
Intramuscular Injections and Dry Needling within Masticatory Muscles in Management of Myofascial Pain. Systematic Review of Clinical Trials

 ,
,  ,
,  ,
, 
Abstract
:1. Introduction
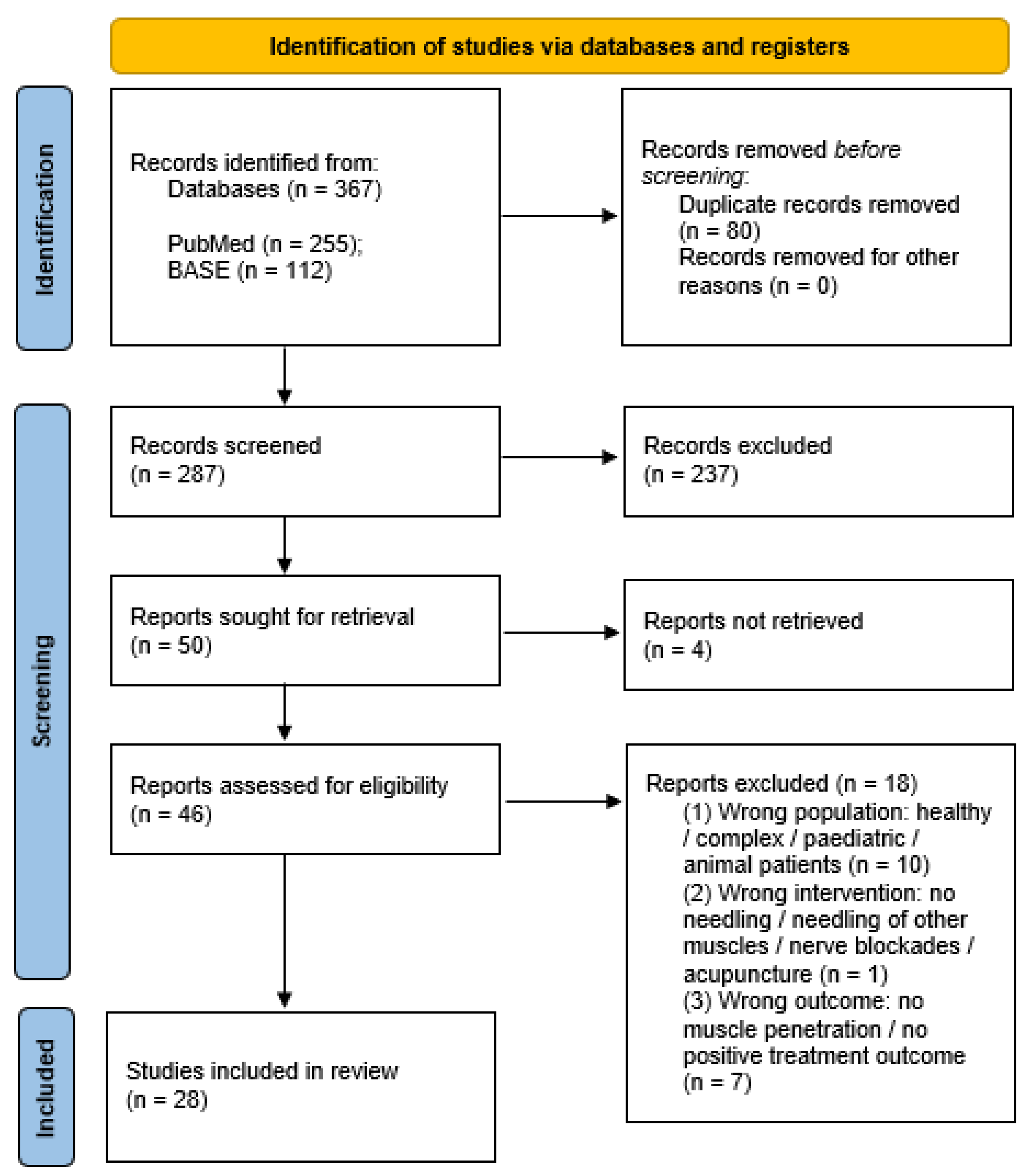
2. Materials and Methods
2.1. Protocol Registration
2.2. Data Sources and Search Strategy
2.3. Eligibility Criteria
2.4. Study Selection
2.5. Data Extraction
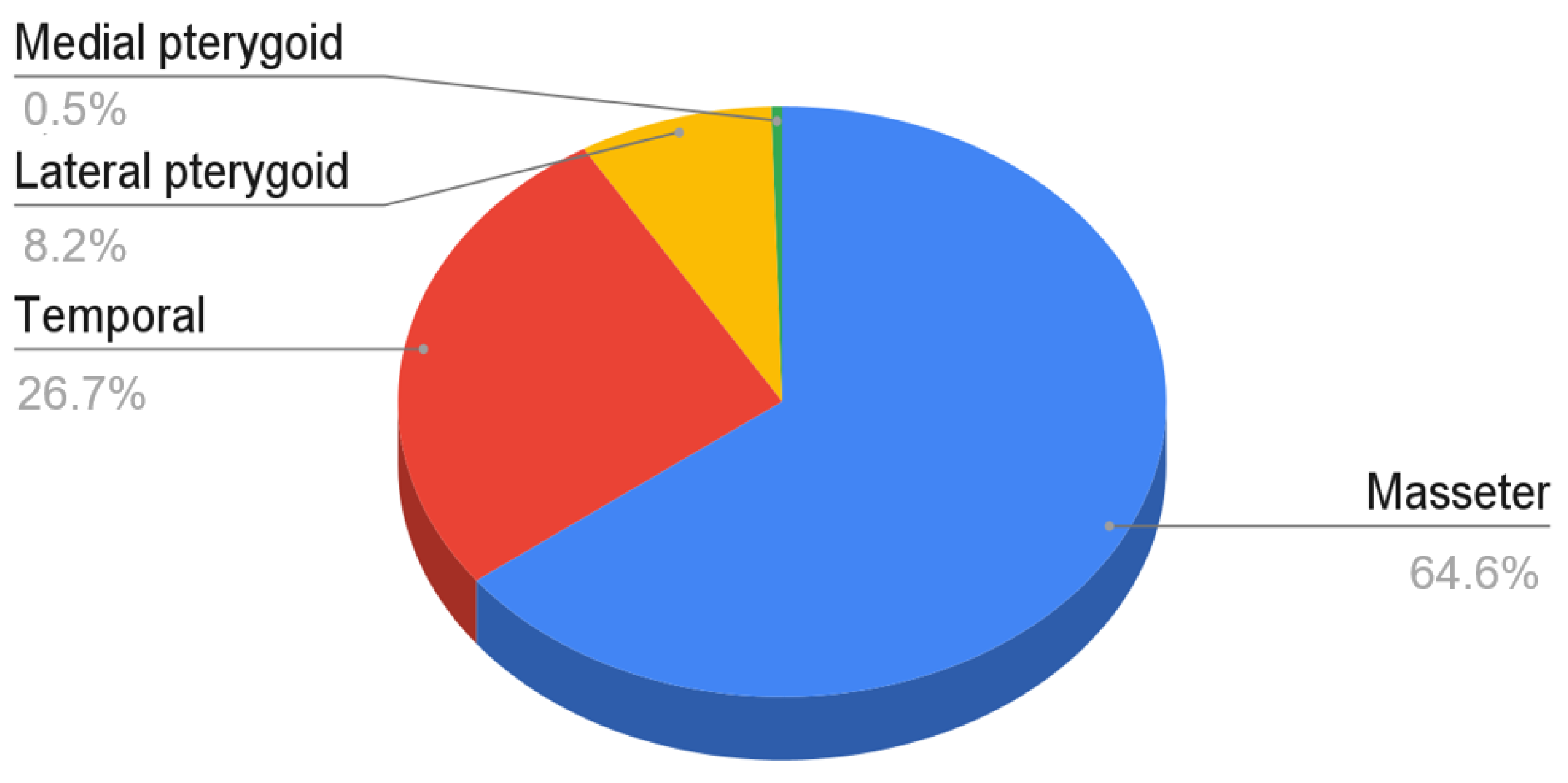
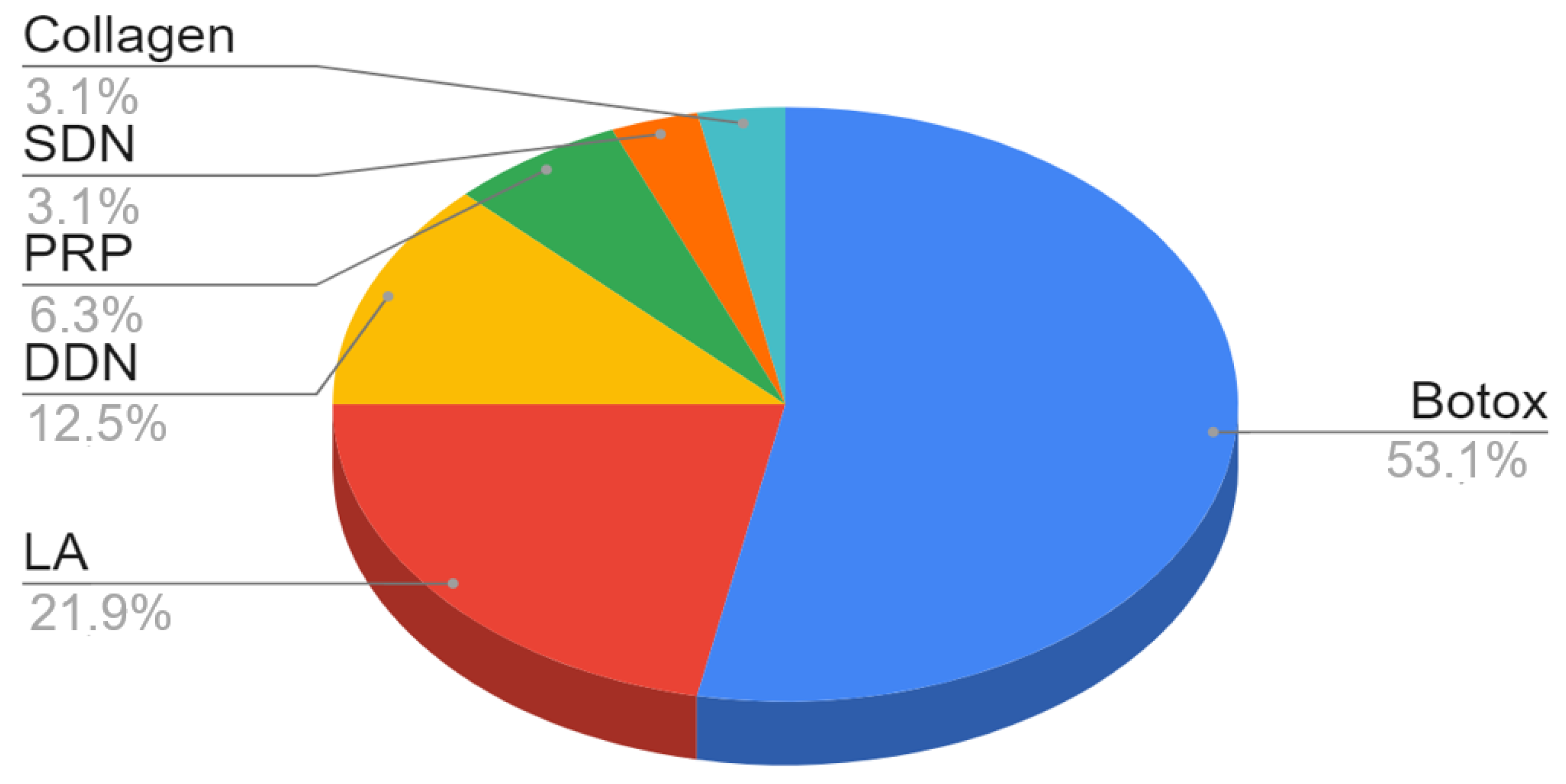
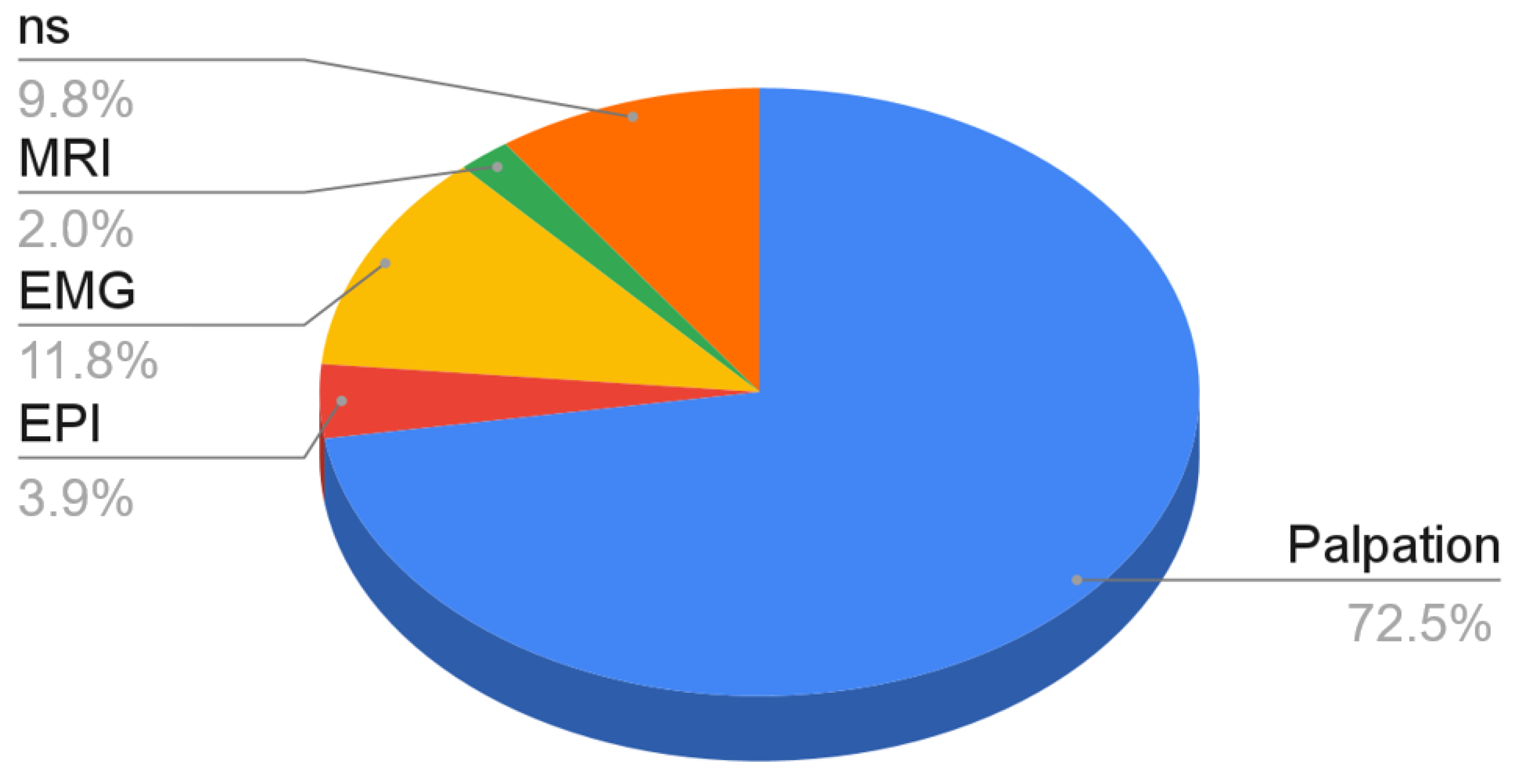
3. Results
4. Discussion
4.1. Intramuscular Injections (Wet Needling)
4.2. Dry Needling
4.3. Techniques Based on Manual Localization
4.4. Techniques Based on Additional Navigation Methods or Support Systems
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Weller, J.L.; Comeau, D.; Otis, J.A.D. Myofascial Pain. Semin. Neurol. 2018, 38, 640–643. [Google Scholar] [PubMed]
- Osiewicz, M.A.; Lobbezoo, F.; Loster, B.W.; Loster, J.E.; Manfredini, D. Frequency of temporomandibular disorders diagnoses based on RDC/TMD in a Polish patient population. CRANIO® 2017, 36, 1–7. [Google Scholar] [CrossRef]
- Deregibus, A.; Ferrillo, M.; Grazia Piancino, M.; Chiara Domini, M.; de Sire, A.; Castroflorio, T. Are occlusal splints effective in reducing myofascial pain in patients with muscle-related temporomandibular disorders? A randomized-controlled trial. Turk. J. Phys. Med. Rehabil. 2021, 67, 32–40. [Google Scholar] [CrossRef]
- Pal, U.S.; Kumar, L.; Mehta, G.; Singh, N.; Singh, G.; Singh, M.; Yadav, H.K. Trends in management of myofacial pain. Natl. J. Maxillofac. Surg. 2014, 5, 109–116. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; et al. Diagnostic Criteria for Temporomandibular Disorders (DC/TMD) for Clinical and Research Applications: Recommendations of the International RDC/TMD Consortium Network* and Orofacial Pain Special Interest Group†. J. Oral Facial Pain Headache 2014, 28, 6–27. [Google Scholar] [CrossRef]
- International Classification of Orofacial Pain, 1st edition (ICOP). Cephalalgia 2020, 40, 129–221. Available online: https://journals.sagepub.com/doi/10.1177/0333102419893823?url_ver=Z39.88-2003&rfr_id=ori:rid:crossref.org&rfr_dat=cr_pub%20%200pubmed (accessed on 7 September 2021). [CrossRef] [Green Version]
- Reissmann, D.R.; John, M.T.; Aigner, A.; Schön, G.; Sierwald, I.; Schiffman, E.L. Interaction Between Awake and Sleep Bruxism Is Associated with Increased Presence of Painful Temporomandibular Disorder. J. Oral Facial Pain Headache 2017, 31, 299–305. [Google Scholar] [CrossRef] [Green Version]
- Wieckiewicz, M.; Zietek, M.; Smardz, J.; Zenczak-Wieckiewicz, D.; Grychowska, N. Mental Status as a Common Factor for Masticatory Muscle Pain: A Systematic Review. Front. Psychol. 2017, 8, 656. [Google Scholar] [CrossRef] [Green Version]
- Nitecka-Buchta, A.; Walczynska-Dragon, K.; Batko-Kapustecka, J.; Wieckiewicz, M. Comparison between Collagen and Lidocaine Intramuscular Injections in Terms of Their Efficiency in Decreasing Myofascial Pain within Masseter Muscles: A Randomized, Single-Blind Controlled Trial. Pain Res. Manag. 2018, 2018, 8261090. [Google Scholar] [CrossRef] [Green Version]
- Fernández-De-Las-Peñas, C.; Nijs, J. Trigger point dry needling for the treatment of myofascial pain syndrome: Current perspectives within a pain neuroscience paradigm. J. Pain Res. 2019, 12, 1899–1911. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Simons, D.G.; Travell, J.G.; Simons, L. Myofascial Pain and Dysfunction. The Trigger Point Manual, 3rd ed.; Wolters Kluwer: Philadelphia, PA, USA, 2019. [Google Scholar]
- Ibarra, J.M.; Ge, H.-Y.; Wang, C.; Vizcaino, V.M.; Graven-Nielsen, T.; Arendt-Nielsen, L. Latent Myofascial Trigger Points are Associated With an Increased Antagonistic Muscle Activity During Agonist Muscle Contraction. J. Pain 2011, 12, 1282–1288. [Google Scholar] [CrossRef]
- Sipahi Calis, A.; Colakoglu, Z.; Gunbay, S. The use of botulinum toxin-a in the treatment of muscular temporomandibular joint disorders. J. Stomatol. Oral Maxillofac. Surg. 2019, 120, 322–325. [Google Scholar] [CrossRef]
- Kim, H.-S.; Yun, P.-Y.; Kim, Y.-K. A clinical evaluation of botulinum toxin-A injections in the temporomandibular disorder treatment. Maxillofac. Plast. Reconstr. Surg. 2016, 38, 5. [Google Scholar] [CrossRef] [Green Version]
- Al-Moraissi, E.A.; Alradom, J.; Aladashi, O.; Goddard, G.; Christidis, N. Needling therapies in the management of myofascial pain of the masticatory muscles: A network meta-analysis of randomised clinical trials. J. Oral Rehabil. 2020, 47, 910–922. [Google Scholar] [CrossRef]
- Amir-Behghadami, M.; Janati, A. Population, Intervention, Comparison, Outcomes and Study (PICOS) design as a framework to formulate eligibility criteria in systematic reviews. Emerg. Med. J. 2020, 37, 387. [Google Scholar] [CrossRef] [PubMed]
- PubMed Overview. Available online: https://pubmed.ncbi.nlm.nih.gov/about/ (accessed on 18 April 2021).
- BASE: Content Providers. Available online: https://www.base-search.net/about/en/about_sources_date.php (accessed on 18 April 2021).
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, 71. [Google Scholar] [CrossRef] [PubMed]
- Rayyan QCRI. Available online: https://www.rayyan.ai/about.html (accessed on 18 April 2021).
- Al-Wayli, H. Treatment of chronic pain associated with nocturnal bruxism with botulinum toxin. A prospective and randomized clinical study. J. Clin. Exp. Dent. 2016, 9, e112–e117. [Google Scholar] [CrossRef]
- Ananthan, S.; Kanti, V.; Zagury, J.G.; Quek, S.Y.; Benoliel, R. The effect of the twin block compared with trigger point injections in patients with masticatory myofascial pain: A pilot study. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2020, 129, 222–228. [Google Scholar] [CrossRef]
- Chaurand, J.; Godínez-Victoria, M.; Tellez-Girón, A.; Facio-Umaña, J.-A.; Jimenez-Ponce, F. Incobotulinum toxin type A for treatment of chronic myofascial pain. J. Oral Sci. 2021, 63, 37–40. [Google Scholar] [CrossRef] [PubMed]
- Chaurand, J.; Pacheco-Ruíz, L.; Orozco-Saldívar, H.; López-Valdés, J. Efficacy of botulinum toxin therapy in treatment of myofascial pain. J. Oral Sci. 2017, 59, 351–356. [Google Scholar] [CrossRef] [Green Version]
- Ernberg, M.; Hedenberg-Magnusson, B.; List, T.; Svensson, P. Efficacy of botulinum toxin type A for treatment of persistent myofascial TMD pain: A randomized, controlled, double-blind multicenter study. Pain 2011, 152, 1988–1996. [Google Scholar] [CrossRef] [PubMed]
- Ghavimi, M.A.; Yazdani, J.; Afzalimehr, A.; Ghoreyshizadeh, A.; Dehnad, S.V. Effect of injection of botulinum toxin on decreasing the symptoms and signs of masticatory muscles in patients with temporomandibular dysfunction. J. Dent. Res. Dent. Clin. Dent. Prospect. 2019, 13, 128–132. [Google Scholar] [CrossRef]
- Guarda-Nardini, L.; Stecco, A.; Stecco, C.; Masiero, S.; Manfredini, D. Myofascial Pain of the Jaw Muscles: Comparison of Short-Term Effectiveness of Botulinum Toxin Injections and Fascial Manipulation Technique. CRANIO® 2012, 30, 95–102. [Google Scholar] [CrossRef] [PubMed]
- Hosgor, H.; Altindis, S. Efficacy of botulinum toxin in the management of temporomandibular myofascial pain and sleep bruxism. J. Korean Assoc. Oral Maxillofac. Surg. 2020, 46, 335–340. [Google Scholar] [CrossRef] [PubMed]
- Ivask, O.; Leibur, E.; Akermann, S.; Tamme, T.; Voog-Oras, Ü. Intramuscular botulinum toxin injection additional to arthrocentesis in the management of temporomandibular joint pain. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2016, 122, e99–e106. [Google Scholar] [CrossRef]
- Kang, S.-K.; Lee, Y.-H.; Park, H.; Ro, J.Y.; Auh, Q.-S. Effects of intramuscular morphine in men and women with temporomandibular disorder with myofascial pain. Oral Dis. 2018, 24, 1591–1598. [Google Scholar] [CrossRef]
- Meral, S.E.; Tüz, H.H.; Başlarlı, Ö. Evaluation of patient satisfaction after botulinum toxin A injection for the management of masticatory myofascial pain and dysfunction—A pilot study. CRANIO® 2019, 39, 12–16. [Google Scholar] [CrossRef]
- Nitecka-Buchta, A.; Walczynska-Dragon, K.; Kempa, W.M.; Baron, S. Platelet-Rich Plasma Intramuscular Injections—Antinociceptive Therapy in Myofascial Pain Within Masseter Muscles in Temporomandibular Disorders Patients: A Pilot Study. Front. Neurol. 2019, 10, 250. [Google Scholar] [CrossRef]
- Ozden, M.C.; Atalay, B.; Özden, A.V.; Çankaya, A.; Kolay, E.; Yıldırım, S. Efficacy of dry needling in patients with myofascial temporomandibular disorders related to the masseter muscle. CRANIO® 2020, 38, 305–311. [Google Scholar] [CrossRef]
- Patel, A.A.; Lerner, M.; Blitzer, A. IncobotulinumtoxinA Injection for Temporomandibular Joint Disorder. Ann. Otol. Rhinol. Laryngol. 2017, 126, 328–333. [Google Scholar] [CrossRef] [PubMed]
- Pihut, M.; Ferendiuk, E.; Szewczyk, M.; Kasprzyk, K.; Wieckiewicz, M. The efficiency of botulinum toxin type A for the treatment of masseter muscle pain in patients with temporomandibular joint dysfunction and tension-type headache. J. Headache Pain 2016, 17, 29. [Google Scholar] [CrossRef] [Green Version]
- Pons, M.; Meyer, C.; Euvrard, E.; Weber, E.; Sigaux, N.; Louvrier, A. MR-guided navigation for botulinum toxin injection in the lateral pterygoid muscle. First results in the treatment of temporomandibular joint disorders. J. Stomatol. Oral Maxillofac. Surg. 2018, 120, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Taşkesen, F.; Cezairli, B. The effectiveness of the masseteric nerve block compared with trigger point injections and dry needling in myofascial pain. CRANIO® 2020, 16, 1–6. [Google Scholar] [CrossRef]
- Tesch, R.D.S.; Macedo, L.C.D.S.P.; Fernandes, F.S.; Filho, G.S.D.G.; Goes, C.P.D.Q.F. Effectiveness of dry needling on the local pressure pain threshold in patients with masticatory myofascial pain. Systematic review and preliminary clinical trial. CRANIO® 2019, 39, 171–179. [Google Scholar] [CrossRef]
- Uemoto, L.; Garcia, M.A.C.; Gouvêa, C.V.D.; Vilella, O.; Alfaya, T.A. Laser therapy and needling in myofascial trigger point deactivation. J. Oral Sci. 2013, 55, 175–181. [Google Scholar] [CrossRef] [Green Version]
- Villa, S.; Raoul, G.; Machuron, F.; Ferri, J.; Nicot, R. Improvement in quality of life after botulinum toxin injection for temporomandibular disorder. J. Stomatol. Oral Maxillofac. Surg. 2018, 120, 2–6. [Google Scholar] [CrossRef] [PubMed]
- Yilmaz, O.; Sivrikaya, E.C.; Taskesen, F.; Pirpir, C.; Ciftci, S. Comparison of the Efficacy of Botulinum Toxin, Local Anesthesia, and Platelet-Rich Plasma Injections in Patients With Myofascial Trigger Points in the Masseter Muscle. J. Oral Maxillofac. Surg. 2020, 79, 88.e1–88.e9. [Google Scholar] [CrossRef]
- Yurttutan, M.E.; Tütüncüler Sancak, K.; Tüzüner, A.M. Which Treatment Is Effective for Bruxism: Occlusal Splints or Botulinum Toxin? J. Oral Maxillofac. Surg. 2019, 77, 2431–2438. [Google Scholar] [CrossRef]
- Gonzalez-Perez, L.; Infante-Cossio, P.; Granados-Nunez, M.; Urresti-Lopez, F.; Martos, R.L.; Ruiz-Canela-Mendez, P. Deep dry needling of trigger points located in the lateral pterygoid muscle: Efficacy and safety of treatment for management of myofascial pain and temporomandibular dysfunction. Med. Oral Patol. Oral Cirugía Bucal 2015, 20, e326–e333. [Google Scholar] [CrossRef]
- Martos, R.L.; Gonzalez-Perez, L.; Ruiz-Canela-Mendez, P.; Urresti-Lopez, F.; Gutierrez-Perez, J.; Infante-Cossio, P. Randomized, double-blind study comparing percutaneous electrolysis and dry needling for the management of temporomandibular myofascial pain. Patol. Oral Cir. Bucal. 2018, 23, e454–e462. [Google Scholar]
- Mesa-Jiménez, J.A.; Fernández-De-Las-Peñas, C.; Koppenhaver, S.L.; Sánchez-Gutiérrez, J.; Arias-Buría, J.L. Cadaveric and in vivo validation of needle placement in the medial pterygoid muscle. Musculoskelet. Sci. Pr. 2020, 49, 102197. [Google Scholar] [CrossRef]
- Grassi, A.; Napoli, F.; Romandini, I.; Samuelsson, K.; Zaffagnini, S.; Candrian, C.; Filardo, G. Is Platelet-Rich Plasma (PRP) Effective in the Treatment of Acute Muscle Injuries? A Systematic Review and Meta-Analysis. Sports Med. 2018, 48, 971–989. [Google Scholar] [CrossRef]
- Gigante, A.; Cianforlini, M.; Busilacchi, A.; Manzotti, S.; Mattioli Belmonte, M. Platelet rich fibrin matrix effects on skeletal muscle lesions: An experimental study. J. Biol. Regul. Homeost. Agents 2012, 26, 475–484. [Google Scholar]
- Tsai, W.C.; Yu, T.Y.; Chang, G.J.; Lin, L.P.; Lin, M.S.; Pang, J.H.S. Platelet-rich plasma releasate promotes regeneration and decreases inflammation and apoptosis of injured skeletal muscle. Am. J. Sports Med. 2018, 46, 1980–1986. [Google Scholar] [CrossRef]
- Contreras-Muñoz, P.; Torrella, J.R.; Serres, X.; Rizo-Roca, D.; De La Varga, M.; Viscor, G.; Martínez-Ibáñez, V.; Peiró, J.L.; Järvinen, T.A.H.; Rodas, G.; et al. Postinjury Exercise and Platelet-Rich Plasma Therapies Improve Skeletal Muscle Healing in Rats but Are Not Synergistic When Combined. Am. J. Sports Med. 2017, 45, 2131–2141. [Google Scholar] [CrossRef] [PubMed]
- Milani, L. A new and refined injectable treatment for musculoskeletal disorders-bioscaffold properties of collagen and its clinical use. Physiol. Regul. Med. 2010, 1, 3–15. [Google Scholar]
- Raphael, K.G.; Tadinada, A.; Bradshaw, J.M.; Janal, M.N.; Sirois, D.A.; Chan, K.C.; Lurie, A.G. Osteopenic consequences of botulinum toxin injections in the masticatory muscles: A pilot study. J. Oral Rehabil. 2014, 41, 555–563. [Google Scholar] [CrossRef] [PubMed]
- De la Torre Canales, G.; Alvarez-Pinzon, N.; Muñoz-Lora, V.R.M.; Vieira Peroni, L.; Farias Gomes, A.; Sánchez-Ayala, A.; Haiter-Neto, F.; Manfredini, D.; Rizzatti-Barbosa, C.M. Efficacy and Safety of Botulinum Toxin Type A on Persistent Myofascial Pain: A Randomized Clinical Trial. Toxins 2020, 12, 395. [Google Scholar] [CrossRef] [PubMed]
- Raphael, K.G.; Janal, M.N.; Tadinada, A.; Santiago, V.; Sirois, D.A.; Lurie, A.G. Effect of multiple injections of botulinum toxin into painful masticatory muscles on bone density in the temporomandibular complex. J. Oral Rehabil. 2020, 47, 1319–1329. [Google Scholar] [CrossRef]
- Autralian Society of Acupuncture Physiotherapists (ASAP). Guidelines for Safe Acupuncture and Dry Needling Practice; Autralian Society of Acupuncture Physiotherapists (ASAP): Wellington, Australia, 2014. [Google Scholar]
- Hong, C.-Z. Lidocaine injection versus dry needling to myofascial trigger point. Am. J. Phys. Med. Rehabil. 1994, 73, 256–263. [Google Scholar] [CrossRef] [PubMed]
- Hakim, I.K.; Takamjani, I.E.; Sarrafzadeh, J.; Ezzati, K.; Bagheri, R. The effect of dry needling on the active trigger point of upper trapezius muscle: Eliciting local twitch response on long-term clinical outcomes. J. Back Musculoskelet. Rehabil. 2019, 32, 717–724. [Google Scholar] [CrossRef] [PubMed]
- Perreault, T.; Dunning, J.; Butts, R. The local twitch response during trigger point dry needling: Is it necessary for successful outcomes? J. Bodyw. Mov. Ther. 2017, 21, 940–947. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borodic, G.E.; Joseph, M.; Fay, L.; Cozzolino, D.; Ferrante, R.J. Botulinum a toxin for the treatment of spasmodic torticollis: Dysphagia and regional toxin spread. Head Neck 1990, 12, 392–399. [Google Scholar] [CrossRef] [PubMed]
- Dantec Clavis Handheld Device. Natus. Available online: https://neuro.natus.com/products-services/dantec-clavis-handheld-emg (accessed on 19 July 2021).
- Wong, E.S.; Lam, C.P.S.; Lau, F.H.S.; Lau, W.W.Y.; Yam, J.C. Botulinum toxin as an initial therapy for management of sixth nerve palsies caused by nasopharyngeal carcinomas. Eye 2018, 32, 768–774. [Google Scholar] [CrossRef] [PubMed]
- Datta Gupta, A.; Tucker, G.; Koblar, S.; Visvanathan, R.; Cameron, I.D. Spatiotemporal Gait Analysis and Lower Limb Functioning in Foot Dystonia Treated with Botulinum Toxin. Toxins 2018, 10, 532. [Google Scholar] [CrossRef] [Green Version]
- Datta Gupta, A.; Visvanathan, R.; Cameron, I.; Koblar, S.A.; Howell, S.; Wilson, D. Efficacy of botulinum toxin in modifying spasticity to improve walking and quality of life in post-stroke lower limb spasticity—A randomized double-blind placebo controlled study. BMC Neurol. 2019, 19, 96. [Google Scholar] [CrossRef] [Green Version]
- Morel, C.; Hauret, I.; Andant, N.; Bonnin, A.; Pereira, B.; Coudeyre, E. Efficacy of two injection-site localisation techniques for botulinum toxin injections: A single-blind, crossover, randomised trial protocol among adults with hemiplegia due to stroke. BMJ Open 2016, 6, e011751. [Google Scholar] [CrossRef]
- Margalef, R.; Bosque, M.; Monclús, P.; Flores, P.; Minaya-Muñoz, F.; Valera-Garrido, F.; Santafé, M.M. Percutaneous Application of Galvanic Current in Rodents Reverses Signs of Myofascial Trigger Points. Evid. Based Complement. Altern. Med. 2020, 2020, 4173218. [Google Scholar]
- Oliveira, A.T.; Camilo, A.A.; Bahia, P.R.V.; Varvalho, A.C.P.; DosSantos, M.; da Silva, J.V.L.; Monteiro, A.A. A Novel Method for Intraoral Access to the Superior Head of the Human Lateral Pterygoid Muscle. BioMed Res. Int. 2014, 2014, 432635. [Google Scholar] [CrossRef] [Green Version]
- Yoshida, K. Computer-Aided Design/Computer-Assisted Manufacture–Derived Needle Guide for Injection of Botulinum Toxin into the Lateral Pterygoid Muscle in Patients with Oromandibular Dystonia. J. Oral Facial Pain Headache 2018, 32, e13–e21. [Google Scholar] [CrossRef]
- Sanabria, S.J.; Ruby, L.; Kuonen, J.; Dettwiler, S.; Colombo, V.; Frauenfelder, T.; Ettlin, D.; Rominger, M.B. Ultrasound Imaging of Injections in Masseter Muscle without Contrast Agent Using Strain Elastography and a Novel B-Mode Spatiotemporal Filter. Ultrasound Med. Biol. 2020, 46, 2717–2735. [Google Scholar] [CrossRef]
- Olchowy, A.; Wieckiewicz, M.; Winocur, E.; Dominiak, M.; Dekkers, I.; Łasecki, M.; Olchowy, C. Great potential of ultrasound elastography for the assessment of the masseter muscle in patients with temporomandibular disorders. A systematic review. Dentomaxillofacial Radiol. 2020, 49, 20200024. [Google Scholar] [CrossRef]
- Kang, J.J.; Kim, J.; Park, S.; Paek, S.; Kim, T.H.; Kim, D.K. Feasibility of Ultrasound-Guided Trigger Point Injection in Patients with Myofascial Pain Syndrome. Healthcare 2019, 7, 118. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ataran, R.; Bahramian, A.; Jamali, Z.; Pishahang, V.; Barzegani, H.S.; Sarbakhsh, P.; Yazdani, J. The Role of Botulinum Toxin A in Treatment of Temporomandibular Joint Disorders: A Review. J. Dent. 2017, 18, 157–164. [Google Scholar]
- Litko, M.; Szkutnik, J.; Berger, M.; Różyło-Kalinowska, I. Correlation between the lateral pterygoid muscle attachment type and temporomandibular joint disc position in magnetic resonance imaging. Dentomaxillofacial Radiol. 2016, 45, 20160229. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Altaweel, A.A.; Elsayed, S.; Baiomy, A.; Abdelsadek, S.E.; Hyder, A.A. Extraoral Versus Intraoral Botulinum Toxin Type A Injection for Management of Temporomandibular Joint Disc Displacement With Reduction. J. Craniofacial Surg. 2019, 30, 2149–2153. [Google Scholar] [CrossRef]
- Tecco, S.; Parisi, M.R.; Gastaldi, G.; Polizzi, E.; D’Amicantonio, T.; Zilocchi, I.; Gardini, I.; Gherlone, E.; Lazzarin, A.; Cappare’, P. Point-of-care testing for hepatitis C virus infection at an Italian dental clinic: Portrait of the pilot study population. N Microbiol. 2019, 42, 133–138. [Google Scholar]
- Sikora, M.; Chęciński, M.; Nowak, Z.; Chęcińska, K.; Olszowski, T.; Chlubek, D. The Use of Titanium 3D Mini-Plates in the Surgical Treatment of Fractures of the Mandibular Condyle: A Systematic Review and Meta-Analysis of Clinical Trials. J. Clin. Med. 2021, 10, 3604. [Google Scholar] [CrossRef] [PubMed]
- Sikora, M.; Czerwińska-Niezabitowska, B.; Chęciński, M.A.; Sielski, M.; Chlubek, D. Short-Term Effects of Intra-Articular Hyaluronic Acid Administration in Patients with Temporomandibular Joint Disorders. J. Clin. Med. 2020, 9, 1749. [Google Scholar] [CrossRef]
- Crespi, R.; Capparè, P.; Gherlone, E. Sinus floor elevation by osteotome: Hand mallet versus electric mallet. A prospective clinical study. Int. J. Oral Maxillofac. Implants 2012, 27, 1144–1150. [Google Scholar]
- Sikora, M.; Chęciński, M.; Nowak, Z.; Chlubek, D. Variants and Modifications of the Retroauricular Approach Using in Temporomandibular Joint Surgery: A Systematic Review. J. Clin. Med. 2021, 10, 2049. [Google Scholar] [CrossRef] [PubMed]
- Sikora, M.; Chęciński, M.; Chlubek, D. Retro-Auricular Approach to the Fractures of the Mandibular Condyle: A Systematic Review. J. Clin. Med. 2021, 10, 230. [Google Scholar] [CrossRef] [PubMed]
- Lucchese, A.; Manuelli, M.; Bassani, L.; Albertini, P.; Matarese, G.; Perillo, L.; Gastaldi, G.; Gherlone, E. Fiber reinforced composites orthodontic retainers. Minerva Stomatol. 2015, 64, 323–333. [Google Scholar]
- D’Orto, B.; Tetè, G.; Polizzi, E. Osseointegrated dental implants supporting fixed prostheses in patients affected by Sjögren’s Sindrome: A narrative review. J. Biol. Regul. Homeost. Agents 2020, 34, 91–93. [Google Scholar] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Search Strategy | |
|---|---|
| PubMed | (masseter OR temporalis OR lateral pterygoid OR medial pterygoid OR masticatory OR mastication) AND (muscle OR muscles OR intra-muscular OR intramuscular OR intra muscular OR trigger points) AND (injection OR injections OR puncture OR punctures OR administration OR needling OR dry needling OR acupuncture) AND (pain OR discomfort OR myofascial pain OR antinociceptive OR anti-nociceptive) AND (therapy OR treatment OR management OR pharmacotherapy OR diagnosis OR diagnostic OR diagnostics) AND (technique OR techniques OR method OR methods OR protocol OR protocols OR guidelines) |
| BASE | (masseter OR temporalis OR pterygoid OR masticatory OR mastication) AND (muscle OR muscles OR intra-muscular OR intramuscular OR intra muscular OR trigger points) AND (injection OR injections OR puncture OR punctures OR administration OR needling OR dry needling OR acupuncture) AND (pain OR discomfort OR myofascial pain OR antinociceptive OR anti-nociceptive) AND (therapy OR treatment OR management OR pharmacotherapy OR diagnosis OR diagnostic OR diagnostics) AND (technique OR techniques OR method OR methods OR protocol OR protocols OR guidelines) |
| Inclusion Criteria | Exclusion Criteria | |
|---|---|---|
| Population | Adult patients with myofascial orofacial pain according to the RDC/TMD or DC/TMD or ICOP | Animal patients, patients suffering with fibromyalgia, neuralgia, oromandibular dystonia, cerebral palsy, hypertrophic masseter muscles, clinically induced pain |
| Intervention | Intramuscular injections into masticatory muscles, dry needling of masticatory muscles | Intramuscular injections into other than masticatory muscles, nerve blockades, acupuncture |
| Comparison | Any or none | - |
| Outcome | Primary outcome: Effective penetration of the masticatory muscle in the course of its needling. Secondary outcome: Any positive treatment outcome (eg. pain decrease, increase in maximum mouth opening, pressure pain threshold increase, MTPs desactivation etc.) | - |
| Study design | Primary studies with an evidence level 1 to 3; description of the needling technique | Papers published prior to 2011; non-English articles |
| Author, Year of Publication | Study Group Size | Wet/Dry Needling (Injected Substance) | Navigation Method or Support System | Needle Penetration Spot(s) | Amount of Injected Substance (per Muscle) | Number of Treatment Sessions |
|---|---|---|---|---|---|---|
| Al-Wayli, 2017 [21] | 25 | BTX | manual palpation; deposition spots located regularly in the lower part of the muscle | 3 sites | 20 IU | 1 |
| Ananthan, 2019 [22] | 25 | LA (2% lidocaine) | digital palpation | MTPs | ns | 1 |
| Chaurand, 2020 [23] | 22 | BTX | digital palpation | 2 sites | 30 IU | 1 |
| Chaurand, 2017 [24] | 11 | BTX | manual palpation; one spot near mandibular angle and one near zygomatic arch | 2 sites | 20 IU | 1 |
| Ernberg, 2011 [25] | 21 | BTX | EMG; 15 mm deep | 3 sites | 50 IU | 2 |
| Ghavimi, 2019 [26] | 61 | BTX | manual palpation; deposition spots located regularly along the long axis of the muscle; 10 mm deep | 3 sites | 50 IU | 1 |
| Guarda-Nardini, 2012 [27] | 15 | BTX | manual palpation; 2 cm skin surface over most prominent area of the muscle after clenching | minimum 5 sites in reverse pyramid pattern | ns | 1 |
| Hosgor, 2020 [28] | 44 | BTX | manual palpation | 3 sites | 150 IU | 1 |
| Ivask,2016 [29] | 20 | BTX | manual palpation; most painful spot | 5 sites | ns | 1 |
| Kang, 2018 [30] | 24 | LA (1,5 or 5 mg morphine sulfate) | manual palpation; most painful spot | 1 site | 0.3 mL | 1 |
| Kang, 2018 [30] | 11 | LA (2% lidocaine) | manual palpation; most painful spot | 1 site | 0.3 mL | 1 |
| Kim, 2016 [30] | 21 | BTX | manual palpation | 3 sites | 150 IU | 1 |
| Meral, 2019 [31] | 25 | BTX | Ns | 6 sites | 24 IU | 1 |
| Nitecka-Buchta, 2019 [32] | 29 | PRP | manual palpation; 5–10 mm deep | 3 MTPs near the origin, under zygomatic arch | 1.5 mL | 1 |
| Nitecka-Buchta, 2018 [9] | 18 | collagen | manual palpation; 10–15 mm deep | MTPs | 2 mL | 2 |
| Nitecka-Buchta, 2018 [9] | 15 | LA (2% lidocaine) | manual palpation; 10–15 mm deep | MTPs | 2 mL | 2 |
| Ozden, 2018 [33] | 20 | DDN | manual palpation and analogue algometer; 10 mm deep | MTPs | - | 3 |
| Ozden, 2018 [33] | 20 | SDN | manual palpation and analogue algometer; 5 mm deep | MTPs | - | 3 |
| Patel, 2017 [34] | 20 | BTX | EMG and monopolar electrode injection needle | ns | 50 IU | 1 |
| Pihut, 2016 [35] | 42 | BTX | manual palpation, area of the greatest cross-section surface of both masseter bellies | ns | 21 IU | 1 |
| Pons, 2018 [36] | 6 | BTX | manual palpation | 3 sites | 30 IU | 1 |
| Sipahi Calis, 2019 [13] | 9 | BTX | EMG | ns | 30 IU | 1 |
| Taskesen, 2020 [37] | 15 | DDN | manual palpation | MTPs | - | 2 |
| Taskesen, 2020 [37] | 15 | LA (2% lidocaine) | manual palpation | MTPs | 0.2 mL | 2 |
| Tesch, 2019 [38] | 5 | DDN | manual palpation | MTPs | - | 3 |
| Uemoto, 2013 [39] | 7 | LA (2% lidocaine) | digital palpation; 10–20 mm deep | MTPs | 0.25 mL | 4 |
| Uemoto, 2013 [39] | 7 | DDN | digital palpation | MTPs | - | 4 |
| Villa, 2018 [40] | 28 | BTX | Ns | 3 sites | 50 IU | 1 |
| Yilmaz, 2020 [41] | 26 | BTX | manual palpation | MTPs | 10 U/MTP | 1 |
| Yilmaz, 2020 [41] | 27 | LA (3% mepivacaine) | manual palpation | MTPs | 0.5 mL/MTP | 1 |
| Yilmaz, 2020 [41] | 29 | PRP | manual palpation | MTPs | 0.5 mL/MTP | 1 |
| Yurttutan, 2019 [42] | 48 | BTX | manual palpation; deposition spots located regularly across the muscle mass | 5 sites | 30 IU | 1 |
| Author, Year of Publication | Study Group Size | Wet/Dry Needling (Injected Substance) | Navigation Method or Support System | Needle Penetration Spot(s) | Amount of Injected Substance (per Muscle) | Number of Treatment Sessions |
|---|---|---|---|---|---|---|
| Ananthan, 2019 [22] | 25 | LA (2% lidocaine) | digital palpation | MTPs | ns | 1 |
| Chaurand, 2020 [23] | 22 | BTX | digital palpation | 2 sites | 20 IU | 1 |
| Chaurand, 2017 [23] | 11 | BTX | digital palpation | 1 MTP | 10 IU | 1 |
| Guarda-Nardini, 2012 [27] | 15 | BTX | manual palpation; 2 cm skin surface over most prominent area of the muscle after clenching | multiple injections in chess-board pattern | ns | 1 |
| Hosgor, 2020 [28] | 44 | BTX | manual palpation | 2 sites | 100 IU | 1 |
| Ivask, 2016 [29] | 20 | BTX | manual palpation; most painful spot | 5 sites | ns | 1 |
| Kim, 2016 [14] | 21 | BTX | manual palpation | 3 sites | 100 IU | 1 |
| Meral, 2019 [31] | 25 | BTX | Ns | 3 sites | 12 IU | 1 |
| Patel, 2017 [34] | 20 | BTX | EMG and monopolar electrode injection needle | ns | 25 IU | 1 |
| Pons, 2018 [36] | 6 | BTX | manual palpation | 2 sites | 20 IU | 1 |
| Sipahi Calis, 2019 [13] | 9 | BTX | EMG | ns | 20 IU | 1 |
| Villa, 2018 [40] | 28 | BTX | Ns | 2 sites | 25 IU | 1 |
| Yurttutan, 2019 [42] | 48 | BTX | Ns | 3 sites | 15 IU | 1 |
| Author, Year of Publication | Study Group Size | Wet/Dry Needling (Injected Substance) | Navigation Method or Support System | Needle Penetration Spot(s) | Amount of Injected Substance (per Muscle) | Number of Treatment Sessions |
|---|---|---|---|---|---|---|
| Gonzalez-Perez, 2015 [43] | 24 | DDN | manual palpation; proper puncture confirmed by jump reaction or local twitch response | MTPs | - | 3 |
| Lopez-Martos, 2018 [44] | 20 | DDN | EPI ® electrotherapy equipment | MTPs | - | 3 |
| Lopez-Martos, 2018 [44] | 20 | PNE | EPI ® electrotherapy equipment | MTPs | - | 3 |
| Patel, 2017 [34] | 20 | BTX | EMG and monopolar electrode injection needle | ns | 10 IU | 1 |
| Pons, 2018 [36] | 6 | BTX | MRI infrared navigation; center of the upper head; about 33 mm from the skin | 1 site | 20 IU | 1 |
| Author, Year of Publication | Study Group Size | Wet/Dry Needling (Injected Substance) | Navigation Method or Support System | Needle Penetration Spot(s) | Amount of Injected Substance (per Muscle) | Number of Treatment Sessions |
|---|---|---|---|---|---|---|
| Mesa-Jimenez, 2020 [45] | 5 | DDN | needle insertion at the inferior angle of the mandibular bone, parallelly to the mandible, advanced from an inferior to superior direction to maximum 30 mm; confirmed by pain referral during insertion | medial surface of the inferior angle of the mandible | - | 1 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Nowak, Z.; Chęciński, M.; Nitecka-Buchta, A.; Bulanda, S.; Ilczuk-Rypuła, D.; Postek-Stefańska, L.; Baron, S. Intramuscular Injections and Dry Needling within Masticatory Muscles in Management of Myofascial Pain. Systematic Review of Clinical Trials. Int. J. Environ. Res. Public Health 2021, 18, 9552. https://doi.org/10.3390/ijerph18189552
Nowak Z, Chęciński M, Nitecka-Buchta A, Bulanda S, Ilczuk-Rypuła D, Postek-Stefańska L, Baron S. Intramuscular Injections and Dry Needling within Masticatory Muscles in Management of Myofascial Pain. Systematic Review of Clinical Trials. International Journal of Environmental Research and Public Health. 2021; 18(18):9552. https://doi.org/10.3390/ijerph18189552
Chicago/Turabian StyleNowak, Zuzanna, Maciej Chęciński, Aleksandra Nitecka-Buchta, Sylwia Bulanda, Danuta Ilczuk-Rypuła, Lidia Postek-Stefańska, and Stefan Baron. 2021. "Intramuscular Injections and Dry Needling within Masticatory Muscles in Management of Myofascial Pain. Systematic Review of Clinical Trials" International Journal of Environmental Research and Public Health 18, no. 18: 9552. https://doi.org/10.3390/ijerph18189552
APA StyleNowak, Z., Chęciński, M., Nitecka-Buchta, A., Bulanda, S., Ilczuk-Rypuła, D., Postek-Stefańska, L., & Baron, S. (2021). Intramuscular Injections and Dry Needling within Masticatory Muscles in Management of Myofascial Pain. Systematic Review of Clinical Trials. International Journal of Environmental Research and Public Health, 18(18), 9552. https://doi.org/10.3390/ijerph18189552