
Stability of Class II Malocclusion Treatment with the Austro Repositioner Followed by Fixed Appliances in Brachyfacial Patients

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Samples
- -
- Experimental group: 30 consecutively treated patients, selected from a private practice and treated by the same orthodontist (M.D.A.-M.). The sample was composed of 16 boys and 14 girls, with a mean age of 11.9 (at T1), 14.3 (at T2), and 15.7 (at T3).
- -
- Control group: 30 untreated patients selected from the online Craniofacial Growth Legacy Collection (http://www.aaoflegacycollection.org, accessed on 20 February 2015), which consists of several well-known growth studies such as the Burlington and Michigan growth studies. The sample was composed of 17 boys and 13 girls, with a mean age of 11.7 (at T1), 14.3 (at T2), and 15.6 (at T3).
2.1.1. Inclusion Criteria
2.1.2. Exclusion Criteria
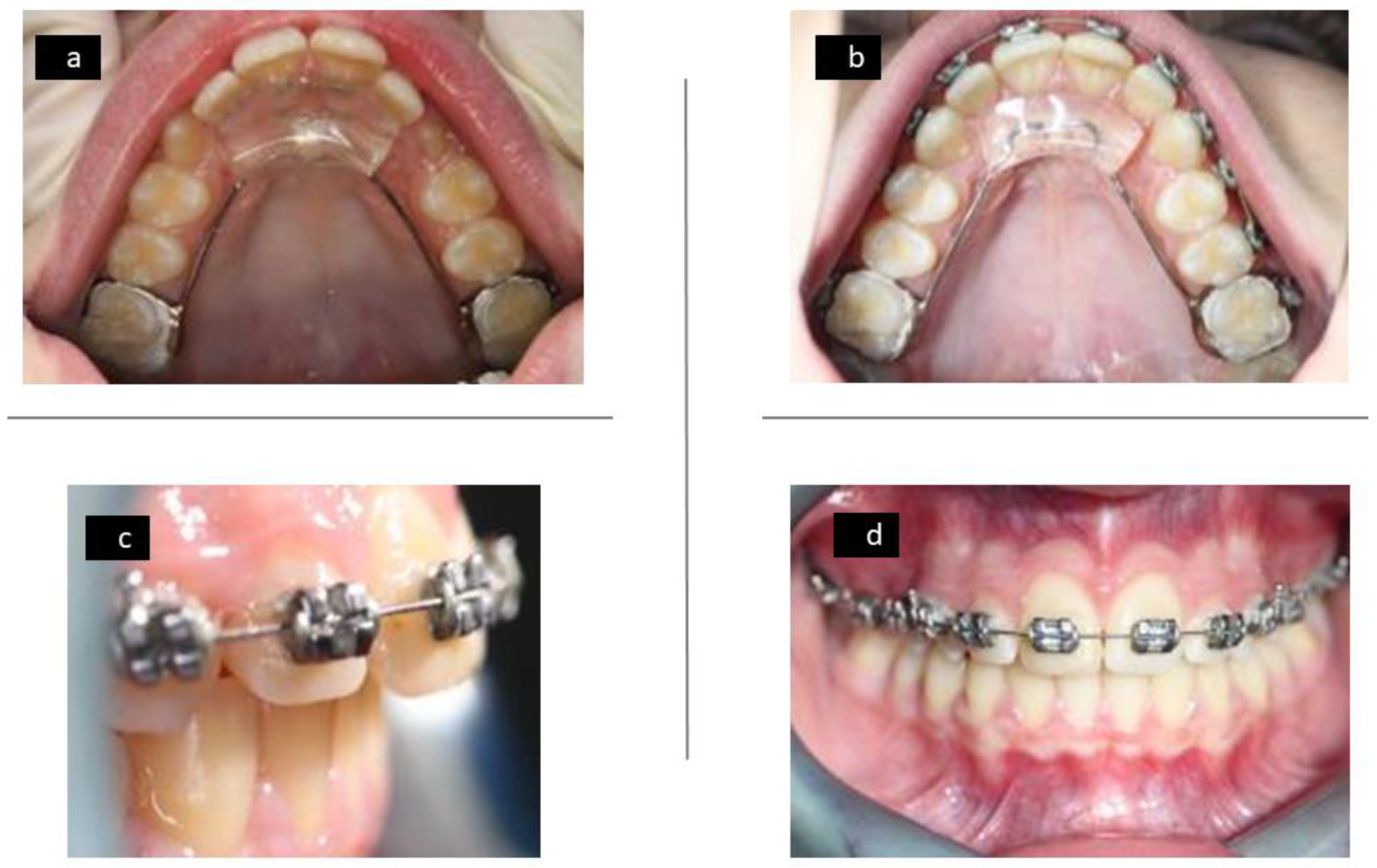
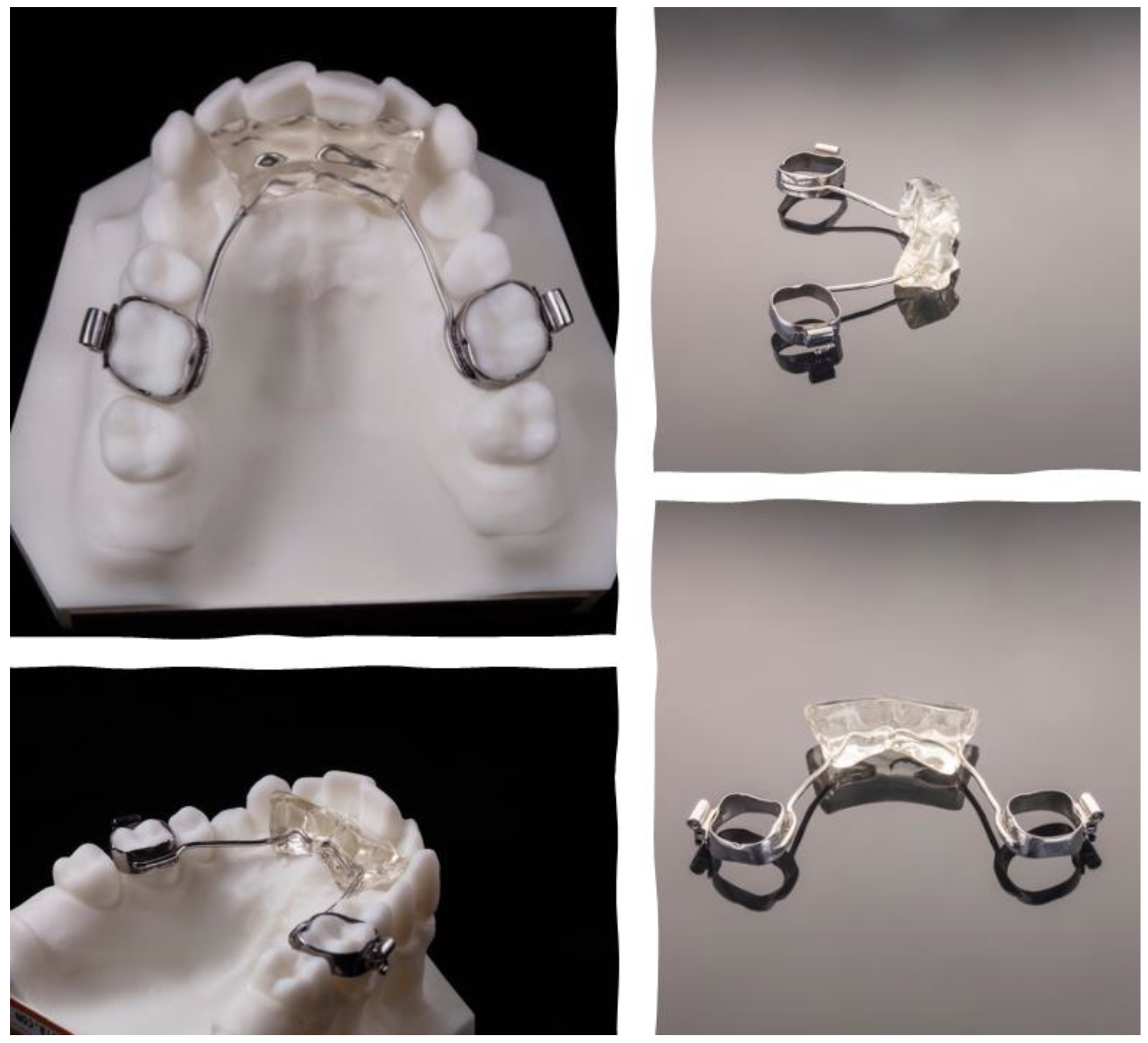
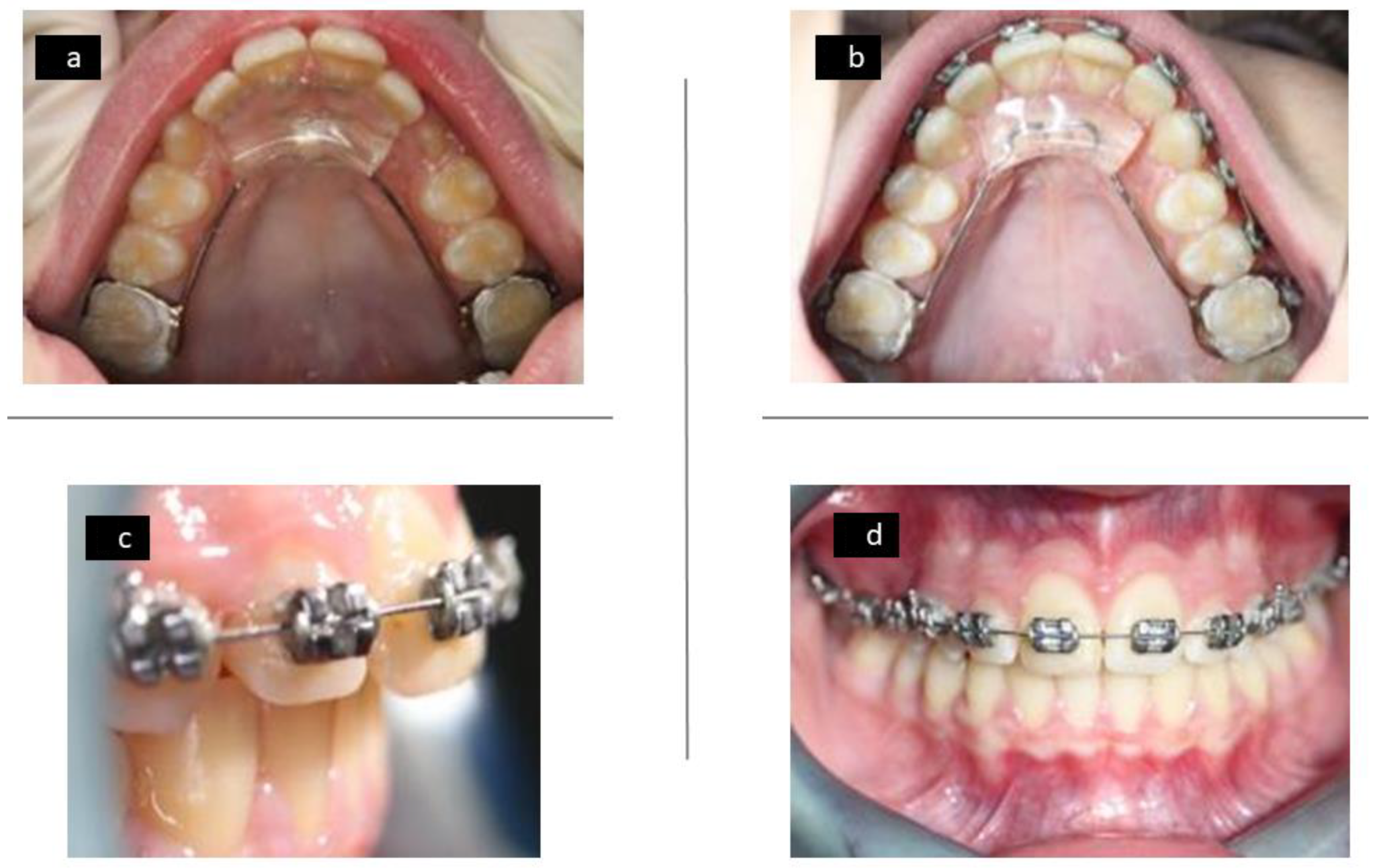
2.2. Class II Malocclusion Treatment Protocol
2.3. Measurement Method
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Buschang, P.H.; Martins, J. Childhood and adolescent changes of skeletal relationships. Angle Orthod. 1998, 68, 199–206; discussion 207–208. [Google Scholar] [CrossRef] [PubMed]
- McNamara, J.A., Jr. Components of class II malocclusion in children 8–10 years of age. Angle Orthod. 1981, 51, 177–202. [Google Scholar] [CrossRef] [PubMed]
- Nelson, B.; Hansen, K.; Hagg, U. Class II correction in patients treated with class II elastics and with fixed functional appliances: A comparative study. Am. J. Orthod. Dentofac. Orthop. 2000, 118, 142–149. [Google Scholar] [CrossRef]
- Souki, B.Q.; Vilefort, P.L.C.; Oliveira, D.D.; Andrade, I., Jr.; Ruellas, A.C.; Yatabe, M.S.; Nguyen, T.; Franchi, L.; McNamara, J.A., Jr.; Cevidanes, L.H.S. Three-dimensional skeletal mandibular changes associated with Herbst appliance treatment. Orthod. Craniofac. Res. 2017, 20, 111–118. [Google Scholar] [CrossRef] [PubMed]
- Zymperdikas, V.F.; Koretsi, V.; Papageorgiou, S.N.; Papadopoulos, M.A. Treatment effects of fixed functional appliances in patients with Class II malocclusion: A systematic review and meta-analysis. Eur. J. Orthod. 2016, 38, 113–126. [Google Scholar] [CrossRef]
- Franchi, L.; Alvetro, L.; Giuntini, V.; Masucci, C.; DeFraia, E.; Baccetti, T. Effectiveness of comprehensive fixed appliance treatment used with the Forsus Fatigue Resistant Device in Class II patients. Angle Orthod. 2011, 81, 678–683. [Google Scholar] [CrossRef] [Green Version]
- Pancherz, H.; Bjerklin, K.; Hashemi, K. Late adult skeletofacial growth after adolescent Herbst therapy: A 32-year longitudinal follow-up study. Am. J. Orthod. Dentofac. Orthop. 2015, 147, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Bock, N.C.; Von Bremen, J.; Ruf, S. Stability of Class II fixed functional appliance therapy—A systematic review and meta-analysis. Eur. J. Orthod. 2015, 38, 129–139. [Google Scholar] [CrossRef]
- Hansen, K.; Pancherz, H.; Hägg, U. Long-term effects of the Herbst appliance in relation to the treatment growth period: A cephalometric study. Eur. J. Orthod. 1991, 13, 471–481. [Google Scholar] [CrossRef]
- Austro, M.D.; Gonzalez, E.; Penalver, M.A.; Perez, D.; Alarcon, J.A. Short-term dentoskeletal changes following Class II treatment using a fixed functional appliance: The Austro Repositioner: A pilot study. J. Orofac. Orthop. 2018, 79, 147–156. [Google Scholar] [CrossRef]
- Linjawi, A.I.; Abbassy, M.A. Dentoskeletal effects of the forsus fatigue resistance device in the treatment of class II malocclusion: A systematic review and meta-analysis. J. Orthod. Sci. 2018, 7, 5. [Google Scholar] [CrossRef]
- Atresh, A.; Cevidanes, L.H.S.; Yatabe, M.; Muniz, L.; Nguyen, T.; Larson, B.; Manton, D.J.; Schneider, P.M. Three-dimensional treatment outcomes in Class II patients with different vertical facial patterns treated with the Herbst appliance. Am. J. Orthod. Dentofac. Orthop. 2018, 154, 238–248.e1. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Zhu, Y.; Long, H.; Zhou, Y.; Jian, F.; Ye, N.; Gao, M.; Lai, W. The effectiveness of the Herbst appliance for patients with Class II malocclusion: A meta-analysis. Eur. J. Orthod. 2016, 38, 324–333. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ehsani, S.; Nebbe, B.; Normando, D.; Lagravere, M.O.; Flores-Mir, C. Short-term treatment effects produced by the Twin-block appliance: A systematic review and meta-analysis. Eur. J. Orthod. 2015, 37, 170–176. [Google Scholar] [CrossRef] [Green Version]
- Baccetti, T.; Franchi, L.; McNamara, J.A., Jr. The cervical vertebral maturation (CVM) method for the assessment of optimal treatment timing in dentofacial orthopedics. Semin. Orthod. 2005, 11, 119–129. [Google Scholar] [CrossRef]
- Steiner, C.C. Cephalometrics for you and me. Am. J. Orthod. 1953, 39, 729–755. [Google Scholar] [CrossRef]
- Ricketts, R.M. Perspectives in the clinical application of cephalometrics. The first fifty years. Angle Orthod. 1981, 51, 115–150. [Google Scholar] [CrossRef] [PubMed]
- McNamara, J.A., Jr. A method of cephalometric evaluation. Am. J. Orthod. 1984, 86, 449–469. [Google Scholar] [CrossRef]
- Viera, A.J.; Garrett, J.M. Understanding interobserver agreement: The kappa statistic. Fam. Med. 2005, 37, 360–363. [Google Scholar] [PubMed]
- Cacciatore, G.; Alvetro, L.; Defraia, E.; Ghislanzoni, L.T.; Franchi, L. Active-treatment effects of the Forsus fatigue resistant device during comprehensive Class II correction in growing patients. Korean J. Orthod. 2014, 44, 136–142. [Google Scholar] [CrossRef]
- Sidlauskas, A. The effects of the Twin-block appliance treatment on the skeletal and dentolaveolar changes in Class II Division 1 malocclusion. Medicina 2005, 41, 392–400. [Google Scholar] [PubMed]
- Gunay, E.A.; Arun, T.; Nalbantgil, D. Evaluation of the Immediate Dentofacial Changes in Late Adolescent Patients Treated with the ForsusTM FRD. Eur. J. Dent. 2011, 5, 423–432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pancherz, H. The mechanism of Class II correction in Herbst appliance treatment. A cephalometric investigation. Am. J. Orthod. 1982, 82, 104–113. [Google Scholar] [CrossRef]
- de Almeida, M.R.; Henriques, J.F.; de Almeida, R.R.; Weber, U.; McNamara, J.A., Jr. Short-term treatment effects produced by the Herbst appliance in the mixed dentition. Angle Orthod. 2005, 75, 540–547. [Google Scholar] [CrossRef] [PubMed]
- Ruf, S.; Pancherz, H. The effect of Herbst appliance treatment on the mandibular plane angle: A cephalometric roentgenographic study. Am. J. Orthod. Dentofac. Orthop. 1996, 110, 225–229. [Google Scholar] [CrossRef]
- Aras, I.; Pasaoglu, A. Class II subdivision treatment with the Forsus Fatigue Resistant Device vs intermaxillary elastics. Angle Orthod. 2017, 87, 371–376. [Google Scholar] [CrossRef] [Green Version]
- Jena, A.K.; Duggal, R.; Parkash, H. Skeletal and dentoalveolar effects of Twin-block and bionator appliances in the treatment of Class II malocclusion: A comparative study. Am. J. Orthod. Dentofac. Orthop. 2006, 130, 594–602. [Google Scholar] [CrossRef]
- Baccetti, T.; Franchi, L.; Toth, L.R.; McNamara, J.A., Jr. Treatment timing for Twin-block therapy. Am. J. Orthod. Dentofac. Orthop. 2000, 118, 159–170. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Measurements | Treated Group | Control Gruop | p Value | |||
|---|---|---|---|---|---|---|
| Mean | SD | Mean | SD | |||
| SNA (°) | 82.1 | 1.84 | 82.07 | 1.77 | 0.827 | NS |
| SNB (°) | 75.32 | 1.72 | 75.38 | 1.52 | 0.91 | NS |
| ANB (°) | 6.72 | 1.31 | 6.68 | 0.98 | 0.545 | NS |
| Pt A-Na perp (mm) | 2.76 | 1.65 | 2.8 | 2.07 | 0.487 | NS |
| Pg-Na perp (mm) | −2.59 | 1.18 | −2.44 | 1.42 | 0.657 | NS |
| Co-Pg (mm) | 100.54 | 2.24 | 100.51 | 2.17 | 0.994 | NS |
| FMA (°) | 19.41 | 0.27 | 19.47 | 0.31 | 0.495 | NS |
| LAFH (mm) | 53.93 | 2.47 | 53.98 | 1.13 | 0.838 | NS |
| OB (mm) | 6.01 | 1.57 | 6.04 | 2.45 | 0.568 | NS |
| OJ (mm) | 6.81 | 1.12 | 6.86 | 1.43 | 0.375 | NS |
| U1 to SN (°) | 103.56 | 2.27 | 103.08 | 2.81 | 0.627 | NS |
| L1 to GoMe (°) | 93.11 | 1.41 | 93.23 | 1.43 | 0.281 | NS |
| Interincisal Angle (°) | 127.01 | 3.51 | 127.97 | 3.37 | 0.933 | NS |
| Measurements | Treated Group | Control Group | Treated vs. Control | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean Differences | SD | p Value | Mean Differences | SD | p Value | p Value | ||||
| SNA (°) | −0.19 | 1.31 | 0.983 | NS | 0.06 | 1.77 | 0.639 | NS | 0.673 | NS |
| SNB (°) | 3.92 | 1.28 | <0.001 | S | 0.85 | 1.52 | <0.001 | S | <0.001 | S |
| ANB (°) | −4.75 | 0.85 | <0.001 | S | −0.64 | 0.98 | 0.001 | S | <0.001 | S |
| Pt A-Na perp (mm) | 0.22 | 1.29 | 0.371 | NS | −0.34 | 2.07 | 0.231 | NS | 0.117 | NS |
| Pg-Na perp (mm) | −5.17 | 1.74 | <0.001 | S | −1.64 | 2.42 | <0.001 | S | <0.001 | S |
| Co-Pg (mm) | 8.18 | 3.23 | <0.001 | S | 2.36 | 2.17 | <0.001 | S | <0.001 | S |
| FMA (°) | 3.94 | 2.04 | <0.001 | S | −0.22 | 1.38 | 0.031 | S | <0.001 | S |
| LAFH (mm) | 3.15 | 1.31 | <0.001 | S | 0.5 | 1.13 | 0.029 | S | <0.001 | S |
| OB (mm) | −3.35 | 1.59 | <0.001 | S | 0.16 | 1.45 | 0.031 | S | <0.001 | S |
| OJ (mm) | −4 | 2.11 | <0.001 | S | −0.64 | 2.43 | <0.001 | S | <0.001 | S |
| U1 to SN (°) | −2.06 | 1.82 | <0.001 | S | −0.56 | 2.81 | 0.048 | NS | <0.001 | S |
| L1 to GoMe (°) | −2.59 | 2.26 | <0.001 | S | 0.36 | 1.34 | 0.522 | S | <0.001 | S |
| Interincisal Angle (°) | 4.17 | 3.91 | <0.001 | S | −0.53 | 3.37 | 0.002 | S | <0.001 | S |
| Measurements | Treated Group | Control Group | Treated vs. Control | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Mean Differences | p Value | Mean Differences | SD | p Value | p Value | |||||
| SNA (°) | 0.5 | 1.79 | 0.877 | NS | 0.21 | 1.56 | 0.251 | NS | 0.531 | NS |
| SNB (°) | 1.2 | 1.02 | 0.407 | NS | 0.92 | 1.63 | 0.047 | NS | 0.001 | S |
| ANB (°) | −0.9 | 0.52 | 0.818 | NS | −0.5 | 0.87 | 0.039 | NS | <0.001 | S |
| Pt A-Na perp (mm) | 0.33 | 1.64 | 0.652 | NS | 0.5 | 1.86 | 0.357 | NS | 0.322 | NS |
| Pg-Na perp (mm) | 0.74 | 1.48 | 0.431 | NS | 0.93 | 2.8 | 0.045 | NS | 0.031 | S |
| Co-Pg (mm) | 0.88 | 3.39 | 0.24 | NS | 0.71 | 2.1 | 0.037 | NS | <0.001 | S |
| FMA (°) | 0.14 | 1.86 | 0.442 | NS | 0.35 | 1.38 | 0.033 | NS | 0.023 | S |
| LAFH (mm) | 0.12 | 2.45 | 0.145 | NS | 0.82 | 1.16 | 0.349 | NS | <0.001 | S |
| OB (mm) | 0.14 | 1.38 | 0.451 | NS | 0.13 | 1.42 | 0.041 | NS | <0.001 | S |
| OJ (mm) | 1.00 | 1.54 | 0.121 | NS | 0.87 | 0.5 | 0.032 | NS | <0.001 | S |
| U1 to SN (°) | 0.61 | 2.52 | 0.371 | NS | 0.12 | 2.62 | 0.049 | NS | 0.033 | S |
| L1 to GoMe (°) | 0.53 | 2.56 | 0.432 | NS | 0.33 | 1.45 | 0.22 | NS | 0.021 | S |
| Interincisal Angle (°) | 0.13 | 3.37 | 0.139 | NS | 0.45 | 3.28 | 0.225 | NS | 0.014 | S |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Austro-Martinez, M.D.; Nicolas-Silvente, A.I.; Velasco-Ortega, E.; Jimenez-Guerra, A.; Alarcon, J.A. Stability of Class II Malocclusion Treatment with the Austro Repositioner Followed by Fixed Appliances in Brachyfacial Patients. Int. J. Environ. Res. Public Health 2021, 18, 9793. https://doi.org/10.3390/ijerph18189793
Austro-Martinez MD, Nicolas-Silvente AI, Velasco-Ortega E, Jimenez-Guerra A, Alarcon JA. Stability of Class II Malocclusion Treatment with the Austro Repositioner Followed by Fixed Appliances in Brachyfacial Patients. International Journal of Environmental Research and Public Health. 2021; 18(18):9793. https://doi.org/10.3390/ijerph18189793
Chicago/Turabian StyleAustro-Martinez, Maria Dolores, Ana I. Nicolas-Silvente, Eugenio Velasco-Ortega, Alvaro Jimenez-Guerra, and Jose A. Alarcon. 2021. "Stability of Class II Malocclusion Treatment with the Austro Repositioner Followed by Fixed Appliances in Brachyfacial Patients" International Journal of Environmental Research and Public Health 18, no. 18: 9793. https://doi.org/10.3390/ijerph18189793