
Urban Nature and Public Health: How Nature Exposure and Sociocultural Background Relate to Depression Risk


Abstract
:1. Introduction
2. Materials and Methods
2.1. Field Survey
2.2. Questionaire
2.3. Data Preparation
2.4. Statistical Analyses
3. Results
3.1. Sample Description
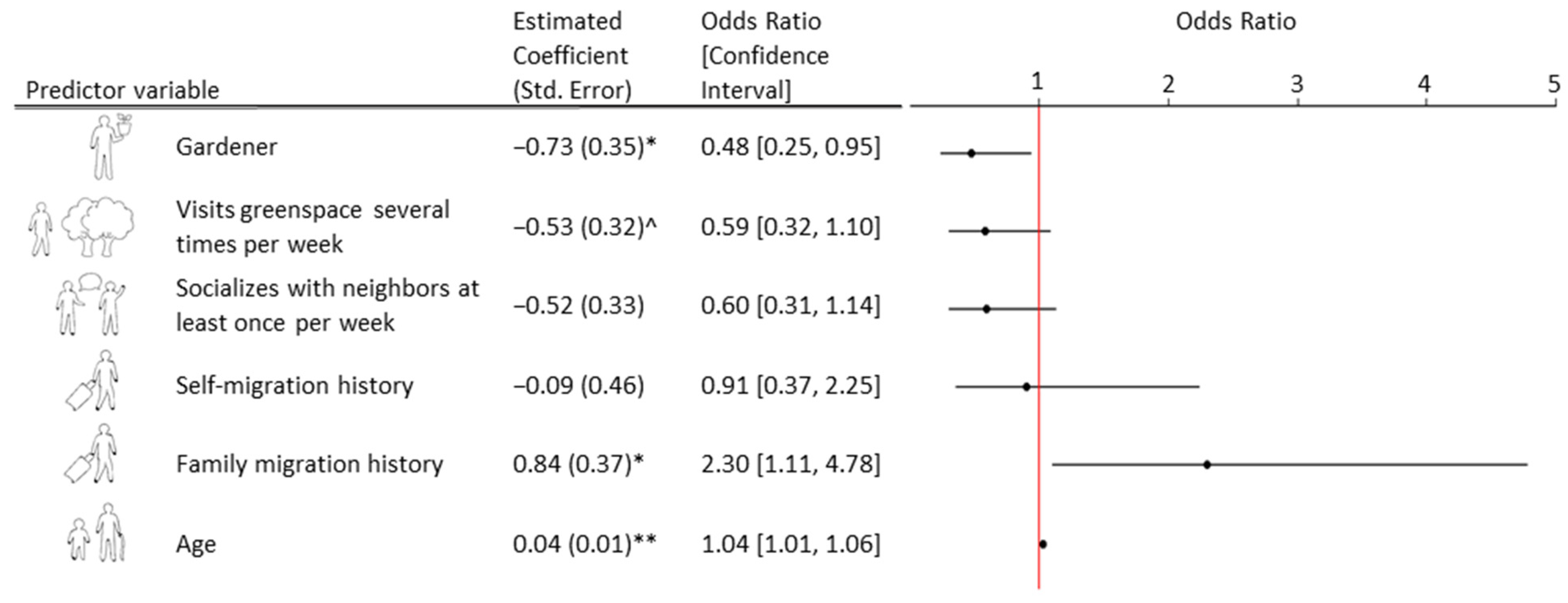
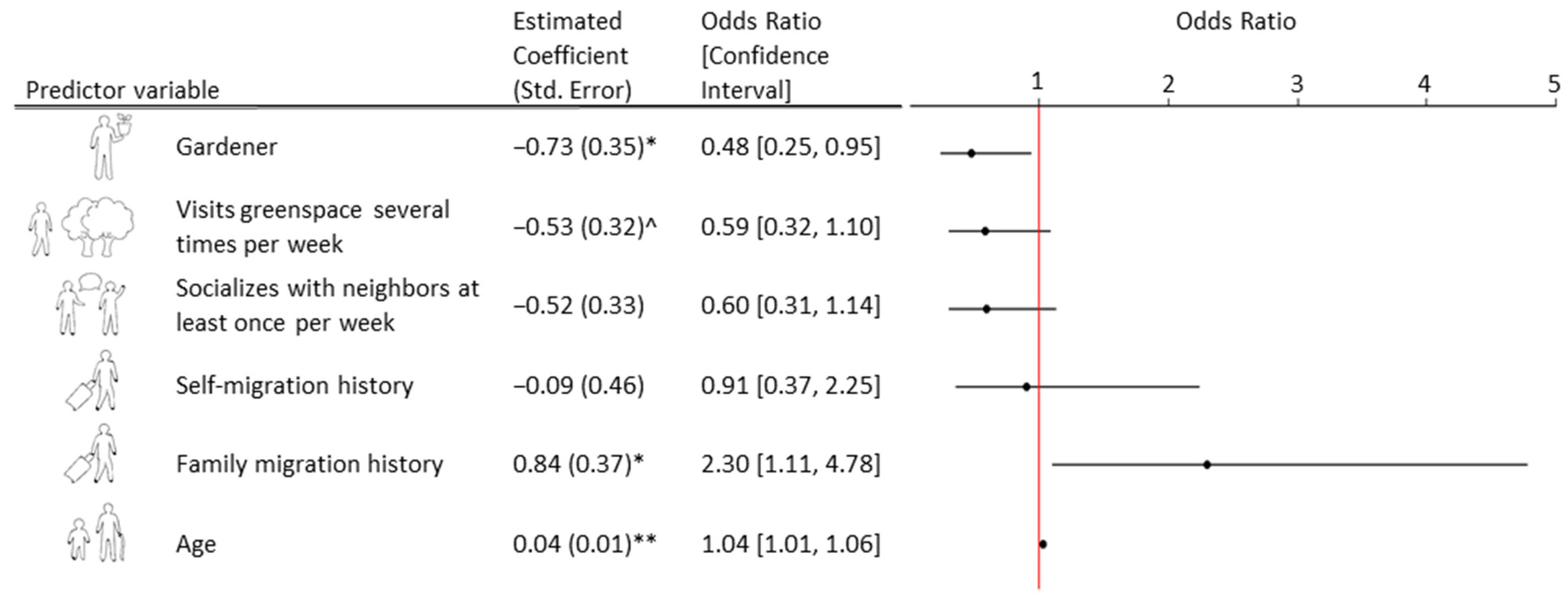
3.2. Urban Nature Exposure and Depression Risk
3.3. Neighborhood Social Interaction and Depression Risk
3.4. Migration History
3.4.1. Depression Risk
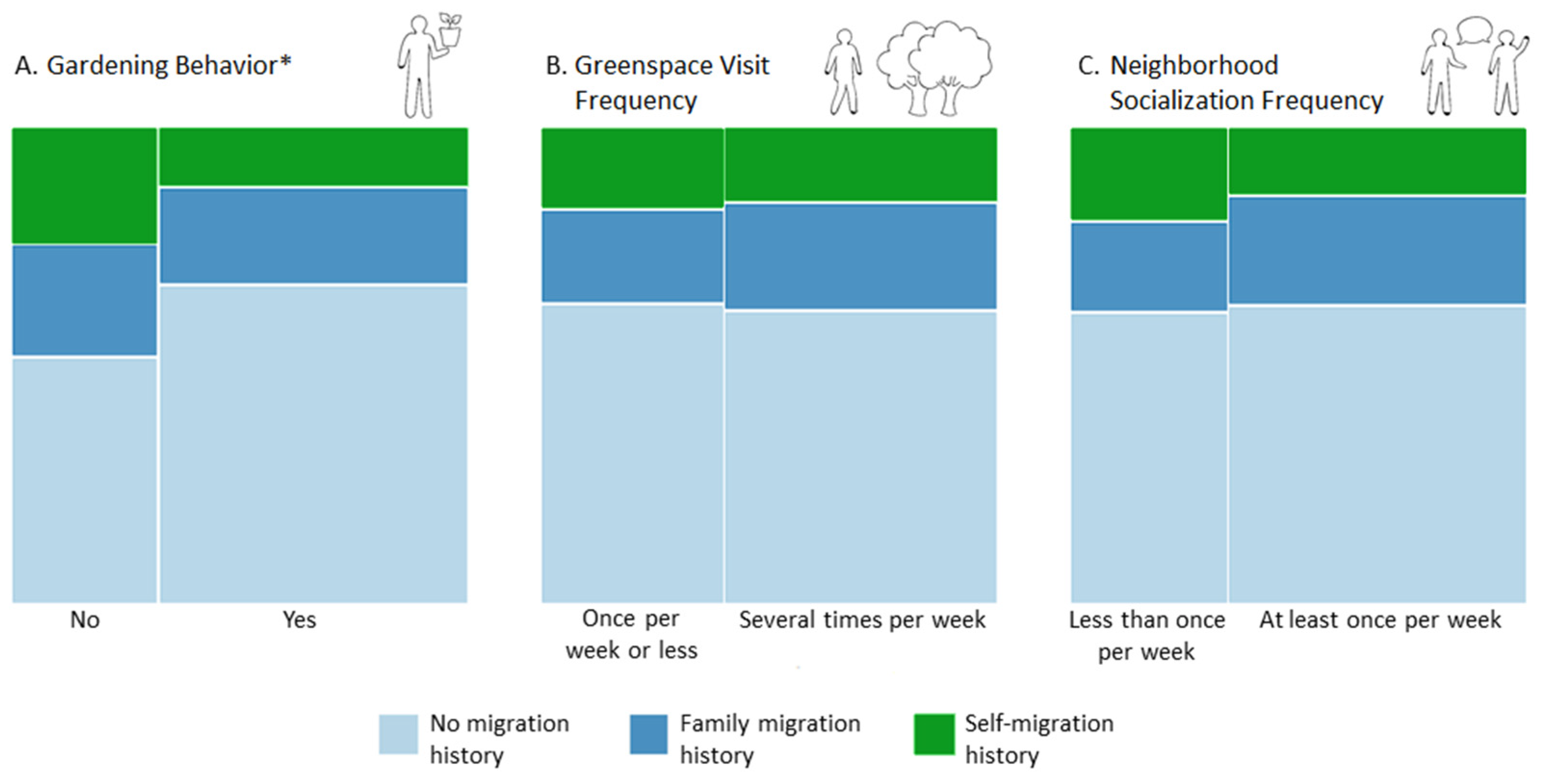
3.4.2. Urban Nature Exposure and Neighborhood Social Interaction
4. Discussion
4.1. Urban Nature Exposure and Depression Risk
4.2. Neighborhood Social Interaction and Depression Risk
4.3. Depression Risk, Urban Nature Exposure and Neighborhood Social Interaction according to Migration History
4.4. Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
| Variable | Original Survey Question | Original Survey Responses | Level Name for Analyses | N for Original Levels | Merged Levels for Analyses | New Level Name of Merged Categories for Analyses | N for Each New Level |
|---|---|---|---|---|---|---|---|
| Depression risk | WHO-5: Over the last two weeks: 1. I have felt cheerful and in good spirits 2. I have felt calm and relaxed 3. I have felt active and vigorous 4. I woke up feeling fresh and rested 5. My daily life has been filled with things that interest me | Responses per WHO-5 question: All the time (5) Most of the time (4) More than half of the time (3) Less than half of the time (2) Some of the time (1) At no time (0) | Originally continuous so no level name (raw score out of 25, multiplied by 4 to yield score out of 100.) | 282 | Cut-off score of WHO-5 ≤ 50 considered ‘At risk of depression.’ | At risk of depression Not at risk of depression | 55 227 |
| Gardening behavior | Do you garden (on balcony, windowsill, etc.)? | Yes No | Yes No | 192 90 | Yes No | Gardener Non-gardener | 192 90 |
| Greenspace visit frequency | In the last two weeks, how often did you visit green spaces in your city? | Several times a week Once a week Less than once a week Never I do not know | Several Once Less Never DK | 169 85 19 9 NA | Several Once + Less + Never | Visits greenspace several times per week Visits greenspace once per week or less | 169 113 |
| Neighborhood socialization frequency | In the last two weeks, how often did you socialize with your neighbors? | Several times a week Once a week Less than once a week Never I do not know | Several Once Less Never DK | 99 86 59 38 NA | Several + Once Less + Never | Socializes with neighbors at least once per week Socializes with neighbors less than once per week | 185 97 |
| Migration history | Were you, your parents or your grandparents born in a country other than Germany? | No, we were all born in Germany. Yes, I was born in another country, specifically in: Yes, at least one of my parents was born in another country, specifically in: Yes, at least one of my grandparents was born in another country, specifically in: I do not know. | German Self Parent_foreign Grandparent_foreign DK | 177 45 43 17 NA | German Self Parent_foreign + Grandparent_foreign | German Self-migration history Family migration history | 177 45 60 |
| Gender | Gender: | Male Female Other | Male Female Other | 125 157 0 | Male Female | Male Female | 125 157 |
| Age | Age: | Write-in | Continuous; no levels | 282 | Age | Age | 282 |
| Educational background | What is the highest level of schooling you have completed? | No formal schooling Primary school completed Secondary school completed Vocational education completed University education completed Other, specifically: | None Primary Secondary Vocational University Other | 1 2 54 52 176 4 | None + Primary + other Secondary Vocational University | Dropped Secondary Vocational University | Dropped 54 52 176 |
| Migration History Subset | Fisher’s Exact p-value |
|---|---|
| No migration history (n = 117) | 0.07 |
| Self-migration history (n = 45) | 0.46 |
| Family migration history (n = 60) | 0.56 |
References
- Banay, R.F.; James, P.; Hart, J.E.; Kubzansky, L.D.; Spiegelman, D.; Okereke, O.I.; Spengler, J.D.; Laden, F. Greenness and Depression Incidence among Older Women. Environ. Health Perspect. 2019, 127, 027001. [Google Scholar] [CrossRef]
- Helbich, M.; Klein, N.; Roberts, H.; Hagedoorn, P.; Groenewegen, P.P. More Green Space Is Related to Less Antidepressant Prescription Rates in the Netherlands: A Bayesian Geoadditive Quantile Regression Approach. Environ. Res. 2018, 166, 290–297. [Google Scholar] [CrossRef] [Green Version]
- Hedblom, M.; Gunnarsson, B.; Iravani, B.; Knez, I.; Schaefer, M.; Thorsson, P.; Lundström, J.N. Reduction of Physiological Stress by Urban Green Space in a Multisensory Virtual Experiment. Sci. Rep. 2019, 9, 10113. [Google Scholar] [CrossRef] [Green Version]
- Herrera, R.; Markevych, I.; Berger, U.; Genuneit, J.; Gerlich, J.; Nowak, D.; Schlotz, W.; Vogelberg, C.; von Mutius, E.; Weinmayr, G.; et al. Greenness and Job-Related Chronic Stress in Young Adults: A Prospective Cohort Study in Germany. BMJ Open 2018, 8, e021599. [Google Scholar] [CrossRef]
- Thompson, C.W.; Roe, J.; Aspinall, P.; Mitchell, R.; Clow, A.; Miller, D. More Green Space Is Linked to Less Stress in Deprived Communities: Evidence from Salivary Cortisol Patterns. Landsc. Urban Plan. 2012, 105, 221–229. [Google Scholar] [CrossRef] [Green Version]
- Villeneuve, P.J.; Jerrett, M.; Su, J.G.; Weichenthal, S.; Sandler, D.P. Association of Residential Greenness with Obesity and Physical Activity in a US Cohort of Women. Environ. Res. 2018, 160, 372–384. [Google Scholar] [CrossRef] [PubMed]
- Huang, W.-Z.; Yang, B.-Y.; Yu, H.-Y.; Bloom, M.S.; Markevych, I.; Heinrich, J.; Knibbs, L.D.; Leskinen, A.; Dharmage, S.C.; Jalaludin, B.; et al. Association between Community Greenness and Obesity in Urban-Dwelling Chinese Adults. Sci. Total Environ. 2020, 702, 135040. [Google Scholar] [CrossRef] [PubMed]
- James, P.; Hart, J.E.; Banay, R.F.; Laden, F. Exposure to Greenness and Mortality in a Nationwide Prospective Cohort Study of Women. Environ. Health Perspect. 2016, 124, 1344–1352. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Crouse, D.L.; Pinault, L.; Balram, A.; Hystad, P.; Peters, P.A.; Chen, H.; van Donkelaar, A.; Martin, R.V.; Ménard, R.; Robichaud, A.; et al. Urban Greenness and Mortality in Canada’s Largest Cities: A National Cohort Study. Lancet Planet. Health 2017, 1, e289–e297. [Google Scholar] [CrossRef]
- United Nations, Department of Economic and Social Affairs, Population Division. World Urbanization Prospects 2018: Highlights; United Nations: New York, NY, USA, 2019; ISBN 978-92-1-148318-5. [Google Scholar]
- Cox, D.T.C.; Shanahan, D.F.; Hudson, H.L.; Fuller, R.A.; Gaston, K.J. The Impact of Urbanisation on Nature Dose and the Implications for Human Health. Landsc. Urban Plan. 2018, 179, 72–80. [Google Scholar] [CrossRef]
- Soga, M.; Gaston, K.J. Extinction of Experience: The Loss of Human–Nature Interactions. Front. Ecol. Environ. 2016, 14, 94–101. [Google Scholar] [CrossRef] [Green Version]
- Okkels, N.; Kristiansen, C.B.; Munk-Jørgensen, P.; Sartorius, N. Urban Mental Health: Challenges and Perspectives. Curr. Opin. Psychiatry 2018, 31, 258–264. [Google Scholar] [CrossRef] [PubMed]
- Hoare, E.; Jacka, F.; Berk, M. The Impact of Urbanization on Mood Disorders: An Update of Recent Evidence. Curr. Opin. Psychiatry 2019, 32, 198–203. [Google Scholar] [CrossRef]
- Fact Sheet—Mental Health. 2019. Available online: https://web.archive.org/web/20210721100601/https://www.euro.who.int/__data/assets/pdf_file/0004/404851/MNH_FactSheet_ENG.pdf (accessed on 19 July 2021).
- Cohen, A. Addressing Comorbidity between Mental Disorders and Major Noncommunicable Diseases: Background Technical Report to Support. Implementation of the WHO European Action Plan. for the Prevention and Control. of Noncommunicable Diseases 2016–2025; World Health Organization Regional Office for Europe: Copenhagen, Denmark, 2017; pp. 1–46. [Google Scholar]
- Cox, D.T.C.; Shanahan, D.F.; Hudson, H.L.; Fuller, R.A.; Anderson, K.; Hancock, S.; Gaston, K.J. Doses of Nearby Nature Simultaneously Associated with Multiple Health Benefits. Int. J. Env. Res. Public Health 2017, 14, 172. [Google Scholar] [CrossRef] [Green Version]
- Shanahan, D.F.; Bush, R.; Gaston, K.J.; Lin, B.B.; Dean, J.; Barber, E.; Fuller, R.A. Health Benefits from Nature Experiences Depend on Dose. Sci. Rep. 2016, 6, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Lee, H.J.; Lee, D.K. Do Sociodemographic Factors and Urban Green Space Affect Mental Health Outcomes among the Urban Elderly Population? Int. J. Environ. Res. Public Health 2019, 16, 789. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Beute, F.; Andreucci, M.B.; Davies, Z.; Glanville, J.; Keune, H.; Marselle, M.; O’Brien, L.A.; Olszewska-Guizzo, A.; Remmen, R.; Russo, A.; et al. Type and Characteristics of Urban. and Peri-Urban. Green Spaces Having an Impact on Human Mental Health and Wellbeing: A Systematic Review; UK Centre for Ecology & Hydrology: Wallingford, UK, 2020; pp. 7–10. ISBN 978-1-906698-75-1. [Google Scholar]
- Bratman, G.N.; Anderson, C.B.; Berman, M.G.; Cochran, B.; de Vries, S.; Flanders, J.; Folke, C.; Frumkin, H.; Gross, J.J.; Hartig, T.; et al. Nature and Mental Health: An Ecosystem Service Perspective. Sci. Adv. 2019, 5. [Google Scholar] [CrossRef] [Green Version]
- Markevych, I.; Schoierer, J.; Hartig, T.; Chudnovsky, A.; Hystad, P.; Dzhambov, A.M.; de Vries, S.; Triguero-Mas, M.; Brauer, M.; Nieuwenhuijsen, M.J.; et al. Exploring Pathways Linking Greenspace to Health: Theoretical and Methodological Guidance. Environ. Res. 2017, 158, 301–317. [Google Scholar] [CrossRef] [PubMed]
- Holt-Lunstad, J.; Smith, T.B.; Layton, J.B. Social Relationships and Mortality Risk: A Meta-Analytic Review. PLoS Med. 2010, 7, e1000316. [Google Scholar] [CrossRef] [PubMed]
- Santini, Z.I.; Koyanagi, A.; Tyrovolas, S.; Mason, C.; Haro, J.M. The Association between Social Relationships and Depression: A Systematic Review. J. Affect. Disord. 2015, 175, 53–65. [Google Scholar] [CrossRef] [PubMed]
- Santini, Z.I.; Jose, P.E.; Cornwell, E.Y.; Koyanagi, A.; Nielsen, L.; Hinrichsen, C.; Meilstrup, C.; Madsen, K.R.; Koushede, V. Social Disconnectedness, Perceived Isolation, and Symptoms of Depression and Anxiety among Older Americans (NSHAP): A Longitudinal Mediation Analysis. Lancet Public Health 2020, 5, e62–e70. [Google Scholar] [CrossRef] [Green Version]
- Werner-Seidler, A.; Afzali, M.H.; Chapman, C.; Sunderland, M.; Slade, T. The Relationship between Social Support Networks and Depression in the 2007 National Survey of Mental Health and Well-Being. Soc. Psychiatry Psychiatr. Epidemiol. 2017, 52, 1463–1473. [Google Scholar] [CrossRef] [PubMed]
- Lane, A.P.; Hou, Y.; Hooi Wong, C.; Yuen, B. Cross-Sectional Associations of Neighborhood Third Places with Social Health among Community-Dwelling Older Adults. Soc. Sci. Med. 2020, 258, 113057. [Google Scholar] [CrossRef] [PubMed]
- Miao, J.; Wu, X.; Sun, X. Neighborhood, Social Cohesion, and the Elderly’s Depression in Shanghai. Soc. Sci. Med. 2019, 229, 134–143. [Google Scholar] [CrossRef] [PubMed]
- Dawson, C.T.; Wu, W.; Fennie, K.P.; Ibañez, G.; Cano, M.Á.; Pettit, J.W.; Trepka, M.J. Perceived Neighborhood Social Cohesion Moderates the Relationship between Neighborhood Structural Disadvantage and Adolescent Depressive Symptoms. Health Place 2019, 56, 88–98. [Google Scholar] [CrossRef]
- Gascon, M.; Sánchez-Benavides, G.; Dadvand, P.; Martínez, D.; Gramunt, N.; Gotsens, X.; Cirach, M.; Vert, C.; Molinuevo, J.L.; Crous-Bou, M.; et al. Long-Term Exposure to Residential Green and Blue Spaces and Anxiety and Depression in Adults: A Cross-Sectional Study. Environ. Res. 2018, 162, 231–239. [Google Scholar] [CrossRef]
- Liu, Y.; Wang, R.; Xiao, Y.; Huang, B.; Chen, H.; Li, Z. Exploring the Linkage between Greenness Exposure and Depression among Chinese People: Mediating Roles of Physical Activity, Stress and Social Cohesion and Moderating Role of Urbanicity. Health Place 2019, 58, 102168. [Google Scholar] [CrossRef]
- Hystad, P.; Payette, Y.; Noisel, N.; Boileau, C. Green Space Associations with Mental Health and Cognitive Function. Environ. Epidemiol. 2019, 3, e040. [Google Scholar] [CrossRef]
- Browning, M.H.E.M.; Lee, K.; Wolf, K.L. Tree Cover Shows an Inverse Relationship with Depressive Symptoms in Elderly Residents Living in U.S. Nursing Homes. Urban For. Urban Green. 2019, 41, 23–32. [Google Scholar] [CrossRef]
- Wood, C.J.; Pretty, J.; Griffin, M. A Case–Control Study of the Health and Well-Being Benefits of Allotment Gardening. J. Public Health 2016, 38, e336–e344. [Google Scholar] [CrossRef]
- Vujcic, M.; Tomicevic-Dubljevic, J.; Grbic, M.; Lecic-Tosevski, D.; Vukovic, O.; Toskovic, O. Nature Based Solution for Improving Mental Health and Well-Being in Urban Areas. Environ. Res. 2017, 158, 385–392. [Google Scholar] [CrossRef]
- Soga, M.; Cox, D.; Yamaura, Y.; Gaston, K.; Kurisu, K.; Hanaki, K. Health Benefits of Urban Allotment Gardening: Improved Physical and Psychological Well-Being and Social Integration. Int. J. Environ. Res. Public Health 2017, 14, 71. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.-H.; Park, S.-A. Horticultural Therapy Program for Middle-Aged Women’s Depression, Anxiety, and Self-Identify. Complement. Ther. Med. 2018, 39, 154–159. [Google Scholar] [CrossRef]
- Ghanbari, S.; Jafari, F.; Bagheri, N.; Neamtolahi, S.; Shayanpour, R. Study of the Effect of Using Purposeful Activity (Gardening) on Depression of Female Resident in Golestan Dormitory of Ahvaz Jundishapur University of Medical Sciences. J. Rehabil. Sci. 2015, 2, 8–11. [Google Scholar] [CrossRef]
- Gonzalez, M.T.; Hartig, T.; Patil, G.G.; Martinsen, E.W.; Kirkevold, M. Therapeutic Horticulture in Clinical Depression: A Prospective Study of Active Components: Therapeutic Horticulture in Clinical Depression. J. Adv. Nurs. 2010, 66, 2002–2013. [Google Scholar] [CrossRef]
- Wilson, J.F.; Christensen, K.M. The Relationship between Gardening and Depression among Individuals with Disabilities. J. Ther. Hortic. 2011, 21, 28–41. [Google Scholar]
- Triguero-Mas, M.; Anguelovski, I.; Cirac-Claveras, J.; Connolly, J.; Vazquez, A.; Urgell-Plaza, F.; Cardona-Giralt, N.; Sanyé-Mengual, E.; Alonso, J.; Cole, H. Quality of Life Benefits of Urban Rooftop Gardening for People With Intellectual Disabilities or Mental Health Disorders. Prev. Chronic. Dis. 2020, 17, 200087. [Google Scholar] [CrossRef]
- Gerber, M.M.; Callahan, J.L.; Moyer, D.N.; Connally, M.L.; Holtz, P.M.; Janis, B.M. Nepali Bhutanese Refugees Reap Support Through Community Gardening. Int. Perspect. Psychol. 2017, 6, 17–31. [Google Scholar] [CrossRef]
- Masuya, J.; Ota, K.; Mashida, Y. The Effect of a Horticultural Activities Program on the Psychologic, Physical, Cognitive Function and Quality of Life of Elderly People Living in Nursing Homes. Int. J. Nurs. Clin. Pract. 2014, 1, 2394–4978. [Google Scholar] [CrossRef]
- Park, S.-A.; Lee, A.-Y.; Son, K.-C.; Lee, W.-L.; Kim, D.-S. Gardening Intervention for Physical and Psychological Health Benefits in Elderly Women at Community Centers. HortTechnology 2016, 26, 474–483. [Google Scholar] [CrossRef] [Green Version]
- Relf, D.; Dorn, S. Horticulture: Meeting the Needs of Special Populations. HortTechnology 1995, 5, 94–103. [Google Scholar] [CrossRef] [Green Version]
- Kabisch, N. The influence of socio-economic and socio-demographic factors in the association between urban green space and health. In Biodiversity and Health in the Face of Climate Change; Springer: Cham, Switzerland, 2019; pp. 91–119. [Google Scholar]
- Roberts, R.E.; Kaplan, G.A.; Shema, S.J.; Strawbridge, W.J. Prevalence and Correlates of Depression in an Aging Cohort: The Alameda County Study. J. Gerontol. B Psychol. Sci. Soc. Sci. 1997, 52B, S252–S258. [Google Scholar] [CrossRef] [Green Version]
- Morawa, E.; Erim, Y. Acculturation and Depressive Symptoms among Turkish Immigrants in Germany. Int. J. Environ. Res. Public Health 2014, 11, 9503–9521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davison, K.M.; Lung, Y.; Lin, S. (Lamson); Tong, H.; Kobayashi, K.M.; Fuller-Thomson, E. Depression in Middle and Older Adulthood: The Role of Immigration, Nutrition, and Other Determinants of Health in the Canadian Longitudinal Study on Aging. BMC Psychiatry 2019, 19, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Sieberer, M.; Maksimović, S.; Ersöz, B.; Machleidt, W.; Ziegenbein, M.; Calliess, I.T. Depressive Symptoms in First-and Second-Generation Migrants: A Cross-Sectional Study of a Multi-Ethnic Working Population. Int. J. Soc. Psychiatry 2012, 58, 605–613. [Google Scholar] [CrossRef]
- Ruiz-Castell, M.; Kandala, N.-B.; Perquin, M.; Bocquet, V.; Kuemmerle, A.; Vögele, C.; Stranges, S. Depression Burden in Luxembourg: Individual Risk Factors, Geographic Variations and the Role of Migration, 2013–2015 European Health Examination Survey. J. Affect. Disord. 2017, 222, 41–48. [Google Scholar] [CrossRef]
- Gentin, S.; Pitkänen, K.; Chondromatidou, A.M.; Præstholm, S.; Dolling, A.; Palsdottir, A.M. Nature-Based Integration of Immigrants in Europe: A Review. Urban Urban Green 2019, 43, 126379. [Google Scholar] [CrossRef]
- Hartwig, K.A.; Mason, M. Community Gardens for Refugee and Immigrant Communities as a Means of Health Promotion. J. Community Health 2016, 41, 1153–1159. [Google Scholar] [CrossRef] [PubMed]
- Stuttgart in Zahlen. Available online: https://web.archive.org/web/20210804132928/https://www.stuttgart.de/service/statistik-und-wahlen/stuttgart-in-zahlen.php (accessed on 13 July 2021).
- Méndez, M.; Ferreras, M.; Cuesta, M. Immigration and general population surveys in Spain: The CIS surveys. In Surveying Ethnic Minorities and Immigrant Populations: Methodological Challenges and Research Strategies; Amsterdam University Press: Amsterdam, The Netherlands, 2013; pp. 195–214. ISBN 978-90-8964-543-2. [Google Scholar]
- Fischer, L.K.; Honold, J.; Cvejić, R.; Delshammar, T.; Hilbert, S.; Lafortezza, R.; Nastran, M.; Nielsen, A.B.; Pintar, M.; van der Jagt, A.P.N.; et al. Beyond Green: Broad Support for Biodiversity in Multicultural European Cities. Glob. Environ. Chang. 2018, 49, 35–45. [Google Scholar] [CrossRef]
- Gopal, D.; Fischer, L. Streetscapes as Surrogate Greenspaces During COVID-19? Front. Sustain. Cities 2021, 3, 710920. [Google Scholar] [CrossRef]
- WHO. Available online: https://web.archive.org/web/20210628142711/https://www.psykiatri-regionh.dk/who-5/Documents/WHO-5%20questionaire%20-%20English.pdf (accessed on 19 July 2021).
- Topp, C.W.; Østergaard, S.D.; Søndergaard, S.; Bech, P. The WHO-5 Well-Being Index: A Systematic Review of the Literature. Psychother. Psychosom. 2015, 84, 167–176. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statsitcal Computing. Available online: https://www.R-project.org/ (accessed on 15 January 2021).
- Europäische Erhebung zur Lebensqualität—Datenvisualisierung. Available online: https://web.archive.org/web/20210804133125/https://www.eurofound.europa.eu/de/data/european-quality-of-life-survey (accessed on 19 July 2021).
- McFarland, A.; Waliczek, T.M.; Etheredge, C.; Sommerfeld Lillard, A.J. Understanding Motivations for Gardening Using a Qualitative General Inductive Approach. HortTechnology 2018, 28, 289–295. [Google Scholar] [CrossRef]
- Hawkins, J.L.; Thirlaway, K.J.; Backx, K.; Clayton, D.A. Allotment Gardening and Other Leisure Activities for Stress Reduction and Healthy Aging. HortTechnology 2011, 21, 577–585. [Google Scholar] [CrossRef] [Green Version]
- Philpott, S.M.; Egerer, M.H.; Bichier, P.; Cohen, H.; Cohen, R.; Liere, H.; Jha, S.; Lin, B.B. Gardener Demographics, Experience, and Motivations Drive Differences in Plant Species Richness and Composition in Urban Gardens. Ecol. Soc. 2020, 25, 8. [Google Scholar] [CrossRef]
- Symptoms—Clinical Depression. Available online: https://web.archive.org/web/20210904033453/https://www.nhs.uk/mental-health/conditions/clinical-depression/symptoms/ (accessed on 6 September 2021).
- Koay, W.I.; Dillon, D. Community Gardening: Stress, Well-Being, and Resilience Potentials. Int. J. Environ. Res. Public. Health 2020, 17, 6740. [Google Scholar] [CrossRef]
- Chalmin-Pui, L.S.; Griffiths, A.; Roe, J.; Heaton, T.; Cameron, R. Why Garden?—Attitudes and the Perceived Health Benefits of Home Gardening. Cities 2021, 112, 103118. [Google Scholar] [CrossRef]
- The Warwick-Edinburgh Mental Wellbeing Scale (WEMWBS). Available online: https://web.archive.org/web/20210804133325/https://warwick.ac.uk/fac/sci/med/research/platform/wemwbs/ (accessed on 16 July 2021).
- Lundin, A.; Hallgren, M.; Theobald, H.; Hellgren, C.; Torgén, M. Validity of the 12-Item Version of the General Health Questionnaire in Detecting Depression in the General Population. Public Health 2016, 136, 66–74. [Google Scholar] [CrossRef]
- Ko, J.Y.; Farr, S.L.; Dietz, P.M.; Robbins, C.L. Depression and Treatment Among U.S. Pregnant and Nonpregnant Women of Reproductive Age, 2005–2009. J. Womens Health 2015, 21, 830–836. [Google Scholar] [CrossRef] [Green Version]
- Farr, S.L.; Bitsko, R.H.; Hayes, D.K.; Dietz, P.M. Mental Health and Access to Services among US Women of Reproductive Age. Am. J. Obstet. Gynecol. 2010, 203, 542.e1. [Google Scholar] [CrossRef]
- Song, H.; Lane, K.J.; Kim, H.; Kim, H.; Byun, G.; Le, M.; Choi, Y.; Park, C.R.; Lee, J.-T. Association between Urban Greenness and Depressive Symptoms: Evaluation of Greenness Using Various Indicators. Int. J. Environ. Res. Public. Health 2019, 16, 173. [Google Scholar] [CrossRef] [Green Version]
- Mair, C.; Roux, A.V.D.; Golden, S.H.; Rapp, S.; Shea, S. Change in Neighborhood Environments and Depressive Symptoms in New York City: The Multi-Ethnic Study of Atherosclerosis. Health Place 2015, 32, 93–98. [Google Scholar] [CrossRef] [Green Version]
- Wang, R.; Xue, D.; Chen, H.; Qiu, Y. The Relationship between Urbanization and Depression in China: The Mediating Role of Neighborhood Social Capital. Int. J. Equity Health 2018, 17, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Nezlek, J.B.; Imbrie, M.; Shean, G.D. Depression and Everyday Social Interaction. J. Per. Soc. Psychol. 1994, 67, 1101–1113. [Google Scholar] [CrossRef]
- Williams, S.N.; Armitage, C.J.; Tampe, T.; Dienes, K. Public Perceptions and Experiences of Social Distancing and Social Isolation during the COVID-19 Pandemic: A UK—Based Focus Group Study. BMJ Open 2020, 10, e039334. [Google Scholar] [CrossRef]
- Infektionen und Todesfälle in Baden-Württemberg (Archiv). Available online: https://web.archive.org/web/20210804133745/https://www.baden-wuerttemberg.de/de/service/aktuelle-infos-zu-corona/archiv-infektionen-und-todesfaelle-in-baden-wuerttemberg/infektionen-und-todesfaelle-in-baden-wuerttemberg-3-quartal-2020/ (accessed on 19 July 2021).
- Alegría, M.; Álvarez, K.; DiMarzio, K. Immigration and Mental Health. Curr. Epidemiol. Rep. 2017, 4, 145–155. [Google Scholar] [CrossRef] [PubMed]
- Bellows, A.C.; Alcaraz, G.V.; Vivar, T. Gardening as a Tool to Foster Health and Cultural Identity in the Context of International Migration: Attitudes and Constraints in a Female Population. Acta Hortic. 2009, 881, 785–792. [Google Scholar] [CrossRef]
- Agustina, I.; Beilin, R. Community Gardens: Space for Interactions and Adaptations. Procedia Soc. Behav. Sci. 2012, 36, 439–448. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization (WHO). Regional Office for Europe Depression in Europe: Facts and Figures. Available online: https://web.archive.org/web/20210804133946/https://www.euro.who.int/en/health-topics/noncommunicable-diseases/mental-health/news/news/2012/10/depression-in-europe/depression-in-europe-facts-and-figures (accessed on 25 June 2021).

| Variable | Level | Percent Sample Population | |
|---|---|---|---|
| 1. Depression risk | At risk of depression (WHO-5 ≤ 50) | 19.5 (n = 55) | |
| Not at risk of depression (WHO-5 > 50) | 80.5 (n = 227) | ||
| 2. Gardening behavior |  | Gardener | 68.1(n = 192) |
| Non-gardener | 31.9 (n = 90) | ||
| 3. Greenspace visit frequency |  | Visits greenspace several times a week | 59.9 (n = 169) |
| Visits greenspace once a week or less | 40.1(n = 113) | ||
| 4. Neighborhood socialization frequency |  | Socializes with neighbors at least once a week | 65.6 (n = 185) |
| Socializes with neighbors less than once a week | 34.4 (n = 97) | ||
| 5. Migration history |  | No migration history (German) | 62.8 (n = 177) |
| Self-migration history | 16.0 (n = 45) | ||
| Family migration history | 21.3 (n = 60) | ||
| 6. Educational background |  | Secondary school completed | 19.1 (n = 54) |
| Vocational education completed | 18.4 (n = 52) | ||
| University education completed | 62.4 (n = 176) | ||
| 7. Gender |  | Female | 55.4 (n = 157) |
| Male | 44.3 (n = 125) | ||
| 8. Age |  | Age (years) | Range: 18–93 Mean: 36.2 (SD: 13.4) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jakstis, K.; Fischer, L.K. Urban Nature and Public Health: How Nature Exposure and Sociocultural Background Relate to Depression Risk. Int. J. Environ. Res. Public Health 2021, 18, 9689. https://doi.org/10.3390/ijerph18189689
Jakstis K, Fischer LK. Urban Nature and Public Health: How Nature Exposure and Sociocultural Background Relate to Depression Risk. International Journal of Environmental Research and Public Health. 2021; 18(18):9689. https://doi.org/10.3390/ijerph18189689
Chicago/Turabian StyleJakstis, Kristen, and Leonie K. Fischer. 2021. "Urban Nature and Public Health: How Nature Exposure and Sociocultural Background Relate to Depression Risk" International Journal of Environmental Research and Public Health 18, no. 18: 9689. https://doi.org/10.3390/ijerph18189689
APA StyleJakstis, K., & Fischer, L. K. (2021). Urban Nature and Public Health: How Nature Exposure and Sociocultural Background Relate to Depression Risk. International Journal of Environmental Research and Public Health, 18(18), 9689. https://doi.org/10.3390/ijerph18189689