
The Efficacy of Renal Replacement Therapy for Rewarming of Patients in Severe Accidental Hypothermia—Systematic Review of the Literature

 , , ,
, , ,  ,
,  , and
, and 
Abstract
1. Introduction
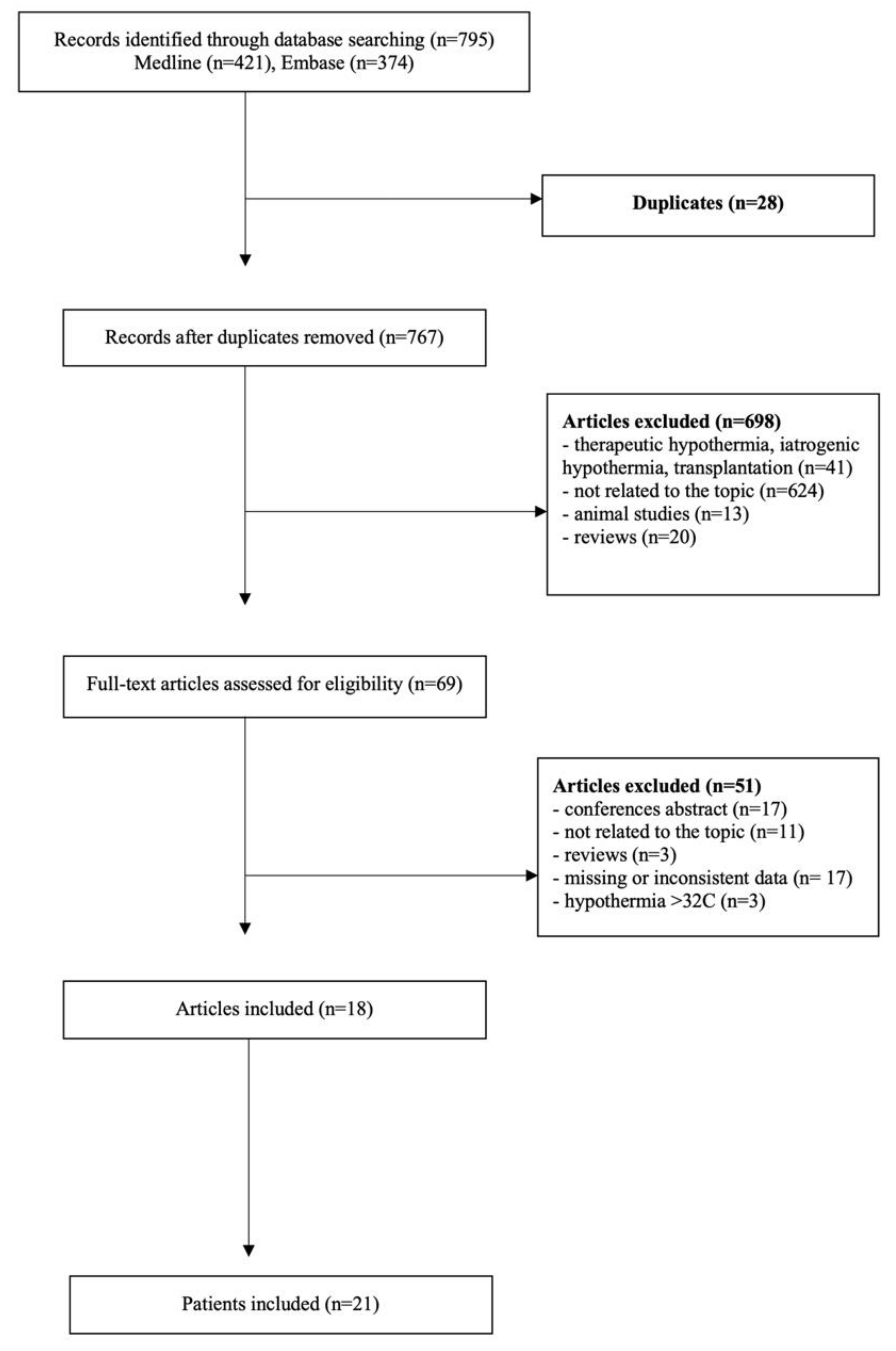
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Musi, M.E.; Sheets, A.; Zafren, K.; Brugger, H.; Paal, P.; Hölzl, N.; Pasquier, M. Clinical Staging of Accidental Hypothermia: The Revised Swiss System. Resuscitation 2021, 162, 182–187. [Google Scholar] [CrossRef] [PubMed]
- Zafren, K. Out-of-Hospital Evaluation and Treatment of Accidental Hypothermia. Emerg. Med. Clin. N. Am. 2017, 35, 261–279. [Google Scholar] [CrossRef] [PubMed]
- Paal, P.; Gordon, L.; Strapazzon, G.; Brodmann Maeder, M.; Putzer, G.; Walpoth, B.; Wanscher, M.; Brown, D.; Holzer, M.; Broessner, G.; et al. Accidental Hypothermia-an Update: The Content of This Review Is Endorsed by the International Commission for Mountain Emergency Medicine (ICAR MEDCOM). Scand. J. Trauma Resusc. Emerg. Med. 2016, 24, 111. [Google Scholar] [CrossRef] [PubMed]
- Mazur, P.; Kosiński, S.; Podsiadło, P.; Jarosz, A.; Przybylski, R.; Litiwnowicz, R.; Piątek, J.; Konstanty-Kalandyk, J.; Gałązkowski, R.; Darocha, T. Extracorporeal Membrane Oxygenation for Accidental Deep Hypothermia-Current Challenges and Future Perspectives. Ann. Cardiothorac. Surg. 2019, 8, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Soar, J.; Nolan, J.P.; Böttiger, B.W.; Perkins, G.D.; Lott, C.; Carli, P.; Pellis, T.; Sandroni, C.; Skrifvars, M.B.; Smith, G.B.; et al. European Resuscitation Council Guidelines for Resuscitation 2015: Section 3. Adult Advanced Life Support. Resuscitation 2015, 95, 100–147. [Google Scholar] [CrossRef]
- Murad, M.H.; Sultan, S.; Haffar, S.; Bazerbachi, F. Methodological Quality and Synthesis of Case Series and Case Reports. BMJ Evid.-Based Med. 2018, 23, 60–63. [Google Scholar] [CrossRef] [PubMed]
- Caluwé, R.; Vanholder, R.; Dhondt, A. Hemodialysis as a Treatment of Severe Accidental Hypothermia. Artif. Organs 2010, 34, 237–239. [Google Scholar] [CrossRef]
- Chen, L.-L.; Fang, J.-T.; Lin, J.-L. Chronic Renal Disease Patients with Severe Star Fruit Poisoning: Hemoperfusion May Be an Effective Alternative Therapy. Clin. Toxicol. Phila. Pa 2005, 43, 197–199. [Google Scholar] [CrossRef]
- Brodersen, H.P.; Meurer, T.; Bolzenius, K.; Konz, K.H.; Larbig, D. Hemofiltration in Very Severe Hypothermia with Favorable Outcome. Clin. Nephrol. 1996, 45, 413–415. [Google Scholar]
- Owda, A.; Osama, S. Hemodialysis in Management of Hypothermia. Am. J. Kidney Dis. Off. J. Natl. Kidney Found. 2001, 38, E8. [Google Scholar] [CrossRef]
- Komatsu, S.; Shimomatsuya, T.; Kobuchi, T.; Nakajima, M.; Amaya, H.; Konishi, S.; Shiraishi, S.; Ono, S.; Maruhashi, K. Severe Accidental Hypothermia Successfully Treated by Rewarming Strategy Using Continuous Venovenous Hemodiafiltration System. J. Trauma 2007, 62, 775–776. [Google Scholar] [CrossRef] [PubMed]
- Rahman, S.; Rubinstein, S.; Singh, J.; Samih, M.; Balsam, L. Early Use of Hemodialysis for Active Rewarming in Severe Hypothermia: A Case Report and Review of Literature. Ren. Fail. 2012, 34, 784–788. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Hernandez, E.; Praga, M.; Alcazar, J.M.; Morales, J.M.; Montejo, J.C.; Jimenez, M.J.; Rodicio, J.L. Hemodialysis for Treatment of Accidental Hypothermia. Nephron 1993, 63, 214–216. [Google Scholar] [CrossRef] [PubMed]
- Sultan, N.; Theakston, K.D.; Butler, R.; Suri, R.S. Treatment of Severe Accidental Hypothermia with Intermittent Hemodialysis. CJEM 2009, 11, 174–177. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Murakami, T.; Yoshida, T.; Kurokochi, A.; Takamatsu, K.; Teranishi, Y.; Shigeta, K.; Tamaki, S.; Morita, S.; Mizuno, R.; Oya, M. Accidental Hypothermia Treated by Hemodialysis in the Acute Phase: Three Case Reports and a Review of the Literature. Intern. Med. Tokyo Jpn. 2019, 58, 2743–2748. [Google Scholar] [CrossRef]
- Hughes, A.; Riou, P.; Day, C. Full Neurological Recovery from Profound (18.0 Degrees C) Acute Accidental Hypothermia: Successful Resuscitation Using Active Invasive Rewarming Techniques. Emerg. Med. J. EMJ 2007, 24, 511–512. [Google Scholar] [CrossRef][Green Version]
- Spooner, K.; Hassani, A. Extracorporeal Rewarming in a Severely Hypothermic Patient Using Venovenous Haemofiltration in the Accident and Emergency Department. J. Accid. Emerg. Med. 2000, 17, 422–424. [Google Scholar] [CrossRef]
- Puzio, T.J.; Chrobak, D.; Jawed, Y.; Tripathy, P.; Carlos, W. Severe Accidental Hypothermia Managed with Continuous Venovenous Hemofiltration. Am. Surg. 2020, 86, 73–75. [Google Scholar] [CrossRef] [PubMed]
- Alfonzo, A.; Lomas, A.; Drummond, I.; McGugan, E. Survival after 5-h Resuscitation Attempt for Hypothermic Cardiac Arrest Using CVVH for Extracorporeal Rewarming. Nephrol. Dial. Transplant. 2009, 24, 1054–1056. [Google Scholar] [CrossRef]
- Carr, M.E.; Wolfert, A.I. Rewarming by Hemodialysis for Hypothermia: Failure of Heparin to Prevent DIC. J. Emerg. Med. 1988, 6, 277–280. [Google Scholar] [CrossRef]
- Singh, T.; Hallows, K.R. Hemodialysis for the Treatment of Severe Accidental Hypothermia. Semin. Dial. 2014, 27, 295–297. [Google Scholar] [CrossRef]
- Wagner, P.L.; Eachempati, S.; Barrio, A.; Muir, J.C.; Wang, J.C.L.; Barie, P.S. Use of Continuous Venovenous Haemodialysis to Reverse Acute Hypothermia after Multiple Trauma. Asian J. Surg. 2008, 31, 151–153. [Google Scholar] [CrossRef][Green Version]
- Hagiwara, S.; Yamada, T.; Furukawa, K.; Ishihara, K.; Nakamura, T.; Ohyama, Y.; Tamura, J.; Oshima, K. Survival after 385 Min of Cardiopulmonary Resuscitation with Extracorporeal Membrane Oxygenation and Rewarming with Haemodialysis for Hypothermic Cardiac Arrest. Resuscitation 2011, 82, 790–791. [Google Scholar] [CrossRef] [PubMed]
- van der Maten, J.; Schrijver, G. Severe Accidental Hypothermia: Rewarming with CVVHD. Neth. J. Med. 1996, 49, 160–163. [Google Scholar] [CrossRef]
- Vanden Hoek, T.L.; Morrison, L.J.; Shuster, M.; Donnino, M.; Sinz, E.; Lavonas, E.J.; Jeejeebhoy, F.M.; Gabrielli, A. Part 12: Cardiac Arrest in Special Situations: 2010 American Heart Association Guidelines for Cardiopulmonary Resuscitation and Emergency Cardiovascular Care. Circulation 2010, 122, S829–S861. [Google Scholar] [CrossRef]
- Watanabe, M.; Matsuyama, T.; Morita, S.; Ehara, N.; Miyamae, N.; Okada, Y.; Jo, T.; Sumida, Y.; Okada, N.; Nozawa, M.; et al. Impact of Rewarming Rate on the Mortality of Patients with Accidental Hypothermia: Analysis of Data from the J-Point Registry. Scand. J. Trauma Resusc. Emerg. Med. 2019, 27, 105. [Google Scholar] [CrossRef] [PubMed]
- Hori, D.; Everett, A.D.; Lee, J.K.; Ono, M.; Brown, C.H.; Shah, A.S.; Mandal, K.; Price, J.E.; Lester, L.C.; Hogue, C.W. Rewarming Rate During Cardiopulmonary Bypass Is Associated With Release of Glial Fibrillary Acidic Protein. Ann. Thorac. Surg. 2015, 100, 1353–1358. [Google Scholar] [CrossRef] [PubMed]
- Jia, D.; Yang, I.X.; Ling, R.R.; Syn, N.; Poon, W.H.; Murughan, K.; Tan, C.S.; Choong, A.M.T.L.; MacLaren, G.; Ramanathan, K. Vascular Complications of Extracorporeal Membrane Oxygenation: A Systematic Review and Meta-Regression Analysis. Crit. Care Med. 2020, 48, e1269–e1277. [Google Scholar] [CrossRef] [PubMed]
- Morita, S.; Seiji, M.; Inokuchi, S.; Sadaki, I.; Inoue, S.; Shigeaki, I.; Akieda, K.; Kazuki, A.; Umezawa, K.; Kazuo, U.; et al. The Efficacy of Rewarming with a Portable and Percutaneous Cardiopulmonary Bypass System in Accidental Deep Hypothermia Patients with Hemodynamic Instability. J. Trauma 2008, 65, 1391–1395. [Google Scholar] [CrossRef] [PubMed]
- Laub, G.W.; Banaszak, D.; Kupferschmid, J.; Magovern, G.J.; Young, J.C. Percutaneous Cardiopulmonary Bypass for the Treatment of Hypothermic Circulatory Collapse. Ann. Thorac. Surg. 1989, 47, 608–611. [Google Scholar] [CrossRef]
- Lee, H.A.; Ames, A.C. HAEMODIALYSIS IN SEVERE BARBITURATE POISONING. Br. Med. J. 1965, 1, 1217–1219. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Deepa, C.; Muralidhar, K. Renal Replacement Therapy in ICU. J. Anaesthesiol. Clin. Pharmacol. 2012, 28, 386. [Google Scholar] [CrossRef] [PubMed]
- 40 Years of Continuous Renal Replacement Therapy; Bellomo, R., Kellum, J.A., La Manna, G., Ronco, C., Eds.; Contributions to nephrology; Karger: Basel, Switzerland; New York, NY, USA, 2018; ISBN 978-3-318-06306-6. [Google Scholar]
- Mendrala, K.; Kosiński, S.; Podsiadło, P.; Pasquier, M.; Mazur, P.; Paal, P.; Gajniak, D.; Darocha, T. The Efficiency of Continuous Renal Replacement Therapy for Rewarming of Patients in Accidental Hypothermia––An Experimental Study. Artif. Organs 2021, aor.14032, Published electronically July 04. [Google Scholar] [CrossRef]
- Bell, M.; Ronco, C.; Hansson, F.; Broman, M. Hypothermia during CRRT, a Comparative Analysis. Acta Anaesthesiol. Scand. 2020, 64, 1162–1166. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Authors/Year of the Publications | Selection | Ascertainment | Causality | Reporting | ||||
|---|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | |
| Caluwe et al. 2010 [7] | ● | ● | ● | n/a | n/a | n/a | ● | ● |
| Chen et al. 2005 [8] | ● | ● | ● | n/a | n/a | n/a | ● | ● |
| Brodersen et al. 1996 [9] | ● | ● | ● | n/a | n/a | n/a | ● | ● |
| Owda et al. 2001 [10] | ● | ● | ● | n/a | n/a | n/a | ● | ● |
| Komatsu et al. 2007 [11] | ● | ● | ● | n/a | n/a | n/a | ● | ● |
| Rahman et al. 2012 [12] | ● | ● | ● | n/a | n/a | n/a | ● | ● |
| Hernandez et al. 1993 [13] | ● | ● | ● | n/a | n/a | n/a | ● | ● |
| Sultan et al. 2009 [14] | ● | ● | ● | n/a | n/a | n/a | ● | ● |
| Murakami et al. 2019 [15] | ● | ● | ● | n/a | n/a | n/a | ● | ● |
| Hughes et al. 2007 [16] | ● | ● | ● | n/a | n/a | n/a | ● | ● |
| Spooner et al. 2000 [17] | ● | ● | ● | n/a | n/a | n/a | ● | ● |
| Puzio et al. 2020 [18] | ● | ● | ● | n/a | n/a | n/a | ● | ● |
| Alfonzo et al. 2009 [19] | ● | ● | ● | n/a | n/a | n/a | ● | ● |
| Carr et al. 1988 [20] | ● | ● | ● | n/a | n/a | n/a | ● | ● |
| Singh et al. 2014 [21] | ● | ● | ● | n/a | n/a | n/a | ● | ● |
| Wagner et al. 2008 [22] | ● | ● | ● | n/a | n/a | n/a | ● | ● |
| Hagiwara et al. 2011 [23] | ● | ● | ● | n/a | n/a | n/a | ● | ● |
| Van der Maten et al. 1996 [24] | ● | ● | ● | n/a | n/a | n/a | ● | ● |
| Authors/Year of the Publications | RRT | Anticoagulation | Tinitial °C | Ttarget °C | Rewarming Rate °C/h | Initial/Ongoing Rewarming Technique | Technical Aspects | CPR | Survived |
|---|---|---|---|---|---|---|---|---|---|
| Caluwe et al. 2010 [7] | HD | No | 28.8 | 35 | 1.1 | wIVF | Qd (39 °C) 500 ml/min Qb 300 ml/min | No | Yes |
| Chen et al. 2005 [8] | HD | NS | 30.4 | 36.8 | 1.6 | wB, wAir, wIVF, RH | NS | No | Yes |
| Brodersen et al. 1996 [9] | HF | NS | 24 | 32 | 1.3 | ns | Heater (37 °C) Qb 180 ml/min | No | Yes |
| Owda et al. 2001 [10] | HD | No | 30.2 | 36.7 | 1.9 | wB, wIVF, PD | NS | No | Yes |
| Komatsu et al. 2007 [11] | CVVHDF | NS | 26.8 | 33.0 | 1.4 | wIVF, wAir | High room temperature Hot dialysate Shorten drains | No | Yes |
| Rahman et al. 2012 [12] | HD | NS | 27.3 | 36.3 | 3.3 | wB, wIVF, wAir | Qd (37 °C) 500 ml/min Qb 300 ml/min | No | Yes |
| Hernandez et al. 1993 [13] | HD | H | 27.4 | 33 | 2.2 | wIVF | Qd (40 °C) 500 ml/min Qb 450–500 ml/min | No | Yes |
| Sultan et al. 2009 [14] | HD | H | 30.6 34.1* | 33 36.3 | 2.1 1.1 | wB, wIVF, WAir, BL | Qd (35–36 °C) 500 ml/min Qb 200 ml/min | No | Yes |
| Murakami et al. 2019 [15] | HD | N | 28.3 | 32.4 | 1.6 | wB, wIV | Qd (35 °C) 500 ml/min Qb 100–150 ml/min | No | Yes |
| HD | H | 28.3 | 32.7 | 1.5 | wB, wIVF | Qd (37 °C) 500 ml/min Qb 150 ml/min | No | Yes | |
| HD | N | 28.2 | 32 | 1.4 | wB, wIVF | Qd (35 °C) 500 ml/min Qb 120 ml/min | No | No | |
| Hughes et al. 2007 [16] | CVVH | NS | 18 | 31 | 3.3 | wIVF, wAir, BL G | blood warmed on outlet drain | Yes | Yes |
| Spooner et al. 2000 [17] | CVVH | H | 30 | 34 | 4 | wB, wIVF, GL, BL | NS | Yes | No |
| Puzio et al. 2020 [18] | CVVHD | NS | 30.7 | 37.2 | 0.6 | wIVF, wB, WE, BL, GL | NS | Yes | Yes |
| Alfonzo et al. 2009 [19] | CVVH | H | 25.1 | 30.2 | 0.7 | wB, wIVF, BL, GL, PL | blood drain heater (38.5 °C) Qb 150–200 ml/min | Yes | Yes |
| Carr et al. 1988 [20] | HD | H | 23.9 | 32.4 | 2.8 | wB, wIVF, wAir | NS | Yes | No |
| Singh et al. 2014 [21] | HD | No | 28 | 34 | 1.5 | wB, wIVF, wAir, PlL, PL | Qd (36–38 °C) 800 ml/min Qb 400 ml/min | Yes | No |
| Wagner et al. 2008 [22] | CVVHD | NS | 32 | 37 | 1.9 | wIVF/other (NS) | Qb 200–300 ml/min | Yes | Yes |
| Hagiwara et al. 2011 [23] | HD | NS | 20 | 31.8 | 2.7 | wB, wIVF | ECMO with no heater | Yes | Yes |
| Van der Maten et al. 1996 [24] | CVVHD | H | 24 | 30 | 1.3 | wB, wIVF, wAir, RH | Qb 100–150 ml/min | Yes | No |
| CVVHD | NS | 21 | 33 | 2.4 | wB, wIVF | NS | No | Yes |
| Authors | Gender | Age | Situational Circumstances | Comorbidities | Neurological Status | BP (mmHg) | ECG | pH | pO2 | pCO2 | Glc | Coagulation | Cr | K | Lac | Hospital Stay (Days) | Neurological Outcome |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Caluwe et al. 2010 [7] | M | 71 | Indoor | DM2 CHF CKD | GCS 9 | NS | AV3 30 /min | 7.09 uc | 46.7 | 78.9 | 39 | PT 61 % | 2.5 | 5.8 | NS | 30 | Good |
| Chen et al. 2005 [8] | M | 60 | NS | DM2 CHF HT AUD | U | 117/52 | NS 91 /min | 7.32 ns | 60.7 | 30.0 | 302 | NS | 7.3 | 4.6 | NS | NS | Good |
| Brodersen et al. 1996 [9] | F | 63 | Indoor | NS | U | NS | STE 50 /min | 7.61 c | NS | NS | 219 | NS | NS | 2.9 | NS | NS | Good |
| Owda et al. 2001 [10] | M | 73 | Outdoor | CHF CKD HT | U | NS | NS 25 /min | NS | NS | NS | NS | NS | NS | NS | NS | NS | NS |
| Komatsu et al. 2007 [11] | M | 48 | Outdoor | NS | GCS 6 | NS | LQT J-waves | 7.18 ns | NS | NS | NS | NS | NS | NS | 13.4 | 6 | Good |
| Rahman et al. 2012 [12] | M | 45 | Outdoor | AUD | D | 110/73 | Sinus J-waves 50 /min | 7.27 ns | 150 | 62 | NS | NS | 0.4 | 3.2 | NS | 5 | Good |
| Hernandez et al. 1993 [13] | M | 43 | Outdoor | NS | U | 50/30 | Sinus 40 /min | 7.11 c | 45 | 19 | NS | APT 81 s | 2.4 | 3.9 | NS | NS | Good |
| Sultan et al. 2009 [14] | M | 65 | Outdoor | NS | GCS 12 | 116/77 | Sinus J-waves wQRS, ST changes 70 /min | 7.27 ns | NS | NS | NS | NS | 0.7 | 2.4 | NS | 2 | Good |
| Murakami et al. 2019 [15] | M | 48 | Outdoor | AUD | GCS 8 | 114/99 | Sinus J-waves LQT 48 /min | 7.20 ns | NS | NS | 60 | NS | 0.4 | 3.6 | 4.7 | 4 | Good |
| M | 78 | Indoor | NS | GCS 3 | 78/40 | Sinus J-waves 39 /min | NS | NS | NS | 54 | NS | NS | NS | NS | NS | NS | |
| F | 77 | Indoor | NS | GCS 3 | 133/83 | J-waves 63 /min | 7.33 ns | NS | NS | NS | NS | NS | 2.8 | 8.5 | NS | Death | |
Hughes et al. 2007 [16] | F | 17 | Outdoor | NS | CPR | CPR | Asystole | 7.17 uc | 30.8 | 63.8 | 112 | INR 2.4 APT ratio 1.6 | NS | 3.2 | NS | 11 | Good |
| Spooner et al. 2000 [17] | F | 77 | Indoor | NS | GCS 8 | 93/55 CPR | Sinus 89 /min VF | NS | NS | NS | NS | NS | NS | NS | NS | 1 | Death |
| Puzio et al. 2020 [18] | F | 25 | NS | DM1 GD | CPR | CPR | NS | NS | NS | NS | NS | NS | NS | NS | NS | 20 | Good |
| Alfonzo et al. 2009 [19] | F | 23 | Outdoor | NS | GCS 3 | CPR | PEA VF | NS | NS | NS | NS | NS | 1* | NS | NS | 16 | Good |
| Carr et al. 1988 [20] | M | 35 | Outdoor | Quadri-plegia | CPR | CPR | VF | 7.24 c | NS | 43.8 | NS | PT 11.7 s PTT 49 s | NS | NS | NS | 1 | Death |
| Singh et al. 2014 [21] | M | 49 | Indoor | AUD | CPR/ROSC | 160/90 | NS 58 /min | 6.80 ns | 90 | 38 | NS | NS | 2.5 | 4.4 | 10.6 | 1 | Death |
| Wagner et al. 2008 [22] | M | 39 | Outdoor (trauma) | NS | GCS 12 | 67/37CPR | NS 100 /min | 6.91 ns | NS | NS | NS | NS | NS | NS | NS | 54 | Good |
| Hagiwara et al. 2011 [23] | F | 30 | Outdoor | NS | CPR | CPR | VF | NS | NS | NS | NS | NS | NS | NS | NS | NS | Good |
| Van der Maten et al. 1996 [24] | M | 46 | Outdoor | None | CPR | CPR | VF | 6.72 ns | NS | NS | 149 | NS | 1 | 5.4 | 24 | 5.5 h | Death |
| M | 27 | Outdoor | NS | GCS 3 | 80/45 | Bradycardia | 7.06 ns | 350 | 78 | 423 | NS | NS | 3.5 | 2.6 | 3 | Good |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mendrala, K.; Kosiński, S.; Podsiadło, P.; Pasquier, M.; Paal, P.; Mazur, P.; Darocha, T. The Efficacy of Renal Replacement Therapy for Rewarming of Patients in Severe Accidental Hypothermia—Systematic Review of the Literature. Int. J. Environ. Res. Public Health 2021, 18, 9638. https://doi.org/10.3390/ijerph18189638
Mendrala K, Kosiński S, Podsiadło P, Pasquier M, Paal P, Mazur P, Darocha T. The Efficacy of Renal Replacement Therapy for Rewarming of Patients in Severe Accidental Hypothermia—Systematic Review of the Literature. International Journal of Environmental Research and Public Health. 2021; 18(18):9638. https://doi.org/10.3390/ijerph18189638
Chicago/Turabian StyleMendrala, Konrad, Sylweriusz Kosiński, Paweł Podsiadło, Mathieu Pasquier, Peter Paal, Piotr Mazur, and Tomasz Darocha. 2021. "The Efficacy of Renal Replacement Therapy for Rewarming of Patients in Severe Accidental Hypothermia—Systematic Review of the Literature" International Journal of Environmental Research and Public Health 18, no. 18: 9638. https://doi.org/10.3390/ijerph18189638
APA StyleMendrala, K., Kosiński, S., Podsiadło, P., Pasquier, M., Paal, P., Mazur, P., & Darocha, T. (2021). The Efficacy of Renal Replacement Therapy for Rewarming of Patients in Severe Accidental Hypothermia—Systematic Review of the Literature. International Journal of Environmental Research and Public Health, 18(18), 9638. https://doi.org/10.3390/ijerph18189638