
Presence and Maturation Dynamics of Mandibular Third Molars and Their Influence on Late Mandibular Incisor Crowding: A Longitudinal Study

 ,
,
Abstract
:1. Introduction
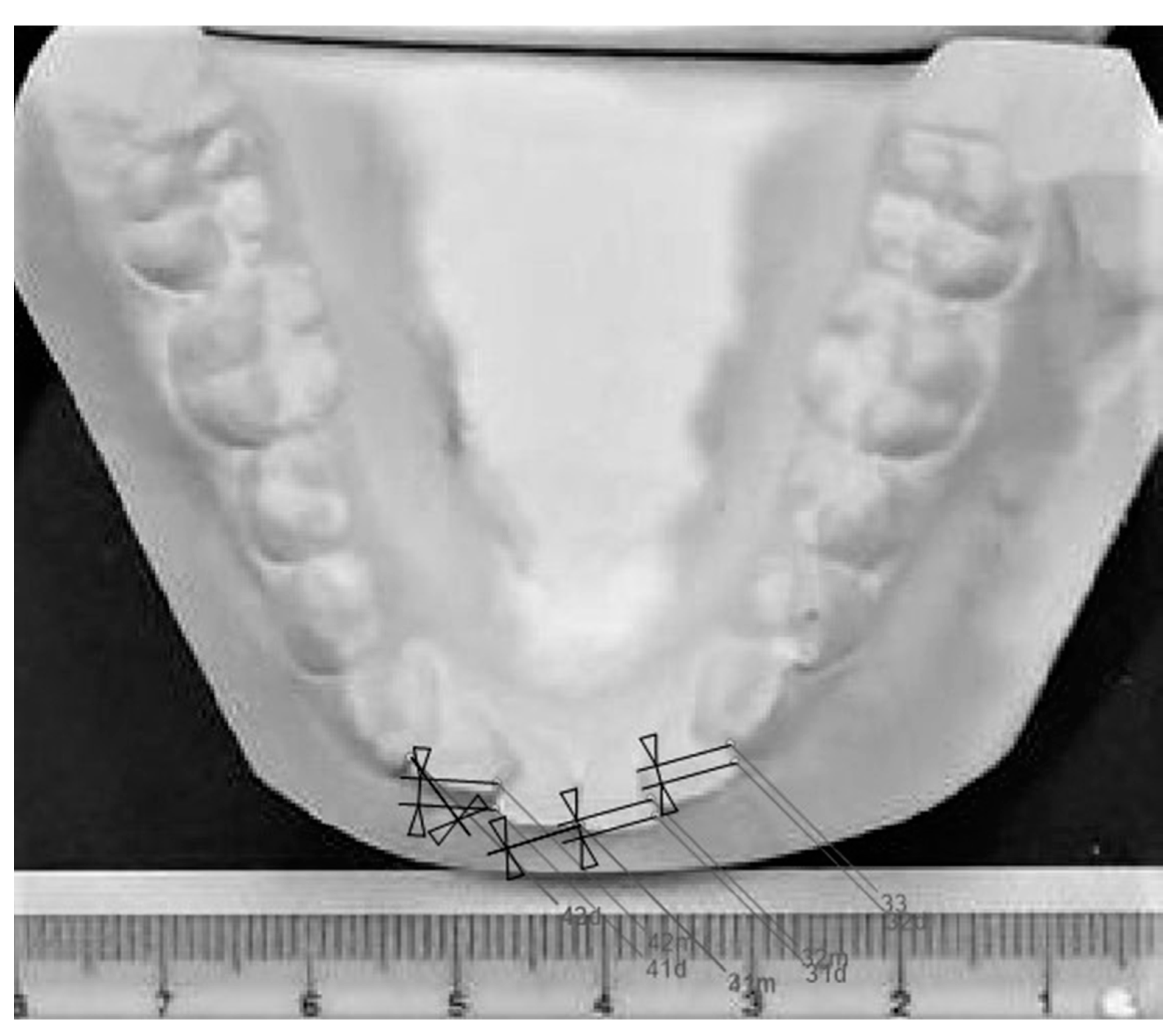
2. Materials and Methods
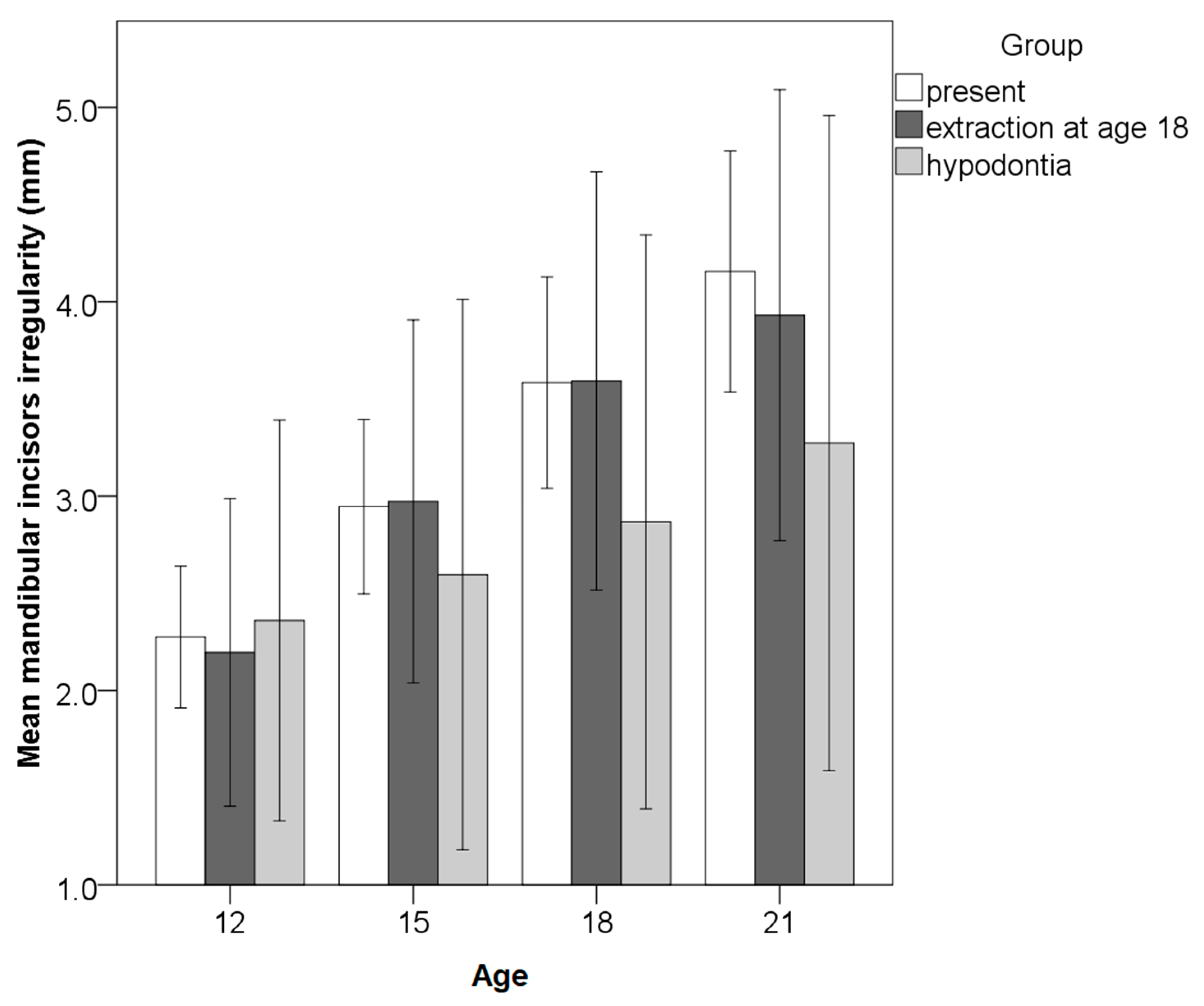
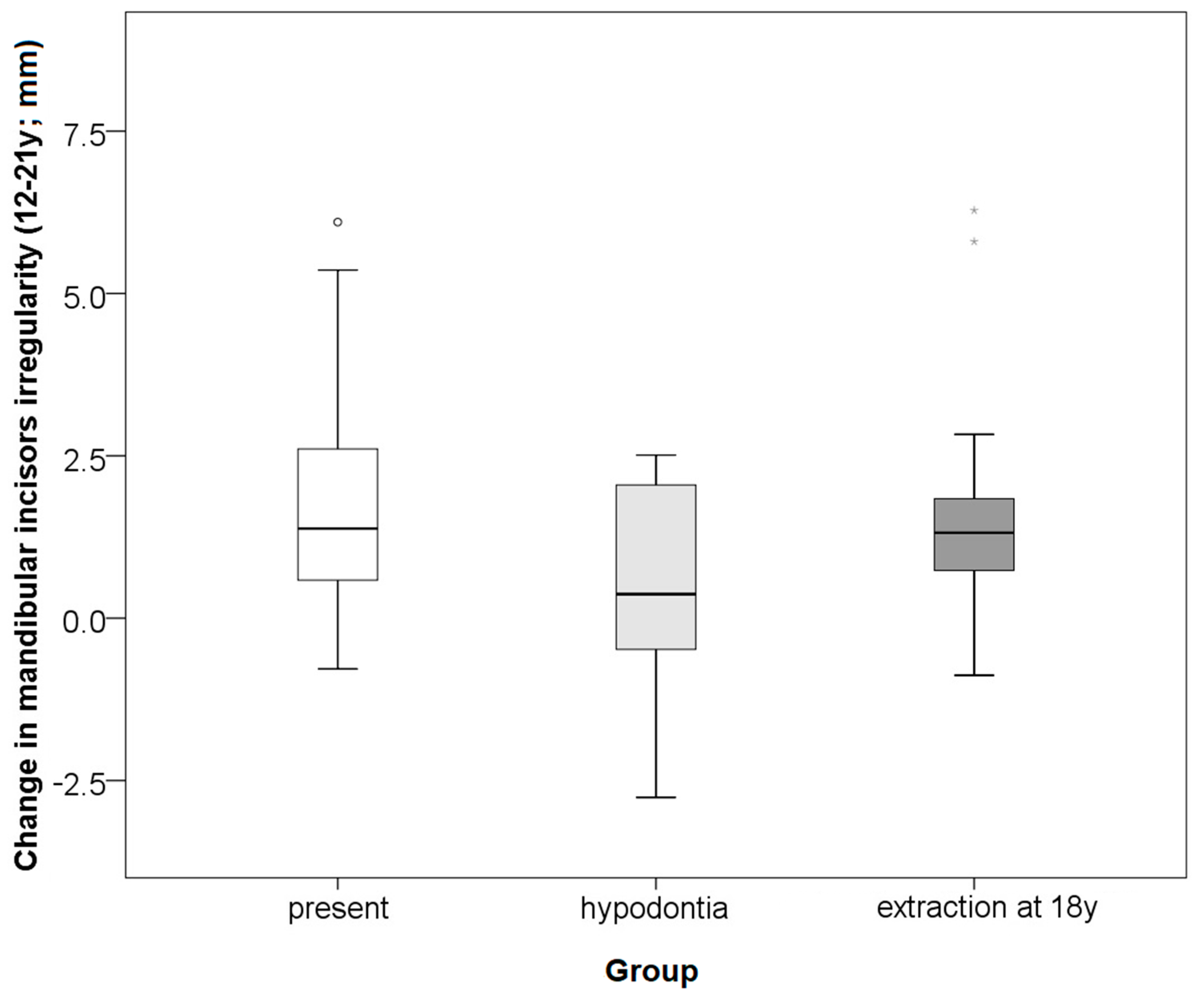
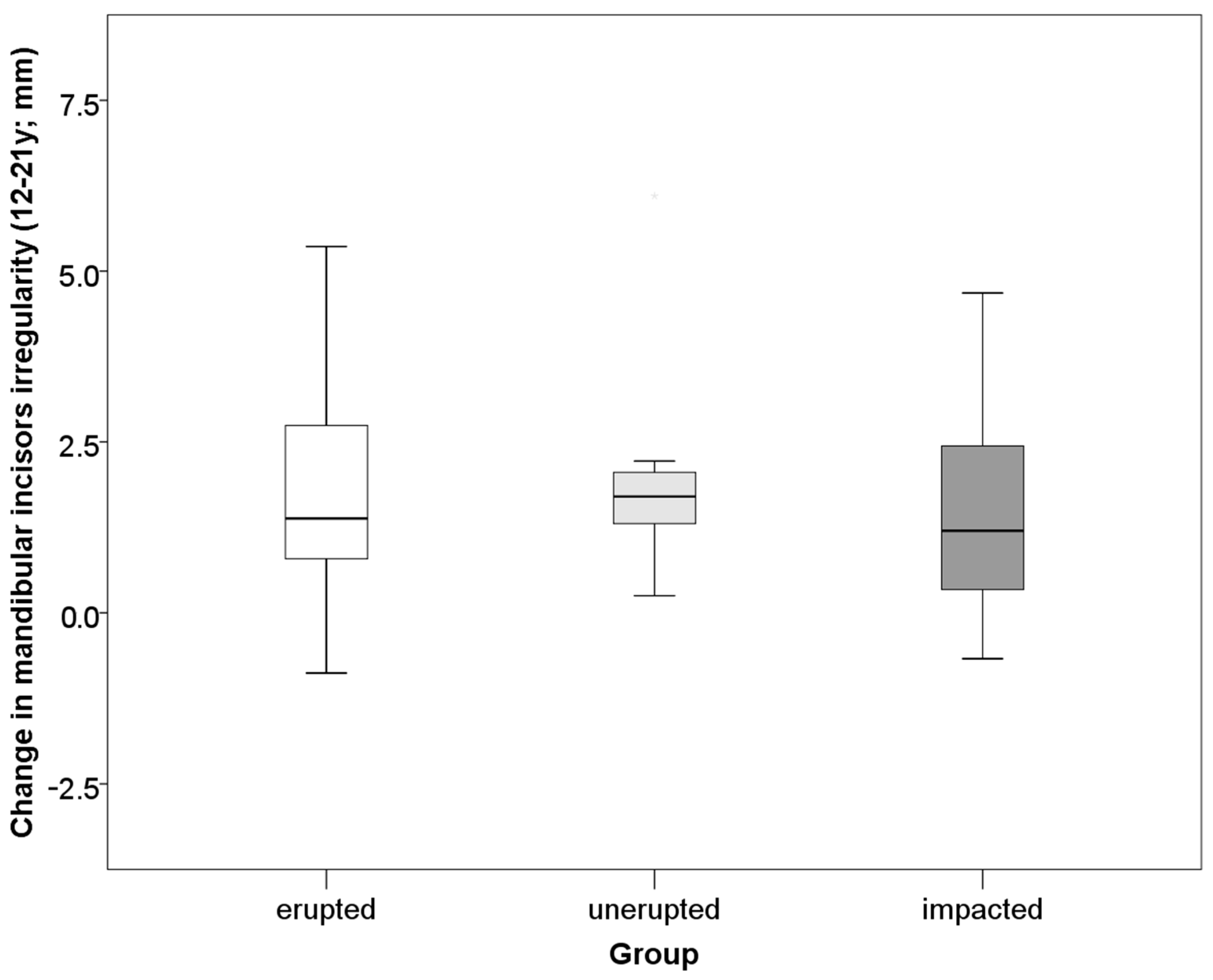
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Richardson, M.E. Late lower arch crowding in relation to skeletal and dental morphology and growth changes. Br. J. Orthod. 1996, 23, 249–254. [Google Scholar] [CrossRef]
- Ihlow, D.; Kubein-Meesenburg, D.; Fanghänel, J.; Lohrmann, B.; Elsner, V.; Nägerl, H. Biomechanics of the dental arch and incisal crowding. J. Orofac. Orthop. 2004, 65, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Harradine, N.W.T.; Pearson, M.H.; Toth, B. The effect of extraction of third molars on late lower incisor crowding: A randomized controlled trial. Br. J. Orthod. 1998, 25, 117–122. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lindqvist, B.; Thilander, B. Extraction of third molars in cases of anticipated crowding in the lower jaw. Am. J. Orthod. 1982, 81, 130–139. [Google Scholar] [CrossRef]
- Okşayan, R.; Topcuoglu, T. Effects of Mandibular Third Molar Angulation and Position on Crowding. Turk. J. Orthod. 2013, 26, 129–133. [Google Scholar] [CrossRef] [Green Version]
- Sood, A.; Bhullar, M.; Mittal, S.; Aggarwal, I.; Singla, D.; Sharma, A. Relationship of mandibular third molar to mandibular anterior crowding. Dent. J. Adv. Stud. 2018, 6, 89–96. [Google Scholar] [CrossRef] [Green Version]
- Niedzielska, I. Third molar influence on dental arch crowding. Eur. J. Orthod. 2005, 27, 518–523. [Google Scholar] [CrossRef]
- Hasegawa, Y.; Terada, K.; Kageyama, I.; Tsuchimochi, T.; Ishikawa, F.; Nakahara, S. Influence of third molar space on angulation and dental arch crowding. Odontology 2013, 101, 22–28. [Google Scholar] [CrossRef]
- Buschang, P.H.; Stroud, J.; Alexander, R.G. Differences in dental arch morphology among adult females with untreated Class I and Class II malocclusion. Eur. J. Orthod. 1994, 16, 47–52. [Google Scholar] [CrossRef] [PubMed]
- Marques, L.S.; Pordeus, I.A.; Ramos-Jorge, M.L.; Filogônio, C.A.; Filogônio, C.B.; Pereira, L.J.; Paiva, S.M. Factors associated with the desire for orthodontic treatment among Brazilian adolescents and their parents. BMC Oral Health 2009, 9, 34. [Google Scholar] [CrossRef] [Green Version]
- Dong, J.K.; Jin, T.H.; Cho, H.W.; Oh, S.C. The esthetics of the smile: A review of some recent studies. Int. J. Prosthodont. 1999, 12, 9–19. [Google Scholar]
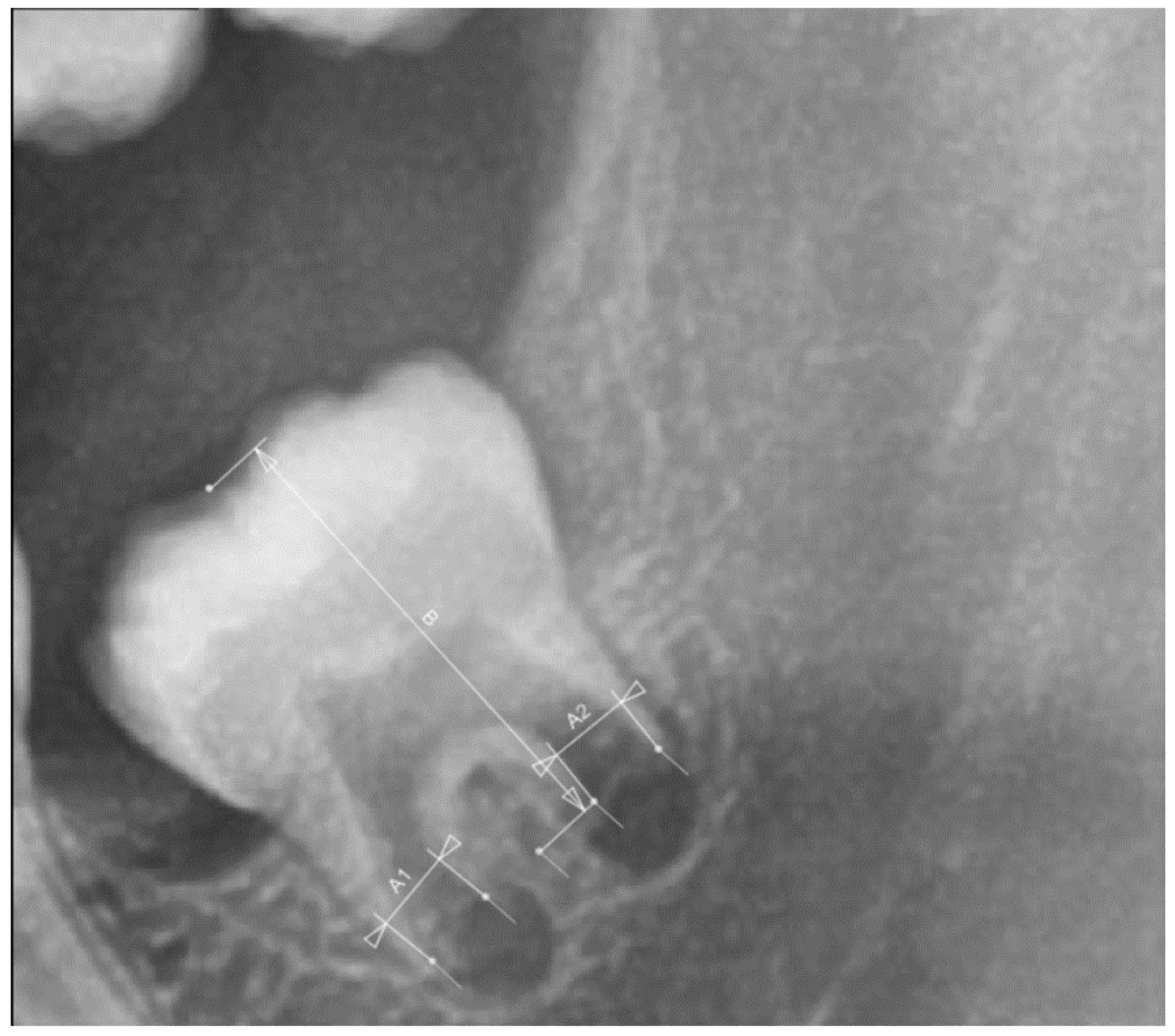
- Cameriere, R.; Ferrante, L.; Cingolani, M. Age estimation in children by measurement of open apices in teeth. Int. J. Leg. Med. 2006, 120, 49–52. [Google Scholar] [CrossRef] [Green Version]
- Galic, I.; Vodanović, M.; Cameriere, R.; Nakaš, E.; Galić, E.; Selimović, E.; Brkić, H. Accuracy of Cameriere, Haavikko, and Willems radiographic methods on age estimation on Bosnian-Herzegovian children age groups 6–13. Int. J. Leg. Med. 2011, 125, 315–321. [Google Scholar] [CrossRef] [PubMed]
- Mazzilli, L.E.N.; Melani, R.F.H.; Lascala, C.A.; Palacio, L.A.V.; Cameriere, R. Age estimation: Cameriere’s open apices methodology accuracy on a southeast Brazilian sample. J. Forensic Leg. Med. 2018, 58, 164–168. [Google Scholar] [CrossRef] [PubMed]
- Marinkovic, N.; Milovanovic, P.; Djuric, M.; Nedeljkovic, N.; Zelic, K. Dental maturity assessment in Serbian population: A comparison of Cameriere’s European formula and Willems’ method. Forensic Sci. Int. 2018, 288, e1–e331. [Google Scholar] [CrossRef] [PubMed]
- Gannepalli, A.; Balla, S.B.; Pacha, V.B.; Gandhi Babu, D.B.; Vinay, B.H.; Perkari, S. Applicability of Cameriere European formula for age estimation of 10-15 years legal threshold in South Indian population. J. Forensic Dent. Sci. 2019, 11, 78–83. [Google Scholar] [CrossRef] [PubMed]
- Cameriere, R.; De Angelis, D.; Ferrante, L.; Scarpino, F.; Cingolani, M. Age estimation in children by measurement of open apices in teeth: A European formula. Int. J. Leg. Med. 2007, 121, 449–453. [Google Scholar] [CrossRef] [Green Version]
- De Luca, S.; Biagi, R.; Begnoni, G.; Farronato, G.; Cingolani, M.; Merelli, V.; Ferrante, L.; Cameriere, R. Accuracy of Cameriere’s cut-off value for third molar in assessing 18 years of age. Forensic Sci. Int. 2014, 235, 102e1–102e6. [Google Scholar] [CrossRef]
- Legović, M.; Cehić, A. Longitudinal analysis of the development of eugnathia and dysgnathia from the primary dentition to the permanent dentition. Acta Stomatol. Croat. 1986, 20, 3–9. [Google Scholar]
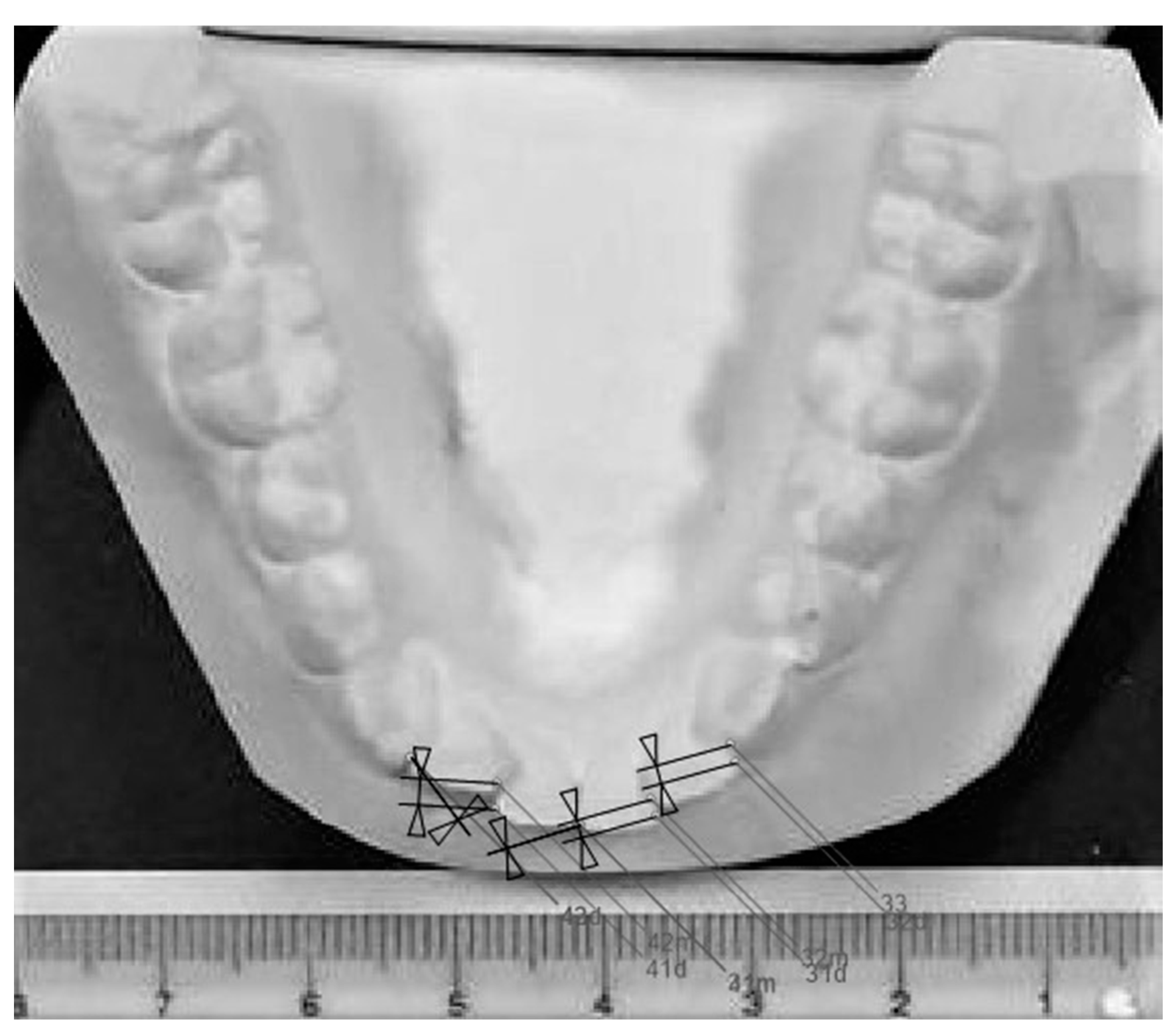
- Little, R.M. The irregularity index: A quantitative score of mandibular anterior alignment. Am. J. Orthod. 1975, 68, 554–563. [Google Scholar] [CrossRef]
- Bishara, S.E.; Jakobsen, J.R.; Treder, J.E.; Stasl, M.J. Changes in the maxillary and mandibular tooth size-arch length relationship from early adolescence to early adulthood: A longitudinal study. Am. J. Orthod. Dentofac. Orthop. 1989, 95, 46–59. [Google Scholar] [CrossRef]
- Zigante, M.; Pavlic, A.; Vandevska Radunovic, V.; Mathewson, A.; Kotarac Knezevic, A.; Spalj, S. Changes of mandibular dental arch shape during adolescence and its influence on late mandibular incisor crowding. Homo 2019, 70, 185–192. [Google Scholar] [CrossRef] [PubMed]
- Richardson, M.E. Late lower arch crowding in relation to primary crowding. Angle Orthod. 1982, 52, 300–312. [Google Scholar] [CrossRef] [PubMed]
- Ades, A.G.; Joondeph, D.R.; Little, R.M.; Chapko, M.K. A long-term study of the relationship of third molars to changes in the mandibular dental arch. Am. J. Orthod. Dentofac. Orthop. 1990, 97, 323–335. [Google Scholar] [CrossRef]
- Vego, L. A longitudinal study of mandibular arch perimeter. Angle Orthod. 1962, 32, 187–192. [Google Scholar] [CrossRef]
- Little, R.M.; Wallen, T.R.; Riedel, R.A. Stability and relapse of mandibular anterior alignment-first premolar extraction cases treated by traditional edgewise orthodontics. Am. J. Orthod. 1981, 80, 349–365. [Google Scholar] [CrossRef]
- Zawawi, K.H.; Melis, M. The role of mandibular third molars on lower anterior teeth crowding and relapse after orthodontic treatment: A systematic review. Sci. World J. 2014, 2014, 615429. [Google Scholar] [CrossRef]
- Stanaitytė, R.; Trakinienė, G.; Gervickas, A. Do wisdom teeth induce lower anterior teeth crowding? A systematic literature review. Stomatologija 2014, 16, 15–18. [Google Scholar]
- Genest-Beucher, S.; Graillon, N.; Bruneau, S.; Benzaquen, M.; Guyot, L. Does mandibular third molar have an impact on dental mandibular anterior crowding? A literature review. J. Stomatol. Oral Maxillofac. Surg. 2018, 119, 204–207. [Google Scholar] [CrossRef]
- Solow, B.; Siersbaek-Nielsen, S.; Greve, E. Airway adequacy, head posture, and craniofacial morphology. Am. J. Orthod. 1984, 86, 214–223. [Google Scholar] [CrossRef]
- Alam, M.K.; Hamza, M.A.; Khafiz, M.A.; Rahman, S.A.; Shaari, R.; Hassan, A. Multivariate analysis of factors affecting presence and/or agenesis of third molar tooth. PLoS ONE 2014, 9, e101157. [Google Scholar] [CrossRef] [PubMed]
- Karasawa, L.H.; Rossi, A.C.; Groppo, F.C.; Prado, F.B.; Caria, P.H.F. Cross-sectional study of correlation between mandibular incisor crowding and third molars in young Brazilians. Med. Oral Patol. Oral Cir. Bucal 2013, 18, 505–509. [Google Scholar] [CrossRef]
- Sujon, M.K.; Alam, M.K.; Rahman, S.A. Prevalence of third molar agenesis: Associated dental anomalies in non-syndromic 5923 patients. PLoS ONE 2016, 11, e0162070. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kindler, S.; Ittermann, T.; Bülow, R.; Holtfreter, B.; Klausenitz, C.; Metelmann, P.; Mksoud, M.; Pink, C.; Seebauer, C.; Kocher, T. Does craniofacial morphology affect third molars impaction? Results from a population-based study in northeastern Germany. PLoS ONE 2019, 14, e0225444. [Google Scholar] [CrossRef]
- Cheng, H.C.; Peng, B.Y.; Hsieh, H.Y.; Tam, K.W. Impact of third molars on mandibular relapse in post-orthodontic patients: A meta-analysis. J. Dent. Sci. 2018, 13, 1–7. [Google Scholar] [CrossRef]
- Kaygisiz, E.; Uzuner, F.D.; Yeniay, A.; Darendeliler, N. Secular trend in the maturation of permanent teeth in a sample of Turkish children over the past 30 years. Forensic Sci. Int. 2016, 259, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Sasso, A.; Spalj, S.; Mady Maricic, B.; Sasso, A.; Cabov, T.; Legović, M. Secular trend in the development of permanent teeth in a population of Istria and the littoral region of Croatia. J. Forensic Sci. 2013, 58, 673–677. [Google Scholar] [CrossRef]
- Yan-Vergnes, W.; Vergnes, J.N.; Dumonce, l.J.; Baron, P.; Marchal-Sixou, C.; Braga, J. Asynchronous dentofacial development and dental crowding: A cross-sectional study in a contemporary sample of children in France. J. Physiol. Anthropol. 2013, 32, 22. [Google Scholar] [CrossRef] [Green Version]
- Sasso, A.; Legovic, M.; Mady Maricic, B.; Pavlic, A.; Spalj, S. Secular trend of earlier onset and decelerated development of third molars: Evidence from Croatia. Forensic Sci. Int. 2015, 249, 202–206. [Google Scholar] [CrossRef]
- Meinl, A.; Tangl, S.; Huber, C.; Maurerd, B.; Watzekc, G. The chronology of third molar mineralization in the Austrian population--a contribution to forensic age estimation. Forensic Sci. Int. 2007, 169, 161–167. [Google Scholar] [CrossRef]
- von Cramon-Taubadel, N. Global human mandibular variation reflects differences in agricultural and hunter-gatherer subsistence strategies. Proc. Natl. Acad. Sci. USA 2011, 108, 19546–19551. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Normando, D.; Almeida, M.A.O.; Quintão, C.C.A. Dental crowding. Angle Orthod. 2013, 83, 10–15. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Mean ± SD | Median (IQR) | Range (Min–Max) |
|---|---|---|---|
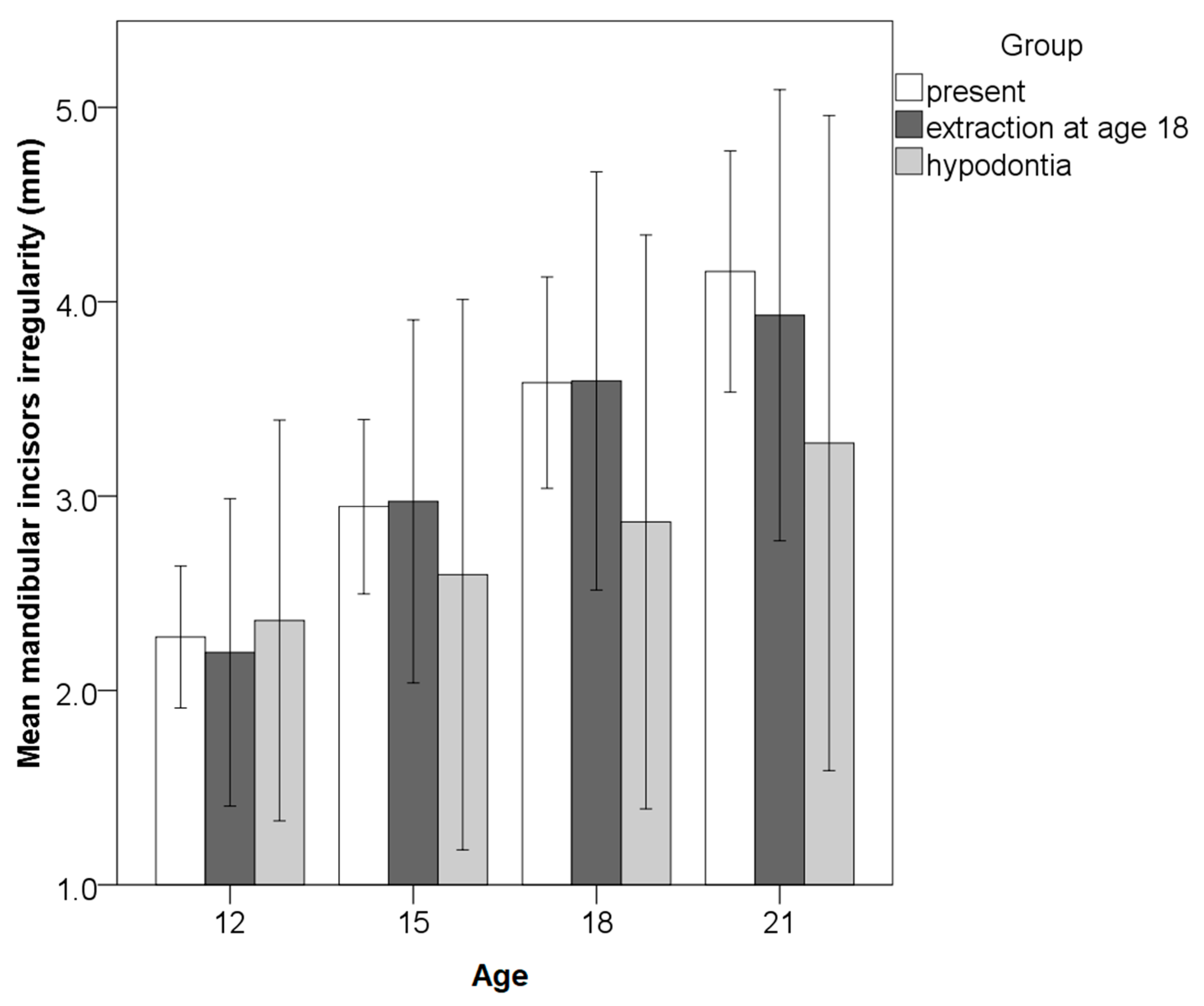
| Irregularity index 12 years (mm) | 2.4 ± 1.3 | 2.2 (1.4–3.2) | 0.4–5.7 |
| Irregularity index 21 years (mm) | 3.9 ± 2.0 | 3.8 (2.3–4.7) | 0.9–10.4 |
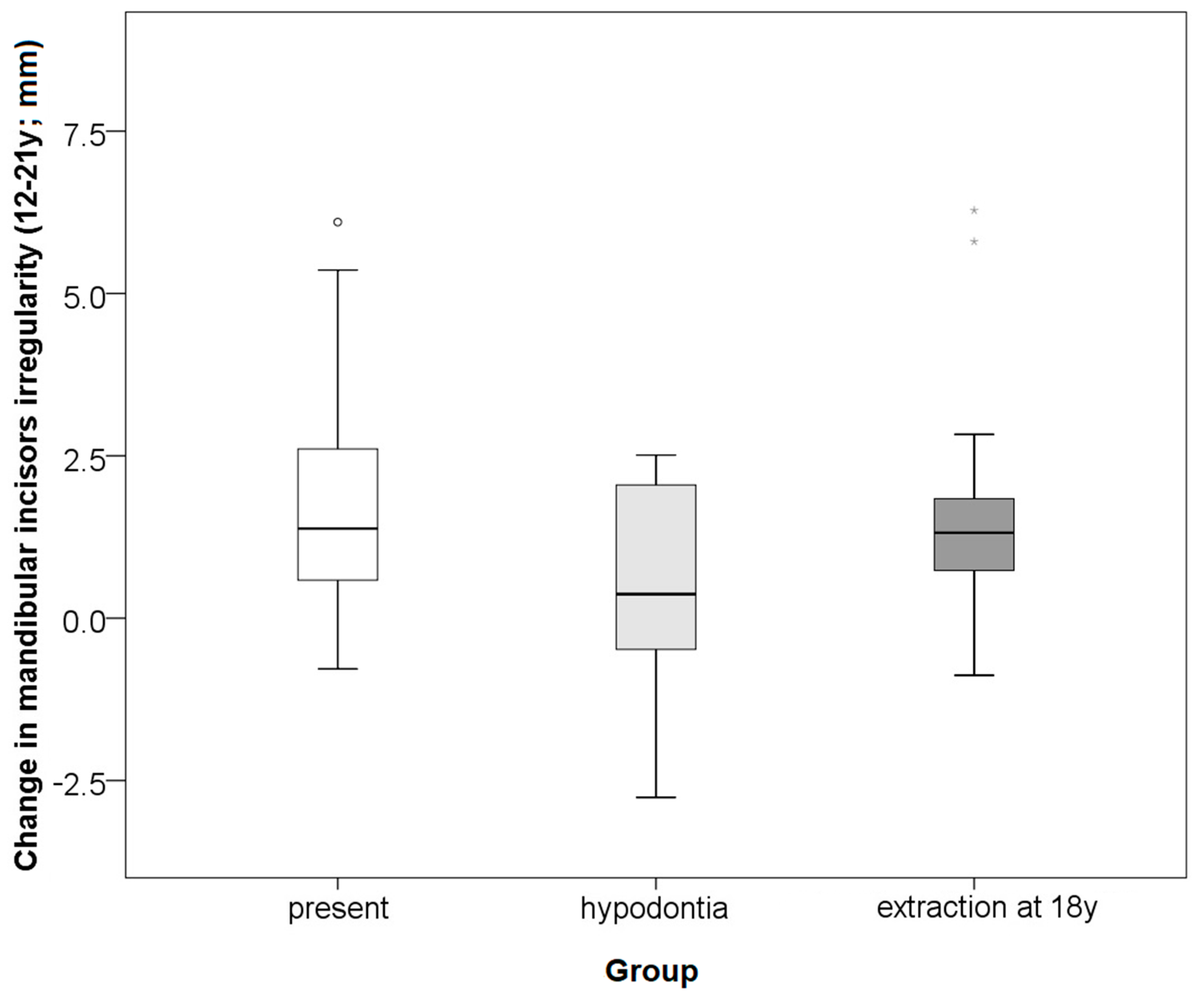
| Change of irregularity index 21–12 years (mm) | 1.6 ± 1.7 | 1.4 (0.5–2.5) | −2.8–6.3 |
| Cameriere’s index 15 years | 0.95 ± 0.37 | 0.89 (0.77–1.10) | 0.28–2.27 |
| Cameriere’s index 18 years | 0.28 ± 0.24 | 0.20 (0.10–0.39) | 0.01–0.97 |
| Cameriere’s index 21 years | 0.05 ± 0.11 | 0.01 (0.01–0.02) | 0.00–0.58 |
| Change of Cameriere’s index 18-15 years | 0.68 ± 0.23 | 0.67 (0.50–0.82) | 0.24–1.36 |
| Change of Cameriere’s index 21-18 years | 0.23 ± 0.15 | 0.20 (0.11–0.34) | 0.01–0.68 |
| Change of Cameriere’s index 21-15 years | 0.90 ± 0.31 | 0.87 (0.74–1.06) | 0.26–2.00 |
| Group | Incidence of Additional Irregularity (≥1 mm) | Incidence of Additional Irregularity (≥2 mm) | Mean ± SD | Median (IQR) | Range (Min–Max) |
|---|---|---|---|---|---|
| Third molars present at 21 years | 65% | 38% | 1.8 ± 1.6 | 1.4 (0.6–2.7) | −0.8–6.1 |
| Hypodontia of third molars | 38% | 25% | 0.5 ± 1.8 | 0.4 (−0.6–2.2) | −2.8–2.5 |
| Extraction of the third molars at 18 years | 75% | 19% | 1.7 ± 2.0 | 1.3 (0.6–1.9) | −0.9–6.3 |
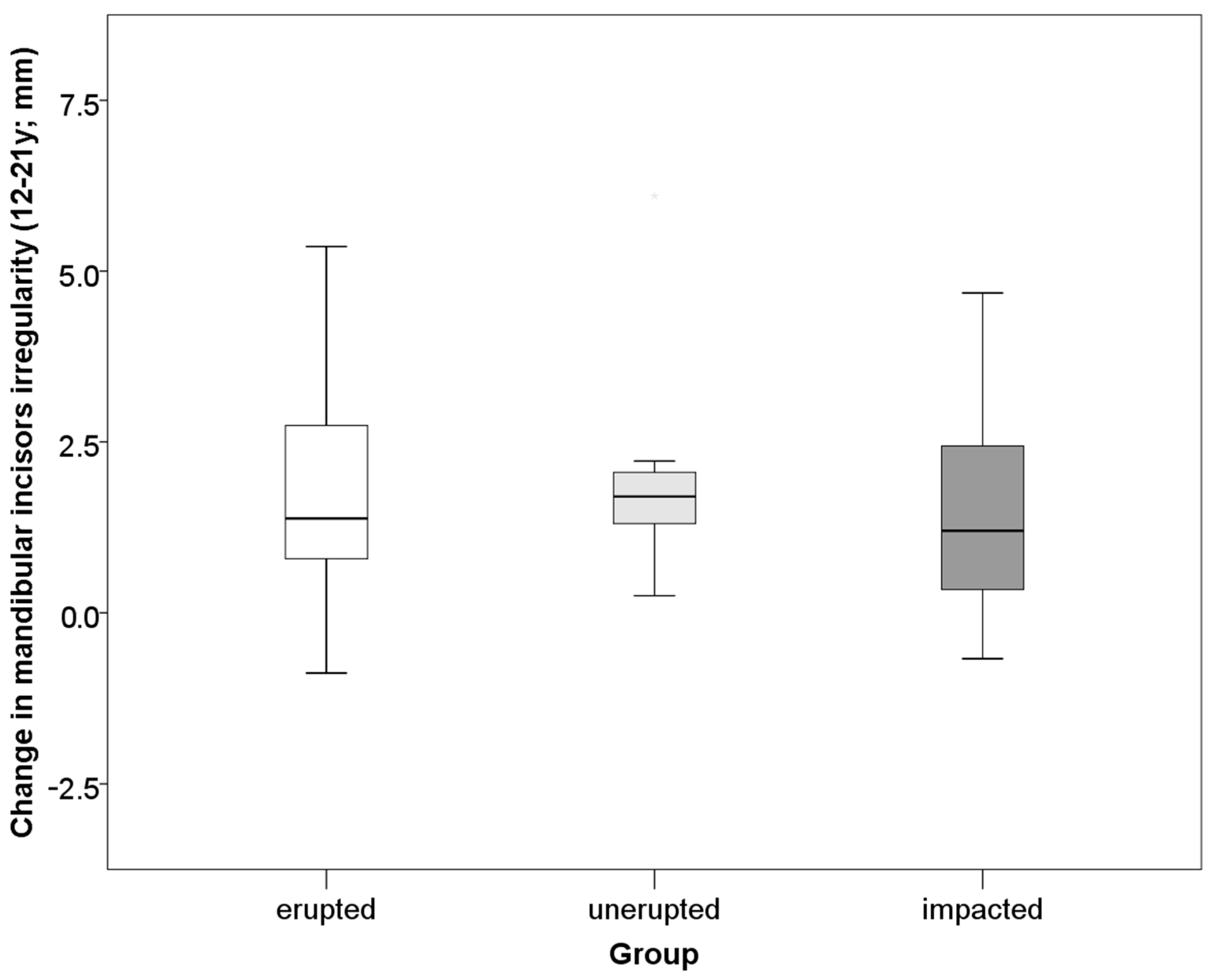
| Impacted at 21 years | 53% | 29% | 1.3 ± 1.4 | 1.2 (0.3–2.5) | −0.7–4.7 |
| Unerupted at 21 years | 82% | 27% | 1.9 ± 1.5 | 1.7 (1.3–2.2) | 0.3–6.1 |
| Erupted at 21 years | 65% | 39% | 1.7 ± 1.6 | 1.4 (0.7–2.8) | −0.9–5.4 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zigante, M.; Pavlic, A.; Morelato, L.; Vandevska-Radunovic, V.; Spalj, S. Presence and Maturation Dynamics of Mandibular Third Molars and Their Influence on Late Mandibular Incisor Crowding: A Longitudinal Study. Int. J. Environ. Res. Public Health 2021, 18, 10070. https://doi.org/10.3390/ijerph181910070
Zigante M, Pavlic A, Morelato L, Vandevska-Radunovic V, Spalj S. Presence and Maturation Dynamics of Mandibular Third Molars and Their Influence on Late Mandibular Incisor Crowding: A Longitudinal Study. International Journal of Environmental Research and Public Health. 2021; 18(19):10070. https://doi.org/10.3390/ijerph181910070
Chicago/Turabian StyleZigante, Martina, Andrej Pavlic, Luka Morelato, Vaska Vandevska-Radunovic, and Stjepan Spalj. 2021. "Presence and Maturation Dynamics of Mandibular Third Molars and Their Influence on Late Mandibular Incisor Crowding: A Longitudinal Study" International Journal of Environmental Research and Public Health 18, no. 19: 10070. https://doi.org/10.3390/ijerph181910070
APA StyleZigante, M., Pavlic, A., Morelato, L., Vandevska-Radunovic, V., & Spalj, S. (2021). Presence and Maturation Dynamics of Mandibular Third Molars and Their Influence on Late Mandibular Incisor Crowding: A Longitudinal Study. International Journal of Environmental Research and Public Health, 18(19), 10070. https://doi.org/10.3390/ijerph181910070