazio, N.; Galvano, F. Mediterranean Diet and Cardiovascular Risk Factors: A Systematic Review. Crit. Rev. Food Sci. Nutr. 2014, 54, 593–610. [Google Scholar] [CrossRef]
- Tong, T.Y.N.; Wareham, N.J.; Khaw, K.-T.; Imamura, F.; Forouhi, N.G. Prospective association of the Mediterranean diet with cardiovascular disease incidence and mortality and its population impact in a non-Mediterranean population: The EPIC-Norfolk study. BMC Med. 2016, 14, 135. [Google Scholar] [CrossRef]
- Singh, B.; Parsaik, A.K.; Mielke, M.M.; Erwin, P.J.; Knopman, D.S.; Petersen, R.C.; Roberts, R.O. Association of Mediterranean Diet with Mild Cognitive Impairment and Alzheimer’s Disease: A Systematic Review and Meta-Analysis. J. Alzheimer’s Dis. 2014, 39, 271–282. [Google Scholar] [CrossRef]
- Alcalay, R.N.; Gu, Y.; Mejia-Santana, H.; Cote, L.; Marder, K.S.; Scarmeas, N. The association between Mediterranean diet adherence and Parkinson’s disease. Mov. Disord. 2012, 27, 771–774. [Google Scholar] [CrossRef]
- Esposito, K.; Maiorino, M.I.; Ceriello, A.; Giugliano, D. Prevention and control of type 2 diabetes by Mediterranean diet: A systematic review. Diabetes Res. Clin. Pract. 2010, 89, 97–102. [Google Scholar] [CrossRef]
- Esposito, K. Effects of a Mediterranean-Style Diet on the Need for Antihyperglycemic Drug Therapy in Patients with Newly Diagnosed Type 2 Diabetes. Ann. Intern. Med. 2009, 151, 306. [Google Scholar] [CrossRef] [PubMed]
- Jensen, M.D.; Ryan, D.H.; Apovian, C.M.; Ard, J.D.; Comuzzie, A.G.; Donato, K.A.; Hu, F.B.; Hubbard, V.S.; Jakicic, J.M.; Kushner, R.F.; et al. 2013 AHA/ACC/TOS Guideline for the Management of Overweight and Obesity in Adults. Circulation 2014, 129, S102–S138. [Google Scholar] [CrossRef] [PubMed]
- LeBlanc, E.S.; O’Connor, E.; Whitlock, E.P.; Patnode, C.D.; Kapka, T. Effectiveness of Primary Care-Relevant Treatments for Obesity in Adults: A Systematic Evidence Review for the U.S. Preventive Services Task Force. Ann. Intern. Med. 2011, 155, 434. [Google Scholar] [CrossRef]
- Cooper, M.; Morton, J. Digital Health and Obesity: How Technology Could Be the Culprit and Solution for Obesity; Springer: Cham, Switzerland, 2018; pp. 169–178. [Google Scholar]
- Tison, G.H.; Marcus, G.M. Will the smartphone become a useful tool to promote physical activity? Lancet Digit. Health 2019, 1, e322–e323. [Google Scholar] [CrossRef]
- Dallinga, J.M.; Mennes, M.; Alpay, L.; Bijwaard, H.; de la Faille-Deutekom, M.B. App use, physical activity and healthy lifestyle: A cross sectional study. BMC Public Health 2015, 15, 833. [Google Scholar] [CrossRef] [PubMed]
- Shcherbina, A.; Hershman, S.G.; Lazzeroni, L.; King, A.C.; O’Sullivan, J.W.; Hekler, E.; Moayedi, Y.; Pavlovic, A.; Waggott, D.; Sharma, A.; et al. The effect of digital physical activity interventions on daily step count: A randomised controlled crossover substudy of the MyHeart Counts Cardiovascular Health Study. Lancet Digit. Health 2019, 1, e344–e352. [Google Scholar] [CrossRef]
- European Commission. Blueprint Digital Transformation of Health and Care for the Ageing Society [Internet]. Available online: https://ec.europa.eu/eip/ageing/blueprint_en (accessed on 15 October 2020).
- Linger, H.; Fisher, J.; Wojtkowski, W.; Wojtkowski, W.G.; Zupančič, J.; Vigo, K. (Eds.) Constructing the Infrastructure for the Knowledge Economy; Springer: Boston, MA, USA, 2004. [Google Scholar] [CrossRef]
- Vincent, C.J.; Blandford, A. The challenges of delivering validated personas for medical equipment design. Appl. Ergon. 2014, 45, 1097–1105. [Google Scholar] [CrossRef]
- Navarro, F.H. Profiles of Attitudes toward Healthcare: Psychographic Segmentation. MA Psychol. Res. 1990. [Google Scholar] [CrossRef]
- LeRouge, C.; Ma, J.; Sneha, S.; Tolle, K. User profiles and personas in the design and development of consumer health technologies. Int. J. Med. Inform. 2013, 82, e251–e268. [Google Scholar] [CrossRef]
- Puhl, R.M.; Latner, J.D. Stigma, obesity, and the health of the nation’s children. Psychol. Bull. 2007, 133, 557–580. [Google Scholar] [CrossRef]
- Carl, J.; Thedinga, H.K.; Zipfel, S.; Thiel, A. Stimulating Weight Stigma in Future Experimental Designs on Physical Activity—Development and Pilot Validation of a Video Instrument. Obes. Facts 2018, 11, 206–220. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Global NCD Target Halt the Rise in Obesity. 2016. Available online: https://www.who.int/beat-ncds/take-action/policy-brief-halt-obesity.pdf (accessed on 15 October 2020).
- World Health Organization (WHO) D. Digital Health [Internet]. Available online: https://www.who.int/health-topics/digital-health#tab=tab_2 (accessed on 15 October 2020).
- Dhingra, D.; Dabas, A. Global Strategy on Digital Health. Indian Pediatr. 2020, 57, 356–358. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Sustainable Development Goals [Internet]. Available online: https://www.who.int/health-topics/sustainable-development-goals#tab=tab_1 (accessed on 15 October 2020).
- World Health Organization (WHO). Thirteenth General Programme of Work (GPW13): Methods for Impact Measurement; World Health Organization (WHO): Geneva, Switzerland, 2020. [Google Scholar]
- World Health Organization (WHO). Health Data: A Critical Element to Meet the SDGs [Internet]. Available online: https://www.who.int/data/stories/health-data-a-critical-element-to-meet-the-sdgs (accessed on 15 October 2020).
- European Commission. Europe 2020—For a Healthier EU [Internet]. Available online: https://ec.europa.eu/health/europe_2020_it (accessed on 15 October 2020).
- European Commission. Innovation Union [Internet]. 2020. Available online: https://ec.europa.eu/info/research-and-innovation/strategy/goals-research-and-innovation-policy/innovation-union_en (accessed on 15 October 2020).
- European Commission. Blueprint for a Digital Transformation of Health and Care in an Ageing Society [Internet]. Available online: https://ec.europa.eu/digital-single-market/en/blueprint-digital-transformation-health-and-care-ageing-society (accessed on 1 October 2020).
- European Commission. European Innovation Partenership [Internet]. Available online: https://ec.europa.eu/eip/ageing/home_en (accessed on 15 October 2020).
- European Commission. Shaping the Digital Single Market [Internet]. Available online: https://ec.europa.eu/digital-single-market/en/policies/shaping-digital-single-marke (accessed on 15 October 2020).
- European Commission. Health Strategy [Internet]. Available online: https://ec.europa.eu/health/policies/background/review/strategy_it (accessed on 15 October 2020).
- European Commission. EU Action Plan on Childhood Obesity 2014–2020 [Internet]. 2014. Available online: https://ec.europa.eu/health/sites/health/files/nutrition_physical_activity/docs/childhoodobesity_actionplan_2014_2020_en.pdf (accessed on 15 October 2020).
- European Commission. White Paper on a Strategy for Europe on Nutrition, Overweight and Obesity Related Health Issues. 2014. Available online: https://ec.europa.eu/health/archive/ph_determinants/life_style/nutrition/documents/nutrition_wp_en. (accessed on 15 October 2020).
- Illario, M.; Maione, A.S.; Rusciano, M.R.; Goossens, E.; Rauter, A.; Braz, N.; Jager-Wittenaar, H.; Di Somma, C.; Crola, C.; Soprano, M.; et al. NutriLive: An Integrated Nutritional Approach as a Sustainable Tool to Prevent Malnutrition in Older People and Promote Active and Healthy Ageing—The EIP-AHA Nutrition Action Group. Adv. Public Health 2016, 2016, 1–9. [Google Scholar] [CrossRef]
- Ministero della Salute. Piano Nazionale della Prevenzione [Internet]. Available online: http://www.salute.gov.it/portale/temi/p2_4.jsp?lingua=italiano&tema=Prevenzione&area=prevenzione (accessed on 15 October 2020).
- Ministero della Salute. Piano Nazionale della Cronicità. 2016. Available online: http://www.salute.gov.it/imgs/C_17_pubblicazioni_2584_allegato.pdf (accessed on 15 October 2020).
- Regione Campania. OKkio alla Salute. Italia. 2016. Available online: https://www.epicentro.iss.it/okkioallasalute/reportregionali2016/OKkio2016_Campania_Report Regionale.pdf (accessed on 15 October 2020).
- Istiituto Superiore di Sanità, Italia. Passi d’Argento [Internet]. Available online: https://www.epicentro.iss.it/passi-argento/ (accessed on 15 October 2020).
- Regione Campania I. Piano Regionale della Prevenzione [Internet]. Available online: http://www.regione.campania.it/regione/it/news/salute-7054/piano-regionale-della-prevenzione?page=1 (accessed on 15 October 2020).
- Regione Campania I. Linee d’indirizzo Regionali per le aa.ss.ll. sulla Promozione dell’attività Fisica Adattata (afa) in Soggetti con Malattie Croniche non Trasmissibili (mcnt) Stabilizzate. Available online: http://www.regione.campania.it/assets/documents/linee-di-indirizzo-afa-con-allegati (accessed on 15 October 2020).
- Requirez, S.; Leonardi, F.; Carruba, G.; Di Fiore, P.; Falconeri, D.A.E. Programma “Formazione Educazione Dieta” (FED) per la promozione della Dieta Mediterranea. Sist. Salut. 2016, 60, 51–67. [Google Scholar]
- Carruba, G.; Trosko, J.E. The Long Evolutionary Journey of Cancer from Ancestor to Modern Humans. Crit. Rev. Oncog. 2017, 22, 323–352. [Google Scholar] [CrossRef]
- European Commission. Best Practice Portal [Internet]. Available online: https://webgate.ec.europa.eu/dyna/bp-portal/ (accessed on 15 October 2020).
- DG SANTE—DG for Health and Food Safety EC. Knowledge for Policy [Internet]. Available online: https://ec.europa.eu/knowledge4policy/organisation/dg-sante-dg-health-food-safety_en (accessed on 15 October 2020).
- Early Childhood Ireland [Internet]. Available online: https://www.earlychildhoodireland.ie/ (accessed on 15 October 2020).
- Seafood [Internet]. Available online: https://www.safefood.eu/Education/Pre-school/Little-Bites-(ROI).aspx (accessed on 15 October 2020).
- Presidenza del Consiglio dei Ministri. Agenzia per l’Italia Digitale (AGID) [Internet]. Available online: https://www.agid.gov.it/it (accessed on 25 October 2020).
- Presidenza del Consiglio dei Ministri. Digital Healthcare System [Internet]. Available online: https://www.agid.gov.it/en/piattaforme/digital-healthcare-system (accessed on 15 October 2020).
- Smart Health [Internet]. Available online: https://www.sanita-digitale.com/2019/03/07/telemedicina-fastweb-lancia-smart-health/ (accessed on 15 October 2020).
- Ippocrate [Internet]. Available online: https://www.ippocrateas.eu/ (accessed on 15 October 2020).
- Promoting Healthy Lifestyles in the Autonomous Province of Trento, Italy: The “Move Your Health” Project [Internet]. Available online: https://www.euro.who.int/en/countries/italy/news/news/2020/01/promoting-healthy-lifestyles-in-the-autonomous-province-of-trento,-italy-the-move-your-health-project (accessed on 15 October 2020).
- Regione Campania. Soresa [Internet]. Available online: https://www.soresa.it/ (accessed on 15 October 2020).
- Regione Siciliana. Sanità Digitale. Agenda Digitale Sicilia [Internet]. 2018. Available online: http://pti.regione.sicilia.it/portal/page/portal/PIR_PORTALE/PIR_Iniziative/Agenda_Digitale_Sicilia (accessed on 15 October 2020).
- Università Degli Studi di Napoli Federico II. Opera [Internet]. Available online: https://www.unescochairnapoli.it/ (accessed on 15 October 2020).
- Campus Salute [Internet]. Available online: http://www.campussalute.it/onlus/ (accessed on 15 October 2020).
- Una vita su Misura [Internet]. Available online: https://unavitasumisura.it/ (accessed on 15 October 2020).
- Berman, A.H.; Kolaas, K.; Petersén, E.; Bendtsen, P.; Hedman-Lagerlöf, E.; Linderoth, C.; Müssener, U.; Sinadinovic, K.; Spak, F.; Gremyr, I.; et al. Clinician experiences of healthy lifestyle promotion and perceptions of digital interventions as complementary tools for lifestyle behavior change in primary care. BMC Fam. Pract. 2018, 19, 139. [Google Scholar] [CrossRef]
- Lianov, L.S.; Fredrickson, B.L.; Barron, C.; Krishnaswami, J.; Wallace, A. Positive Psychology in Lifestyle Medicine and Health Care: Strategies for Implementation. Am. J. Lifestyle Med. 2019, 13, 480–486. [Google Scholar] [CrossRef]
- Kanera, I.M.; Bolman, C.A.W.; Willems, R.A.; Mesters, I.; Lechner, L. Lifestyle-related effects of the web-based Kanker Nazorg Wijzer (Cancer Aftercare Guide) intervention for cancer survivors: A randomized controlled trial. J. Cancer Surviv. 2016, 10, 883–897. [Google Scholar] [CrossRef]
- Beleigoli, A.M.; Andrade, A.Q.; Cançado, A.G.; Paulo, M.N.; Diniz, M.D.F.H.; Ribeiro, A.L. Web-Based Digital Health Interventions for Weight Loss and Lifestyle Habit Changes in Overweight and Obese Adults: Systematic Review and Meta-Analysis. J. Med. Internet Res. 2019, 21, e298. [Google Scholar] [CrossRef]
- Liotta, G.; Ussai, S.; Illario, M.; O’Caoimh, R.; Cano, A.; Holland, C.; Roller-Wirnsberger, R.; Capanna, A.; Grecuccio, C.; Ferraro, M.; et al. Frailty as the Future Core Business of Public Health: Report of the Activities of the A3 Action Group of the European Innovation Partnership on Active and Healthy Ageing (EIP on AHA). Int. J. Environ. Res. Public Health 2018, 15, 2843. [Google Scholar] [CrossRef]
- Illario, M.; De Luca, V.; Tramontano, G.; Menditto, E.; Iaccarino, G.; Bertorello, L.; Palummeri, E.; Romano, V.; Moda, G.; Maggio, M.; et al. The Italian reference sites of the European innovation partnership on active and healthy ageing: Progetto Mattone Internazionale as an enabling factor. Ann. Ist. Super. Sanita 2017, 53, 60–69. [Google Scholar] [PubMed]
- De Luca, V.; Birov, S.; Beyhan, O.; Robinson, S.; Sanchez-Nanclares, G.; Acuña, M.; Fernandes, A.; Hammerschmidt, R.; Annuzzi, G.; Iaccarino, G.; et al. European Specifications for Value-based Pre-Commercial Procurement of Innovative ICT for Empowerment and Self-management of Diabetes Mellitus Patients. In Proceedings of the 5th International Conference on Information and Communication Technologies for Ageing Well and e-Health, Crete, Greece, 2–4 May 2019; SCITEPRESS—Science and Technology Publications: Setúbal, Portugal, 2019; pp. 19–27. [Google Scholar]



{kind=link}
{kind=link}
| Health Policy |
| World Health Organization |
Global Strategy on Digital Health 2020–2025:
|
| Europe |
EU’s 10-year economic growth strategy:
|
| White Paper on a Strategy for Europe on Nutrition, Overweight and Obesity-related health issues |
| Italy |
|
| Campania and Sicily Regions |
|
| Digital Tool | Blueprint Persona |
|---|---|
| Europe | |
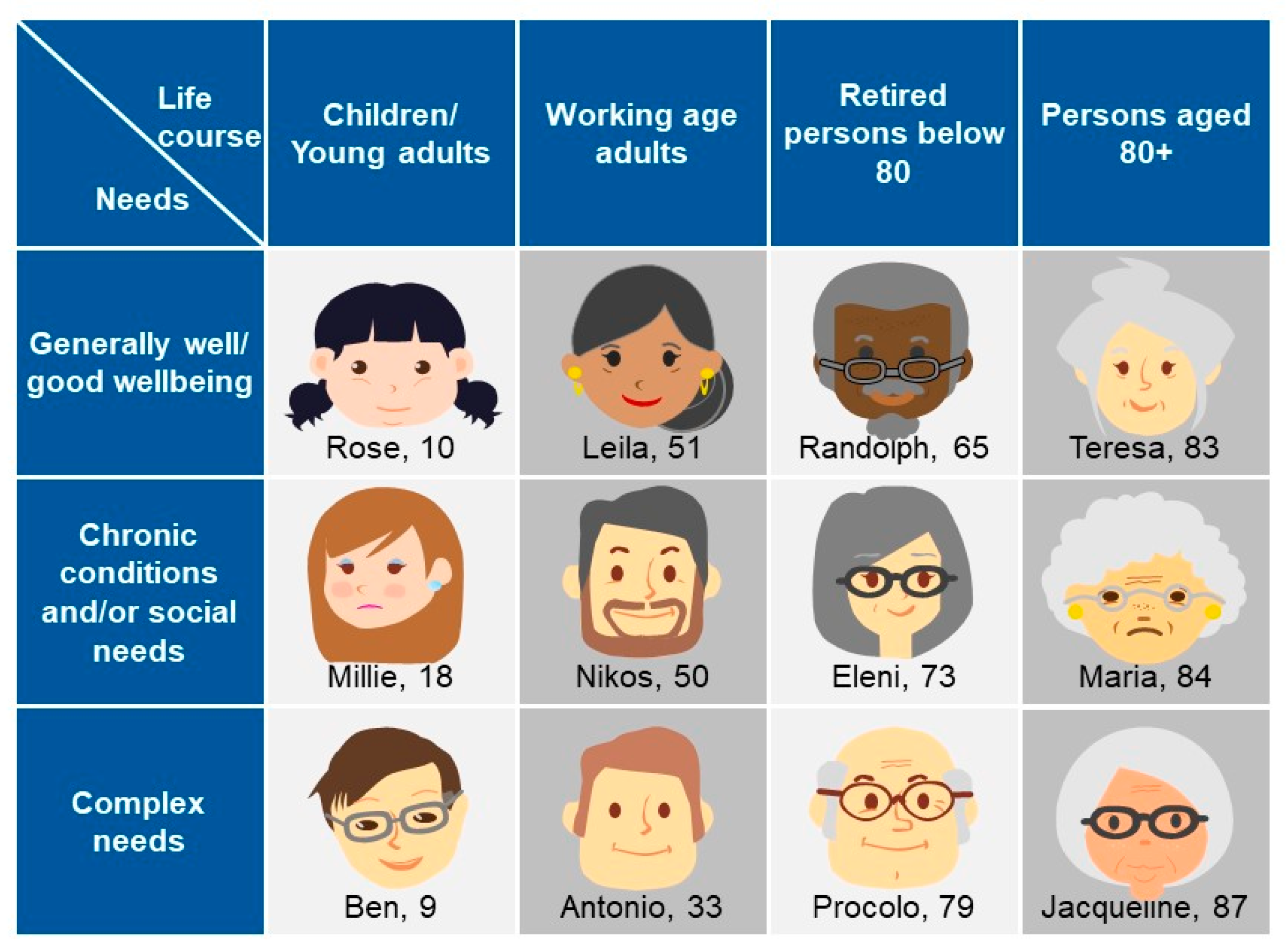
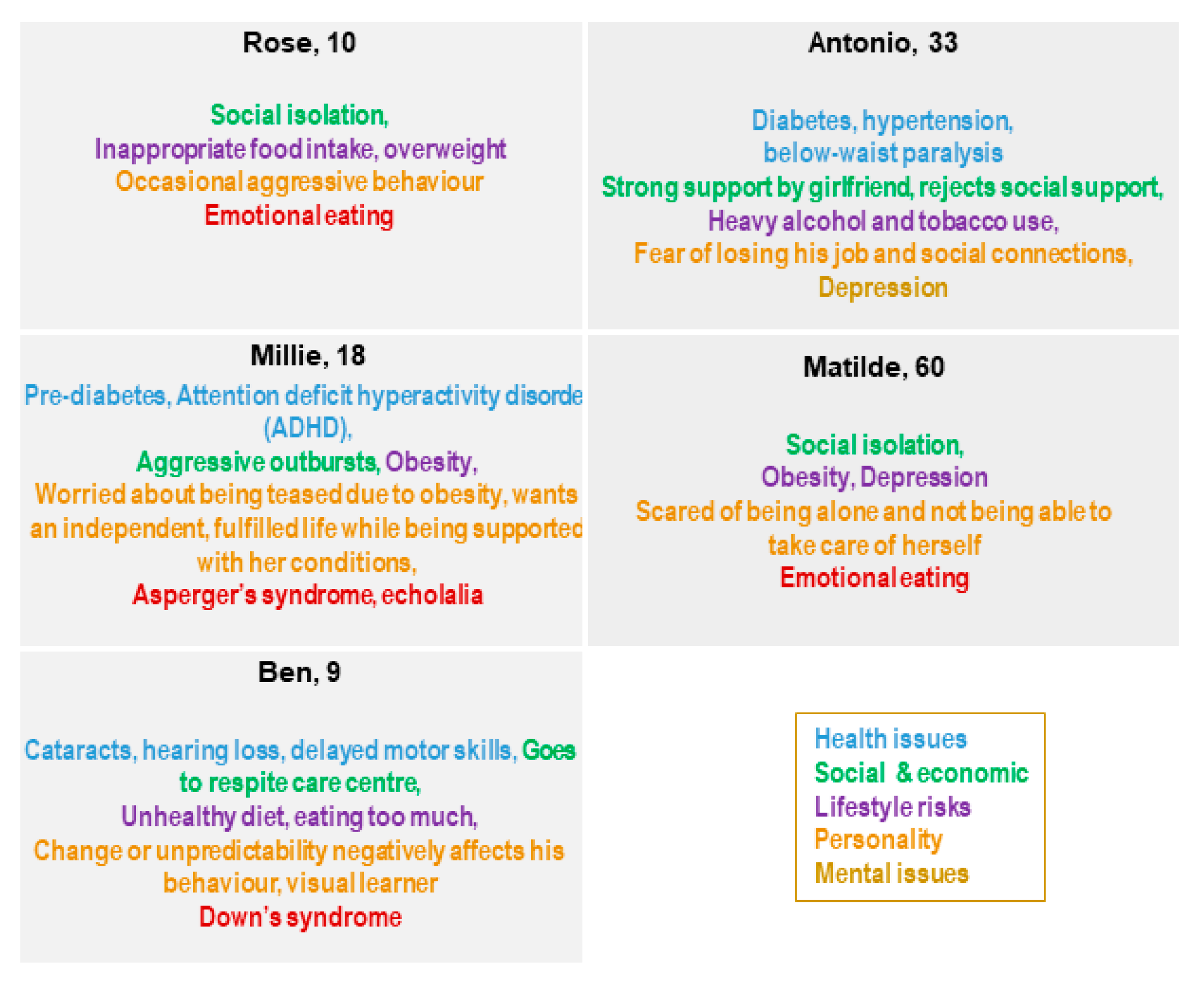
| Rose, Millie, and Ben: healthy diet and eating advice to control body weight |
| Italy | |
| Antonio and Matilde: home telemonitoring, remote diagnosis support, update data in real-time to the doctor, medical devices to be monitored remotely, reducing the inconvenience and costs of travel for visits and controls at health facilities |
| Rose, Milli, Ben Antonio and Matilde: improve activities such as prevention, diagnosis, and treatment, as well as improve the monitoring and management of health and lifestyles |
| Rose, Milli, Ben Antonio and Matilde: choosing healthier lifestyles and reducing health inequalities associated with outreach activities, involving migrant or socioeconomically disadvantaged families |
| Campania and Sicily Regions | |
| Rose, Milli, Ben Antonio and Matilde: innovative free path to men and women who want to lose weight, healthy diet and eating advice to control body weight, psychological support |
| Rose, Milli, Ben Antonio and Matilde: psychological support, the patient himself/herself who tells his/her story, exposes his/her doubts, and presents his/her difficulties |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Patalano, R.; De Luca, V.; Vogt, J.; Birov, S.; Giovannelli, L.; Carruba, G.; Pivonello, C.; Stroetmann, V.; Triassi, M.; Colao, A.; et al. An Innovative Approach to Designing Digital Health Solutions Addressing the Unmet Needs of Obese Patients in Europe. Int. J. Environ. Res. Public Health 2021, 18, 579. https://doi.org/10.3390/ijerph18020579
Patalano R, De Luca V, Vogt J, Birov S, Giovannelli L, Carruba G, Pivonello C, Stroetmann V, Triassi M, Colao A, et al. An Innovative Approach to Designing Digital Health Solutions Addressing the Unmet Needs of Obese Patients in Europe. International Journal of Environmental Research and Public Health. 2021; 18(2):579. https://doi.org/10.3390/ijerph18020579
Chicago/Turabian StylePatalano, Roberta, Vincenzo De Luca, Jess Vogt, Strahil Birov, Lucia Giovannelli, Giuseppe Carruba, Claudia Pivonello, Veli Stroetmann, Maria Triassi, Annamaria Colao, and et al. 2021. "An Innovative Approach to Designing Digital Health Solutions Addressing the Unmet Needs of Obese Patients in Europe" International Journal of Environmental Research and Public Health 18, no. 2: 579. https://doi.org/10.3390/ijerph18020579
APA StylePatalano, R., De Luca, V., Vogt, J., Birov, S., Giovannelli, L., Carruba, G., Pivonello, C., Stroetmann, V., Triassi, M., Colao, A., & Illario, M. (2021). An Innovative Approach to Designing Digital Health Solutions Addressing the Unmet Needs of Obese Patients in Europe. International Journal of Environmental Research and Public Health, 18(2), 579. https://doi.org/10.3390/ijerph18020579