The Impact of Using Kinesio Tape on Non-Infectious Complications after Impacted Mandibular Third Molar Surgery




Abstract
1. Introduction
2. Materials and Methods
2.1. Patient Recruitment and Study Groups
- Study group (n = 50): kinesio tape applied for five days after surgery
- Control group (n = 50): non-kinesio tape applied.
2.2. Surgery
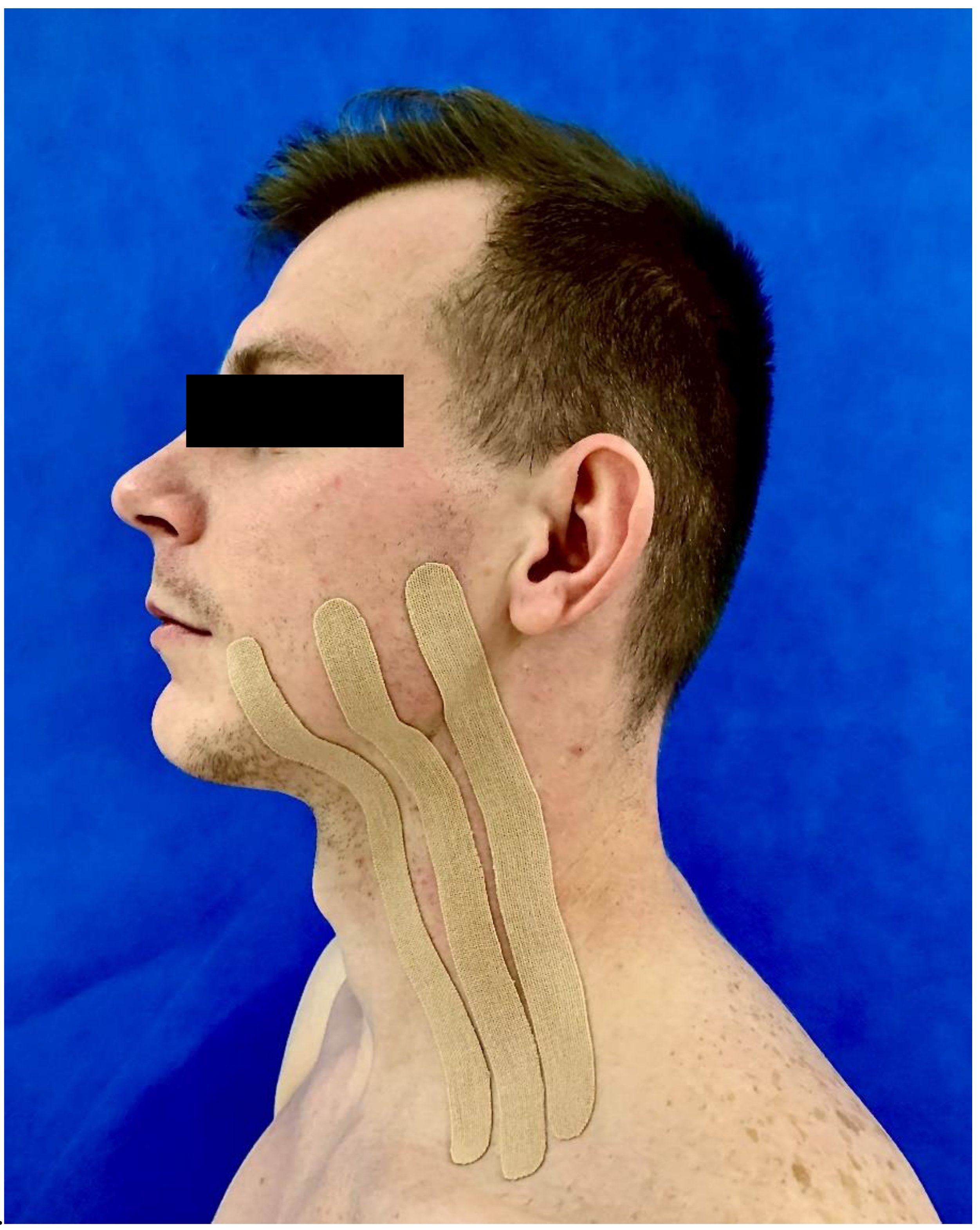
2.3. Kinesiotaping
2.4. Data Collection
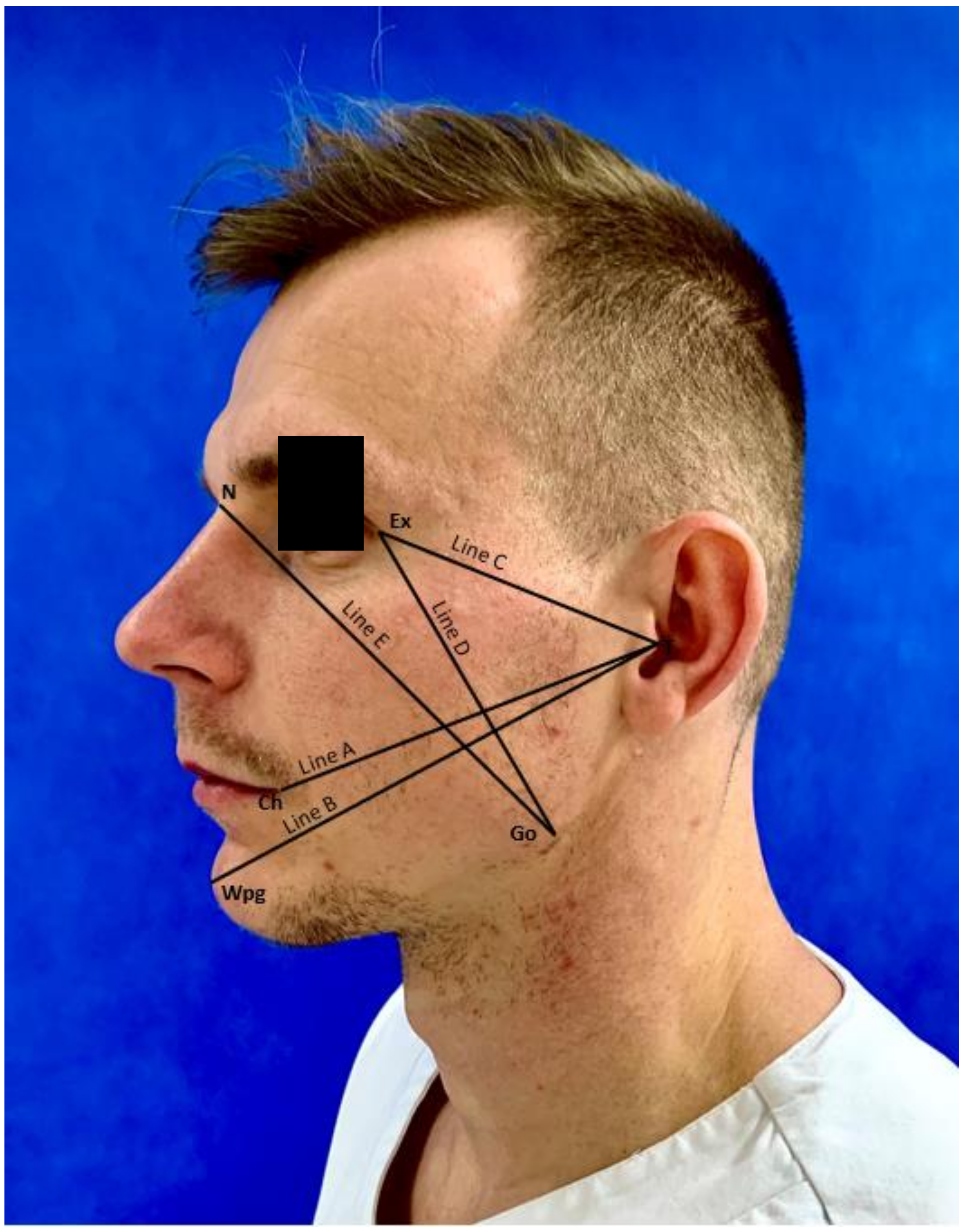
2.4.1. Edema
- Line A—from tragus (T) to cheilon (Ch)
- Line B—from tragus (T) to pogonion (WPg)
- Line C—from tragus (T) to exocanthion (Ex)
- Line D—from exocanthion (Ex) to gonion (Go)
- Line E—from gonion (Go) to nasion (N)
2.4.2. Trismus
2.4.3. Pain
2.5. Statistical Methodology
3. Results
3.1. Baseline Characteristics
3.2. Analysis of Postoperative Edema Measurements
3.3. Analysis of Postoperative Trismus Measurements
3.4. Analysis of Postoperative Pain Measurements
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bui, C.H.I.; Seldin, E.; Dodson, T. Types, frequencies, and risk factors for complications after third molar extraction. J. Oral. Maxillofac. Surg. 2003, 61, 1379–1389. [Google Scholar] [CrossRef]
- Yuasa, H.; Sugiura, M. Clinical postoperative findings after removal of impacted mandibular third molars: Prediction of postoperative facial swelling and pain based on preoperative variables. J. Oral. Maxillofac. Surg. 2004, 42, 209–214. [Google Scholar] [CrossRef]
- Zandi, M.; Amini, P.; Keshavarz, A. Effectiveness of cold therapy in reducing pain, trismus, and edema after impacted mandibular third molar surgery: A randomized, self-controlled, observer-blind, split-mouth clinical trial. J. Oral. Maxillofac. Surg. 2015, 45, 118–123. [Google Scholar] [CrossRef]
- Osunde, O.; Saheeb, B.; Bassey, G. Indications and risk factors for complications of lower third molar surgery in a nigerian teaching hospital. Ann. Med. Health Sci. Res. 2014, 4, 938–942. [Google Scholar] [CrossRef]
- Miloro, M.; Ghali, G.E.; Larsen, P.E.; Waite, P.D. Peterson’s Principles of Oral and Maxillofacial Surgery, 2nd ed.; BC Decker: London, UK, 2004. [Google Scholar]
- Gbotolorum, O.M.; Arotiba, G.T.; Ladeine, A.L. Assessment of factors associated with surgical difficulty in impacted mandibular third molar extraction. J. Oral. Maxillofac. Surg. 2007, 65, 1977–1983. [Google Scholar] [CrossRef]
- Jaroń, A.; Aniko-Włodarczyk, M.; Preuss, O.; Trybek, G. Radiological assessment of the type of retention and the degree of difficulty of surgical removal of an impacted wisdom tooth in the mandible extended with three-dimensional modeling. (Ocena radiologiczna typu retencji oraz stopnia trudności operacyjnego usunięcia zatrzymanego zęba mądrości w żuchwie poszerzona o modelowanie trójwymiarowe.). In Proceedings of the Kongres Polskiego Towarzystwa Chirurgii Stomatologicznej i Szczękowo-Twarzowej, Lublin, Poland, 9–11 May 2019. [Google Scholar]
- Jaroń, A.; Jedliński, M.; Grzywacz, E.; Mazur, M.; Trybek, G. Kinesiology Taping as an Innovative Measure against Post-Operative Complications after Third Molar Extraction—Systematic Review. J. Clin. Med. 2020, 9, 3988. [Google Scholar] [CrossRef]
- Osorio, J.A.; Vairo, G.L.; Rozea, G.D.; Bosha, P.J.; Millard, R.L.; Aukerman, D.F.; Sebastianelli, W.J. The effects of two therapeutic patellofemoral taping techniques on strength, endurance, and pain responses. Phys. Ther. Sport 2013, 14, 199–206. [Google Scholar] [CrossRef]
- Lee, M.S.; Lee, J.H. Ankle inversion taping using kinesiology tape for treating medial ankle sprain in an amatour soccer player. J. Phys. Ther. Sci. 2015, 27, 2407–2408. [Google Scholar] [CrossRef][Green Version]
- Kiebzak, W.; Kowalski, I.M.; Pawłowski, M.; Gąsior, J.; Zaborowska-Sapeta, K.; Wolska, O.; Śliwiński, Z. Wykorzystanie metody Kinesiology Tapingu w praktyce fizjoterapeutycznej: Przegląd literatury. Fizjoter Pol. 2012, 12, 1–11. [Google Scholar]
- Hałas, I.; Senderek, T.; Krupa, L. Wykorzystanie kinesiotapingu w usprawnianiu pacjentki po rekonstrukcji nerwu twarzowego. Fizjoter Pol. 2005, 5, 272–276. [Google Scholar]
- Tozzi, U.; Santaga, M.; Sellitto, A.; Tartaro, G.P. Influence of Kinesiologic Tape on postoperative swelling after orthognatic surgery. J. Oral. Maxillofac. Surg. 2015, 15, 52–58. [Google Scholar] [CrossRef]
- Mikołajewska, E. Kinesiotaping; Wydawnictwo Lekarskie PZWL: Warszawa, Poland, 2011. [Google Scholar]
- Gómez-Soriano, J.; Abián-Vicén, J.; Aparicio-García, C.; Ruiz-Lázaro, P.; Simón-Martínez, C.; Bravo-Esteban, E.; Fernández-Rodríguez, J.M. The effects of Kinesio taping on muscle tone in healthy subjects: A double-blind, placebo-controlled crossover trial. Man. Ther. 2014, 19, 131–136. [Google Scholar] [CrossRef]
- Zhang, S.; Fu, W.; Pan, J.; Wang, L.; Xia, R.; Liu, Y. Acute effects of Kinesio taping on muscle strength and fatigue in the forearm of tennis players. J. Sci. Med. Sport 2015, 19, 459–464. [Google Scholar] [CrossRef]
- Śliwiński, Z.; Krajczy, M. Dynamiczne Plastrowanie, Podręcznik Kinesiology Taping; Markmed: Wrocław, Poland, 2014. [Google Scholar]
- Ristow, O.; Hohlweg-Majert, B.; Stürzenbaum, S.R.; Kehl, V.; Koerdt, S.; Hahnefeld, L.; Pautke, C. Therapeutic elastic tape reduces morbidity after wisdom teeth removal—A clinical trial. Clin. Oral. Investig. 2014, 18, 1205–1212. [Google Scholar] [CrossRef]
- Adeyemo, W.L.; Ladeinde, A.L.; Ogunlewe, M.O. Clinical evaluation of post-extraction site wound healing. J. Contemp. Dent. Pract. 2006, 7, 40–49. [Google Scholar] [CrossRef]
- Trybek, G.; Chamarczuk, A.; Falkowska, J.; Grzegorzewska, M.; Preuss, O.; Aniko-Włodarczyk, M. Intraoral odontogenic abscesses in patients of The Department of Oral Surgery at the Pomeranian Medical University in Szczecin: 7 years of observation. Postep. Hig. Med. Dosw. 2018, 72, 491–498. [Google Scholar] [CrossRef]
- Trybek, G.; Chruściel-Nogalska, M.; Machnio, M.; Smektała, T.; Malinowski, J.; Tutak, M.; Sporniak-Tutak, K. Surgical extraction of impacted teeth in elderly patients. A retrospective analysis of perioperative complications—The experience of a single institution. Gerodontology 2016, 33, 410–415. [Google Scholar] [CrossRef]
- Chen, P.C.; Tung, Y.C.; Wu, P.W.; Wu, L.S.; Lin, Y.S.; Chang, C.J.; Kung, S.; Chu, P.H. Dental procedures and the risk of infective endocarditis. Medicine 2015, 94, 1826–1832. [Google Scholar] [CrossRef]
- Little, J.W.; Jacobson, J.J.; Lockhart, P.B. The dental treatment of patients with joint replacements: A position paper from American Academy of Oral Medicine. JADA 2010, 141, 667–671. [Google Scholar] [CrossRef]
- Osunde, O.D.; Saheeb, B.D. Effect of age, sex and level of surgical difficulty on inflammatory complications after third molar surgery. J. Maxillofac. Oral. Surg. 2015, 14, 7–12. [Google Scholar] [CrossRef]
- Al-Khateeb, T.H.; Nusair, Y. Effect of the proteolytic enzyme serrapeptase on swelling, pain and trismus after surgical extraction of mandibular third molars. Int. J. Oral. Maxillofac. Surg. 2008, 37, 264–268. [Google Scholar] [CrossRef]
- Garczyński, W.; Lubkowska, A.; Dobek, A.; Andryszczyk, M. Wpływ aplikacji kinesiology tapingu techniką mięśniową na zakres ruchomości lędźwiowego odcinka kręgosłupa oraz subiektywne odczuwanie natężenia bólu u chorych z dolegliwościami bólowymi kręgosłupa. Ann. Acad. Med. Stetin. 2014, 2, 19–24. [Google Scholar] [CrossRef]
- Świerczyńska, A.; Kłusek, R.; Czachor, T.; Gajda, B. Kinezjotaping jako jedna z metod leczenia urazów rdzenia kręgowego. Prz. Lek. 2011, 68, 1144–1148. [Google Scholar]
- Bortoluzzi, M.C.; Guollo, A.; Capella, D.L.; Manfro, R. Pain levels after third molar surgical removal: An evaluation of predictive variables. J. Contemp. Dent. Pract. 2011, 12, 239–244. [Google Scholar] [CrossRef]
- Mohammed, I.A.; Delemi, Z.H. Kinesiology tape in comparison with oral Diclofenac sodium in reducing swelling after surgical removal of lower wisdom teeth. Al Rafidain Dent. J. 2019, 19, 90–97. [Google Scholar] [CrossRef]
- Kase, K.; Wallis, J.; Kase, T. Clinical Therapeutic Applications of the Kinesio Taping Method, 2nd ed.; Ken Ikai: Tokyo, Japan, 2003. [Google Scholar]
- Markowski, A. Kinesiotaping; Wydawnictwo SBM: Warszawa, Poland, 2015. [Google Scholar]
- Genc, A.; Cakarer, S.; Yalcin, B.K.; Kilic, B.B.; Isler, S.C.; Keskin, C. A comparative study of surgical drain placement and the use of kinesiologic tape to reduce postoperative morbidity after third molar surgery. Clin. Oral. Investig. 2019, 23, 345–350. [Google Scholar] [CrossRef]
- Erdil, A.; Akbulut, N.; Altan, A.; Demirsoy, M.S. Comparison of the effect of therapeutic elastic bandage, submucosal dexamethasone, or dexketoprofen trometamol on inflammatory symptoms and quality of life following third molar surgery: A randomized clinical trial. Clin. Oral. Investig. 2020, 15. [Google Scholar] [CrossRef]
- Tatli, U.; Benlidayi, I.C.; Salimov, F.; Guzel, R. Effectiveness of kinesio taping onpostoperative morbidity after impacted mandibular third molar surgery: A prospective, randomized, placebo-controlled clinical study. J. Appl. Oral. Sci. 2020, 28, e20200159. [Google Scholar] [CrossRef]
- Gözlüklü, Ö.; Ulu, M.; Gözlüklü, H.Ö.; Yilmaz, N. Comparison of Different Kinesio Taping Techniques After Third Molar Surgery. J. Oral. Maxillofac. Surg. 2020, 78, 695–704. [Google Scholar] [CrossRef]
- Da Rocha Heras, A.C.T.; De Oliveira, D.M.S.; Guskuma, M.H.; De Araújo, M.C.; Fernandes, K.B.P.; Da Silva Junior, R.A.; Andraus, R.A.C.; Maia, L.P.; Fernandes, T.M.F. Kinesio taping use to reduce pain and edema after third molar extraction surgery: A randomized controlled split-mouth study. J. Craniomaxillofac. Surg. 2020, 48, 127–131. [Google Scholar] [CrossRef]
- Yurttutan, M.E.; Sancak, K.T. The effect of kinesio taping with the web strip technique on pain, edema, and trismus after impacted mandibular third molar surgery. Niger. J. Clin. Pract. 2020, 23, 1260–1265. [Google Scholar] [CrossRef]
- Xue, P.; Wang, J.; Wu, B.; Ma, Y.; Wu, F.; Hou, R. Efficacy of antibiotic prophylaxis on postoperative inflammatory complications in Chinese patients having impacted mandibular third molars removed: A split-mouth, double-blind, self-controlled, clinical trial. Br. J. Oral. Maxillofac. Surg. 2015, 53, 416–420. [Google Scholar] [CrossRef]
- Mohammed, I.A.; Delemi, Z.H. Kinesiology Tape in Comparison with Submucosal Injection of Dexamethasone in Reducing Pain and Swelling After Surgical Removal of Impacted Lower Wisdom Teeth. Al Rafidain Dent. J. 2020, 20, 18–24. [Google Scholar] [CrossRef]
- Chiang, K.C.; Bhushan, N.S.; Kalyan, U.; Bhavana, R. Use of kinesiologic therapeutic tape on pain, trismus, swelling and its influence on quality of life after mandibular third molar surgery. J. Clin. Diagn. Res. 2020, 14, 13–17. [Google Scholar] [CrossRef]
- Bello, S.A.; Adeyemo, W.L.; Bamgbose, B.O.; Obi, E.V.; Adeyinka, A.A. Effect of age, impaction types and operative time on inflammatory tissue reactions following lower third molar surgery. Head Face Med. 2011, 7, 1–8. [Google Scholar] [CrossRef]
- Kau, C.H.; Cronin, A.; Durning, P.; Zhurov, A.I.; Sandham, A.; Richmond, S. A new method for the 3D measurement of postoperative swelling following orthognathic surgery. Orthod. Craniofac. Res. 2006, 9, 31–37. [Google Scholar] [CrossRef]
- Yip, E.; Smith, A.; Yoshino, M. Volumetric evaluation of facial swelling utilizing a 3-D range camera. Int. J. Oral. Maxillofac. Surg. 2004, 33, 179–182. [Google Scholar] [CrossRef]
- Metlerski, M.; Grocholewicz, K.; Jaroń, A.; Lipski, M.; Trybek, G. Comparison of Presurgical Dental Models Manufactured with Two Different Three-Dimensional Printing Techniques. J. Healthc. Eng. 2020, 2020, 8893338. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Feature | Study Group (n = 50) | Control Group (n = 50) | Total (n = 100) | p * | ||||
|---|---|---|---|---|---|---|---|---|
| Median | Min–Max | Median | Min–Max | Median | Min–Max | |||
| Age | 26.5 | 19–59 | 25 | 18–38 | 25.5 | 18–59 | 0.221 | |
| Operation time [min] | 21 | 10–60 | 24.5 | 6–60 | 23 | 6–60 | 0.801 | |
| Feature | n | % | n | % | n | % | p ** | |
| Sex | Woman | 36 | 72.00% | 38 | 76.00% | 74 | 74.00% | 0.82 |
| Man | 14 | 28.00% | 12 | 24.00% | 26 | 26.00% | ||
| Tooth number | 38 | 30 | 60.00% | 28 | 56.00% | 58 | 58.00% | 0.839 |
| 48 | 20 | 40.00% | 22 | 44.00% | 42 | 42.00% | ||
| Measurement on the 3rd Day (cm) | Group | n | Mean | SD | Median | Min | Max | Q1 | Q3 | p * |
|---|---|---|---|---|---|---|---|---|---|---|
| Line A | study | 50 | 11.75 | 0.78 | 11.55 | 10.45 | 13.5 | 11.1 | 12.4 | p = 0.336 |
| control | 50 | 11.89 | 0.91 | 11.78 | 10 | 14.5 | 11.45 | 12.5 | ||
| Line B | study | 50 | 15.42 | 1.07 | 15.07 | 13.6 | 18 | 14.56 | 16 | p = 0.304 |
| control | 50 | 15.52 | 0.84 | 15.43 | 14 | 18.05 | 15 | 16 | ||
| Line C | study | 50 | 8.42 | 0.89 | 8.35 | 6.95 | 11.25 | 7.78 | 8.91 | p = 0.724 |
| control | 50 | 8.45 | 0.67 | 8.22 | 7 | 10 | 8 | 9 | ||
| Line D | study | 50 | 9.99 | 0.75 | 10 | 8.5 | 12 | 9.5 | 10.45 | p = 0.008 |
| control | 50 | 10.35 | 0.79 | 10.22 | 8 | 12 | 10 | 10.97 | ||
| Line E | study | 50 | 14.89 | 0.9 | 15 | 12.5 | 16.6 | 14.16 | 15.5 | p = 0.005 |
| control | 50 | 15.44 | 0.9 | 15.5 | 13.5 | 16.9 | 14.75 | 16.24 |
| Measurement on the 7th Day (cm) | Group | n | Mean | SD | Median | Min | Max | Q1 | Q3 | p * |
|---|---|---|---|---|---|---|---|---|---|---|
| Line A | study | 50 | 11.52 | 0.76 | 11.5 | 10 | 13.4 | 11 | 12 | p = 0.964 |
| control | 50 | 11.53 | 0.87 | 11.5 | 9.75 | 13.75 | 10.96 | 12.04 | ||
| Line B | study | 50 | 15.15 | 1.13 | 15 | 12 | 18 | 14.5 | 15.76 | p = 0.714 |
| control | 50 | 15.02 | 0.86 | 15 | 13.25 | 17.05 | 14.5 | 15.57 | ||
| Line C | study | 50 | 8.2 | 0.74 | 8.15 | 7 | 10 | 7.55 | 8.66 | p = 0.732 |
| control | 50 | 8.22 | 0.54 | 8.07 | 7 | 9.25 | 8 | 8.5 | ||
| Line D | study | 50 | 9.8 | 0.77 | 10 | 8.25 | 11.5 | 9.25 | 10.15 | p = 0.227 |
| control | 50 | 9.93 | 0.93 | 10 | 7.75 | 11.5 | 9.51 | 10.57 | ||
| Line E | study | 50 | 14.57 | 0.95 | 14.53 | 12.1 | 16.6 | 14 | 15.24 | p = 0.029 |
| control | 50 | 15 | 0.94 | 15 | 12.8 | 16.5 | 14.26 | 16 |
| Jaw Opening (cm) | Group | n | Mean | SD | Median | Min | Max | Q1 | Q3 | p * |
|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | study | 50 | 4.73 | 0.72 | 4.62 | 3.5 | 6.5 | 4.01 | 5 | p = 0.135 |
| control | 50 | 4.5 | 0.56 | 4.43 | 3.75 | 6.1 | 4 | 4.93 | ||
| 3rd day | study | 50 | 2.93 | 1.08 | 3 | 1 | 5 | 2.02 | 3.73 | p = 0.012 |
| control | 50 | 2.42 | 0.69 | 2.5 | 1.25 | 4 | 1.85 | 2.79 | ||
| 7th day | study | 50 | 3.97 | 1.03 | 4.08 | 1.5 | 6.35 | 3.06 | 4.74 | p = 0.02 |
| control | 50 | 3.55 | 0.81 | 3.6 | 1.5 | 6 | 3 | 4 |
| Level of Pain Intensity (VAS) | Group | n | Mean | SD | Median | Min | Max | Q1 | Q3 | p * |
|---|---|---|---|---|---|---|---|---|---|---|
| Baseline | study | 50 | 5.2 | 10.74 | 0 | 0 | 30 | 0 | 0 | p = 0.065 |
| control | 50 | 1.6 | 5.48 | 0 | 0 | 20 | 0 | 0 | ||
| 3rd day | study | 50 | 37.6 | 25.36 | 30 | 0 | 90 | 20 | 50 | p = 0.003 |
| control | 50 | 52 | 23.82 | 50 | 0 | 100 | 40 | 70 | ||
| 7th day | study | 50 | 16.8 | 20.04 | 20 | 0 | 80 | 0 | 27.5 | p = 0.06 |
| control | 50 | 25 | 22.7 | 20 | 0 | 80 | 0 | 47.5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jaroń, A.; Preuss, O.; Grzywacz, E.; Trybek, G. The Impact of Using Kinesio Tape on Non-Infectious Complications after Impacted Mandibular Third Molar Surgery. Int. J. Environ. Res. Public Health 2021, 18, 399. https://doi.org/10.3390/ijerph18020399
Jaroń A, Preuss O, Grzywacz E, Trybek G. The Impact of Using Kinesio Tape on Non-Infectious Complications after Impacted Mandibular Third Molar Surgery. International Journal of Environmental Research and Public Health. 2021; 18(2):399. https://doi.org/10.3390/ijerph18020399
Chicago/Turabian StyleJaroń, Aleksandra, Olga Preuss, Elżbieta Grzywacz, and Grzegorz Trybek. 2021. "The Impact of Using Kinesio Tape on Non-Infectious Complications after Impacted Mandibular Third Molar Surgery" International Journal of Environmental Research and Public Health 18, no. 2: 399. https://doi.org/10.3390/ijerph18020399
APA StyleJaroń, A., Preuss, O., Grzywacz, E., & Trybek, G. (2021). The Impact of Using Kinesio Tape on Non-Infectious Complications after Impacted Mandibular Third Molar Surgery. International Journal of Environmental Research and Public Health, 18(2), 399. https://doi.org/10.3390/ijerph18020399