
Childhood Socioeconomic Position, Adult Educational Attainment and Health Behaviors: The Role of Psychological Capital and Health Literacy



Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Procedure and Measures
3. Results
3.1. Correlations
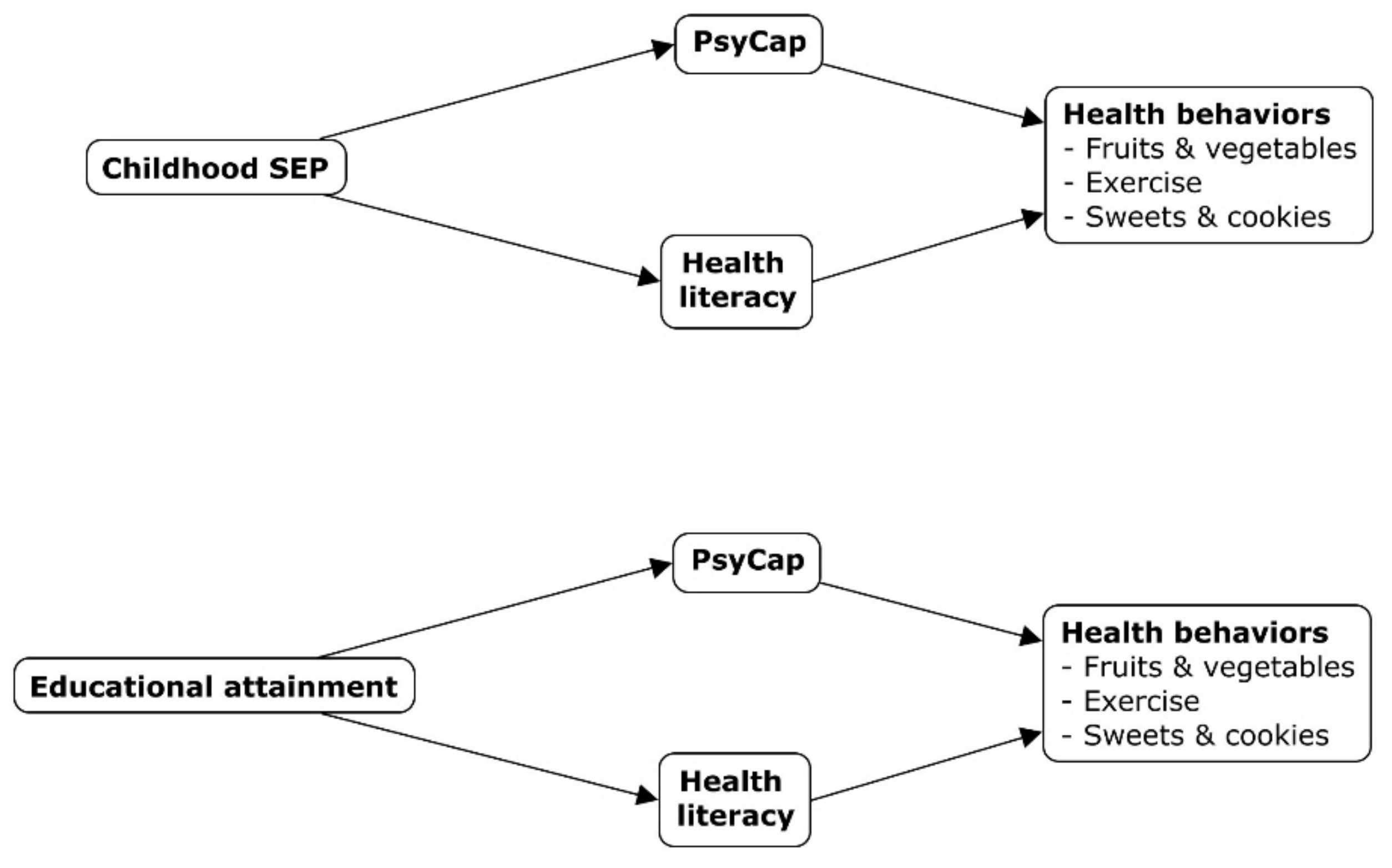
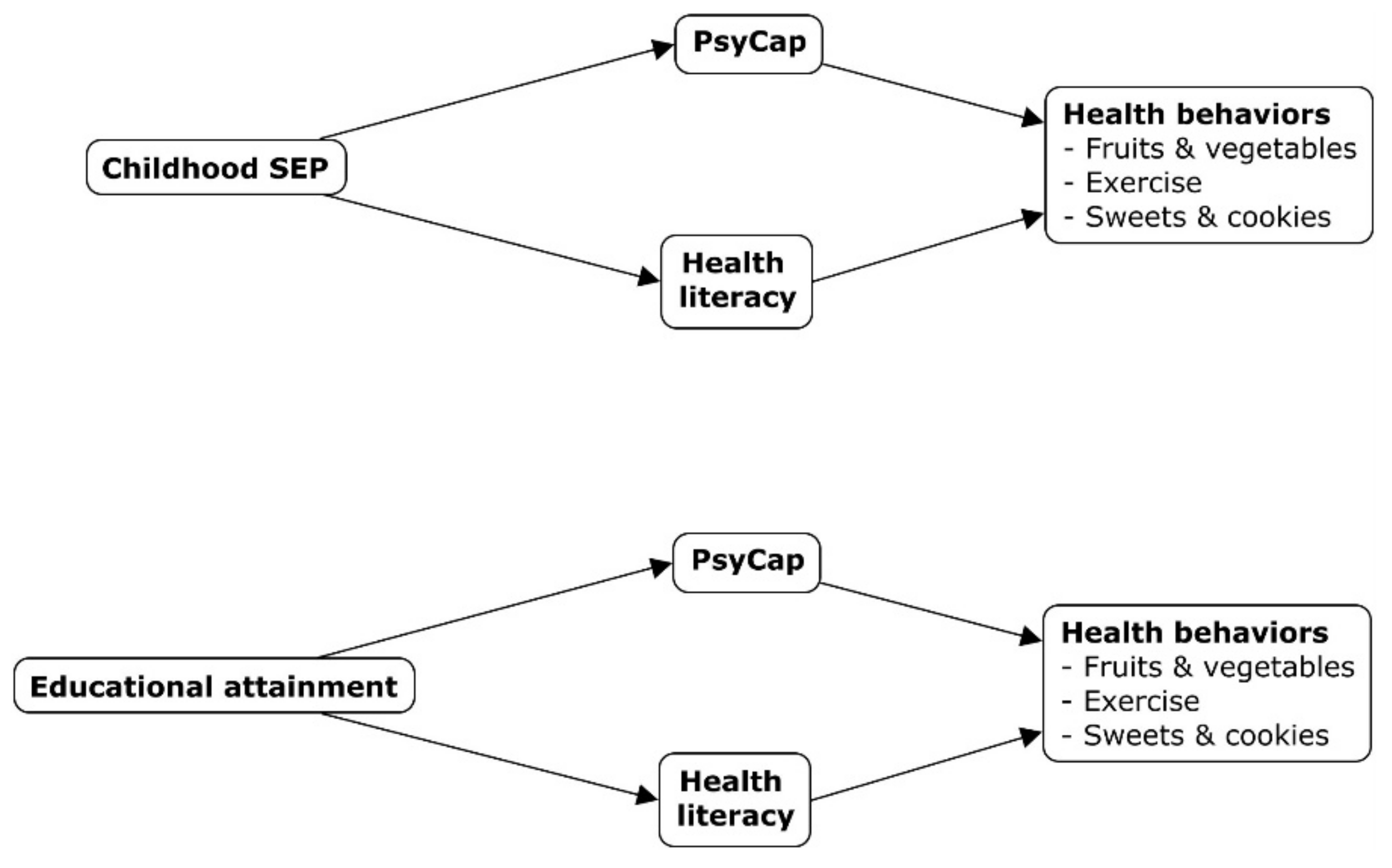
3.2. Mediation Analyses
3.2.1. Childhood SEP
Fruits and Vegetables
Exercise
Sweets and Cookies
3.2.2. Adult Educational Attainment
Fruits and Vegetables
Exercise
Sweets and Cookies Consumption
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Poulton, R.; Caspi, A.; Milne, B.J.; Thomson, W.M.; Taylor, A.; Sears, M.R.; Moffitt, T.E. Association between children’s experience of socioeconomic disadvantage and adult health: A life-course study. Lancet 2002, 360, 1640–1645. [Google Scholar] [CrossRef] [Green Version]
- Pollitt, R.A.; Kaufman, J.S.; Rose, K.M.; Diez-Roux, A.V.; Zeng, D.; Heiss, G. Early-life and adult socioeconomic status and inflammatory risk markers in adulthood. Eur. J. Epidemiol. 2007, 22, 55–66. [Google Scholar] [CrossRef]
- Giesinger, I.; Goldblatt, P.; Howden-Chapman, P.; Marmot, M.; Kuh, D.; Brunner, E. Association of socioeconomic position with smoking and mortality: The contribution of early life circumstances in the 1946 birth cohort. J. Epidemiol. Community Health 2014, 68, 275–279. [Google Scholar] [CrossRef] [Green Version]
- Vohra, J.; Marmot, M.G.; Bauld, L.; Hiatt, R.A. Socioeconomic position in childhood and cancer in adulthood: A rapid-review. J. Epidem. Community Health 2016, 6, 629–634. [Google Scholar] [CrossRef]
- Chaparro, M.P.; Koupil, I. The impact of parental educational trajectories on their adult offspring’s overweight/obesity status: A study of three generations of Swedish men and women. Soc. Sci. Med. 2014, 120, 199–207. [Google Scholar] [CrossRef] [PubMed]
- Galobardes, B.; Lynch, J.W.; Smith, G.D. Is the association between childhood socioeconomic circumstances and cause-specific mortality established? Update of a systematic review. J. Epidemiol. Comm. Health 2008, 62, 387–390. [Google Scholar] [CrossRef]
- Counts, C.J.; Grubin, F.C.; John-Henderson, N.A. Childhood socioeconomic status and risk in early family environments: Predictors of global sleep quality in college students. Sleep Health 2018, 4, 301–306. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Donoghue, G.; Kennedy, A.; Puggina, A.; Aleksovska, K.; Buck, C.; Burns, C.; Boccia, S. Socio-economic determinants of physical activity across the life course: A" DEterminants of DIet and Physical ACtivity"(DEDIPAC) umbrella literature review. PLoS ONE 2018, 13, e0190737. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Komulainen, K.; Mittleman, M.A.; Jokela, M.; Laitinen, T.T.; Pahkala, K.; Elovainio, M.; Pulkki-Råback, L. Socioeconomic position and intergenerational associations of ideal health behaviors. Eur. J. Prev. Card. 2019, 26, 1605–1612. [Google Scholar] [CrossRef] [PubMed]
- Puolakka, E.; Pahkala, K.; Laitinen, T.T.; Magnussen, C.G.; Hutri-Kähönen, N.; Männistö, S.; Juonala, M. Childhood socioeconomic status and lifetime health behaviors: The Young Finns Study. Int. J. Card. 2018, 258, 289–294. [Google Scholar] [CrossRef] [Green Version]
- Yanagi, N.; Hata, A.; Kondo, K.; Fujiwara, T. Association between childhood socioeconomic status and fruit and vegetable intake among older Japanese: The JAGES 2010 study. Prev. Med. 2018, 106, 130–136. [Google Scholar] [CrossRef]
- Hill, S.E.; Prokosch, M.L.; DelPriore, D.J.; Griskevicius, V.; Kramer, A. Low childhood socioeconomic status promotes eating in the absence of energy need. Psych. Sci. 2016, 27, 354–364. [Google Scholar] [CrossRef] [Green Version]
- Solís, C.B.; Fantin, R.; Castagné, R.; Lang, T.; Delpierre, C.; Kelly-Irving, M. Mediating pathways between parental socio-economic position and allostatic load in mid-life: Findings from the 1958 British birth cohort. Soc. Sci. Med. 2016, 165, 19–27. [Google Scholar] [CrossRef]
- Sheikh, M.A.; Abelsen, B.; Olsen, J.A. Clarifying associations between childhood adversity, social support, behavioral factors, and mental health, health, and well-being in adulthood: A population-based study. Front. Psych. 2016, 7, 727. [Google Scholar] [CrossRef]
- Gallo, L.C.; Bogart, L.M.; Vranceanu, A.M.; Matthews, K.A. Socioeconomic status, resources, psychological experiences, and emotional responses: A test of the reserve capacity model. J. Pers. Soc. Psych. 2005, 88, 386–399. [Google Scholar] [CrossRef] [Green Version]
- Schelleman-Offermans, K.; Massar, K. Explaining socioeconomic inequalities in self-reported health outcomes: The mediating role of perceived life stress, financial self-reliance, psychological capital, and time perspective orientations. PLoS ONE 2020, 15, e0243730. [Google Scholar] [CrossRef] [PubMed]
- Schöllgen, I.; Huxhold, O.; Schüz, B.; Tesch-Römer, C. Resources for health: Differential effects of optimistic self-beliefs and social support according to socioeconomic status. Health Psych. 2020, 30, 326–335. [Google Scholar] [CrossRef] [PubMed]
- Turiano, N.A.; Chapman, B.P.; Agrigoroaei, S.; Infurna, F.J.; Lachman, M. Perceived control reduces mortality risk at low, not high, education levels. Health Psych 2014, 33, 883–890. [Google Scholar] [CrossRef] [Green Version]
- Luthans, F.; Youssef, C.M.; Avolio, B.J. Psychol. Capital; Oxford University Press: New York, NY, USA, 2007. [Google Scholar]
- Non, A.L.; Román, J.C.; Clausing, E.S.; Gilman, S.E.; Loucks, E.B.; Buka, S.L.; Kubzansky, L.D. Optimism and social support predict healthier adult behaviors despite socially disadvantaged childhoods. Int. J. Behav. Med. 2020, 27, 200–212. [Google Scholar] [CrossRef] [PubMed]
- Perna, L.; Mielck, A.; Lacruz, M.E.; Emeny, R.T.; Holle, R.; Breitfelder, A.; Ladwig, K.H. Socioeconomic position, resilience, and health behaviour among elderly people. Int. J. Public Health 2012, 57, 341–349. [Google Scholar] [CrossRef]
- Luthans, F.; Youssef, C.M.; Sweetman, D.S.; Harms, P.D. Meeting the leadership challenge of employee well-being through relationship PsyCap and health PsyCap. J. Leadersh. Org. Stud. 2013, 20, 118–133. [Google Scholar] [CrossRef]
- De Buhr, E.; Tannen, A. Parental health literacy and health knowledge, behaviours and outcomes in children: A cross-sectional survey. BMC Public Health 2020, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Bostock, S.; Steptoe, A. Association between low functional health literacy and mortality in older adults: Longitudinal cohort study. BMJ 2012, 344, e1602. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lastrucci, V.; Lorini, C.; Caini, S.; Florence Health Literacy Research Group; Bonaccorsi, G. Health literacy as a mediator of the relationship between socioeconomic status and health: A cross-sectional study in a population-based sample in Florence. PLoS ONE 2019, 14, e0227007. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Friis, K.; Lasgaard, M.; Rowlands, G.; Osborne, R.H.; Maindal, H.T. Health literacy mediates the relationship between educational attainment and health behavior: A Danish population-based study. J. Health Comm. 2016, 21, 54–60. [Google Scholar] [CrossRef]
- Luthans, F.; Avey, J.B.; Avolio, B.J.; Norman, S.M.; Combs, G.J. Psychological capital development: Toward a micro-intervention. J. Organ. Beh. 2006, 27, 387–393. [Google Scholar] [CrossRef] [Green Version]
- Dello Russo, S.; Stoykova, P. Psychological capital intervention (PCI): A replication and extension. Hum. Resour. Dev. Quart. 2015, 26, 329–347. [Google Scholar] [CrossRef] [Green Version]
- Walters, R.; Leslie, S.J.; Polson, R.; Cusack, T.; Gorely, T. Establishing the efficacy of interventions to improve health literacy and health behaviours: A systematic review. BMC Public Health 2020, 20, 1–17. [Google Scholar] [CrossRef]
- Faul, F.; Erdfelder, E.; Buchner, A.; Lang, A.G. Statistical power analyses using G*Power 3.1: Tests for correlation and regression analyses. Beh. Res. Meth. 2009, 41, 1149–1160. [Google Scholar] [CrossRef] [Green Version]
- Sørensen, K.; Van den Broucke, S.; Pelikan, J.M.; Fullam, J.; Doyle, G.; Slonska, Z.; Brand, H. Measuring health literacy in populations: Illuminating the design and development process of the European Health Literacy Survey Questionnaire (HLS-EU-Q). BMC Public Health 2013, 13, 1–10. [Google Scholar] [CrossRef] [Green Version]
- Lorenz, T.; Beer, C.; Pütz, J.; Heinitz, K. Measuring psychological capital: Construction and validation of the compound PsyCap scale (CPC-12). PLoS ONE 2016, 11, e0152892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayes, A.F. Beyond Baron and Kenny: Statistical mediation analysis in the new millennium. Comm. Monographs 2009, 76, 408–420. [Google Scholar] [CrossRef]
- Zhao, X.; Lynch Jr, J.G.; Chen, Q. Reconsidering Baron and Kenny: Myths and truths about mediation analysis. J. Consum. Res. 2010, 37, 197–206. [Google Scholar] [CrossRef]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach, 2nd ed.; Guilford Publications: New York, NY, USA, 2018. [Google Scholar]
- Kasprzak, C.M.; Sauer, H.A.; Schoonover, J.J.; Lapp, M.M.; Leone, L.A. Barriers and facilitators to fruit and vegetable consumption among lower-income families: Matching preferences with stakeholder resources. J. Hunger. Env. Nutr. 2021, 16, 490–508. [Google Scholar] [CrossRef]
- Riolli, L.; Savicki, V.; Richards, J. Psychological capital as a buffer to student stress. Psychology 2012, 3, 1202–1207. [Google Scholar] [CrossRef] [Green Version]
- Quaglio, G.; Sørensen, K.; Rübig, P.; Bertinato, L.; Brand, H.; Karapiperis, T.; Dario, C. Accelerating the health literacy agenda in Europe. Health Prom.Int. 2017, 32, 1074–1080. [Google Scholar] [CrossRef]
- Paakkari, L.; Torppa, M.; Mazur, J.; Boberova, Z.; Sudeck, G.; Kalman, M.; Paakkari, O. A Comparative Study on Adolescents’ Health Literacy in Europe: Findings from the HBSC Study. Int. J. Environ. Res. Public Health 2020, 17, 3543. [Google Scholar] [CrossRef]
- Rew, L.; Powell, T.; Brown, A.; Becker, H.; Slesnick, N. An intervention to enhance psychological capital and health outcomes in homeless female youths. West. J. Nurs. Res. 2017, 39, 356–373. [Google Scholar] [CrossRef]
- Rabenu, E.; Yaniv, E.; Elizur, D. The relationship between psychological capital, coping with stress, well-being, and performance. Curr. Psych. 2017, 36, 875–887. [Google Scholar] [CrossRef]
- McKenzie, S.K.; Carter, K.N. Are retrospective measures of childhood socioeconomic position in prospective adult health surveys useful? Australas. Epidemiol. 2009, 16, 22–24. [Google Scholar] [CrossRef]
- Quon, E.C.; McGrath, J.J. Subjective socioeconomic status and adolescent health: A meta-analysis. Health Psychol. 2014, 33, 433–447. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fernandez-Jimenez, R.; Al-Kazaz, M.; Jaslow, R.; Carvajal, I.; Fuster, V. Children present a window of opportunity for promoting health: JACC review topic of the week. J. Am. Coll. Card. 2018, 72, 3310–3319. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variable | Mean (SD) | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 |
|---|---|---|---|---|---|---|---|---|---|---|
| 1. Childh. SEP | 3.49 (0.94) | -- | ||||||||
| 2. Health lit. | 5.30 (0.80) | 0.12 | ||||||||
| 3. PsyCap | 5.43 (0.80) | 0.20 * | 0.52 ** | |||||||
| 4. Fruit/veg. | 4.36 (2.38) | 0.11 | 0.04 | 0.21 * | ||||||
| 5. Exercise | 4.23 (2.06) | 0.06 | 0.27 ** | 0.32 ** | 0.26 ** | |||||
| 6. Cookies | 4.32 (2.07) | −0.04 | −0.19 * | −0.15 | −0.07 | −0.20 * | ||||
| 7. Age | 34.98 (13.58) | −0.19 * | 0.08 | 0.18 * | −0.18 * | 0.07 | 0.07 | |||
| 8. Gender | -- | 0.04 | −0.10 | −0.17 * | 0.15 | −0.09 | 0.22 ** | −0.16 | ||
| 9. BMI | 24.25 (4.19) | −0.07 | 0.004 | 0.01 | −0.18 * | −0.19 * | 0.004 | 0.32 ** | −0.29 ** | |
| 10. Adult Educ. | -- | 0.04 | 0.25 ** | 0.20 * | 0.11 | 0.18 * | 0.002 | −0.02 | −0.11 | −0.16 |
| DirectEffect a | Adjusted Direct Effect b | R2 | Mediator(s) | Indirect Effect c | Indirect Effect 95% CI d | |
|---|---|---|---|---|---|---|
| Childhood SEP | ||||||
| Fruits and vegetables | 0.18 | 0.03 | 0.13 | PsyCap | 0.14 | 0.014 to 0.307 |
| Health literacy | −0.04 | −0.162 to 0.029 | ||||
| Health literacy and PsyCap | 0.05 | −0.013 to 0.135 | ||||
| Exercise | 0.11 | −0.07 | 0.17 | PsyCap | 0.10 | 0.006 to 0.216 |
| Health literacy | 0.04 | −0.022 to 0.152 | ||||
| Health literacy and PsyCap | 0.04 | −0.010 to 0.111 | ||||
| Sweets and cookies | −0.08 | −0.003 | 0.09 | PsyCap | −0.03 | −0.113 to 0.051 |
| Health literacy | −0.04 | −0.158 to 0.027 | ||||
| Health literacy and PsyCap | −0.01 | −0.056 to 0.018 | ||||
| Adult Education | ||||||
| Fruits and vegetables | 0.21 | 0.15 | 0.13 | PsyCap | 0.04 | −0.056 to 0.177 |
| Health literacy | −0.06 | −0.176 to 0.046 | ||||
| Health literacy and PsyCap | 0.08 | 0.017 to 0.176 | ||||
| Exercise | 0.27 | 0.13 | 0.17 | PsyCap | 0.03 | −0.044 to 0.122 |
| Health literacy | 0.06 | −0.028 to 0.175 | ||||
| Health literacy and PsyCap | 0.06 | 0.006 to 0.135 | ||||
| Sweets and cookies | 0.07 | 0.17 | 0.09 | PsyCap | −0.009 | −0.061 to 0.025 |
| Health literacy | −0.07 | −0.224 to 0.028 | ||||
| Health literacy and PsyCap | −0.02 | −0.069 to 0.026 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Massar, K.; Kopplin, N.; Schelleman-Offermans, K. Childhood Socioeconomic Position, Adult Educational Attainment and Health Behaviors: The Role of Psychological Capital and Health Literacy. Int. J. Environ. Res. Public Health 2021, 18, 9399. https://doi.org/10.3390/ijerph18179399
Massar K, Kopplin N, Schelleman-Offermans K. Childhood Socioeconomic Position, Adult Educational Attainment and Health Behaviors: The Role of Psychological Capital and Health Literacy. International Journal of Environmental Research and Public Health. 2021; 18(17):9399. https://doi.org/10.3390/ijerph18179399
Chicago/Turabian StyleMassar, Karlijn, Natalie Kopplin, and Karen Schelleman-Offermans. 2021. "Childhood Socioeconomic Position, Adult Educational Attainment and Health Behaviors: The Role of Psychological Capital and Health Literacy" International Journal of Environmental Research and Public Health 18, no. 17: 9399. https://doi.org/10.3390/ijerph18179399
APA StyleMassar, K., Kopplin, N., & Schelleman-Offermans, K. (2021). Childhood Socioeconomic Position, Adult Educational Attainment and Health Behaviors: The Role of Psychological Capital and Health Literacy. International Journal of Environmental Research and Public Health, 18(17), 9399. https://doi.org/10.3390/ijerph18179399