
Circulation of Respiratory Viruses in Hospitalized Adults before and during the COVID-19 Pandemic in Brescia, Italy: A Retrospective Study

 ,
, 
Abstract
:1. Introduction
- (a)
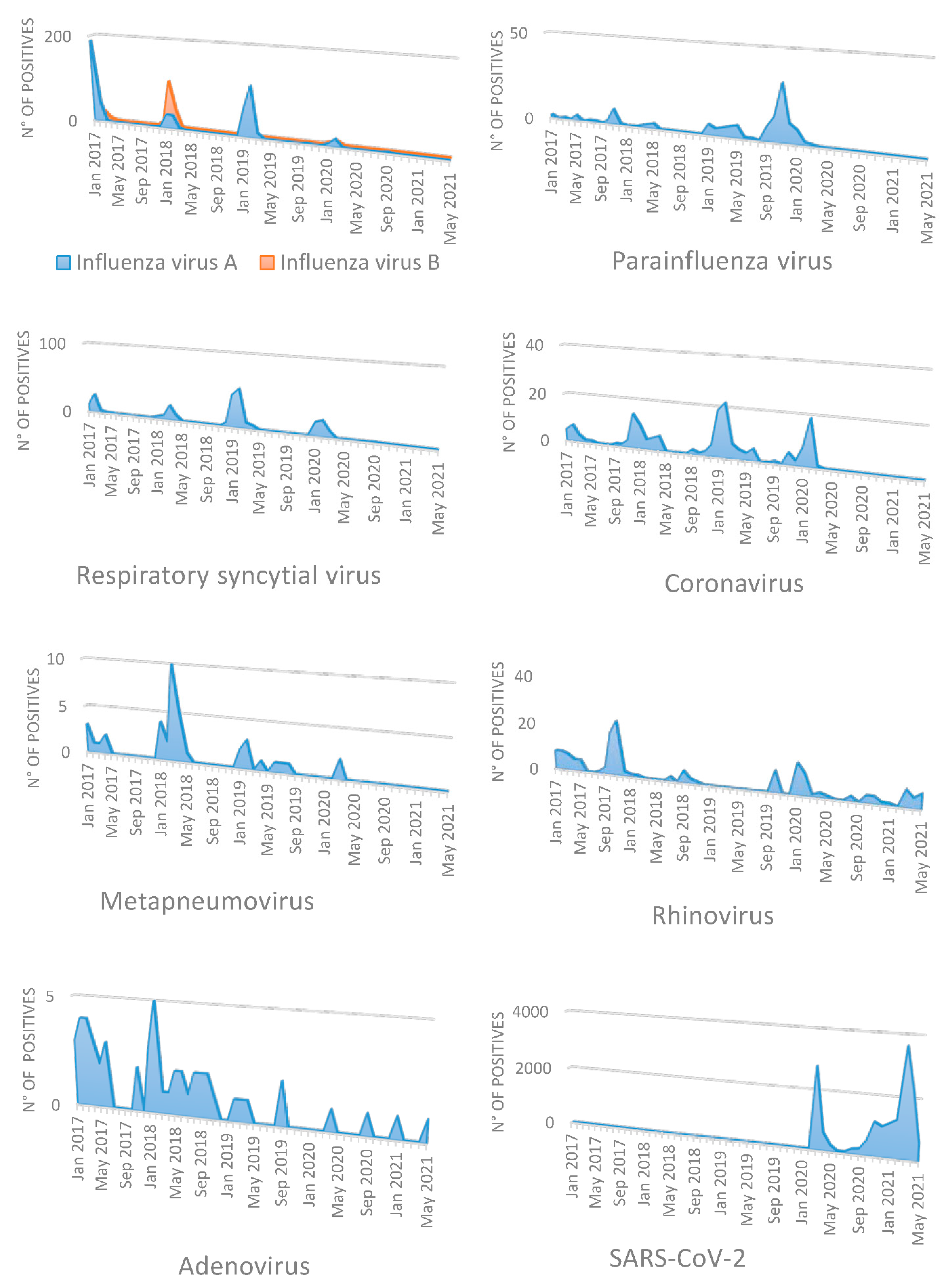
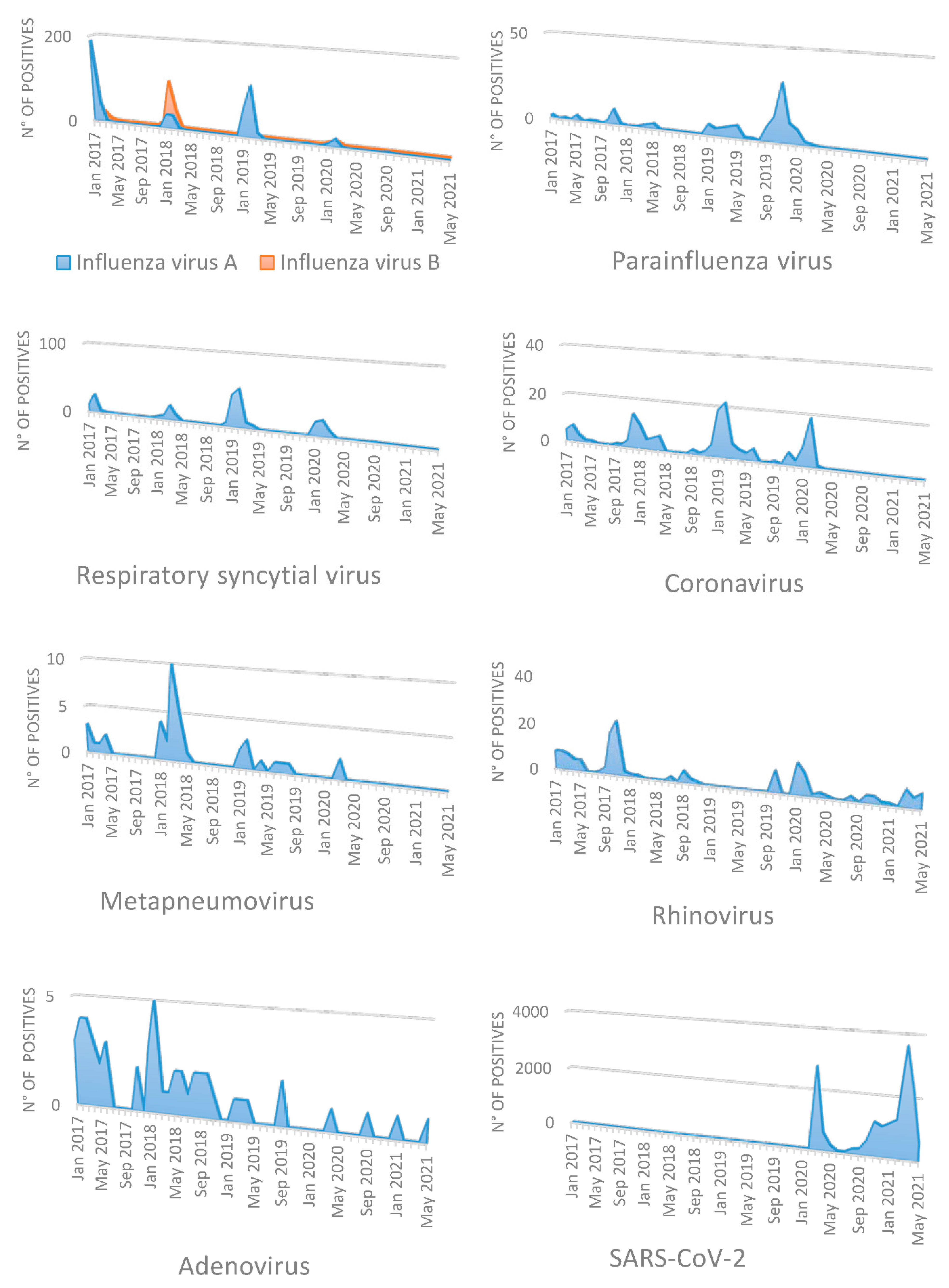
- To evaluate the prevalence of different respiratory viruses (FLU A and FLU B, RV, RSV, hMPV, AdV, PIV and human CoVs) during the COVID-19 pandemic period, in samples collected from hospitalized adults, compared to that observed in the three years before the pandemic period;
- (b)
- To correlate the possible impact of non-pharmaceutical measures, recommended in response to the COVID-19 pandemic, on the circulation of seasonal respiratory viruses.
2. Materials and Methods
2.1. Study Design and Patients
2.2. Detection of Respiratory Viruses and SARS-CoV-2
- (a)
- Respiratory Viral ELITe MGB® Panel (ELITech Italy, Turin, Italy) for influenza viruses (A and B) and RSV detection;
- (b)
- FTD HAdV/HMPV/HBoV (Fast Track Diagnostics) for human metapneumovirus A and B and human adenovirus detection;
- (c)
- FTD HPIV for PIV (serotypes 1, 2, 3 and 4) detection;
- (d)
- FTD (Fast Track Diagnostics) for human endemic coronaviruses (HKU1, NL63, 229 and OC43) detection.
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- James, S.L.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [Green Version]
- Roth, G.A.; Abate, D.; Abate, K.H.; Abay, S.M.; Abbafati, C.; Abbasi, N.; Abbastabar, H.; Abd-Allah, F.; Abdela, J.; Abdelalim, A.; et al. Global, regional, and national age sex-specific mortality for 282 causes of death in 195 countries and territories, 1980–2017: A systematic analysis for the Global Burden of disease Study 2017. Lancet 2018, 392, 1736–1788. [Google Scholar] [CrossRef] [Green Version]
- Blackburn, R.; Zhao, H.; Pebody, R.; Hayward, A.; Warren-Gash, C. Laboratory-confirmed respiratory infections as predictors of hospital admission for myocardial infarction and stroke: Time series analysis of English data for 2004–2015. Clin. Infect. Dis. 2018, 67, 8–17. [Google Scholar] [CrossRef]
- Mohan, A.; Chandra, S.; Agarwal, D.; Guleria, R.; Broor, S.; Gaur, B.; Pandey, R.M. Prevalence of viral infection detected by PCR and RT-PCR in patients with acute exacerbations of COPD: A systematic review. Respirology 2010, 15, 536–542. [Google Scholar] [CrossRef] [PubMed]
- Widmer, K.; Zhu, Y.; Williams, J.V.; Griffin, M.R.; Edwards, K.M.; Keipp, T.H. Rates of hospitalizations for respiratory syncytial virus, human metapneumovirus, and influenza virus in older adults. J. Infect. Dis. 2012, 206, 56–62. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Asten, L.; van den Wijngaard, C.; van Pelt, W.; van de Kassteele, J.; Meijer, A.; van der Hoek, W.; Kretzschmar, M.; Koopmans, M. Mortality attributable to 9 common infections: Significant effect of influenza A, respiratory syncytial virus, influenza B, norovirus, and parainfluenza in elderly persons. J. Infect. Dis. 2012, 206, 628–639. [Google Scholar] [CrossRef] [Green Version]
- Lim, Y.K.; Kweon, O.J.; Kim, H.R.; Kim, T.H.; Lee, M.K. Clinical featuresm epidemiology, and climatic impact of genotype-specific human metapneumovirus infections: Long-term surveillance of hospitalized patients in South Korea. Clin. Infect. Dis. 2020, 70, 2683–2694. [Google Scholar] [CrossRef]
- Falsey, A.R.; Hennessey, P.A.; Formica, M.A.; Cox, C.; Walsh, E.E. Respiratory syncytial virus infection on elderly and high-risk adults. N. Engl. J. Med. 2005, 352, 1749–1759. [Google Scholar] [CrossRef] [PubMed]
- Fendrick, A.; Monto, A.S.; Nightengale, B.; Sarnes, M. The economic burden of non-influenza-related viral respiratory tract infection in the United States. Arch. Intern. Med. 2003, 163, 487–494. [Google Scholar] [CrossRef] [PubMed]
- Covid-19, Situation in Italy. Available online: salute.gov.it (accessed on 7 April 2021).
- Prevention and Response to COVID-19: Evolution of Strategy and Planning in the Transition Phase for the Autumn-Winter Season. Available online: https://www.iss.it/documents/5430402/0/COVID+19+strategyISSMoH+%281%29.pdf/f0d91693-c7ce-880b-e554-643c049ea0f3?t=1604675600974 (accessed on 11 December 2020).
- Leung, N.H.L.; Chu, D.K.W.; Shiu, E.Y.C.; Chan, K.H.; McDevitt, J.J.; Hau, B.J.P.; Yen, H.L.; Li, Y.; Ip, D.K.M.; Peiris, J.S.M.; et al. Respiratory virus shedding in exhaled breath and efficacy of face masks. Nat. Med. 2020, 26, 676–680. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wu, D.; Lu, J.; Liu, Y.; Zhang, Z.; Luo, L. Positive effects of COVID-19 control measures on influenza prevention. Int. J. Infect. Dis. 2020, 95, 345–346. [Google Scholar] [CrossRef]
- Sakamoto, H.; Ishikane, M.; Ueda, P. Seasonal influenza acivity during the SARS-CoV-2 outbreak in Japan. JAMA 2020, 323, 1969–2212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cowling, B.J.; Ali, S.T.; Ng, T.W.Y.; Tsang, T.K.; Li, J.C.M.; Fong, M.W.; Liao, Q.; Kwan, M.Y.; Lee, S.L.; Wu, J.T.; et al. Impact assessment of non-pharmaceutical interventions against coronavirus dsease 2019 and influenza in Hong Kong: An observational study. Lancet Public Health 2020, 5, e279–e288. [Google Scholar] [CrossRef]
- Olsen, S.J.; Winn, A.K.; Budd, A.P.; Prill, M.M.; Steel, J.; Midgley, C.M.; Kniss, K.; Burns, E.; Rowe, T.; Foust, A.; et al. Changes in influenza and other respiratory virus activity during the COVID-19 pandemic—United States, 2020–2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1013–1019. [Google Scholar] [CrossRef]
- Lee, H.; Lee, H.; Song, K.H.; Kim, E.S.; Park, J.S.; Jung, J.; Ahn, S.; Jeong, E.K.; Park, H.; Kim, H.B. Impact of public health interventions on seasonal influenza activity during the SARS-CoV-2 outbreak in Korea. Clin. Infect. Dis. 2021, 73, e132–e140. [Google Scholar] [CrossRef]
- Fricke, L.M.; Glöckner, S.; Dreier, M.; Lange, B. Impact of non-pharmaceutical interventions targeted at COVID-19 pandemic on influenza burden- a systematic review. J. Infect. 2021, 82, 1–35. [Google Scholar] [CrossRef]
- Hatoun, J.; Correa, E.T.; Donahue, S.M.A.; Vernacchio, L. Social distancing for COVID-19 and diagnoses of other infectious diseases in children. Pediatrics 2020, 146, e2020006460. [Google Scholar] [CrossRef] [PubMed]
- Kim, M.C.; Kweon, O.J.; Lim, Y.K.; Choi, S.H.; Chung, J.W.; Lee, M.K. Impact of social distancing on the spread of common respiratory viruses during the coronavirus disease outbreak. PLoS ONE 2021, 16, e0252963. [Google Scholar]
- Park, K.Y.; Seo, S.; Han, J.; Park, J.Y. Respiratory virus surveillance in Canada during the COVID-19 pandemic: An epidemiological analysis of the effectiveness of pandemic-related public health measures in reducing seasonal respiratory viruses test positivity. PLoS ONE 2021, 16, e0253451. [Google Scholar] [CrossRef]
- Rodgers, L.; Sheppard, M.; Smith, A.; Dietz, S.; Jayanthi, P.; Yuan, Y.; Bull, L.; Wotiz, S.; Schwars, T.; Azondekon, R.; et al. Changes in seasonal respiratory illnesses in the United States during the coronavirus disease 2019 (COVID-19) pandemic. Clin. Infect. Dis. 2021, 73, S110–S117. [Google Scholar] [CrossRef]
- Calderaro, A.; De Conto, F.; Buttrini, M.; Piccolo, G.; Montecchini, S.; Maccari, C.; Martinelli, M.; Di Maio, A.; Ferraglia, F.; Pinardi, F.; et al. Human respiratory viruses, including SARS-CoV-2, circulating on the winter season 2019-2020 in Parma, Northern Italy. Int. J. Infect. Dis. 2021, 102, 79–84. [Google Scholar] [CrossRef]
- Sberna, G.; Amendola, A.; Valli, M.B.; Carletti, F.; Capobianchi, M.R.; Bordi, L.; Lalle, E. Trend of respiratory pathogens during the COVID-19 epidemic. J. Clin. Virol. 2020, 129, 104470. [Google Scholar] [CrossRef] [PubMed]
- Satia, I.; Cusack, R.; Greene, J.M.; O’Byrne, P.; Killian, K. Prevalnece and contribution of respiratory viruses in the community to rates of emergency department visits and hospitalizations with respiratory tract infections, chronic obstructive pulmonary disease and asthma. PLoS ONE 2020, 15, e0228544. [Google Scholar] [CrossRef] [PubMed]
- Parry, F.; Shah, A.K.; Sestovic, M.; Salter, S. Precipitous fall in common respiratory viral infections during COVID-19. Open Forum Infect. Dis. 2020, 11, ofaa511. [Google Scholar] [CrossRef]
- Olsen, S.J.; Azziz-Baumgartner, E.; Budd, A.P.; Brammer, L.; Sullivan, S.; Pineda, R.F.; Cohen, C.; Fry, A.M. Decreased influenza activity during the COVID-19 pandemic-Unitd States, Australia, Chile, and South Africa, 2020. Am. J. Transplant. 2020, 20, 3681–3685. [Google Scholar] [CrossRef] [PubMed]
- Baker, R.E.; Park, S.W.; Yang, W.; Vecchi, G.A.; Metcalf, C.J.E.; Grenfell, B.T. The impact of COVID-19 nonpharmaceutical interventions on the future dynamics of endemic infections. Proc. Natl. Acad. Sci. USA 2020, 117, 30547–30553. [Google Scholar] [CrossRef]
- Nickbakhsh, S.; Mair, C.; Matthews, L.; Reeve, R.; Johnson, P.C.D.; Thorburn, F.; von Wissmann, B.; Reynolds, A.; McMenamin, J.; Gunson, R.N.; et al. Virus–virus interactions impact the population dynamics of influenza and the common cold. Proc. Natl. Acad. Sci. USA. 2019, 116, 27142–27150. [Google Scholar] [CrossRef] [Green Version]
- Hsieh, C.; Lin, C.; Wang, W.Y.C.; Pauleen, D.J.; Chen, J.V. The outcome and implications of public precautionary measures in Taiwan. Declining respiratory disease case in the COVID-19 pandemic. Int. J. Environ. Res. Public Health 2020, 17, 4877. [Google Scholar] [CrossRef]
- Partridge, E.; McCleery, E.; Cheema, R.; Nakra, N.; Lakshminrusmha, S.; Tancredi, D.J.; Blumberg, D.A. Evaluation of seasonal respiratory virus activity before and after the statewide COVID-19 shelter-in-place order in North California. JAMA Netw. Open 2021, 4, e2035281. [Google Scholar] [CrossRef] [PubMed]
- Yeoh, D.K.; Foley, D.A.; Minney-Smith, C.A.; Marin, A.C.; Mace, A.O.; Sikazwe, C.T.; Le, H.; Levy, A.; Blyth, C.C.; Moore, H.C. The impact of COVID-19 public health measures on detection of influenza and respiratory syncytial virus in children during the 2020 Australian winter. Clin. Infect. Dis. 2020, 72, 2199–2202. [Google Scholar] [CrossRef]
- Varela, F.H.; Scotta, M.C.; Polese-Bonatto, M.; Sartor, I.T.S.; Ferreira, C.F.; Fernandes, I.R.; Zavaglia, G.O.; Ferreira de Almeida, W.A.; Arakaki-Sanchez, D.; Pinto, L.A.; et al. Absence of detection of RSV and influenza during the COVID-19 pandemic in a Brazilian cohort: Likely role of a lower transmission in the community. J. Glob. Health 2021, 11, 05007. [Google Scholar] [CrossRef]
- Agh, R.; Avner, J.R. Delayed seasonal RSV surge observed during the COVID-19 pandemic. Pediatrics 2021, 148, e2021052089. [Google Scholar] [CrossRef]
- Lavoie, P.M.; Reicherz, F.; Solimano, A.; Langley, J.M. Potential resurgence of respiratory syncytial virus in Canada. CMAJ 2021, 193, E1140–E1141. [Google Scholar] [CrossRef] [PubMed]
- Takashita, E.; Kawakami, C.; Momoki, T.; Saikusa, M.; Shimizu, K.; Ozawa, H.; Kimazaki, M.; Usuku, S.; Tanaka, N.; Okubo, I.; et al. Increased risk of rhinovirus infection in children during the coronavirus disease-19 pandemic. Influenza Other Respir. Viruses 2021, 15, 488–494. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, Y.; Kamioka, Y.; Seki, M. Rhinovirus infected patients in the COVID-19 pandemic period. Infect. Drug Resist. 2021, 14, 609–611. [Google Scholar] [CrossRef] [PubMed]
- Kiymet, E.; Bonc, E.; Sahinkaya, S.; Cem, E.; Celebi, M.Y.; Dugzol, M.; Kara, A.A.; Otiken, K.; Arikan, K.O.; Aydin, T.; et al. Distribution of spreading viruses during COVID-19 pandemic: Effect of mitigation strategies. Am. J. Infect. Control 2021, 49, 1142–1145. [Google Scholar] [CrossRef] [PubMed]
- To, K.K.W.; Yip, C.C.Y.; Yuen, K.Y. Rhinovirus-from bench to bedside. Formos Med. Assoc. 2017, 116, 496–504. [Google Scholar] [CrossRef] [Green Version]
- Jacobs, S.E.; Lamson, D.; St George, K.; Walsh, T.J. Human rhinoviruses. Clin. Microbiol. Rev. 2013, 26, 135–162. [Google Scholar] [CrossRef] [Green Version]
- Liu, P.; Xu, M.; Cao, L.; Su, L.; Lu, L.; Dong, N.; Jia, R.; Zhu, X.; Xu, J. Impact of COVID-19 pandemic on the prevalence of respiratory viruses in children with lower respiratory tract infections in China. Virol. J. 2021, 18, 1–7. [Google Scholar] [CrossRef]
- Lai, C.C.; Wang, C.Y.; Hsueh, P.R. Co-infections among patients with COVID-19: The need for combination therapy with non-anti—SARS-CoV-2 agents? J. Microbiol. Immunol. Infect. 2020, 53, 505–512. [Google Scholar] [CrossRef]
- Hazra, A.; Collison, M.; Pisano, J.; Kumar, M.; Oehler, C.; Ridgway, J.P. Coinfections with SARS-CoV-2 and other respiratory pathogens. Infect. Control Hosp. Epidemiol. 2020, 41, 1228–1236. [Google Scholar] [CrossRef]
- Kim, K.W.; Deveson, I.W.; Pang, C.N.; Yeang, M.; Naingm, Z.; Adikari, T.; Hammond, J.M.; Stevanovski, I.; Beukers, A.G.; Verich, A.; et al. Respiratory viral co-infections among SARS-CoV-2 cases confirmed by virome capture sequencing. Sci. Rep. 2021, 11, 3934. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| January 2017–February 2020 (Pre-Pandemic) | March 2020–May 2021 (During Pandemic) | p | January 2017–February 2020 (Pre-Pandemic) | March 2020–May 2021 (During Pandemic) | p | |
|---|---|---|---|---|---|---|
| Samples tested (N°) | 10,121 | 2362 | ||||
| Positive (N°) | 1475 | 63 | ||||
| Frequency (%) | 14.6 | 2.7 | <0.0001 a | |||
| Total population tested | Positive population | |||||
| Demographic characteristics | ||||||
| Male, n (%) | 5098 (50.3) | 1341 (55.5) | <0.0001 | 878 (59.5) | 41 (65) | 0.4 |
| Mean Age | 65.1 | 63.5 | <0.0001 | 64.02 | 59.9 | 0.07 |
| Age in years, n (%) | ||||||
| 18–44 | 1355 (13.2) | 261 (11) | 0.002 | 240 (16.2) | 9 (14.2) | 0.86 |
| 45–64 | 3012 (29.7) | 940 (39.7) | <0.0001 | 414 (28) | 27 (42.8) | 0.01 |
| 65–79 | 3561 (35.1) | 838 (35.4) | 0.79 | 524 (35.5) | 24 (38) | 0.68 |
| ≥80 | 2193 (21.6) | 323 (13.6) | <0.0001 | 297 (20) | 3 (4.7) | 0.001 |
| January 2017–February 2020 (Pre-Pandemic) | March 2020–May 2021 (During Pandemic) | p | |
|---|---|---|---|
| Influenza A virus Test positivity number/total number tests (%) | 523/6881 (7.6) | 3/1628 (0.18) | <0.0001 a |
| Influenza B virus Test positivity number/total number tests (%) | 210/6881 (3) | 1/1628 (0.06) | <0.0001 |
| Respiratory syncytial virus Test positivity number/total number tests (%) | 238/3240 (7.3) | 10/734 (1.4) | <0.0001 |
| Metapneumovirus Test positivity number/total number tests (%) | 38/3240 (1.1) | 2/734 (0.27) | 0.04 |
| Adenovirus Test positivity number/total number tests (%) | 48/3240 (1.4) | 4/734 (0.6) | 0.08 |
| Parainfluenza viruses Test positivity number/total number tests (%) | 131/3240 (4) | 1/734 (0.14) | <0.0001 |
| Rhinovirus Test positivity number/total number tests (%) | 123/3240 (3.8) | 41/734 (5.6) | 0.02 |
| Coronaviruses Test positivity number /total number tests (%) | 164/3240 (5) | 1/734 (0.14) | <0.0001 |
| January 2017–February 2020 (Pre-Pandemic) | March 2020–May 2021 (During Pandemic) | |
|---|---|---|
| Virus detected | No. of patients | |
| RhV and RSV | 1 | 0 |
| PIV and RSV | 1 | 0 |
| Coronavirus and RSV | 2 | 0 |
| AdV and RSV | 1 | 0 |
| Coronavirus and PIV | 1 | 0 |
| FluA and RSV | 1 | 0 |
| FluA and Coronavirus | 2 | 0 |
| FluA, FluB and Coronavirus | 1 | 0 |
| FluB and RSV | 1 | 0 |
| FluA and PIV | 1 | 0 |
| SARS-CoV-2 and RhV | 0 | 6 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Francesco, M.A.; Pollara, C.; Gargiulo, F.; Giacomelli, M.; Caruso, A. Circulation of Respiratory Viruses in Hospitalized Adults before and during the COVID-19 Pandemic in Brescia, Italy: A Retrospective Study. Int. J. Environ. Res. Public Health 2021, 18, 9525. https://doi.org/10.3390/ijerph18189525
De Francesco MA, Pollara C, Gargiulo F, Giacomelli M, Caruso A. Circulation of Respiratory Viruses in Hospitalized Adults before and during the COVID-19 Pandemic in Brescia, Italy: A Retrospective Study. International Journal of Environmental Research and Public Health. 2021; 18(18):9525. https://doi.org/10.3390/ijerph18189525
Chicago/Turabian StyleDe Francesco, Maria Antonia, Caterina Pollara, Franco Gargiulo, Mauro Giacomelli, and Arnaldo Caruso. 2021. "Circulation of Respiratory Viruses in Hospitalized Adults before and during the COVID-19 Pandemic in Brescia, Italy: A Retrospective Study" International Journal of Environmental Research and Public Health 18, no. 18: 9525. https://doi.org/10.3390/ijerph18189525
APA StyleDe Francesco, M. A., Pollara, C., Gargiulo, F., Giacomelli, M., & Caruso, A. (2021). Circulation of Respiratory Viruses in Hospitalized Adults before and during the COVID-19 Pandemic in Brescia, Italy: A Retrospective Study. International Journal of Environmental Research and Public Health, 18(18), 9525. https://doi.org/10.3390/ijerph18189525