
Ambient PM2.5 and PM10 Exposure and Respiratory Disease Hospitalization in Kandy, Sri Lanka

 , ,
, , 
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
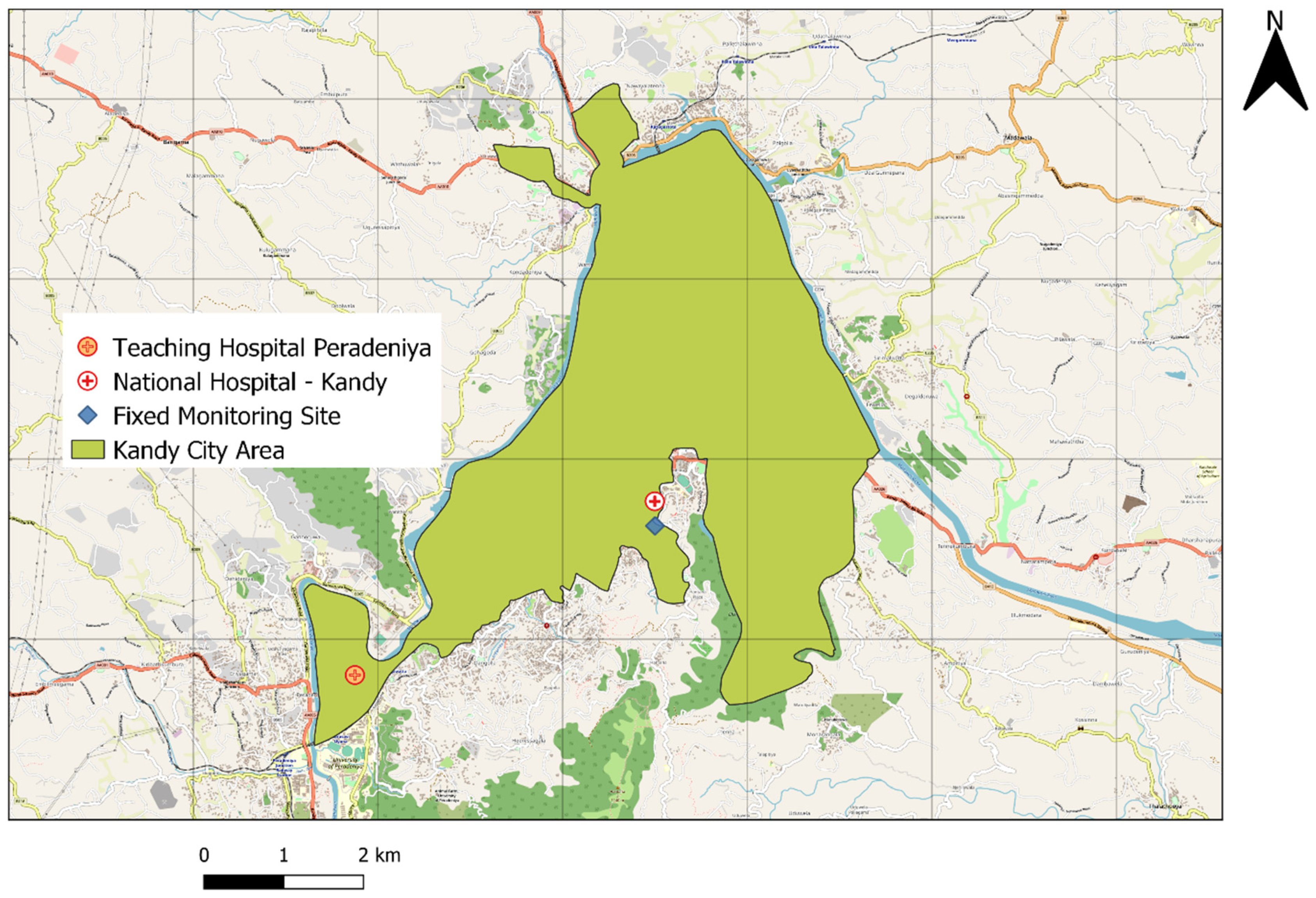
2.1. Study Population
2.2. Air Pollution and Meteorology Data
2.3. Hospitalizations for Respiratory Diseases
2.4. Statistical Analysis
2.4.1. Short Term Effects of PM2.5 and PM10 on Hospitalizations for Respiratory Diseases
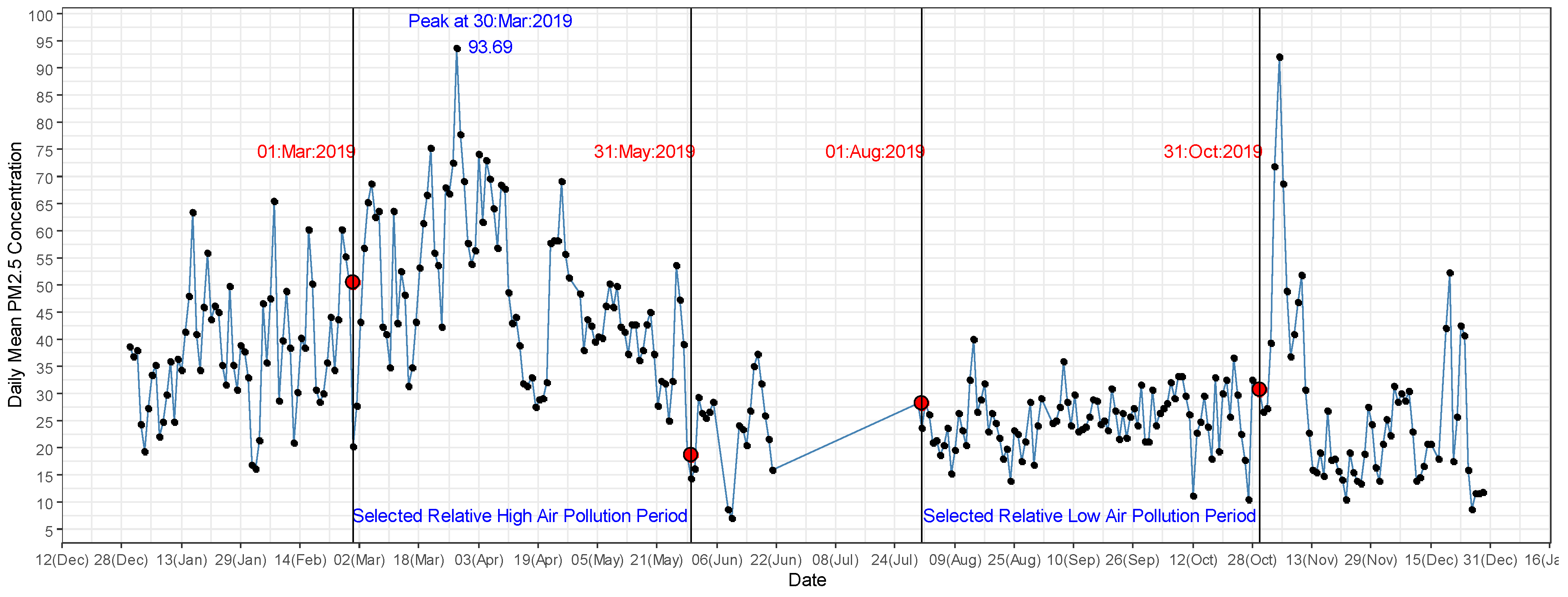
2.4.2. Respiratory Disease Hospitalizations in Two Distinct Air Pollution Seasons in 2019
3. Results
3.1. Associations between Short Term PM2.5 and PM10 Exposure and Hospitalizations for Respiratory Diseases
3.2. Increased Respiratory Disease Hospitalizations in High Air Pollution Period in 2019
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Forum of International Respiratory Societies. The Global Impact of Respiratory Disease, 2nd ed.; European Respiratory Society: Sheffield, UK, 2017; ISBN 9781849840873. [Google Scholar]
- Hubbard, R. The Burden of Lung Disease. Thorax 2006, 61, 557–558. [Google Scholar] [CrossRef] [Green Version]
- Alvarez-Herranz, A.; Balsalobre-Lorente, D.; Shahbaz, M.; Cantos, J.M. Energy Innovation and Renewable Energy Consumption in the Correction of Air Pollution Levels. Energy Policy 2017, 105, 386–397. [Google Scholar] [CrossRef]
- Sun, H.; Kporsu, A.K.; Taghizadeh-Hesary, F.; Edziah, B.K. Estimating Environmental Efficiency and Convergence: 1980 to 2016. Energy 2020, 208, 118224. [Google Scholar] [CrossRef]
- Luo, L.; Zhang, Y.; Jiang, J.; Luan, H.; Yu, C.; Nan, P.; Luo, B.; You, M. Short-Term Effects of Ambient Air Pollution on Hospitalization for Respiratory Disease in Taiyuan, China: A Time-Series Analysis. Int. J. Environ. Res. Public Health 2018, 15, 2160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, F.; Li, L.; Krafft, T.; Lv, J.; Wang, W.; Pei, D. Study on the Association between Ambient Air Pollution and Daily Cardiovascular and Respiratory Mortality in an Urban District of Beijing. Int. J. Environ. Res. Public Health 2011, 8, 2109–2123. [Google Scholar] [CrossRef] [PubMed]
- Phosri, A.; Ueda, K.; Phung, V.L.H.; Tawatsupa, B.; Honda, A.; Takano, H. Effects of Ambient Air Pollution on Daily Hospital Admissions for Respiratory and Cardiovascular Diseases in Bangkok, Thailand. Sci. Total Environ. 2019, 651, 1144–1153. [Google Scholar] [CrossRef] [PubMed]
- Feng, W.; Li, H.; Wang, S.; Van Halm-Lutterodt, N.; An, J.; Liu, Y.; Liu, M.; Wang, X.; Guo, X. Short-Term PM10 and Emergency Department Admissions for Selective Cardiovascular and Respiratory Diseases in Beijing, China. Sci. Total Environ. 2019, 657, 213–221. [Google Scholar] [CrossRef] [PubMed]
- Mannucci, P.M.; Franchini, M. Health Effects of Ambient Air Pollution in Developing Countries. Int. J. Environ. Res. Public Health 2017, 14, 1048. [Google Scholar] [CrossRef]
- Nandasena, Y.L.S.; Wickremasinghe, A.R.; Sathiakumar, N. Air Pollution and Health in Sri Lanka: A Review of Epidemiologic Studies. BMC Public Health 2010, 10, 300. [Google Scholar] [CrossRef] [Green Version]
- Ileperuma, O.A. Review of Air Pollution Studies in Sri Lanka. Ceylon J. Sci. 2020, 49, 225. [Google Scholar] [CrossRef]
- Wickramasinghe, A.P.; Karunaratne, D.G.G.P.; Sivakanesan, R. PM10-Bound Polycyclic Aromatic Hydrocarbons: Concentrations, Source Characterization and Estimating Their Risk in Urban, Suburban and Rural Areas in Kandy, Sri Lanka. Atmos. Environ. 2011, 45, 2642–2650. [Google Scholar] [CrossRef]
- Senaratna, M.; Priyankara, S.; Jayaratne, R.; Morawska, L.; Gayan, B. Monitoring the Air Quality in Kandy Using Smart Sensor Technology. In Proceedings of the Young Scientist’s Symposium on Multidisciplinary Research 2019, Kandy, Sri Lanka, 23–24 May 2019. [Google Scholar]
- Premasiri, H.D.S.; Samarasinghe, I.H.K.; Lakmali, K.M.N. Population Exposure Risk Assessment to Air Pollution in Kandy City Area. In National Building Research Organisation; 2010. Available online: https://nbro.gov.lk/images/content_image/publications/symposia/2010/population_exposure_risk_assessment.pdf (accessed on 10 January 2021).
- Liu, X.; Jayaratne, R.; Thai, P.; Kuhn, T.; Zing, I.; Christensen, B.; Lamont, R.; Dunbabin, M.; Zhu, S.; Gao, J.; et al. Low-Cost Sensors as an Alternative for Long-Term Air Quality Monitoring. Environ. Res. 2020, 185, 109438. [Google Scholar] [CrossRef]
- Zhou, Y.; Zheng, H. Digital Universal Particle Concentration Sensor: PMS5003 Series Data Manual; Plantower: Beijing, China, 2016; p. 15. [Google Scholar]
- Jayaratne, R.; Liu, X.; Thai, P.; Dunbabin, M.; Morawska, L. The Influence of Humidity on the Performance of a Low-Cost Air Particle Mass Sensor and the Effect of Atmospheric Fog. Atmos. Meas. Tech. 2018, 11, 4883–4890. [Google Scholar] [CrossRef] [Green Version]
- Kelly, K.E.; Whitaker, J.; Petty, A.; Widmer, C.; Dybwad, A.; Sleeth, D.; Martin, R.; Butterfield, A. Ambient and Laboratory Evaluation of a Low-Cost Particulate Matter Sensor. Environ. Pollut. 2017, 221, 491–500. [Google Scholar] [CrossRef]
- Peng, R.; Dominici, F.; Louis, T. Model Choice in Time Series Studies of Air Pollution and Mortality. J. R. Stat. Soc. Ser. A-Stat. Soc. 2006, 169, 179–203. [Google Scholar] [CrossRef] [Green Version]
- Ravindra, K.; Rattan, P.; Mor, S.; Aggarwal, A.N. Generalized Additive Models: Building Evidence of Air Pollution, Climate Change and Human Health. Environ. Int. 2019, 132, 104987. [Google Scholar] [CrossRef]
- Dastoorpoor, M.; Sekhavatpour, Z.; Masoumi, K.; Mohammadi, M.J.; Aghababaeian, H.; Khanjani, N.; Hashemzadeh, B.; Vahedian, M. Air Pollution and Hospital Admissions for Cardiovascular Diseases in Ahvaz, Iran. Sci. Total Environ. 2019, 652, 1318–1330. [Google Scholar] [CrossRef]
- Ma, Y.; Zhang, H.; Zhao, Y.; Zhou, J.; Yang, S.; Zheng, X.; Wang, S. Short-Term Effects of Air Pollution on Daily Hospital Admissions for Cardiovascular Diseases in Western China. Environ. Sci. Pollut. Res. 2017, 24, 14071–14079. [Google Scholar] [CrossRef] [PubMed]
- Renjie, C.; Zhuohui, Z.; Haidong, K. Heavy Smog and Hospital Visits in Reversal of Vascular Leak with Imatinib. Am. J. Respitory Crit. Care Med. 2013, 188, 9–11. [Google Scholar]
- Liu, P.; Wang, X.; Fan, J.; Xiao, W.; Wang, Y. Effects of Air Pollution on Hospital Emergency Room Visits for Respiratory Diseases: Urban-Suburban Differences in Eastern China. Int. J. Environ. Res. Public Health 2016, 13, 341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tramuto, F.; Cusimano, R.; Cerame, G.; Vultaggio, M.; Calamusa, G.; Maida, C.M.; Vitale, F. Urban Air Pollution and Emergency Room Admissions for Respiratory Symptoms: A Case-Crossover Study in Palermo, Italy. Environ. Health 2011, 10, 31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Peled, R. Air Pollution Exposure: Who Is at High Risk? Atmos. Environ. 2011, 45, 1781–1785. [Google Scholar] [CrossRef]
- Tian, Y.; Xiang, X.; Juan, J.; Sun, K.; Song, J.; Cao, Y.; Hu, Y. Fine Particulate Air Pollution and Hospital Visits for Asthma in Beijing, China. Environ. Pollut. 2017, 230, 227–233. [Google Scholar] [CrossRef] [PubMed]
- Guarnieri, M.; Balmes, J.R. Outdoor Air Pollution and Asthma. Lancet 2014, 383, 1581–1592. [Google Scholar] [CrossRef] [Green Version]
- Rodopoulou, S.; Samoli, E.; Chalbot, M.-C.G.; Kavouras, I.G. Air Pollution and Cardiovascular and Respiratory Emergency Visits in Central Arkansas: A Time-Series Analysis. Sci. Total Environ. 2015, 536, 872–879. [Google Scholar] [CrossRef] [Green Version]
- Li, M.-H.; Fan, L.-C.; Mao, B.; Yang, J.-W.; Choi, A.M.K.; Cao, W.-J.; Xu, J.-F. Short-Term Exposure to Ambient Fine Particulate Matter Increases Hospitalizations and Mortality in COPD: A Systematic Review and Meta-Analysis. Chest 2016, 149, 447–458. [Google Scholar] [CrossRef]
- Abbey, D.E.; Burchette, R.J.; Knutsen, S.F.; McDonnell, W.F.; Lebowitz, M.D.; Enright, P.L. Long-Term Particulate and Other Air Pollutants and Lung Function in Nonsmokers. Am. J. Respir. Crit. Care Med. 1998, 158, 289–298. [Google Scholar] [CrossRef]
- Zhang, Y.; Peng, M.; Yu, C.; Zhang, L. Burden of Mortality and Years of Life Lost Due to Ambient PM10 Pollution in Wuhan, China. Environ. Pollut. 2017, 230, 1073–1080. [Google Scholar] [CrossRef]
- Tao, Y.; Mi, S.; Zhou, S.; Wang, S.; Xie, X. Air Pollution and Hospital Admissions for Respiratory Diseases in Lanzhou, China. Environ. Pollut. 2014, 185, 196–201. [Google Scholar] [CrossRef]
- Simon, A.K.; Hollander, G.A.; McMichael, A. Evolution of the Immune System in Humans from Infancy to Old Age. Proc. R. Soc. B Biol. Sci. 2015, 282. [Google Scholar] [CrossRef]
- Pruthi, N.; Multani, N. Influence of Age on Lung Function Tests. J. Exerc. Sci. Physiother. 2012, 8, 1–6. [Google Scholar] [CrossRef] [Green Version]
- Meegahakotuwa, U.S.; Nianthi, K.W.G.R. Variation of Annual and Seasonal Rainfall Patterns in Kandy District of Sri Lanka. Int. J. Sci. Res. Publ. 2018, 8. [Google Scholar] [CrossRef]
- Begum, B.A.; Hopke, P.K.; Markwitz, A. Air Pollution by Fine Particulate Matter in Bangladesh. Atmos. Pollut. Res. 2013, 4, 75–86. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
| Factors | Mean (SD) | Min | P25 | Median | P75 | Max |
|---|---|---|---|---|---|---|
| Meteorological factors (daily mean) | ||||||
| Temperature °C | 27.65 (1.99) | 22.21 | 26.33 | 27.59 | 28.85 | 40.03 |
| Humidity % | 73.06 (8.56) | 48.80 | 66.30 | 72.52 | 79.04 | 97.32 |
| Air pollutants (µg/m3) | ||||||
| PM2.5 | 34.48 (15.75) | 7.02 | 23.54 | 30.65 | 42.73 | 93.69 |
| PM10 | 38.52 (18.23) | 7.53 | 25.86 | 33.90 | 47.93 | 107.65 |
| Respiratory disease (mean daily hospital admissions) | ||||||
| All | 30.63 (9.84) | 2 | 24 | 29 | 37 | 60 |
| Male | 16.52 (5.79) | 0 | 13 | 16 | 20 | 36 |
| Female | 14.16 (5.47) | 1 | 11 | 14 | 17 | 32 |
| ≤64 years | 19.33 (6.88) | 2 | 15 | 19 | 23 | 43 |
| 65+ years | 11.33 (4.43) | 0 | 8 | 11 | 14 | 27 |
| Pneumonia | 1.51 (0.74) | 0 | 1 | 1 | 2 | 4 |
| COPD | 7.13 (3.25) | 0 | 5 | 7 | 9 | 20 |
| Asthma | 6.35(2.99) | 0 | 4 | 6 | 8 | 16 |
| Hospitalization Due to All Respiratory Diseases (%) | ||||
|---|---|---|---|---|
| PM2.5 | PM10 | |||
| Lags | PM2.5 | 95% CI | PM10 | 95% CI |
| Lag0 | 1.95 * | 0.25, 3.67 | 1.63 * | 0.16, 3.12 |
| Lag1 | 1.31 | −0.40, 3.06 | 1.12 | −0.37, 2.63 |
| Lag2 | −0.07 | −1.81, 1.69 | −0.06 | −1.57,1.47 |
| Lag3 | −0.64 | −2.38, 1.13 | −0.57 | −2.09, 0.96 |
| Lag4 | −0.29 | −2.06, 1.52 | −0.25 | −1.79, 1.32 |
| Lag5 | −0.55 | −2.33, 1.27 | −0.50 | −2.05, 1.08 |
| Hospitalization due to respiratory diseases—males only (%) | ||||
| Lags | PM2.5 | 95% CI | PM10 | 95% CI |
| Lag0 | 2.24 * | 0.08, 4.44 | 1.96 * | 0.09, 3.87 |
| Lag1 | 1.62 | −0.55, 3.84 | 1.42 | −0.47, 3.33 |
| Lag2 | 0.70 | −1.50, 2.94 | 0.64 | −1.27, 2.59 |
| Lag3 | −0.24 | −2.44, 2.00 | −0.20 | −2.11, 1.75 |
| Lag4 | 0.08 | −2.14, 2.36 | 0.14 | −1.80, 2.12 |
| Lag5 | 0.30 | −1.94, 2.59 | 0.26 | −1.69, 2.25 |
| Hospitalization due to respiratory diseases—female only (%) | ||||
| Lag0 | 2.35 * | 0.08, 4.68 | 1.89 | −0.09, 3.90 |
| Lag1 | 1.71 | −0.60, 4.08 | 1.44 | −0.57, 3.48 |
| Lag2 | −0.19 | −2.53, 2.20 | −0.20 | −2.23, 1.88 |
| Lag3 | −0.33 | −2.69, 2.08 | −0.33 | −2.38, 1.77 |
| Lag4 | 0.08 | −2.32, 2.53 | 0.00 | −2.09, 2.14 |
| Lag5 | −0.45 | −2.86, 2.01 | −0.45 | −2.54, 1.69 |
| Respiratory diseases hospitalization of age 65+ group (%) | ||||
| Lag0 | 2.74 * | 0.29, 5.26 | 2.28 * | 0.15, 4.46 |
| Lag1 | 0.27 | −2.21, 2.82 | 0.19 | −1.97, 2.40 |
| Lag2 | −1.08 | −3.59, 1.49 | −0.95 | −3.14, 1.29 |
| Lag3 | −0.62 | −3.15, 1.99 | −0.48 | −2.70, 1.78 |
| Lag4 | −0.87 | −3.43, 1.77 | −0.70 | −2.94, 1.59 |
| Lag5 | 0.01 | −2.58, 2.66 | 0.04 | −2.21, 2.35 |
| Respiratory diseases hospitalization of age ≤65 group (%) | ||||
| Lag0 | 1.76 | −0.31, 3.87 | 1.49 | −0.30, 3.32 |
| Lag1 | 2.23 * | 0.14, 4.37 | 1.93 * | 0.11, 3.78 |
| Lag2 | 0.82 | −1.30, 2.99 | 0.73 | −1.12, 2.61 |
| Lag3 | −0.39 | −2.50, 1.77 | −0.39 | −2.23, 1.49 |
| Lag4 | 0.33 | −1.83, 2.53 | 0.27 | −1.61, 2.18 |
| Lag5 | −0.45 | −2.62, 1.77 | −0.45 | −2.34, 1.48 |
| Hospitalization due to COPD (%) | ||||
| Lag0 | 2.96 | −0.28, 6.30 | 2.42 | −0.39, 5.31 |
| Lag1 | 1.69 | −1.58, 5.07 | 1.33 | −1.52, 4.25 |
| Lag2 | −1.39 | −4.66, 2.00 | −1.27 | −4.13, 1.68 |
| Lag3 | 0.37 | −2.96, 3.82 | 0.17 | −2.73, 3.16 |
| Lag4 | 0.14 | −3.22, 3.63 | 0.06 | −2.88, 3.08 |
| Lag5 | 2.54 | −0.86, 6.06 | 2.19 | −0.76, 5.23 |
| Hospitalization due to pneumonia (%) | ||||
| Lag0 | 0.37 | −4.35, 5.32 | 0.38 | −3.71, 4.65 |
| Lag1 | 0.03 | −4.71, 5.00 | 0.02 | −4.09, 4.30 |
| Lag2 | −0.58 | −5.37, 4.47 | −0.29 | −4.46, 4.06 |
| Lag3 | 1.73 | −3.23, 6.94 | 1.57 | −2.71, 6.04 |
| Lag4 | 0.64 | −4.49, 6.05 | 0.42 | −4.01, 5.07 |
| Lag5 | 2.67 | −2.44, 8.04 | 2.01 | −2.40, 6.61 |
| Hospitalization due to asthma (%) | ||||
| Lag0 | 4.67 * | 1.23, 8.23 | 4.04 * | 1.06, 7.11 |
| Lag1 | 3.27 | −0.24, 6.90 | 2.85 | −0.19, 5.99 |
| Lag2 | 2.62 | −0.95, 6.32 | 2.26 | −0.84, 5.46 |
| Lag3 | −0.11 | −3.67, 3.59 | −0.02 | −3.13, 3.19 |
| Lag4 | −0.84 | −4.39, 2.85 | −0.79 | −3.89, 2.42 |
| Lag5 | −0.07 | −3.65, 3.65 | −0.24 | −3.37, 2.99 |
| Air Pollution Period | Minimum | Mean (SD) | Maximum | p Value * | |
|---|---|---|---|---|---|
| PM2.5 (µg/m3) | Low | 10.48 | 25.31 (5.38) | 40.04 | <0.0001 |
| High | 18.73 | 48.77 (14.87) | 93.69 | ||
| PM10 (µg/m3) | Low | 11.28 | 27.74 (5.94) | 44.49 | <0.0001 |
| High | 20.81 | 54.97 (17.13) | 107.46 | ||
| Temperature (°C) | Low | 22.21 | 26.36 (1.64) | 29.98 | <0.0001 |
| High | 24.80 | 28.66 (1.33) | 30.84 | ||
| Humidity (%) | Low | 64.88 | 80.07 (6.80) | 97.32 | <0.0001 |
| High | 48.80 | 68.20 (7.98) | 85.51 | ||
| All | Low | 12 | 26.97 (7.14) | 46 | <0.0001 |
| High | 13 | 32.73 (9.07) | 54 | ||
| Male | Low | 3 | 14.02 (4.88) | 31 | <0.0001 |
| High | 9 | 18.09 (5.15) | 36 | ||
| Female | Low | 3 | 12.94 (3.86) | 26 | 0.07 |
| High | 2 | 14.64 (5.81) | 31 | ||
| ≤64 years | Low | 7 | 17.62 (5.16) | 37 | 0.004 |
| High | 9 | 20.51 (6.69) | 38 | ||
| 65+ years | Low | 2 | 9.34 (3.82) | 20 | <0.0001 |
| High | 4 | 12.22 (3.96) | 24 | ||
| Pneumonia | Low | 0 | 1.53 (0.69) | 3 | 0.6561 |
| High | 0 | 1.61(0.76) | 4 | ||
| COPD | Low | 0 | 5.90 (2.75) | 14 | <0.0001 |
| High | 2 | 7.86 (3.26) | 17 | ||
| Asthma | Low | 1 | 5.93 (2.52) | 15 | 0.5948 |
| High | 0 | 6.28 (2.93) | 15 |
| Respiratory Disease Hospitalizations | Rate Ratio (95% CI) |
|---|---|
| All | 1.21 (1.15, 1.28) |
| Male | 1.29 (1.20, 1.39) |
| Female | 1.13 (1.05, 1.22) |
| 65+ years | 1.31 (1.20, 1.43) |
| ≤64 years | 1.16 (1.09, 1.25) |
| COPD | 1.35 (1.20, 1.51) |
| Pneumonia | 1.58 (1.13, 2.20) |
| Asthma | 1.05 (0.93, 1.18) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Priyankara, S.; Senarathna, M.; Jayaratne, R.; Morawska, L.; Abeysundara, S.; Weerasooriya, R.; Knibbs, L.D.; Dharmage, S.C.; Yasaratne, D.; Bowatte, G. Ambient PM2.5 and PM10 Exposure and Respiratory Disease Hospitalization in Kandy, Sri Lanka. Int. J. Environ. Res. Public Health 2021, 18, 9617. https://doi.org/10.3390/ijerph18189617
Priyankara S, Senarathna M, Jayaratne R, Morawska L, Abeysundara S, Weerasooriya R, Knibbs LD, Dharmage SC, Yasaratne D, Bowatte G. Ambient PM2.5 and PM10 Exposure and Respiratory Disease Hospitalization in Kandy, Sri Lanka. International Journal of Environmental Research and Public Health. 2021; 18(18):9617. https://doi.org/10.3390/ijerph18189617
Chicago/Turabian StylePriyankara, Sajith, Mahesh Senarathna, Rohan Jayaratne, Lidia Morawska, Sachith Abeysundara, Rohan Weerasooriya, Luke D. Knibbs, Shyamali C. Dharmage, Duminda Yasaratne, and Gayan Bowatte. 2021. "Ambient PM2.5 and PM10 Exposure and Respiratory Disease Hospitalization in Kandy, Sri Lanka" International Journal of Environmental Research and Public Health 18, no. 18: 9617. https://doi.org/10.3390/ijerph18189617
APA StylePriyankara, S., Senarathna, M., Jayaratne, R., Morawska, L., Abeysundara, S., Weerasooriya, R., Knibbs, L. D., Dharmage, S. C., Yasaratne, D., & Bowatte, G. (2021). Ambient PM2.5 and PM10 Exposure and Respiratory Disease Hospitalization in Kandy, Sri Lanka. International Journal of Environmental Research and Public Health, 18(18), 9617. https://doi.org/10.3390/ijerph18189617