Barriers to Accessing Medicines among Syrian Asylum Seekers and Refugees in a German Federal State


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Sampling Design
2.3. Participants and Eligibility Criteria
Inclusion Criteria
2.4. Community Involvement
2.5. Questionnaire Development
2.6. Recruitment and Data Collection
2.7. Data Analysis
2.7.1. Qualitative Data Analysis
2.7.2. Quantitative Data Analysis
3. Results
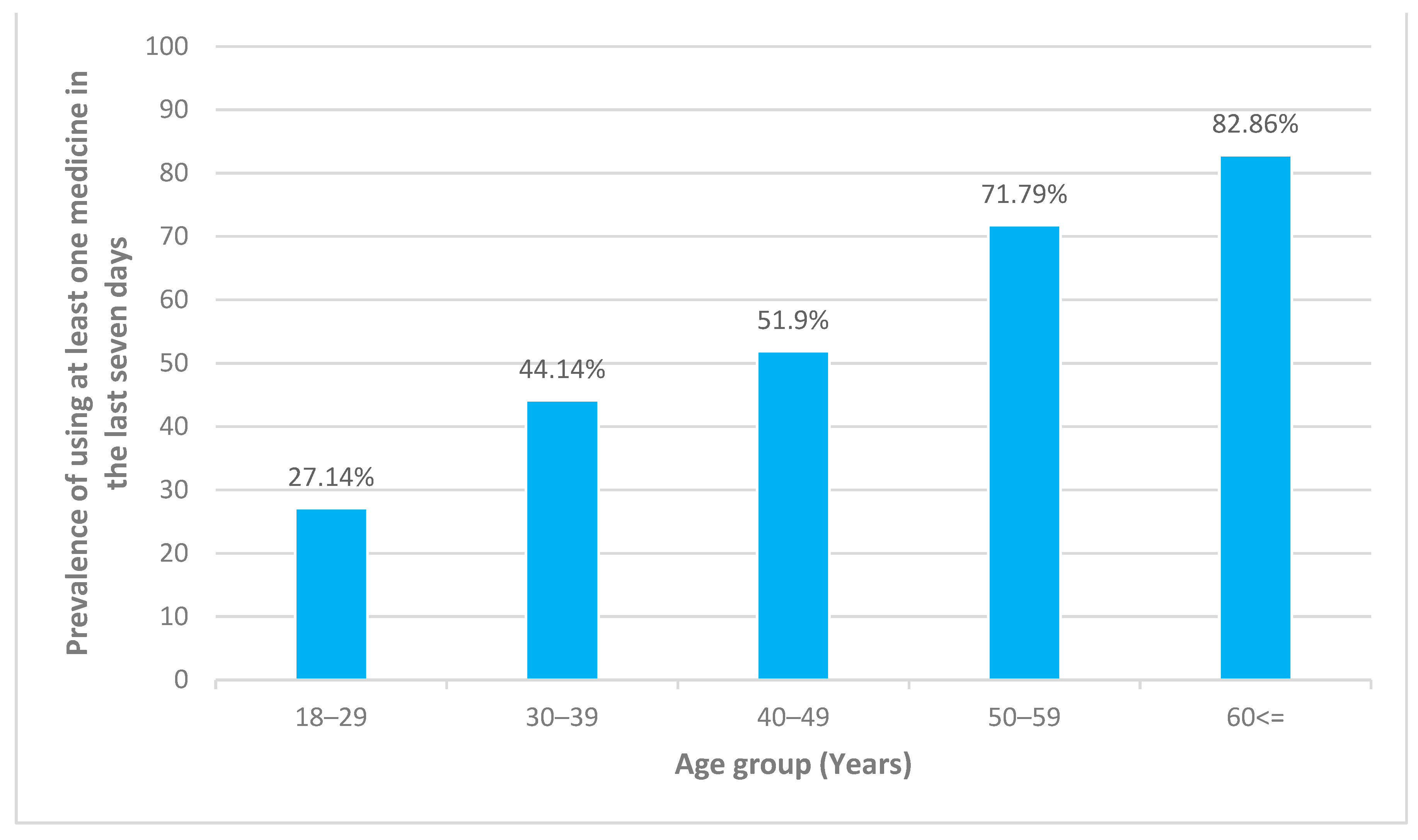
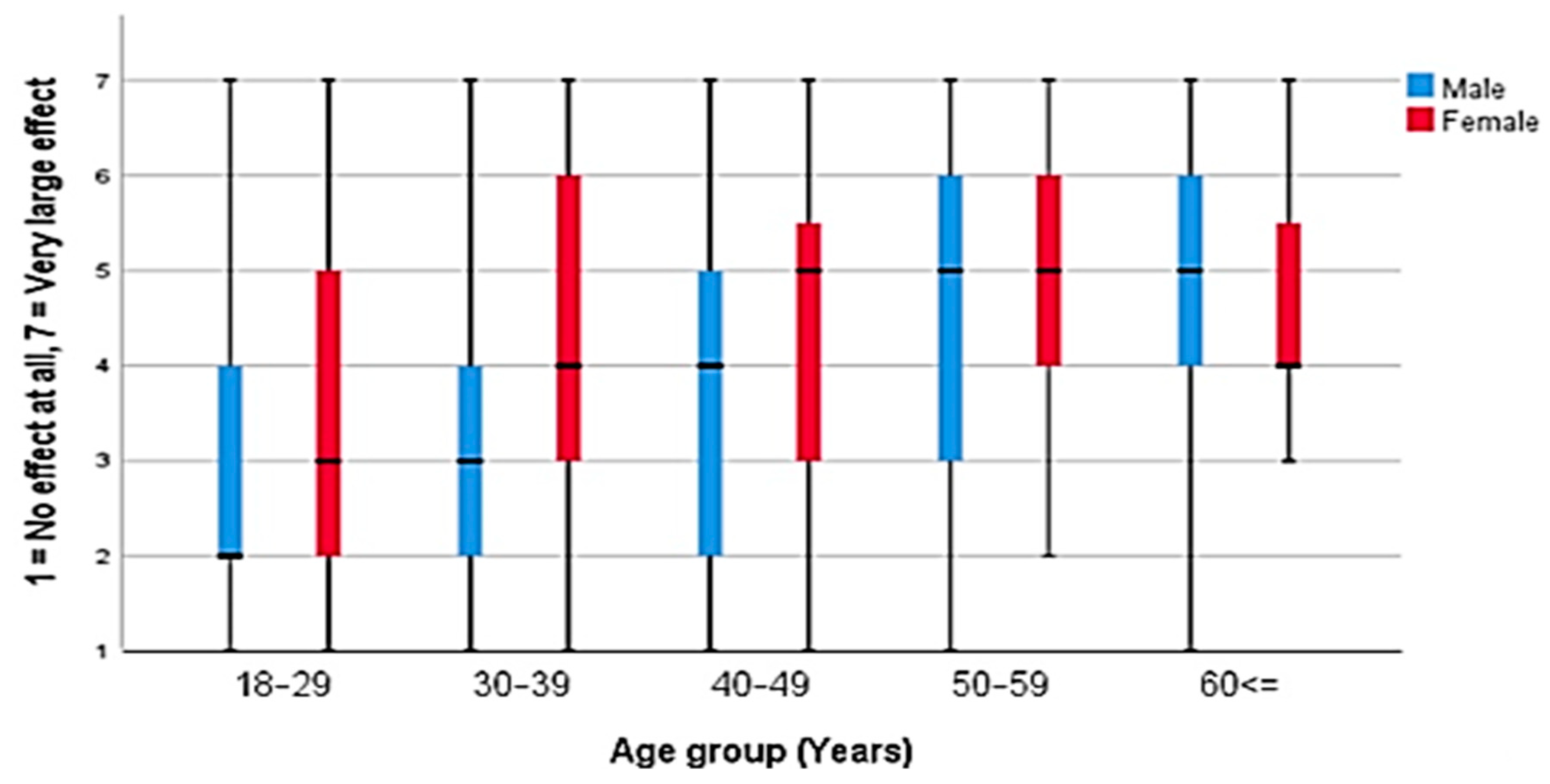
3.1. Barriers to Accessing Medicines
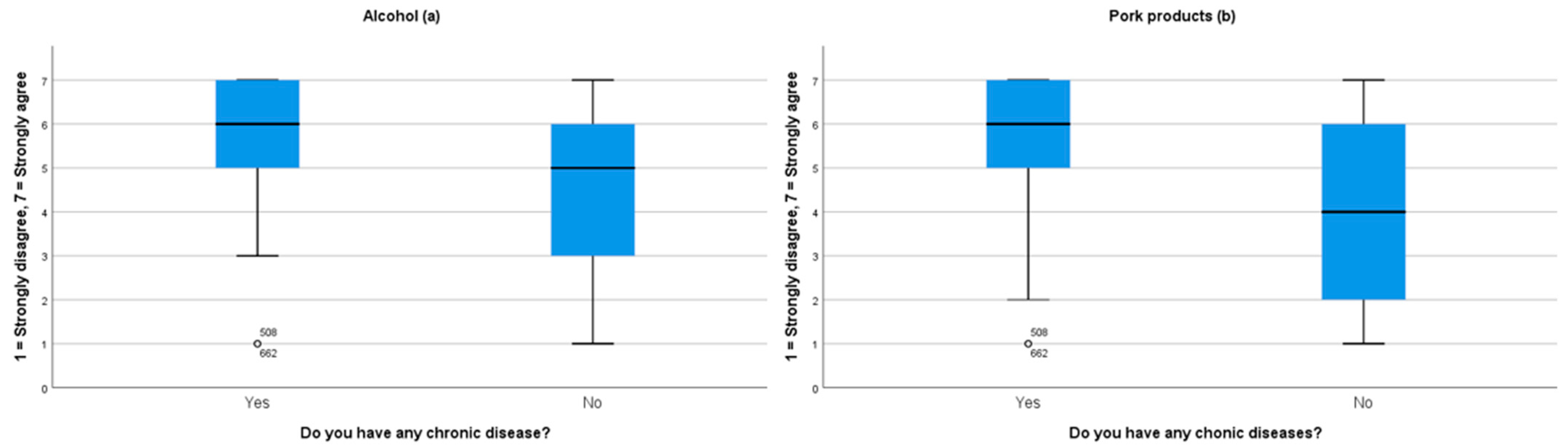
3.2. Acceptance of Medicines Containing Alcohol or Pork Products
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations High Commissioner for Refugees. Global Trends Forced Displacement in 2019. Available online: https://www.unhcr.org/5ee200e37.pdf (accessed on 15 September 2020).
- Bundesamt für Migration und Flüchtlinge. Das Bundesamt in Zahlen 2019: Asyl, Migration und Integration, 2020. Available online: https://www.bamf.de/SharedDocs/Anlagen/DE/Statistik/BundesamtinZahlen/bundesamt-in-zahlen-2019.pdf?__blob=publicationFile&v=4 (accessed on 20 September 2020).
- Gottlieb, N.; Bozorgmehr, K.; Trummer, U.; Rechel, B. Health policies and mixed migration—Lessons learnt from the ‘Refugee Crisis’. Health Policy 2019, 123, 805–808. [Google Scholar] [CrossRef] [PubMed]
- Puchner, K.; Karamagioli, E.; Pikouli, A.; Tsiamis, C.; Kalogeropoulos, A.; Kakalou, E.; Pavlidou, E.; Pikoulis, E. Time to rethink refugee and migrant health in Europe: Moving from emergency response to integrated and individualized health care provision for migrants and refugees. Int. J. Environ. Res. Public Health 2018, 15, 1100. [Google Scholar] [CrossRef] [PubMed]
- United Nations High Commissioner for Refugees. Global Report, 2005. Available online: https://www.unhcr.org/449267670.pdf (accessed on 15 December 2020).
- United Nations High Commissioner for Refugees. The 1951 Refugee Convention. Available online: https://www.unhcr.org/1951-refugee-convention.html (accessed on 15 December 2020).
- Bozorgmehr, K.; Samuilova, M.; Petrova-Benedict, R.; Girardi, E.; Piselli, P.; Kentikelenis, A. Infectious disease health services for refugees and asylum seekers during a time of crisis: A scoping study of six European Union countries. Health Policy 2019, 123, 882–887. [Google Scholar] [CrossRef] [PubMed]
- Bozorgmehr, K.; Razum, O. Effect of restricting access to health care on health expenditures among asylum-seekers and refugees: A quasi-experimental study in Germany, 1994–2013. PLoS ONE 2015, 10, e0131483. [Google Scholar] [CrossRef]
- Bozorgmehr, K.; Razum, O. Refugees in Germany—Untenable restrictions to health care. Lancet 2016, 388, 2351–2352. [Google Scholar] [CrossRef]
- Bozorgmehr, K.; Wenner, J.; Razum, O. Restricted access to health care for asylum-seekers: Applying a human rights lens to the argument of resource constraints. Eur. J. Public Health 2017, 27, 592–593. [Google Scholar] [CrossRef]
- Bundesministerium für Gesundheit. Zuzahlung und Erstattung von Arzneimitteln. Available online: https://www.bundesgesundheitsministerium.de/zuzahlung-und-erstattung-arzneimittel.html#c12485 (accessed on 16 December 2020).
- Bundesamt für Justiz. Asylbewerberleistungsgesetz (AsylbLG). Available online: https://www.gesetze-im-internet.de/asylblg/BJNR107410993.html (accessed on 20 September 2020).
- OECD European Union. Health at a Glance: Europe 2018. State of Health in the EU Cycle; OECD Publishing: Paris, France, 2018. [Google Scholar]
- Bauhoff, S.; Göpffarth, D. Asylum-seekers in Germany differ from regularly insured in their morbidity, utilizations and costs of care. PLoS ONE 2018, 13. [Google Scholar] [CrossRef]
- Claassen, K.; Jäger, P. Impact of the introduction of the electronic health insurance card on the use of medical services by asylum seekers in Germany. Int. J. Environ. Res. Public Health 2018, 15, 856. [Google Scholar] [CrossRef]
- Epping, B. Medizinische Versorgung von Flüchtlingen: Teure Hürden. Z. Orthop. Unfall. 2017, 155, 129–134. [Google Scholar] [CrossRef]
- §264 SGB V—Übernahme der Krankenbehandlung für Nicht Versicherungspflichtige Gegen Kostenerstattung. Available online: http://www.lexsoft.de/cgi-bin/lexsoft/justizportal_nrw.cgi?xid=137489,351 (accessed on 15 September 2020).
- Jäger, P.; Claassen, K.; Ott, N.; Brand, A. Does the electronic health card for asylum seekers lead to an excessive use of the health system? Results of a survey in two municipalities of the German ruhr area. Int. J. Environ. Res. Public Health 2019, 16, 1178. [Google Scholar] [CrossRef]
- Kay, M.; Wijayanayaka, S.; Cook, H.; Hollingworth, S. Understanding quality use of medicines in refugee communities in Australian primary care: A qualitative study. Br. J. Gen. Pract. 2016, 66, e397–e409. [Google Scholar] [CrossRef] [PubMed]
- Hadgkiss, E.J.; Renzaho, A.M.N. The physical health status, service utilisation and barriers to accessing care for asylum seekers residing in the community: A systematic review of the literature. Aust. Health Rev 2014, 38, 142–159. [Google Scholar] [CrossRef] [PubMed]
- Lerner-Geva, L.; Blumstein, T.; Boyko, V.; Farhi, A.; Benyamini, Y. Cultural disparities in the use of prescription and nonprescription medications among midlife women in Israel. Int. J. Health Serv. 2017, 47, 440–459. [Google Scholar] [CrossRef] [PubMed]
- Bellamy, K.; Ostini, R.; Martini, N.; Kairuz, T. Access to medication and pharmacy services for resettled refugees: A systematic review. Aust. J. Prim. Health 2015, 21, 273–278. [Google Scholar] [CrossRef]
- Shahin, W.; Kennedy, G.A.; Stupans, I. The impact of personal and cultural beliefs on medication adherence of patients with chronic illnesses: A systematic review. Patient Pref. Adherence 2019, 13, 1019–1035. [Google Scholar] [CrossRef]
- Attum, B.; Hafiz, S.; Malik, A.; Shamoon, Z. Cultural Competence in the Care of Muslim Patients and Their Families; StatPearls Publishing: Treasure Island, FL, USA, 2020. [Google Scholar]
- Bruhn, C. Koscher, Halal und Vegan: Was Ist Verboten, Was Ist Erlaubt? Deutsche Apotheker Zeitung. 2016. Available online: https://www.deutsche-apotheker-zeitung.de/daz-az/2016/daz-43-2016/koscher-halal-und-vegan (accessed on 20 September 2020).
- Bloch, A. Methodological challenges for national and multi-sited comparative survey research. J. Refug. Stud. 2007, 20, 230–247. [Google Scholar] [CrossRef]
- Enticott, J.C.; Shawyer, F.; Vasi, S.; Buck, K.; Cheng, I.-H.; Russell, G.; Kakuma, R.; Minas, H.; Meadows, G. A systematic review of studies with a representative sample of refugees and asylum seekers living in the community for participation in mental health research. BMC Med. Res. Methodol. 2017, 17, 37. [Google Scholar] [CrossRef]
- Dean, J.; Wollin, J.; Stewart, D.; Debattista, J.; Mitchell, M. Hidden yet visible: Methodological challenges researching sexual health in Sudanese refugee communities. Cult. Health Sex 2012, 14, 911–924. [Google Scholar] [CrossRef]
- Landesbetrieb IT.NRW Statistik und IT-Dienstleistungen. Available online: https://www.it.nrw/ (accessed on 28 May 2019).
- Sulaiman-Hill, C.M.R.; Thompson, S. Sampling challenges in a study examining refugee resettlement. BMC Int. Health Hum. Rights 2011, 11, 2. [Google Scholar] [CrossRef]
- Spring, M.; Westermeyer, J.; Halcon, L.; Savik, K.; Robertson, C.; Johnson, D.R.; Butcher, J.N.; Jaranson, J. Sampling in difficult to access refugee and immigrant communities. J. Nerv. Ment. Dis. 2003, 191, 813–819. [Google Scholar] [CrossRef]
- Zeisler, M.-L.; Bilgic, L.; Schumann, M.; Wengler, A.; Lemcke, J.; Gößwald, A.; Lampert, T.; Santos-Hovener, C.; Schmich, P. Interventions to increase the reachability of migrants in Germany with health interview surveys: Mixed-mode feasibility study. JMIR Form. Res. 2020, 4, e14747. [Google Scholar] [CrossRef] [PubMed]
- Robert Koch Institute. Studie zur Gesundheit Erwachsener in Deutschland (DEGS). Available online: https://www.degs-studie.de/deutsch/home.html (accessed on 1 March 2018).
- Robert Koch Institute. Studie zur Gesundheit von Kindern und Jugendlichen in Deutschland (KIGGS). Available online: https://www.kiggs-studie.de/deutsch/home.html (accessed on 1 March 2018).
- Svarstad, B.L.; Chewning, B.A.; Sleath, B.L.; Claesson, C. The brief medication questionnaire: A tool for screening patient adherence and barriers to adherence. Patient Educ. Couns. 1999, 37, 113–124. [Google Scholar] [CrossRef]
- Al-Faham, Z.; Habboub, G.; Takriti, F. The sale of antibiotics without prescription in pharmacies in Damascus, Syria. J. Infect. Dev. Ctries 2011, 5, 396–399. [Google Scholar] [CrossRef] [PubMed]
- Morgan, D.J.; Okeke, I.N.; Laxminarayan, R.; Perencevich, E.N.; Weisenberg, S. Non-prescription antimicrobial use worldwide: A systematic review. Lancet Infect Dis 2011, 11, 692–701. [Google Scholar] [CrossRef]
- Institut für Medizinmanagement und Gesundheitswissenschaften, Universität Bayreuth. Auswirkungen des Zustroms von Asylbewerbern auf Die Gesundheitliche Versorgung in Bayern. Available online: https://www.lgl.bayern.de/gesundheit/gesundheitsversorgung/doc/kurzbericht_auswirkungen_zustrom_asylbewerber_gv_by.pdf (accessed on 1 August 2018).
- Lampert, T.; Müters, S.; Stolzenberg, H.; Kroll, L.E. Messung des sozioökonomischen Status in der KiGGS-Studie Erste Folgebefragung (KiGGS Welle 1). Bundesgesundheitsblatt Gesundh. Gesundh. 2014, 57, 762–770. [Google Scholar] [CrossRef]
- Lampert, T.; Kroll, L.; Müters, S.; Stolzenberg, H. Messung des sozioökonomischen Status in der Studie zur Gesundheit Erwachsener in Deutschland (DEGS1). Bundesgesundheitsblatt Gesundh. Gesundh. 2013, 56, 631–636. [Google Scholar] [CrossRef]
- World Health Organization. Process of Translation and Adaptation of Instruments. Available online: https://www.who.int/substance_abuse/research_tools/translation/en/ (accessed on 10 January 2019).
- Qualtrics. Provo, UT, USA, 2020. Available online: https://www.qualtrics.com (accessed on 5 April 2019).
- Mohammad, A.M.; Moles, R.J.; Chen, T.F. Medication-related burden and patients’ lived experience with medicine: A systematic review and metasynthesis of qualitative studies. BMJ Open 2016, 6, 16. [Google Scholar] [CrossRef]
- Council of Europe. Common European Framework of Reference for Languages (CEFR). Available online: https://www.coe.int/en/web/common-european-framework-reference-languages/level-descriptions (accessed on 18 August 2018).
- Clark, A.; Gilbert, A.; Rao, D.; Kerr, L. ‘Excuse me, do any of you ladies speak English?’ Perspectives of refugee women living in South Australia: Barriers to accessing primary health care and achieving the Quality Use of Medicines. Aust. J. Prim. Health 2014, 20, 92–97. [Google Scholar] [CrossRef]
- Alkahtani, S.; Cherrill, J.; Millward, C.; Grayson, K.; Hilliam, R.; Sammons, H.; Choonara, I. Access to medicines by child refugees in the East Midlands region of England: A cross-sectional study. BMJ Open 2014, 4, e006421. [Google Scholar] [CrossRef]
- Siegel, M.; Busse, R. Can People Afford to Pay for Health Care? New Evidence on Financial Protection in Germany; WHO Regional Office for Europe: København, Denmark, 2018. [Google Scholar]
- Kohlenberger, J.; Buber-Ennser, I.; Rengs, B.; Leitner, S.; Landesmann, M. Barriers to health care access and service utilization of refugees in Austria: Evidence from a cross-sectional survey. Health Policy 2019, 123, 833–839. [Google Scholar] [CrossRef]
- Worbs, S.; Baraulina, T. Geflüchtete Frauen in Deutschland: Sprache, Bildung und Arbeitsmarkt. BAMF-Kurzanalyse. Available online: https://www.bamf.de/SharedDocs/Anlagen/DE/Forschung/Kurzanalysen/kurzanalyse7_gefluchetete-frauen.pdf?__blob=publicationFile&v=14 (accessed on 30 September 2020).
- Eisnecker, P.; Giesecke, J.; Kroh, M.; Liebau, E.; Marcus, J.; Salikutluk, Z.; Schacht, D.; Spieß, C.K.; Westermaier, F. Die integration geflüchteter—Erkenntnisse aus der vergangenhei. DIW-Wochenbericht 2016, 83, 727–730. [Google Scholar]
- Li, W.W. Comparative study on social-economic status, trauma and mental health disorders among older and younger refugees in Australia. J. Trop. Psych. 2016, 6, 1–9. [Google Scholar] [CrossRef]
- Al Hassan, M.; Bengtsson, S.; Kohlenberger, J. Understanding the Syrian Educational System in a Context of Crisis. Vienna Institute of Demography Working Papers, No. 09/2016, Austrian Academy of Sciences (ÖAW), Vienna Institute of Demography (VID), Vienna, 2016. Available online: https://www.econstor.eu/bitstream/10419/156317/1/875728065.pdf (accessed on 19 October 2020).
- World Health Organization. Medication Without Harm, WHO Global Patient Safety Challenge, 2017. Available online: https://apps.who.int/iris/bitstream/handle/10665/255263/WHO-HIS-SDS-2017.6-eng.pdf;jsessionid=80005B1CD84D740DA575470D29021F89?sequence=1 (accessed on 15 May 2019).
- Wettermark, B.; Godman, B.; Bennie, M. Drug Utilization Research: Methods and Applications; John Wiley & Sons Inc.: Hoboken, NJ, USA, 2016; ISBN 9781118949788. [Google Scholar]
- Saha, T.; Rifat, T.; Shimanto, S. Prospects of halal pharmaceuticals. Asian J. Ethnopharmacol. Med. Foods 2019, 5, 17–23. [Google Scholar]
- Asmak, A.; Fatimah, S.; Huzaimah, I.; Khuriah, A.H.; Siti Khadijah, A.M. Is our medicine lawful (Halal)? Middle East J. Sci. Res. 2015, 23, 367–373. [Google Scholar] [CrossRef]
- Public Health England. The Children’s Flu Vaccination Programme, the Nasal Flu Vaccine Fluenzand Porcine Gelatine, 2014. Available online: https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/386842/2902998_PHE_FluPorcine_QAforParents_FINAL_CT.pdf (accessed on 23 October 2020).




{kind=link}
{kind=link}
{kind=link}
| Participant Characteristics | Number of Participants | Proportion (%) |
|---|---|---|
| Sex | ||
| Male | 1024 | 62.4% |
| Female | 617 | 37.6% |
| Age | ||
| 0–17 | 578 | 35.22% |
| 18–29 | 468 | 28.52% |
| 30–39 | 318 | 19.38% |
| 40–49 | 158 | 9.63% |
| 50–59 | 78 | 4.75% |
| 60≤ | 41 | 2.5% |
| Health insurance | ||
| Yes | 1616 | 98.48% |
| No | 23 | 1.4% |
| Missing | 2 | 0.12% |
| Residency status | ||
| Refugee status or subsidiary protection | 1603 | 97.68% |
| Asylum seeker | 38 | 2.32% |
| Accommodation | ||
| Initial reception center | 18 | 1.1% |
| Long-term accommodation center | 318 | 19.38% |
| Private housing | 1289 | 78.55% |
| Missing | 16 | 0.97% |
| Chronic disease (Adults only) | ||
| Yes (22 different chronic diseases) | 146 | 13.74% |
| No | 914 | 85.98% |
| Missing | 3 | 0.28% |
| The most common chronic diseases | ||
| Hypertension | 71 | 6.68 |
| Diabetes | 44 | 4.14 |
| Hypothyroidism | 30 | 2.82 |
| Hyperlipoproteinemia | 21 | 1.98 |
| Anemia | 21 | 1.98 |
| Other chronic diseases | 66 | 6.21 |
| Employment (Adults only) | ||
| Employed | 249 | 23.42% |
| Retired | 16 | 1.51% |
| Vocational training | 237 | 22.29% |
| Not employed | 537 | 50.52% |
| Missing | 24 | 2.26% |
| German language level 1 | ||
| A1-A1 | 242 | 22.77% |
| B1-B2 | 495 | 46.57% |
| C1-C2 | 168 | 15.8% |
| None | 131 | 12.32% |
| Missing | 27 | 2.54% |
| Marriage status (Adults only) | ||
| Single | 381 | 35.84% |
| Married | 613 | 57.67% |
| In a relationship | 27 | 2.54% |
| Divorced | 19 | 1.79% |
| Widowed | 13 | 1.22% |
| Missing | 10 | 0.94% |
| Participant Subgroups | Language Barriers | Unavailability of Certain Medicines in Pharmacies | Financial Barriers | Purchasing Medicines without a Prescription | ||
|---|---|---|---|---|---|---|
| Total 1 | ||||||
| Adults | Median (IQR 2) | 3 (2–5) *** | 1 (0) | 1 (0) | 1 (1–3) | |
| Parents | Median (IQR) | 4 (3–5) *** | 1 (0) | 1 (0) | 1 (1–3) | |
| Adults | ||||||
| Sex 1 | ||||||
| Female | Median (IQR) | 4 (2–5) *** | 1 (0) | 1 (0) | 1 (1–3) | |
| Male | Median (IQR) | 3 (2–4) *** | 1 (0) | 1 (0) | 1 (1–3) | |
| Age 3 | ||||||
| 18–29 | Median (IQR) | 2 (2–4) *** | 1 (0) | 1 (0) ** | 1 (0) * | |
| 30–39 | Median (IQR) | 4 (2–5) *** | 1 (0) | 1 (0) ** | 1 (1–3) * | |
| 40–49 | Median (IQR) | 4 (3–5) *** | 1 (0) | 1 (0) ** | 1 (1–3) * | |
| 50–59 | Median (IQR) | 5 (4–6) *** | 1 (0) | 1 (0) ** | 1 (1–3) * | |
| ≤60 | Median (IQR) | 5 (4–6) *** | 1 (0) | 1 (1–3) ** | 1 (1–4) * | |
| Chronic diseases 1 | ||||||
| Yes | Median (IQR) | 4 (3–5) *** | 1 (0) | 1 (1–2) *** | 1 (1–3) *** | |
| No | Median (IQR) | 3 (2–5) *** | 1 (0) | 1 (0) *** | 1 (1–2) *** |
| Participant Subgroups | Alcohol | Pork Products | ||
|---|---|---|---|---|
| Total | ||||
| Adults | Median (IQR 1) | 4 (1–7) | 4 (1–7) | |
| Sex 2 | ||||
| Female | Median (IQR) | 1 (1–4) *** | 1 (1–4) *** | |
| Male | Median (IQR) | 7 (3–7) *** | 4 (2–7) *** | |
| Age 3 | ||||
| 18–19 | Median (IQR) | 7 (1–7) *** | 7 (1–7) *** | |
| 30–39 | Median (IQR) | 4 (1–7) *** | 4 (1–7) *** | |
| 40–49 | Median (IQR) | 4 (1–7) *** | 3 (1–7) *** | |
| 50–59 | Median (IQR) | 4 (1–7) *** | 4 (1–7) *** | |
| ≥60 | Median (IQR) | 4 (1–5) *** | 4 (1–4) *** | |
| Chronic diseases 2 | ||||
| Yes | Median (IQR) | 4 (2–7) | 4 (1–7) | |
| No | Median (IQR) | 4 (1–7) | 4 (1–4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aljadeeah, S.; Wirtz, V.J.; Nagel, E. Barriers to Accessing Medicines among Syrian Asylum Seekers and Refugees in a German Federal State. Int. J. Environ. Res. Public Health 2021, 18, 519. https://doi.org/10.3390/ijerph18020519
Aljadeeah S, Wirtz VJ, Nagel E. Barriers to Accessing Medicines among Syrian Asylum Seekers and Refugees in a German Federal State. International Journal of Environmental Research and Public Health. 2021; 18(2):519. https://doi.org/10.3390/ijerph18020519
Chicago/Turabian StyleAljadeeah, Saleh, Veronika J. Wirtz, and Eckhard Nagel. 2021. "Barriers to Accessing Medicines among Syrian Asylum Seekers and Refugees in a German Federal State" International Journal of Environmental Research and Public Health 18, no. 2: 519. https://doi.org/10.3390/ijerph18020519
APA StyleAljadeeah, S., Wirtz, V. J., & Nagel, E. (2021). Barriers to Accessing Medicines among Syrian Asylum Seekers and Refugees in a German Federal State. International Journal of Environmental Research and Public Health, 18(2), 519. https://doi.org/10.3390/ijerph18020519