
Surgical Treatment Using Sinus Tarsi Approach with Anterolateral Fragment Open-Door Technique in Sanders Type 3 and 4 Displaced Intraarticular Calcaneal Fracture

 ,
,  , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
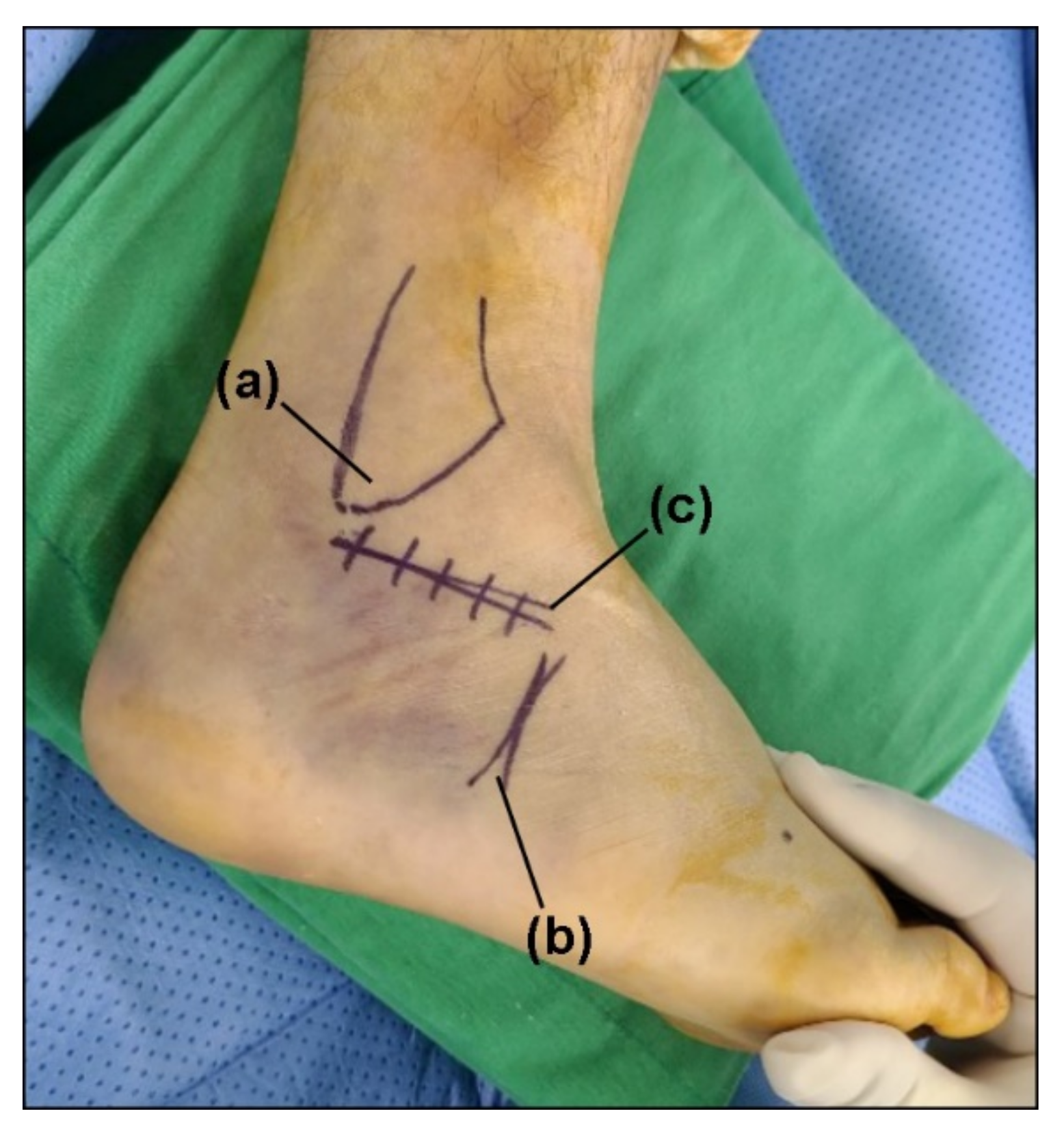
2.2. Surgical Technique
2.3. Postoperative Management
2.4. Radiologic Measurement
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Essex-Lopresti, P. The mechanism, reduction technique, and results in fractures of the os calcis. Br. J. Surg. 1952, 39, 395–419. [Google Scholar] [CrossRef] [PubMed]
- Tennent, T.D.; Calder, P.R.; Salisbury, R.D.; Allen, P.W.; Eastwood, D.M. The operative management of displaced intra-articular fractures of the calcaneum: A two-centre study using a defined protocol. Injury 2001, 32, 491–496. [Google Scholar] [CrossRef]
- Abidi, N.A.; Dhawan, S.; Gruen, G.S.; Vogt, M.T.; Conti, S.F. Wound-healing risk factors after open reduction and internal fixation of calcaneal fractures. Foot Ankle Int. 1998, 19, 856–861. [Google Scholar] [CrossRef] [PubMed]
- Lim, E.V.; Leung, J.P. Complications of intraarticular calcaneal fractures. Clin. Orthop. Relat. Res. 2001, 391, 7–16. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Su, Y.; Chen, W.; Zhang, Q.; Liu, Y.; Li, M.; Wang, H.; Zhang, Y. Functional outcome of displaced intra-articular calcaneal fractures: A comparison between open reduction/internal fixation and a minimally invasive approach featured an anatomical plate and compression bolts. J. Trauma Acute Care Surg. 2012, 73, 743–751. [Google Scholar] [CrossRef]
- Yeo, J.-H.; Cho, H.-J.; Lee, K.-B. Comparison of two surgical approaches for displaced intra-articular calcaneal fractures: Sinus tarsi versus extensile lateral approach. BMC Musculoskelet. Disord. 2015, 16, 63. [Google Scholar] [CrossRef] [Green Version]
- Weber, M.; Lehmann, O.; Sägesser, D.; Krause, F. Limited open reduction and internal fixation of displaced intra-articular fractures of the calcaneum. J. Bone Jt. Surgery. Br. Vol. 2008, 90, 1608–1616. [Google Scholar] [CrossRef]
- Holmes, G.B., Jr. Treatment of displaced calcaneal fractures using a small sinus tarsi approach. Tech Foot Ankle Surg 2005, 4, 35–41. [Google Scholar] [CrossRef]
- Schepers, T.; Kieboom, B.C.; Bessems, G.H.; Vogels, L.M.; van Lieshout, E.M.; Patka, P. Subtalar versus triple arthrodesis after intra-articular calcaneal fractures. Strateg. Trauma Limb Reconstr. 2010, 5, 97–103. [Google Scholar] [CrossRef] [Green Version]
- Wiley, W.B.; Norberg, J.D.; Klonk, C.J.; Alexander, I.J. “Smile” incision: An approach for open reduction and internal fixation of calcaneal fractures. Foot Ankle Int. 2005, 26, 590–592. [Google Scholar] [CrossRef] [Green Version]
- Palmer, I. The mechanism and treatment of fractures of the calcaneus; open reduction with the use of cancellous grafts. J. Bone Jt. Surgery. Am. Vol. 1948, 30, 2–8. [Google Scholar] [CrossRef]
- Ceccarini, P.; Manfreda, F.; Petruccelli, R.; Talesa, G.; Rinonapoli, G.; Caraffa, A. Minimally invasive sinus tarsi approach in Sanders II-III calcaneal fractures in high-demand patients. Med. Glas.: Off. Publ. Med Assoc. Zenica-Doboj Canton Bosnia Herzeg 2021, 18, 322–327. [Google Scholar] [CrossRef]
- Zeng, Z.; Yuan, L.; Zheng, S.; Sun, Y.; Huang, F. Minimally invasive versus extensile lateral approach for sanders type II and III calcaneal fractures: A meta-analysis of randomized controlled trials. Int. J. Surg. 2018, 50, 146–153. [Google Scholar] [CrossRef] [PubMed]
- Hospodar, P.; Guzman, C.; Johnson, P.; Uhl, R. Treatment of displaced calcaneus fractures using a minimally invasive sinus tarsi approach. Orthopedics 2008, 31, 1112. [Google Scholar] [CrossRef] [PubMed]
- Sanders, R.; Vaupel, Z.M.; Erdogan, M.; Downes, K. Operative treatment of displaced intraarticular calcaneal fractures: Long-term (10-20 Years) results in 108 fractures using a prognostic CT classification. J. Orthop. Trauma 2014, 28, 551–563. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H.; Chun, D.I.; Park, K.R.; Park, G.H.; Park, S.; Yang, J.; Cho, J. Can sural nerve injury be avoided in the sinus tarsi approach for calcaneal fracture: A cadaveric study. Medicine 2019, 98, e17611. [Google Scholar] [CrossRef] [PubMed]
- Schepers, T.; Ginai, A.Z.; Mulder, P.G.; Patka, P. Radiographic evaluation of calcaneal fractures: To measure or not to measure. Skelet. Radiol. 2007, 36, 847–852. [Google Scholar] [CrossRef] [Green Version]
- Ellis, S.J.; Williams, B.R.; Garg, R.; Campbell, G.; Pavlov, H.; Deland, J.T. Incidence of plantar lateral foot pain before and after the use of trial metal wedges in lateral column lengthening. Foot Ankle Int. 2011, 32, 665–673. [Google Scholar] [CrossRef]
- Leung, K.S.; Yuen, K.M.; Chan, W.S. Operative treatment of displaced intra-articular fractures of the calcaneum. Medium-term results. J. Bone Jt. Surgery. Br. Vol. 1993, 75, 196–201. [Google Scholar] [CrossRef] [PubMed]
- Kwon, D.G.; Chung, C.Y.; Lee, K.M.; Kim, T.W.; Sung, K.H.; Kim, D.H.; Park, M.S. Revisit of Broden’s view for intraarticular calcaneal fracture. Clin. Orthop. Surg. 2012, 4, 221–226. [Google Scholar] [CrossRef]
- Park, J.; Che, J.H. The sinus tarsi approach in displaced intra-articular calcaneal fractures. Arch. Orthop. Trauma Surg. 2017, 137, 1055–1065. [Google Scholar] [CrossRef]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Sanders, R.; Fortin, P.; DiPasquale, T.; Walling, A. Operative treatment in 120 displaced intraarticular calcaneal fractures. Results using a prognostic computed tomography scan classification. Clin. Orthop. Relat. Res. 1993, 290, 87–95. [Google Scholar]
- Epstein, N.; Chandran, S.; Chou, L. Current concepts review: Intra-articular fractures of the calcaneus. Foot Ankle Int. 2012, 33, 79–86. [Google Scholar] [CrossRef] [PubMed]
- Loucks, C.; Buckley, R. Bohler’s angle: Correlation with outcome in displaced intra-articular calcaneal fractures. J. Orthop. Trauma 1999, 13, 554–558. [Google Scholar] [CrossRef] [PubMed]
- Song, J.H.; Kang, C.; Hwang, D.S.; Kang, D.H.; Park, J.W. Extended Sinus Tarsi Approach for Treatment of Displaced Intraarticular Calcaneal Fractures Compared to Extended Lateral Approach. Foot Ankle Int. 2019, 40, 167–177. [Google Scholar] [CrossRef]
- Bedigrew, K.M.; Blair, J.A.; Possley, D.R.; Kirk, K.L.; Hsu, J.R. Comparison of Calcaneal Exposure Through the Extensile Lateral and Sinus Tarsi Approaches. Foot Ankle Spec. 2018, 11, 142–147. [Google Scholar] [CrossRef] [PubMed]
- Ceccarini, P.; Rinonapoli, G.; Antinolfi, P.; Caraffa, A. Effectiveness of ankle arthroscopic debridement in acute, subacute ankle- bimalleolar, and trimalleolar fractures. Int. Orthop. 2021, 45, 721–729. [Google Scholar] [CrossRef]
- Banerjee, S.; Gupta, A.; Elhence, A.; Choudhary, R. Arthroscopic Subtalar Arthrodesis as a Treatment Strategy for Subtalar Arthritis: A Systematic Review. J. Foot Ankle Surg.: Off. Publ. Am. Coll. Foot Ankle Surg. 2021, 60, 1023–1028. [Google Scholar] [CrossRef] [PubMed]
- Nosewicz, T.; Knupp, M.; Barg, A.; Maas, M.; Bolliger, L.; Goslings, J.C.; Hintermann, B. Mini-open sinus tarsi approach with percutaneous screw fixation of displaced calcaneal fractures: A prospective computed tomography—Based study. Foot Ankle Int. 2012, 33, 925–933. [Google Scholar] [CrossRef] [PubMed]
- Meng, Q.; Wang, Q.; Wu, X.; Peng, A.; Yan, J. Clinical application of the sinus tarsi approach in the treatment of intra-articular calcaneal fracture. Medicine 2018, 97, e0175. [Google Scholar] [CrossRef] [PubMed]
- Otero, J.E.; Westerlind, B.O.; Tantavisut, S.; Karam, M.D.; Phisitkul, P.; Akoh, C.C.; Gao, Y.; Marsh, J.L. There is poor reliability of Böhler’s angle and the crucial angle of Gissane in assessing displaced intra-articular calcaneal fractures. Foot Ankle Surg.: Off. J. Eur. Soc. Foot Ankle Surg. 2015, 21, 277–281. [Google Scholar] [CrossRef] [PubMed]
- Schepers, T. The sinus tarsi approach in displaced intra-articular calcaneal fractures: A systematic review. Int. Orthop. 2011, 35, 697–703. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lin, J.; Xie, C.; Chen, K.; Sun, S.; Zhou, K.; Zhou, C.; Shui, X.; Kong, J. Comparison of sinus tarsi approach versus extensile lateral approach for displaced intra-articular calcaneal fractures Sanders type IV. Int. Orthop. 2019, 43, 2141–2149. [Google Scholar] [CrossRef]
- Joseph, N.M.; Benedick, A.; McMellen, C.; Napora, J.; Wetzel, R.; Sontich, J.; Ochenjele, G. Acute Fixation of Displaced Intra-articular Calcaneus Fractures Is Safe Using the Sinus Tarsi Approach. J. Orthop. Trauma 2021, 35, 289–295. [Google Scholar] [CrossRef]
- Ho, C.J.; Huang, H.T.; Chen, C.H.; Chen, J.C.; Cheng, Y.M.; Huang, P.J. Open reduction and internal fixation of acute intra-articular displaced calcaneal fractures: A retrospective analysis of surgical timing and infection rates. Injury 2013, 44, 1007–1010. [Google Scholar] [CrossRef] [PubMed]
- Makki, D.; Alnajjar, H.M.; Walkay, S.; Ramkumar, U.; Watson, A.J.; Allen, P.W. Osteosynthesis of displaced intra-articular fractures of the calcaneum: A long-term review of 47 cases. J. Bone Jt. Surgery. Br. Vol. 2010, 92, 693–700. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Frequency Count (%) or Mean ± SD 1 |
|---|---|
| Sex | |
| Male | 22 (88%) |
| Female | 3 (12%) |
| Age (Year) | 55.84 ± 11.89 |
| Side | |
| Right | 13 (52%) |
| Left | 12 (48%) |
| BMI (kg/m2) | 23.45 ± 2.55 |
| History | |
| Diabetes | 2 (8%) |
| Smoking | 5 (20%) |
| Injury Mechanism | |
| Fall from <1 m | 4 (16%) |
| Fall from 1–2 m | 14 (56%) |
| Fall from >2 m | 6 (24%) |
| Traffic accidents | 1 (4%) |
| Sanders Classification | |
| III | 18 (72%) |
| IV | 7 (28%) |
| Associated other fractures | |
| Thoracic or Lumbar vertebra | 5 (20%) |
| Patella | 1 (4%) |
| Scaphoid | 1 (4%) |
| Time of injury to surgery (Days) | 3.28 ± 1.86 |
| Preoperative | Postoperative | p-Value * | |
|---|---|---|---|
| Bohler’s angle | 5.07 ± 13.43 | 24.23 ± 7.59 | <0.001 |
| Gissane’s angle | 109.72 ± 21.10 | 111.70 ± 6.82 | 0.6591 |
| Calcaneal height | 41.22 ± 5.71 | 47.31 ± 4.02 | <0.001 |
| Calcaneal length | 77.51 ± 5.67 | 78.97 ± 5.73 | 0.018 |
| Calcaneal width | 44.02 ± 4.33 | 41.38 ± 4.65 | 0.006 |
| Articular step-off | 4.28 ± 2.01 | 0.76 ± 0.98 | <0.001 + |
| CT Articular step-off | 5.65 ± 2.56 | 0.53 ± 0.83 | <0.001 + |
| Characteristics | Frequency Count (%) or Mean ± SD |
|---|---|
| Complication | |
| Superficial infection | 2 (8%) |
| Sural nerve injury | 0 (0%) |
| VAS score | 0.92 ± 0.95 |
| AOFAS score | 90.08 ± 6.44 |
| Follow up period (Months) | 15.28 ± 6.50 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cho, J.; Kim, J.; Kang, E.M.; Lee, J.S.; Min, T.-H.; Won, S.H.; Yi, Y.; Chun, D.-i. Surgical Treatment Using Sinus Tarsi Approach with Anterolateral Fragment Open-Door Technique in Sanders Type 3 and 4 Displaced Intraarticular Calcaneal Fracture. Int. J. Environ. Res. Public Health 2021, 18, 10400. https://doi.org/10.3390/ijerph181910400
Cho J, Kim J, Kang EM, Lee JS, Min T-H, Won SH, Yi Y, Chun D-i. Surgical Treatment Using Sinus Tarsi Approach with Anterolateral Fragment Open-Door Technique in Sanders Type 3 and 4 Displaced Intraarticular Calcaneal Fracture. International Journal of Environmental Research and Public Health. 2021; 18(19):10400. https://doi.org/10.3390/ijerph181910400
Chicago/Turabian StyleCho, Jaeho, Jahyung Kim, Eun Myeong Kang, Jeong Seok Lee, Tae-Hong Min, Sung Hun Won, Young Yi, and Dong-il Chun. 2021. "Surgical Treatment Using Sinus Tarsi Approach with Anterolateral Fragment Open-Door Technique in Sanders Type 3 and 4 Displaced Intraarticular Calcaneal Fracture" International Journal of Environmental Research and Public Health 18, no. 19: 10400. https://doi.org/10.3390/ijerph181910400
APA StyleCho, J., Kim, J., Kang, E. M., Lee, J. S., Min, T.-H., Won, S. H., Yi, Y., & Chun, D.-i. (2021). Surgical Treatment Using Sinus Tarsi Approach with Anterolateral Fragment Open-Door Technique in Sanders Type 3 and 4 Displaced Intraarticular Calcaneal Fracture. International Journal of Environmental Research and Public Health, 18(19), 10400. https://doi.org/10.3390/ijerph181910400