
The COVID-19 Clinician Cohort (CoCCo) Study: Empirically Grounded Recommendations for Forward-Facing Psychological Care of Frontline Doctors

 , , , ,
, , , ,
Abstract
:1. Introduction
Study Aims
2. Materials and Methods
2.1. Measures
2.2. Participants
2.3. Procedure
2.4. Analysis
2.5. Development of Recommendations and Model of Psychological Care
2.6. Patient and Public Involvement
3. Results
3.1. Main Themes
“In some ways maybe having had this peak is a perfect opportunity to incorporate more into the workplace, because clearly it took until breaking point for us to even acknowledge that we have an endemic problem within the profession.”(#115, F, Intensive Care)
“There’s already a significant degree of burnout and exhaustion, and I think that one of the worst things about this pandemic was that it was on top of that; a lot of people were already working by running on empty almost and then this happened.”(I#121, M, Anaesthetist, ICU)
3.1.1. Coping Strategies

{kind=link}
| Quote Number | Illustrative Quote |
| A1: Exercise | A1: “I would rather go for a run or see my family, or bake, or do something creative rather than sit and breathe quietly with my eyes shut.” (#106, F, An, ICU) |
| A2: Drinking | A2: “To be perfectly honest with you more drinking, not to stupid quantities where I feel like I’ve needed to go and get help, but to quantities where I wouldn’t want… when I have children I wouldn’t want to be drinking as much as I am drinking now.” (#127, M, EM, ICU) |
| A3: Store it up. | A3: “There’s been a lot of stuff I’ve seen that hasn’t been very pleasant, and obviously in the moment you think about it and you’re upset about it, but I have somewhat just packaged that up and put it to the one side.” (#103, F, An, ICU) |
| A4: Wait until it’s bad. | A4: “I found it very easy to just think to myself I’ve just got to get on with this, this is it’s normal to be feeling really anxious and to not be sleeping. I know that burnout is a concept that exists but that can’t be happening to me.” (#122, M, An, ICU) |
| A5: Psychological help is for others | A5: “I am fine,.. I don’t need that service as much as other people, so I’m not going to use that resource. I don’t want to be the one who is taking up a resource unnecessarily and wasting somebody’s time.” (#109, F, EM) |
3.1.2. Sources of Support
- What helped
- What did not help
| Quote Number | Illustrative Quote |
|---|---|
| B1: Talking to colleagues | B1: “We’re a really good team, so just making sure that everybody is feeling okay, and actually talking about our experiences, … share those experiences that have been difficult, I think that really helps. […] being in a good team has to be the winning thing really.” (#114, F, ICM) |
| B2: Embedded support | B2: “you see the psychologists are just normal people, getting a tea in the tearoom. They are really accessible, and then when people start crying at work they just sidle up and say, “Are you okay?” And I think that’s really good.” (#103, F, An, ICU) |
| B3: Specialist support | B3: “I’ve had two sessions with her [psychologist] just over the phone and that’s been quite good. Working in acute specialties, you are at the pointy end of quite a lot of drama and quite a lot of situations which might stick with you and impact on your mental health and actually maybe you need a little bit of time to process, and it’s helpful to talk through.” (#107, F, An, ICU) |
| B4: Resources | B4: “Our Trust has an excellent wellbeing resource page, … plus everywhere you look now there’s guidance on resilience and wellbeing.” (#105, F, An, ICU) |
| B5: No time to attend… | B5: “Most of the time on my shift I can’t just drop out for things, if you manage to time your break for that time you can do it, if you don’t then you can’t, or you will just end up being tied up in a complex case that you can’t walk away from. In that sense they were quite inaccessible to me.” (#109, F, EM) |
| B6: ... or to talk. | B6: “Often at work if you talk for a few minutes it’s like, “Right get on now,” and there’s not really any time … and we’re policed constantly. It’s always like you’re on a time limit, you never really get to sit down and have that chat, and we can’t see each other outside of work.” (#110, F, EM) |
3.1.3. Organisational Influences on Wellbeing
| Quote Number | Illustrative Quote |
|---|---|
| C1: Positive influences | C1: “We had loads of things around the hospital like decompression rooms or quiet rooms where you just go and be quiet, and they would put colouring books and coffee machines there so you could sit and reflect on what had happened, which was really helpful.” (#102, F, An, ICU) |
| C2: The little things | C2: “I think a huge thing about morale in the NHS actually it is the small things, …the things that really get people down or really lift people’s spirits are not very big, it’s free tea and coffee. There are no rest facilities for doctors anymore, so if there’s a chair that pulls out and a blanket or a pillow, that really lifts people’s spirits. It’s really little stuff like that.” (#103, F, An, ICU) |
| C3: Negative influences | C3: “It felt at times very vulnerable and just a little bit maybe sacrificial you didn’t have any control over anything really, you were just given what you were given and had to work with it, and it would constantly change, and I think it felt like there was a lack of respect from people at managerial and senior levels as to what we were actually doing.” (#107, F, An, ICU) |
| C4: Resilience | C4: “If you say resilience to a doctor, … you’ve lost them already… someone wants to [talk to] me about resilience and they have not just done the week that I have just done, walk a week in my shoes and then talk to me about resilience.” (#105, F, An, ICU) |
| C5: Resilience | C5: “It’s just I think the word resilient should never be used, because it’s just become a swear word,… you’re upset about the fact that you can’t manage your childcare, and your shift, and your pay has been cut… what you need is some resilience training [laughs]. Just makes us all so angry.” (#104, F, An) |
| C6: COVID 1st wave | C6: “The first wave with the redeployment of staff we had lots of staff,…. we worked 24 h, we had packs of teams that worked together, so we did feel like we had enough staff.” (#111, F, EM) |
| C7: COVID 2nd wave | C7: “I felt like this time we had months to prepare, and actually when it arrived it was bigger than was anticipated, we were totally overwhelmed, and people were not redeployed up until the 11th hour.” (#115, F, ICM) |
3.1.4. Improving Engagement with Support
- Facilitators and treatment preferences
- Barriers to access
| Quote Number | Illustrative Quote |
|---|---|
| D1: Safe place | D1: “The concept of a safe space where you can take timeout that’s actually recognised as timeout is absolutely something that should exist.” (#130, F, An, ICU) |
| D2: With colleagues | D2: “I think it would be helpful to be with colleagues, I find that shared experience and the people around you, like the team that supported you through it, having them around for the aftercare is quite helpful.” (#113, F, ICM) |
| D3: Clinical debrief | D3:“There would probably be scope for something more proactive, so for example a structured debrief at the end of every shift.” (#122, M, An, ICU) |
| D4: Someone who understands | D4: “I think it is trust that you can just say how you feel, and also the fact that they would understand how you felt, because they understand it, because they have been through it, which really helps.” (#102, F, An, ICU) |
| D5: Embedded support | D5:“It’s just the visibility of it is important because it normalises it… it’s okay to not be okay, … there’s not necessarily anything wrong with you or anything that needs treating. It’s just you have seen something horrible and you want to have a cry about it. So I think the real presence and visibility of that kind of [psychologist] support is really useful.” (#103, F, An, ICU) |
| D6: Anonymity | D6: “I know some people have deliberately avoided going through work in case there’s any stigma attached to that when it comes to annual review or anything like that,” (#124, M, An, ICU) |
| D7: Safety of information | D7: “Have a blanket measure to help everybody, a safe place to talk, knowing that if I say something somebody is not going to come back to me and say “you said this, why did you say it?”” (#129, M, EM) |
| D8: Leadership | D8: “People who I admire clinically and professionally also trying to step up and actually look after our welfare themselves as individuals and taking on a little bit more of a welfare role, that’s been nice, when I am sure they themselves have actually been experiencing all the same things I am experiencing.” (#107, F, An, ICU) |
| D9: Normalise psychological reactions | D9: “Sometimes I want to be able to say something like I felt like this, and it’s awful I felt like this, but I did feel like that, why?” (#127, M, EM, ICU) |
| D10: Timing | D10: “How are we supposed to get protected time in the context of the NHS being under unprecedented pressure, to do things that are good for our wellbeing? (#112, F, EM) |
| D11: What’s available? | D11: “It feels a bit like the support is there, but you need to go looking for it, as opposed to being encouraged to actively engage with it, I think.” (#122, M, An, ICU) |
| D12: Stigma | D12: “I feel like there’s a fair amount of stigma about mental health, about mental wellbeing, and admitting if you’re struggling or finding things difficult, and I don’t know if I would have gone for fear of being stigmatised for it.” (#109, F, EM) |
| D13: Culture | D13: “It is just a toxic culture within medicine … which comes from the top down … It makes speaking up about having difficulties very difficult …within that acute specialties umbrella there’s almost a macho.… it’s a very masculine thing of heroism… but there’s something there about people think that they should be somehow superhuman and not [affected] in a normal way by some of the very abnormal things that we’re involved with.” (#117, F, EM, ICU) |
| D14: Consequences | D14:“I understand why they are not accessing the mental health support services. There’s so many reasons, one is the perception of failure if you have a mental health problem, second is you don’t want your employer to know if you’re struggling in any way because they are helping your progression to your endpoint of being a consultant, no one wants to admit failure as a doctor.” (#105, F, An, ICU) |
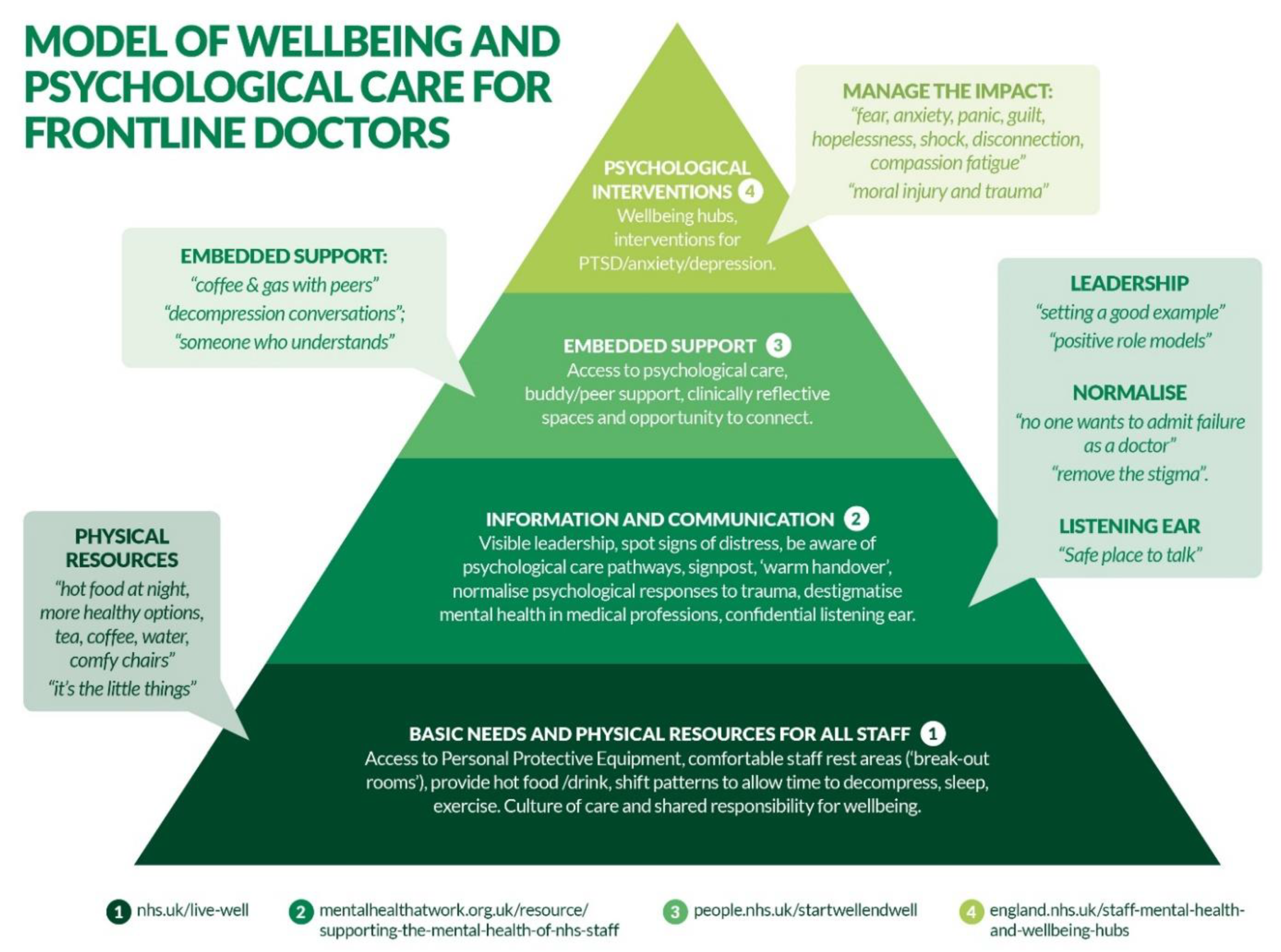
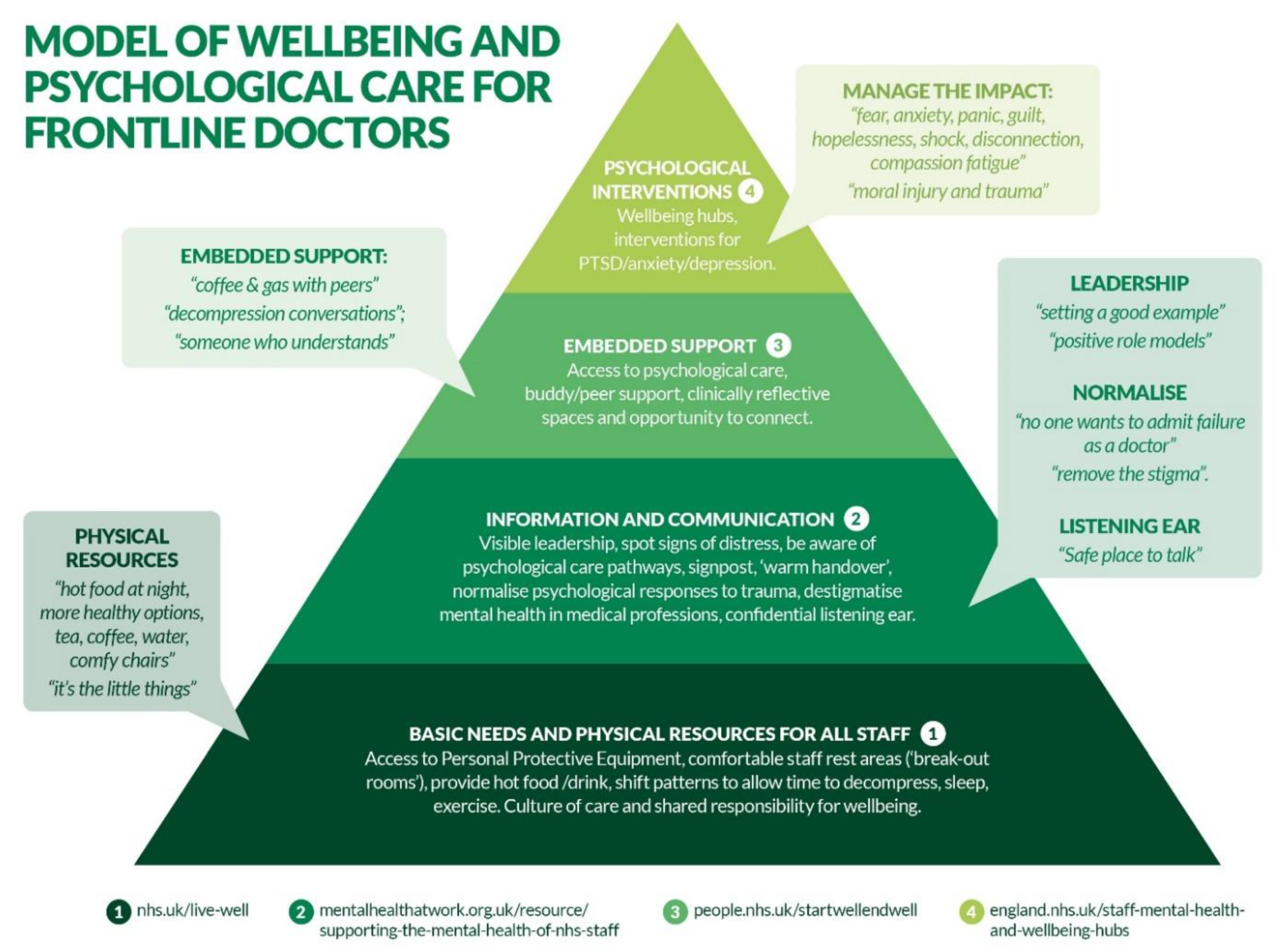
4. Recommendations and Model of Psychological Care
- (1)
- Basic needs and physical resources for all staff
- (2)
- Information and communication
- (3)
- Embedded support
- (4)
- Psychological interventions
- embedded within services (in reach) where possible, offering access to hard to reach groups;
- suitable for ongoing/repeated traumatic events;
- sensitive to mental health stigma known in this population;
- tailored to individual need but considering the wider context of the team wellbeing;
- available in different formats e.g., group, individual, online;
- provided on a regular and reliable basis reflecting best practice;
- accessible to shift workers e.g., by release to attend during work hours;
- able to account for the unique characteristics of working on the frontline, such as moral distress, dealing with uncertainty, fear of harm and concerns over person wellbeing;
5. Discussion
5.1. Strengths and Limitations
5.2. Future Research Directions
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Roberts, T.; Hirst, R.; Sammut-Powell, C.; Reynard, C.; Daniels, J.; Horner, D.; Lyttle, M.D.; Samuel, K.; Graham, B.; Barrett, M.J.; et al. Psychological distress and trauma during the COVID-19 pandemic: Survey of doctors practising anaesthesia, intensive care medicine, and emergency medicine in the United Kingdom and Republic of Ireland. Br. J. Anaesth. 2021, 127, e78–e80. [Google Scholar] [CrossRef]
- Kisely, S.; Warren, N.; McMahon, L.; Dalais, C.; Henry, I.; Siskind, D. Occurrence, prevention, and management of the psychological effects of emerging virus outbreaks on healthcare workers: Rapid review and meta-analysis. BMJ 2020, 369, m1642. [Google Scholar] [CrossRef]
- Pappa, S.; Ntella, V.; Giannakas, T.; Giannakoulis, V.; Papoutsi, E.; Katsaounou, P. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: A systematic review and meta-analysis. Brain Behav. Immun. 2020, 88, 901–907. [Google Scholar] [CrossRef] [PubMed]
- Allan, S.M.; Bealey, R.; Birch, J.; Cushing, T.; Parke, S.; Sergi, G.; Bloomfield, M.; Meiser-Stedman, R. The prevalence of common and stress-related mental health disorders in healthcare workers based in pandemic-affected hospitals: A rapid systematic review and meta-analysis. Eur. J. Psychotraumatol. 2020, 11, 1810903. [Google Scholar] [CrossRef] [PubMed]
- Williamson, V.; Murphy, D.; Greenberg, N. COVID-19 and experiences of moral injury in front-line key workers. Occup. Med. 2020, 70, 317–319. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maunder, R.G.; Lancee, W.J.; Balderson, K.E.; Bennett, J.P.; Borgundvaag, B.; Evans, S.; Fernandes, C.M.; Goldbloom, D.S.; Gupta, M.; Hunter, J.J.; et al. Long-term psychological and occupational effects of providing hospital healthcare during SARS outbreak. Emerg. Infect. Dis. 2006, 12, 1924. [Google Scholar] [CrossRef]
- Lee, S.M.; Kang, W.S.; Cho, A.R.; Kim, T.; Park, J.K. Psychological impact of the 2015 MERS outbreak on hospital workers and quarantined hemodialysis patients. Compr. Psychiatry 2018, 87, 123–127. [Google Scholar] [CrossRef]
- Billings, J.; Kember, T.; Greene, T.; Grey, N.; El-Leithy, S.; Lee, D.; Bloomfield, M. Guidance for Planners of the Psychological Response to Stress Experienced by Hospital Staff Associated with COVID: Early Interventions. COVID Trauma Response Working Group rapid Guidance. 2020. Available online: https://232fe0d6-f8f4-43eb-bc5d- (accessed on 25 May 2021).
- Highfield, J.; Johnston, E.; Jones, T.; Kinman, G.; Maunder, R.; Monaghan, L. The Psychological Needs of Healthcare Staff as a Result of the Coronavirus Pandemic. Br. Psychol. Soc. 2020. Available online: https://www.bps.org.uk/sites/www.bps.org.uk/files/News/News%20-%20Files/Psychological%20needs%20of%20healthcare%20staff.pdf (accessed on 25 May 2021).
- Highfield, J. Advice for Sustaining Staff Wellbeing in Critical Care during and Beyond COVID-19; Intensive Care Society: London, UK, 2020; Available online: https://www.ics.ac.uk/ICS/Wellbeing_hub/PDFs/Sustaining_wellbeing_resource.aspx (accessed on 25 May 2021).
- Makins, H.; Harper, S. Practical Steps to Team Wellbeing During COVID-19. ICM Anaesthesia COVID-19. 2020. Available online: https://icmanaesthesiacovid-19.org/practical-steps-to-team-wellbeing-during-covid19 (accessed on 25 May 2021).
- Kennedy, A. Staff Wellbeing during the COVID-19 Pandemic: Guidance for Organisations. NHS England. 2020. Available online: https://www.ehcap.co.uk/content/sites/ehcap/uploads/NewsDocuments/345/COVID19PsychologicalWellbeingframeworkfororganisations.PDF (accessed on 25 May 2021).
- Shechter, A.; Diaz, F.; Moise, N.; Anstey, D.E.; Ye, S.; Agarwal, S.; Birk, J.L.; Brodie, D.; Cannone, D.E.; Chang, B.; et al. Psychological distress, coping behaviors, and preferences for support among New York healthcare workers during the COVID-19 pandemic. Gen. Hosp. Psychiatry 2020, 66, 1–8. [Google Scholar] [CrossRef]
- Billings, J.; Ching, B.C.; Gkofa, V.; Greene, T.; Bloomfield, M. Healthcare workers experiences of working on the frontline and views about support during COVID-19 and comparable pandemics: A rapid review and meta-synthesis. MedRxiv 2020. [Google Scholar] [CrossRef]
- Bennett, P.; Noble, S.; Johnston, S.; Jones, D.; Hunter, R. COVID-19 confessions: A qualitative exploration of healthcare workers experiences of working with COVID-19. BMJ Open 2020, 10, e043949. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Luo, D.; Haase, J.E.; Guo, Q.; Wang, X.Q.; Liu, S.; Xia, L.; Liu, Z.; Yang, J.; Yang, B.X. The experiences of health-care providers during the COVID-19 crisis in China: A qualitative study. Lancet Glob. Health 2020, 8, e790–e798. [Google Scholar] [CrossRef]
- Moradi, Y.; Baghaei, R.; Hosseingholipour, K.; Mollazadeh, F. Challenges experienced by ICU nurses throughout the provision of care for COVID-19 patients: A qualitative study. J. Nurs. Manag. 2021, 19, 1159–1168. [Google Scholar] [CrossRef] [PubMed]
- Rao, H.; Mancini, D.; Tong, A.; Khan, H.; Gutierrez, B.S.; Mundo, W.; Collings, A.; Cervantes, L. Frontline interdisciplinary clinician perspectives on caring for patients with COVID-19: A qualitative study. BMJ Open 2021, 11, e048712. [Google Scholar] [CrossRef]
- Raza, A.; Matloob, S.; Rahim, N.F.; Halim, H.A.; Khattak, A.; Ahmed, N.H. Factors Impeding Health-Care Professionals to Effectively Treat Coronavirus Disease 2019 Patients in Pakistan: A Qualitative Investigation. Front. Psychol. 2020, 11, 572450. [Google Scholar] [CrossRef]
- Sun, N.; Wei, L.; Shi, S.; Jiao, D.; Song, R.; Ma, L.; Wang, H.; Wang, C.; Wang, Z.; You, Y.; et al. A qualitative study on the psychological experience of caregivers of COVID-19 patients. Am. J. Infect. Control. 2020, 48, 592–598. [Google Scholar] [CrossRef] [PubMed]
- Verhoeven, V.; Tsakitzidis, G.; Philips, H.; Van Royen, P. Impact of the COVID-19 pandemic on the core functions of primary care: Will the cure be worse than the disease? A qualitative interview study in Flemish GPs. BMJ Open 2020, 10, e039674. [Google Scholar] [CrossRef]
- Vindrola-Padros, C.; Andrews, L.; Dowrick, A.; Djellouli, N.; Fillmore, H.; Gonzalez, E.B.; Javadi, D.; Lewis-Jackson, S.; Manby, L.; Mitchinson, L.; et al. Perceptions and experiences of healthcare workers during the COVID-19 pandemic in the, U.K. BMJ Open 2020, 10, e040503. [Google Scholar] [CrossRef]
- Vera San Juan, N.; Aceituno, D.; Djellouli, N.; Sumray, K.; Regenold, N.; Syversen, A.; Mulcahy Symmons, S.; Dowrick, A.; Mitchinson, L.; Singleton, G.; et al. Mental health and well-being of healthcare workers during the COVID-19 pandemic in the UK: Contrasting guidelines with experiences in practice. BJPsych Open 2021, 7, E15. [Google Scholar] [CrossRef]
- Demkowicz, O.; Panayiotou, M.; Parsons, S.; Feltham, A.; Arseneault, L.; Ingram, B.; Patalay, P.; Edge, D.; Pierce, M.; Creswell, C.; et al. Looking back to move forward: Reflections on the strengths and challenges of the COVID-19 UK mental health research response. Front. Psychiatry 2021, 12, 391. [Google Scholar] [CrossRef]
- Brooks, S.K.; Gerada, C.; Chalder, T. Review of literature on the mental health of doctors: Are specialist services needed? J. Ment. Health 2011, 20, 146–156. [Google Scholar] [CrossRef]
- Imo, U.O. Burnout and psychiatric morbidity among doctors in the UK: A systematic literature review of prevalence and associated factors. BJPsych Bull. 2017, 41, 197–204. [Google Scholar] [CrossRef]
- Roberts, T.; Daniels, J.; Hulme, W.; Hirst, R.; Horner, D.; Lyttle, M.D.; Samuel, K.; Graham, B.; Reynard, C.; Barrett, M.J.; et al. Psychological distress and trauma in doctors providing frontline care during the COVID-19 pandemic in the United Kingdom and Ireland: A prospective longitudinal survey cohort study. BMJ Open 2021, 11, e049680. [Google Scholar] [CrossRef]
- Roberts, T.; Daniels, J.; Hulme, W.; Hirst, R.; Horner, D.; Lyttle, M.D.; Samuel, K.; Graham, B.; Reynard, C.; Barrett, M.; et al. Psychological distress during the acceleration phase of the COVID-19 pandemic: A longitudinal survey of doctors practising in emergency medicine, anaesthesia and intensive care medicine in the UK and Ireland. Emerg. Med. J. 2021, 38, 450–459. [Google Scholar] [CrossRef]
- Roberts, T.; Daniels, J.; Hulme, W.; Horner, D.; Lyttle, M.D.; Samuel, K.; Graham, B.; Hirst, R.; Reynard, C.; Barrett, M.; et al. COVID-19 emergency response assessment study: A prospective longitudinal survey of frontline doctors in the UK and Ireland: Study protocol. BMJ Open 2020, 10, e039851. [Google Scholar] [CrossRef]
- Weiss, D.S.; Marmar, C.R. The Impact of Event Scale—Revised. In Assessing Psychological Trauma and PTSD: A Handbook for Practitioners; Wilson, J.P., Keane, T.M., Eds.; Guilford Press: New York, NY, USA, 1997; pp. 399–411. [Google Scholar]
- Brooks, S.K.; Dunn, R.; Amlôt, R.; Rubin, G.J.; Greenberg, N. A systematic, thematic review of social and occupational factors associated with psychological outcomes in healthcare employees during an infectious disease outbreak. J. Occup. Environ. Med. 2018, 60, 248–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Creamer, M.; Bell, R.; Failla, S. Psychometric properties of the impact of event scale—revised. Behav. Res. Ther. 2003, 41, 1489–1496. [Google Scholar] [CrossRef]
- Benfante, A.; Di Tella, M.; Romeo, A.; Castelli, L. Traumatic stress in healthcare workers during COVID-19 pandemic: A review of the immediate impact. Front. Psychol. 2020, 11, 2816. [Google Scholar] [CrossRef] [PubMed]
- d’Ettorre, G.; Ceccarelli, G.; Santinelli, L.; Vassalini, P.; Innocenti, G.P.; Alessandri, F.; Koukopoulos, A.E.; Russo, A.; d’Ettorre, G.; Tarsitani, L. Post-traumatic stress symptoms in healthcare workers dealing with the COVID-19 pandemic: A systematic review. Int. J. Environ. Res. Public Health 2021, 18, 601. [Google Scholar] [CrossRef]
- Buselli, R.; Corsi, M.; Baldanzi, S.; Chiumiento, M.; Del Lupo, E.; Dell’Oste, V.; Bertelloni, C.A.; Massimetti, G.; Dell’Osso, L.; Cristaudo, A.; et al. Professional quality of life and mental health outcomes among health care workers exposed to Sars-Cov-2 (Covid-19). Int. J. Environ. Res. Public Health 2020, 17, 6180. [Google Scholar] [CrossRef] [PubMed]
- Gale, N.K.; Heath, G.; Cameron, E.; Rashid, S.; Redwood, S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med. Res. Methodol. 2013, 13, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Braun, V.; Clarke, V. Can I use TA? Should I use TA? Should I not use TA? Comparing reflexive thematic analysis and other pattern-based qualitative analytic approaches. Couns. Psychother. Res. 2021, 21, 37–47. [Google Scholar] [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int. J. Qual. Health Care 2007, 19, 349–357. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Greenberg, N.; Langston, V.; Jones, N. Trauma risk management (TRiM) in the UK Armed Forces. J. R. Army Med. Corps. 2008, 154, 124–127. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mehta, S.; Machado, F.; Kwizera, A.; Papazian, L.; Moss, M.; Azoulay, É.; Herridge, M. COVID-19: A heavy toll on health-care workers. Lancet Respir. Med. 2021, 9, 226–228. [Google Scholar] [CrossRef]
- Rettie, H.; Daniels, J. Coping and tolerance of uncertainty: Predictors and mediators of mental health during the COVID-19 pandemic. Am. Psychol. 2021, 76, 427–437. [Google Scholar] [CrossRef] [PubMed]
- Jacob, L.; Smith, L.; Armstrong, N.C.; Yakkundi, A.; Barnett, Y.; Butler, L.; McDermott, D.T.; Koyanagi, A.; Shin, J.I.; Meyer, J.; et al. Alcohol use and mental health during COVID-19 lockdown: A cross-sectional study in a sample of UK adults. Drug Alcohol. Depend 2021, 219, 108488. [Google Scholar] [CrossRef] [PubMed]
- West, M. The NHS Crisis of Caring for Staff: What Do We Need To Do. The Kings Fund. 2019. Available online: https://www.kingsfund.org.uk/blog/2019/03/nhs-crisis-caring#:~:text=Humans%20have%20three%20core%20needs,have%20better%20health%20and%20wellbeing (accessed on 10 June 2021).
- Htay, M.N.N.; Marzo, R.R.; Bahari, R.; AlRifai, A.; Kamberi, F.; El-Abasiri, R.A.; Nyamache, J.M.; Hlaing, H.A.; Hassanein, M.; Moe, S.; et al. How healthcare workers are coping with mental health challenges during COVID-19 pandemic?-A cross-sectional multi-countries study. Clin. Epidemiol. Glob. Health 2021, 11, 100759. [Google Scholar] [CrossRef] [PubMed]
- Highfield, J. Intensive Care as a Positive Place to Work: Workforce Wellbeing Best Practice Framework. The Intensive Care Society. 2020. Available online: https://www.cc3n.org.uk/uploads/9/8/4/2/98425184/workforce_wellbeing_best_practice_framework_-_fina.pdf (accessed on 25 May 2021).
- Lown, B.A.; Manning, C.F. The Schwartz Center Rounds: Evaluation of an interdisciplinary approach to enhancing patient-centered communication, teamwork, and provider support. Acad Med. 2010, 85, 1073–1081. [Google Scholar] [CrossRef] [PubMed]
- National Health Service. Start Well End Well. 2020. Available online: https://people.nhs.uk/startwellendwell (accessed on 10 June 2021).
- Van Minde, M.R.C.; van Veen-Belle, D.W.; Ernst-Smelt, H.E.; Rosman, A.N.; Raat, H.; Steegers, E.A.P.; de Kroon, M.L.A. Handover of care and of information by community midwives, maternity care assistants and Preventive Child Healthcare professionals, a qualitative study. Midwifery 2019, 78, 25–31. [Google Scholar] [CrossRef] [Green Version]
- Cohen, D.; Winstanley, S.J.; Greene, G. Understanding doctors’ attitudes towards self-disclosure of mental ill health. Occup. Med. 2016, 66, 383–389. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- National Guideline Alliance (UK). Evidence Reviews for Psychological, Psychosocial and Other Non-Pharmacological Interventions for the Treatment of PTSD in Adults: Post-Traumatic Stress Disorder: Evidence Review, D. London: National Institute for Health and Care Excellence (UK); 2018 Dec. (NICE Guideline, No. 116.). Available online: https://www.ncbi.nlm.nih.gov/books/NBK560230 (accessed on 25 May 2021).
- National Collaborating Centre for Mental Health. Depression: The NICE Guideline on the Treatment and Management of Depression in Adults: Updated Edition. British Psychological Society and Royal College of Psychiatrists. 2010. Available online: http://guidance.nice.org.uk/CG90 (accessed on 25 May 2021).
- Murray, H.; Ehlers, A. Cognitive therapy for moral injury in post-traumatic stress disorder. Cogn. Behav. Ther. 2021, 14, E8. [Google Scholar] [CrossRef] [PubMed]
| Stage 1. | Transcription: Audio recordings were transcribed verbatim and pseudonymised. Detailed notes were taken by each interviewer (all authors), structured around the topic guide and questions to produce a rapid coding matrix. |
| Stage 2. | Familiarisation with the interview: Two authors familiarised themselves with the interview by reviewing the rapid coding notes and full transcript. |
| Stage 3. | Coding: AP developed a matrix in NVivo 12. The initial coding process involved systematically reading (and re-reading) the rapid coding notes and full transcripts for each participant, assigning data to relevant question headings and identifying key subthemes within each component. |
| Stage 4. | Developing a working analytical framework: Qualitative team met to discuss in detail the findings as enabled by the rapid analysis matrix, to agree on the key themes. |
| Stage 5. | Applying the analytical framework: All transcripts were imported into NVivo 12 and the analytical framework established. Each transcript was coded by systematically assigning data to a node in the analytical framework. The framework was revisited after 20 transcripts and additional sub-codes created to aid differentiation of distinct meanings emerging within themes. Ten transcripts were double coded by three researchers (EW, KB, JI) |
| Stage 6. | Charting data: Drawing on the full analysis in NVivo, AP, and KB created a table of the key themes with illustrative quotes and reviewed it with all authors. |
| Stage 7. | Interpreting the data: During regular team meetings (10 meetings over the analysis phase), and via circulation of written materials with the Clinical Advisory Group, impressions and interpretations of the data, coding, and the analytical framework were discussed and agreed. This process was ongoing throughout the analysis process. |
| Characteristic (n = 31) | n (%) |
|---|---|
| Specialty | Anaesthetics = 14 (45%) Emergency Medicine = 13 (42%) Intensive Care = 4 (13%) |
| Gender | Female = 19 (61%) Male = 12 (39%) |
| Seniority | Consultant or equivalent = 10 (32%) Middle grade doctor = 14 (45%) Junior doctor = 7 (22%) |
| Ethnic Origin | White = 23 (74%) Black and Minority Ethnic background = 8 (26%) |
| IES-R Score | Range 24–74; Mean 43.7 (SD 13.3) |
| Theme | Sub-themes | Includes |
|---|---|---|
| A. Coping strategies. Positive and less positive coping strategies |
(1) Storing things up (2) Wait until it gets really bad (3) Psychological help is for others not me | (1) Coping by disconnecting (2) Not realising how bad things have become (3) Others might benefit/need support more |
| B. Sources of support. Formal and informal support available. | (1) What helped at work and outside work (2) What didn’t help at work and outside work | (1) Peer-peer support, senior support, embedded psychological therapists, clinical debrief, apps, family and friends. (2) Peer-peer, senior informal contact, no time to access support. |
| C. Organisational influences on wellbeing. Factors which supported or impeded wellbeing. | (1) Positive influence: Organisational (2) Negative influence: Thoughts on ‘resilience’ | (1) Environmental changes and ‘the little things’, managerial support. (2) Negative environmental changes had a big impact, poor managerial decisions. |
| D. Improving engagement with support. Psychological treatment preferences identified by clinicians. | (1) Facilitators and treatment preferences. (2) Barriers to access | (1) Embedded psychological support, someone who understands us, trust and anonymity, leadership role models, normalising psychological reactions, confidentiality of what is shared. (2) No time off, loss of trust, lack of signposting, too much information, stigma, culture and consequences |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Daniels, J.; Ingram, J.; Pease, A.; Wainwright, E.; Beckett, K.; Iyadurai, L.; Harris, S.; Donnelly, O.; Roberts, T.; Carlton, E. The COVID-19 Clinician Cohort (CoCCo) Study: Empirically Grounded Recommendations for Forward-Facing Psychological Care of Frontline Doctors. Int. J. Environ. Res. Public Health 2021, 18, 9675. https://doi.org/10.3390/ijerph18189675
Daniels J, Ingram J, Pease A, Wainwright E, Beckett K, Iyadurai L, Harris S, Donnelly O, Roberts T, Carlton E. The COVID-19 Clinician Cohort (CoCCo) Study: Empirically Grounded Recommendations for Forward-Facing Psychological Care of Frontline Doctors. International Journal of Environmental Research and Public Health. 2021; 18(18):9675. https://doi.org/10.3390/ijerph18189675
Chicago/Turabian StyleDaniels, Jo, Jenny Ingram, Anna Pease, Elaine Wainwright, Kate Beckett, Lalitha Iyadurai, Sophie Harris, Olivia Donnelly, Tom Roberts, and Edward Carlton. 2021. "The COVID-19 Clinician Cohort (CoCCo) Study: Empirically Grounded Recommendations for Forward-Facing Psychological Care of Frontline Doctors" International Journal of Environmental Research and Public Health 18, no. 18: 9675. https://doi.org/10.3390/ijerph18189675
APA StyleDaniels, J., Ingram, J., Pease, A., Wainwright, E., Beckett, K., Iyadurai, L., Harris, S., Donnelly, O., Roberts, T., & Carlton, E. (2021). The COVID-19 Clinician Cohort (CoCCo) Study: Empirically Grounded Recommendations for Forward-Facing Psychological Care of Frontline Doctors. International Journal of Environmental Research and Public Health, 18(18), 9675. https://doi.org/10.3390/ijerph18189675