
Improving the Sexual Health of Young People (under 25) in High-Risk Populations: A Systematic Review of Behavioural and Psychosocial Interventions

 ,
, 
 and
and 
Abstract
:1. Introduction
2. Methods
2.1. Search Strategy
2.2. Inclusion Criteria
- Were a randomized controlled trial with ≥2 arms;
- Reported sufficient data to satisfy PRISMA and Cochrane guidelines for inclusion in the review;
- Were published in English.
- The primary aim of the study was not to address sexual health;
- There was a later publication of results from the same trial—the paper reporting the longest follow-up data was chosen.
2.3. Data Retrieval
2.4. Data Screening
2.5. Data Extraction
2.6. Quality Assessment of Interventions
3. Results
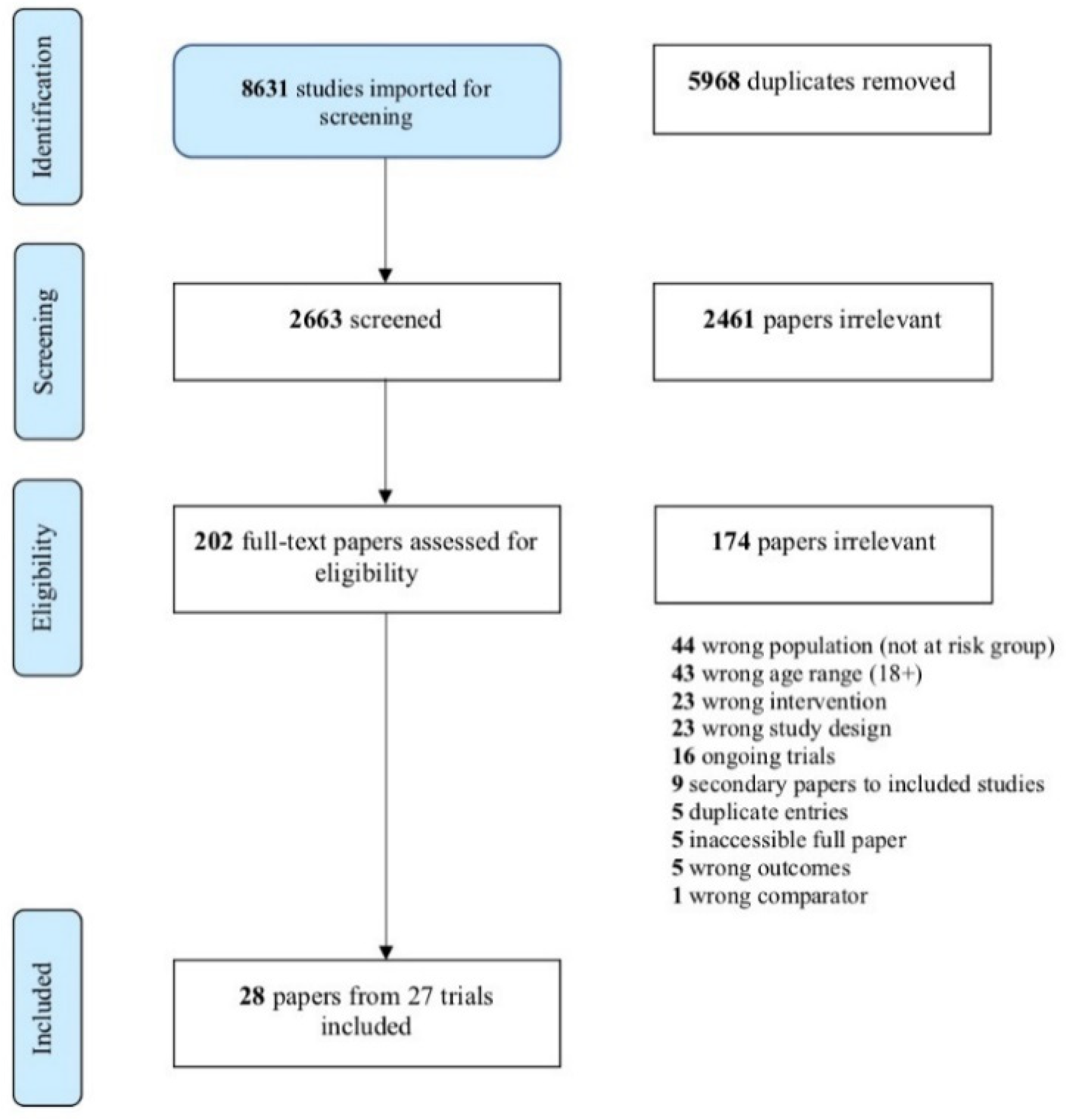
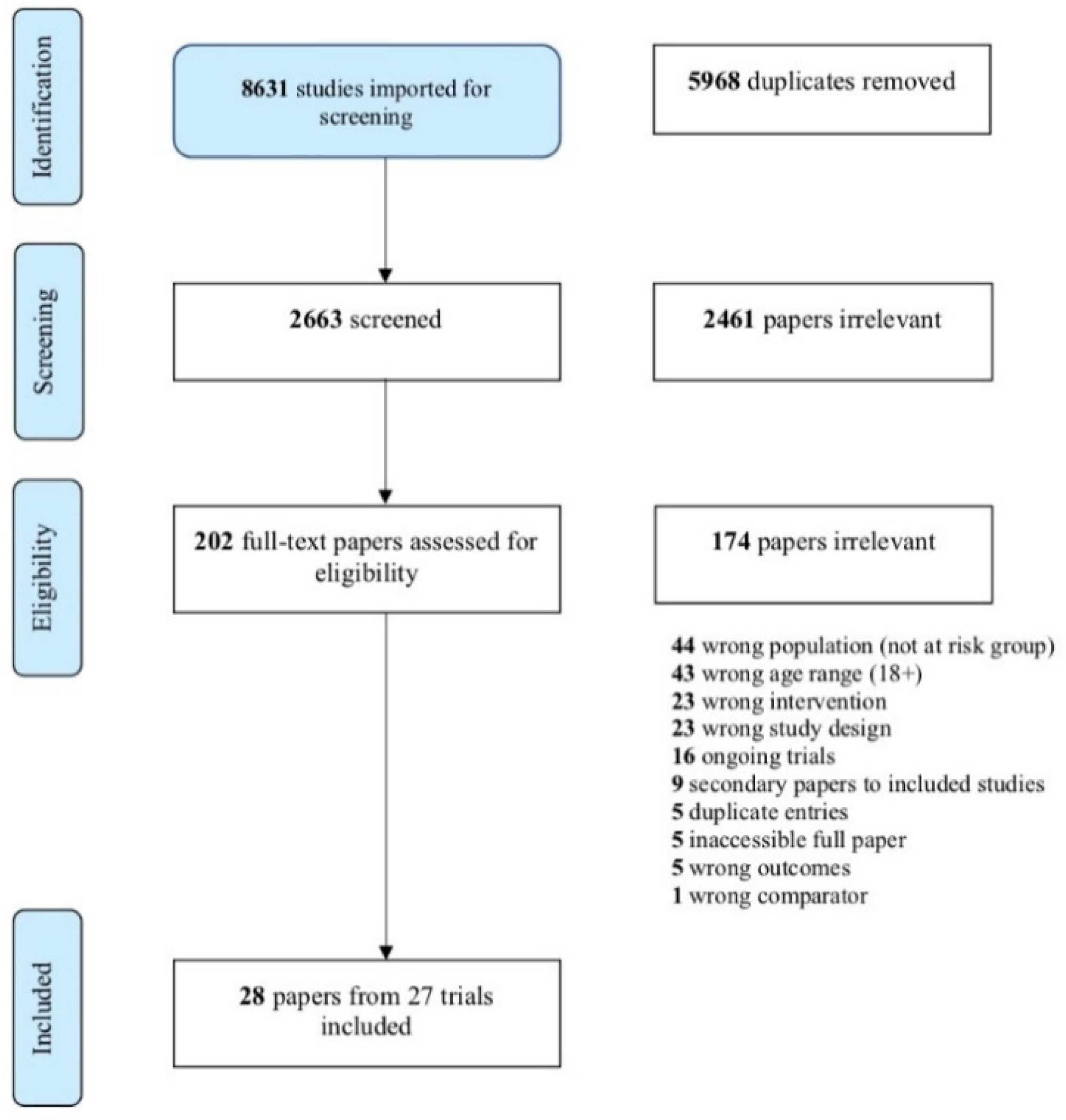
3.1. Search Results
3.2. Included Trials
3.2.1. Alcohol and Other Drug (AOD) Use
3.2.2. Ethnic Minorities
3.2.3. Homelessness
3.2.4. Justice-Involved Youth
3.2.5. LGBTQI+ (Including YMSM)
3.2.6. Mental Ill-Health
3.2.7. Out-of-Home Care
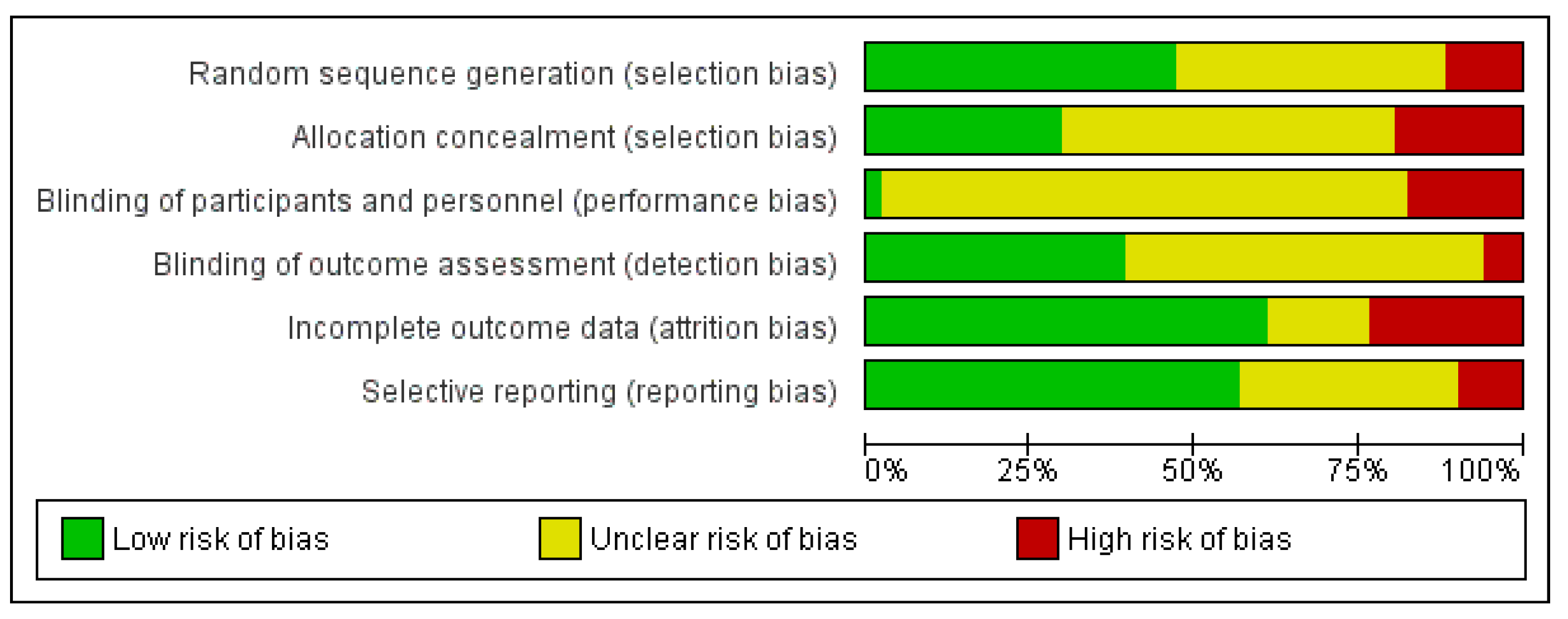
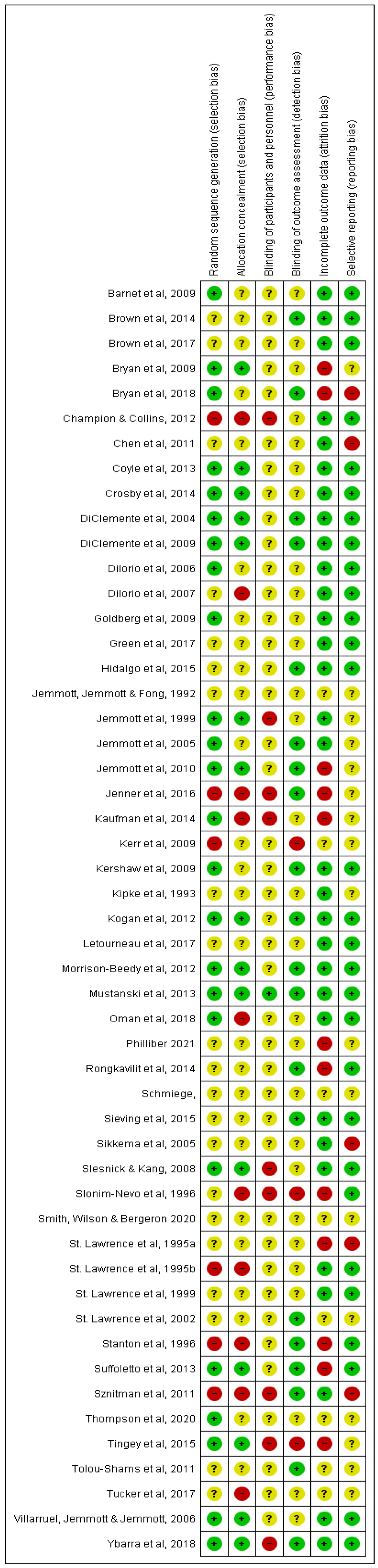
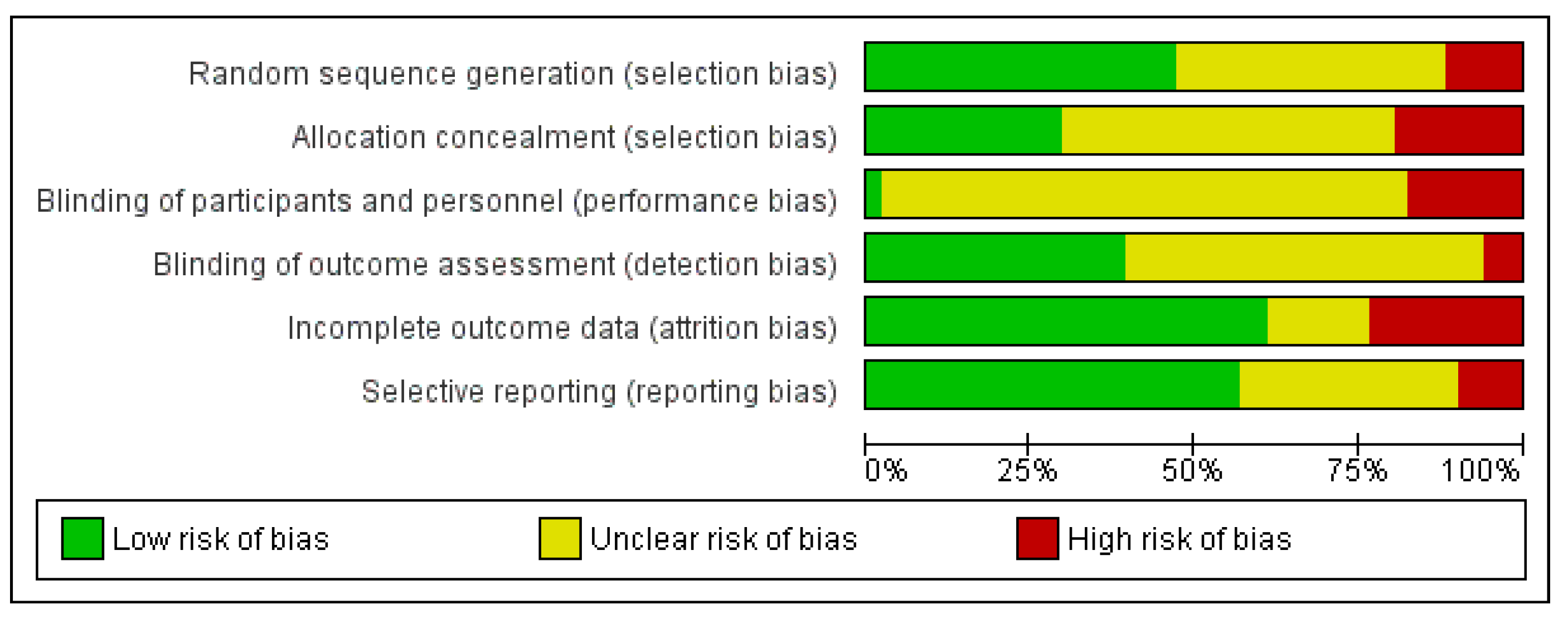
3.3. Quality Assessment
4. Discussion
4.1. Implications and Applicability
4.2. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
| Study | Study Population | Age Range (Years) | Setting | N Randomised (INTV vs. C) | Follow Up Period (Months) | Intervention (s) | Dose | Control | Sexual Health Outcomes | Outcome for Active vs. Control |
|---|---|---|---|---|---|---|---|---|---|---|
| AOD Use | ||||||||||
| Letourneau et al., 2017; USA | AOD use; justice-involved youth | 11–17 | Outpatient clinics | 107 (45 vs. 62) | 3, 6, 9, 12 | Family-focussed risk-reduction intervention for SUD and sexual health (Risk Reduction Therapy for Adolescents) combined with contingency management | 24 × weekly sessions (60–90 min each) delivered over 6–7 months | Usual care | B: Condom use, sex after substance use, HIV risk behaviours | B: No significant findings for any sexual health outcomes. |
| St. Lawrence, et al. 1995(b); Jackson, MS, USA | AOD use | 13–17 | Residential drug treatment facility | 34 (17 vs. 17) | None | Behaviour skills training HIV risk reduction | 6 × 90 min group sessions | Risk education-only control | K + A: AIDS knowledge test, attitudes towards HIV prevention, condom attitudes. B: Sexual risk behaviours over 2 months pre and post intervention | K + A: Post-INTV, INTV group had better AIDS knowledge (p = 0.01), attitudes towards HIV prevention (p = 0.05) and attitudes towards condom (p = 0.05). B: Post-INTV, INTV group less likely to engage in sexual risk behaviours than C, including coercions into unwanted sexual activity, exchange sex for money or drugs, and engaging in casual sex (all, p < 0.05). |
| St Lawrence et al., 2002; MS, USA | AOD use | Mean = 16 (full range not reported) | Residential drug treatment facilities | 161 (Group sizes not reported.) | 6, 12 | Sexual health information plus behavioural skills training (I+B), or information plus skills training plus risk-sensitization motivational component (I+B+M). | 3 × 90 min sessions/week, for 4 weeks. | Sexual health information-only control | K + A: AIDS risk knowledge test, condom attitudes, attitudes toward HIV prevention, self-efficacy and perceived risk. B: Social skill and anger management skill acquisition, self-reported sexual behaviour (unprotected vaginal, oral and anal intercourse; number of partners). | K + A: Significant group x time interactions for AIDS knowledge, attitudes towards prevention and condom attitudes (all, p < 0.05), and for perceived risk (p < 0.01). B: Significant group x time interactions for number of sex partners, unprotected sex frequency, condom use frequency, %age of condom use, (all p < 0.05). |
| Suffoletto et al., 2013; PA, USA | AOD use (females) | 18–25 | Hospital emergency department | 52 (23 vs. 29) | 3 | Sexual risk reduction intervention delivered via text message. | A series of interactive messages delivered weekly for 12 weeks. | Health behaviour survey with weekly text message reminders (non-interactive). | B: Condom use, condom use frequency, abstinence, AOD use, AOD use prior to sex | All results ns. |
| Ethnic Minorities | ||||||||||
| Kipke, Boyer and Hein, 1993; New York, NY, USA | Ethnic minority (Latino and African-American) | 12–16 | Community-based agencies | 87 (41 vs. 46) | none | HIV prevention skills training (ARREST) | 3 × 90 min group sessions | Wait-list control | K + A: HIV knowledge, perception of risk B: Risky sexual behaviours, frequency of sex acts SW: assertiveness and communication skills | K + A: Post-INTV, INTV group had greater HIV knowledge (p < 0.001), perception of risk (p < 0.01), decreased negative attitudes about HIV (p < 0.05) B: ns SW: ability to refuse high-risk (p < 0.001) and propose low-risk behavioural alternatives (p< 0.001). |
| Smith et al., 2020; Texas, USA | Ethnic minority (Hispanic, female) teenage mothers | 15–18 | In-home | 84 (42 vs. 42) | 12 | In-home postpartum educational support plus case management services, plus: in-home and group parenting education, life skills groups, and teen leadership council activities. | Educational support for 4 h/week for 6 weeks, plus biweekly 90 min face-to-face support worker meetings. | In-home postpartum educational support plus case management services. | B: Condom use to prevent pregnancy, condom use to prevent STIs | B: Both groups improved condom use over time (OR 3.21). No significant differences between INTV and C. |
| Tingey et al., 2015; USA | Ethnic minority (American Indian) | 13–19 | Basketball camp in reservation-based community | 267 (138 vs. 129) | 6, 12 | Culturally-sensitive HIV risk reduction education and behavioural skills training | 8 structured lessons delivered to peer groups of 8–10 participants of the same sex and age, 90 min/day. | 8 structured sessions of non-HIV educational control delivered in a large group setting (~50 participants) of mixed sex/age | K + A: Condom use self-efficacy, knowledge regarding prevention and transmission of HIV/AIDS Intent to use a condom | K + A: INTV group better condom use self-efficacy post-camp (p < 0.005), 6 m (p < 0.005) and 12 m (p < 0.05); higher knowledge regarding prevention and transmission of HIV/AIDS post-camp (p < 0.01), 6 m (p < 0.01), at 12 m ns; more likely to intend to use a condom at next sex post-camp (p < 0.01), 6 m and 12 ns. |
| Villarruel, Jemmott and Jemmott, 2006; Philadelphia, USA | Ethnic minority (Latino American) | 13–18 | Schools | 656 (312 vs. 344) | 3, 6, 12 | Culturally sensitive HIV prevention intervention (¡Cuídate!) | 2 × 4 h group sessions on 2 consecutive Saturdays | Generic health-promotion control delivered in same format at INTV | B: self-report measures of sexual activity (frequency, multiple partners, unprotected intercourse) and condom use (consistency, use at last intercourse) | B: Across follow-ups, INTV were less likely to report sexual intercourse (OR 0.66), multiple partners (OR 0.53), and days of unprotected intercourse (RR 0.47) and more likely to report using condoms consistently (OR, 1.91). Condom use at last sex = ns |
| Homeless | ||||||||||
| Slesnick and Kang, 2007; USA | Homeless; AOD | 14–22 | Drop-in centre for homeless youth | 180 (96 vs. 84) | 3, 6 | Community reinforcement approach therapy + HIV education and skills training (later developed from BART) | 12 × 50 min therapy sessions + 4 × 50 min HIV education/skills practice sessions, offered concurrently | TAU at the ‘drop in centre’ | B: ‘Health Risk questionnaire’ including freq. of condom use, no. sexual partners, frequency of intercourse | B: Post hoc analysis revealed younger youths in INTV group had more frequent usage of condoms than the older youths control (p < 0.01). Other outcomes ns |
| Thompson et al., 2020; North-eastern USA | Homeless; AOD | 18–21 | Inner-city crisis shelter | 40 (20 vs. 20) | 2 weeks | Educational, behaviour-tracking smartphone app plus brief motivational intervention | Brief daily app use 1/day for 28 days, plus two counselling sessions to discuss risk behaviours and set goals | TAU | B: Frequency of unprotected sex, freq. of drug use prior to sex, freq. of alcohol prior to sex. | B: At FU, INTV group had fewer episodes of unprotected sex than C, p = 0.01, and fewer episodes of sex after drug use, p = 0.02. |
| Tucker et al., 2017; Los Angeles, CA, USA | Homeless; AOD; ethnic minority | 18–25 | Drop-in centres for homeless youth | 200 (100 vs. 100) | 3 | Group-based MI intervention to reduce risky sexual behaviour and substance use (AWARE) | 4 × 45 min groups | TAU | K + A: Condom use self-efficacy, motivation to change condom use B: Number of sex partners and proportion of unprotected sex | K + A: Both outcomes ns. B: Among those with multiple sex partners, INTV = sig decrease in proportion of unprotected sexual events (p < 0.05), other outcomes ns |
| Justice-Involved Youth | ||||||||||
| Bryan et al., 2018; New Mexico, USA | Justice-involved youth; AOD | 14–18 | Short-term youth detention facility | 460 (162 vs. 155 vs. 143) | 12 | Sexual risk reduction plus alcohol and cannabis content (SRRI + ETOH + THC) and SRRI plus alcohol content (SRRI + ETOH) vs. SSRI only | 1 × 3 hr groups, up to 6 same sex participants. 2 hrs intervention, 1 hr for assessments. Based on ‘motivational enhancement therapy’. | SRRI only | B: Condom use, risky sexual behaviour Bio: STI incidence | B: Not reported. Bio: Lower incidence of STI diagnosis at FU in SRRI + ETOH + THC (3.9%) vs. SRRI + ETOH (10.2%; OR = 0.29) and vs. SRRI (12%; OR = 0.36) |
| Bryan, Schmiege, and Broaddus 2009; Denver, CO USA | Justice-involved youth; AOD | 14–17 | Short-term youth detention facility | 484 (165 vs. 157 vs. 162) | 3, 6, 9, 12 | Sexual and alcohol risk reduction psychosocial intervention (GPI) or GPI + motivational enhancement therapy (GMET) | 1 × 3–4 hr group, same gender | HIV/STI prevention information-only control (GINFO) (1 hr) | B: Condom use, frequency of intercourse while drinking | B: At 3, 6 and 9 month FUs, INTV groups mitigated tendency to decrease condom use over time compared with C, p < 0.01. Other findings ns. |
| Goldberg et al., 2009; Ontario, Canada | Justice-involved youth | 12–18 | Young offender secure custody facilities | 391 | 3, 6 | HIV risk reduction education intervention, or same intervention plus booster session | 6 × 1 h sessions over a 3-week period; or same dose plus one booster session 3 months post intervention | TAU + condensed HIV education session at trial conclusion. | K + A: Attitudes toward HIV prevention, risk behaviour knowledge, condom attitudes, safety behaviour self-efficacy B: Condom use | K + A: At 6 months, males in both INTV groups had increased HIV knowledge (p < 0.001). Females in INTV groups had increased condom attitude scores (p = 0.004). Males in booster group had increased prevention attitude scores (p = 0.017). B: Females in booster INTV group were more likely to use condoms consistently (OR = 4.20) |
| Kerr, Leve and Chamberlain, 2009; OR, USA | Justice-involved youth (female) | 13–17 | Foster care homes | 166 (81 vs. 85) | 24 | Multidimensional Treatment Foster Care–included a component that targeted HIV-risk behaviours | Ongoing elements throughout time in MTFC | TAU-Group care control | B: Pregnancy | B: Odds of pregnancy during FU were 2.44 times greater for C than INTV (p < 0.01) |
| St. Lawrence et al., 1999; Southern USA | Justice-involved youth (male) | Mean 15.8 | State reformatory | 361 (180 vs. 181) | 6 (after release) | sexual risk reduction skills-training-Becoming a Responsible Teen (BART) | 6 × 60 min group sessions, 8–10 participants, twice weekly | Anger management control, 6 sessions | K + A: AIDS knowledge, condom use self-efficacy, condom attitudes scale B: condom skills, %age of unprotected sex | K + A: Post-intervention, INTV = sig higher levels of AIDS knowledge (p < 0.001), condom use self-efficacy (p = 0.01), and positive attitudes about condoms (p = 0.001). B: INTV = sig better condom-use skills (p < 0.005) at post-intervention. Ns Sexual behaviours between groups at FU. |
| Tolou-Shams et al., 2011; North Eastern USA | Justice-involved youth; AOD | 12–18 | Juvenile drug courts | 57 (29 vs. 28) | 3 | Group-based HIV prevention and sexual risk reduction with affect management, Parents and Teens for Health (PATH) Program | 5 × 2 h sessions, delivered weekly, five participants per group | Time and attention-matched general health promotion | K + A: Condom use self-efficacy, attitudes towards condoms, partner communication re: condom use B: Condom use at last intercourse, number of partners, sexual activity in past 90 days, substance use during sex, HIV testing | All results ns. |
| LGBTQI+ (YMSM) | ||||||||||
| Chen, et al., 2011; Multi-site USA | YMSM; HIV+ | 16–24 | HIV clinics | 142 (71 vs. 71) | 6, 9, 12, 15 | Individual MI-based intervention targeting sexual risk behaviour (Healthy Choices) | 4 × sessions, delivered weekly | TAU | B: Condom use | B: Over all FU visits, INTV Ps reported increased likelihood of using condoms (p < 0.001) |
| Hidalgo et al., 2015; Chicago, IL, USA | YMSM | 16–20 | LGBT community health centre | 101 (58 vs. 43) | 1.5, 3 | Group-based, interactive HIV and sexual risk reduction skills training (MyPEEPS) | 6 × 2 h group sessions, 2 × week over 3 weeks in groups of 5–10 participants | Group-based, non-interactive sexual health information | K + A: Self-efficacy for safer sex, health-related partner verbal communication, internalised homophobia, B: Number of sex partners, number of unprotected anal sex partners, freq. of unprotected sex (anal and oral), sex acts under the influence of AOD, unprotected anal sex with AOD, condom errors | K + A: All ns. B: INTV Ps less likely to engage in sex under the influence of AOD, p = 0.05. Other findings ns |
| Mustanski et al., 2013; Chicago, IL, USA | YMSM; ethnic minority | 18–24 | Online | 102 (50 vs. 52) | 3 | Interactive online HIV prevention intervention (Keep It Up!) | 7 modules in total to complete undertaken in 3 × ~2 h blocks, spaced at least 24 h apart. | online didactic HIV knowledge | K + A: HIV knowledge, attitudes to HIV risk and prevention B: Frequency of unprotected sex acts, condom errors and problems | K + A: All ns. B: At FU, INTV had fewer unprotected sex acts than C (p = 0.04). Other findings ns. |
| Philliber, 2021; USA | LGBTQ and questioning youth | 14–22 | Schools, communit-based organisations, conferences | 1401 (551 vs. 515) | 12 | Educational workshop with info on health disparities, role play, safe-sex practices, healthcare self-efficacy and patient rights. | 1 × 3-h session | Time-mateched control activity unrelated to sexual health | K + A: Sexual health knowledge, self-efficacy to advocate for relevant health care B: Incidence of unprotected vaginal, oral and/or anal sex; sexual healthcare participation | K + A: INTV group scored higher on sexual health knowledge (p < 0.001), on self-efficacy generally (p = 0.007) and on self-efficacy to advocate for relevant healthcare, p = 0.02. B: At 12 mo FU, fewer INTV group participants had condomless vaginal sex in previous 3 months than control (p = 0.02) and reported fewer incidents of condomless vaginal sex (p = 0.01). |
| Rongkavilit et al., 2015; Bangkok, Thailand | YMSM; HIV+ | 16–25 | HIV/AIDS Research Centre | 74 (37 vs. 37) | 1, 6 | Individual MI-based counselling to reduce risky sex behaviour and either alcohol use or medication adherence (Healthy Choices) | 4 × weekly sessions | Time-matched general health control | B: Condom use, frequency of anal sex, sex with HIV- or unknown partners | B: At 6 mo: Fewer INTV group had engaged in anal sex in the preceding month than C (38% vs. 65%; p = 0.04) Fewer INTV had engaged in sex with a HIV- or unknown status partner than C (26% vs. 62%; p < 0.01). Other findings ns. |
| Ybarra et al., 2018; USA | YMSM | 14–18 | Text messaging | 302 (150 vs. 152) | 3 | HIV Preventative Program based on ‘Guy2Guy’, delivered by text messages. | 5 × weeks of daily text messages (8–10 a day) + booster week of messages 6 weeks after end | Time-matched general health control | B: Primary-number condomless sex acts. Secondary-rates of abstinence (for those sexually inexperienced), rates of getting an HIV test. | B: Primary = ns Youths in INTV group who were sexually experienced at baseline were sig more likely to report getting an HIV test at FU. (55% vs. 28%, p < 0.001). |
| Mental Ill-Health | ||||||||||
| Brown et al., 2014; Multi-site USA | Mental-ill health | 13–18 | Mental health clinics | 721 (227 vs. 259 vs. 235) | 3 | Family-based HIV prevention vs. adolescent only HIV prevention (Project STYLE) | 1 × 8-h group workshop of 4–8 participants, family intervention adolescent and caregiver attended together vs. adolescent only. | General health promotion intervention delivered in same format at INTV | K + A: HIV knowledge, self-efficacy to practise safe sex, B: Sexual activity, condom use, number of partners SW: openness of sex communication with parents | K + A: At FU, family INTV parents had greater HIV knowledge (p < 0.01) than C. B: At FU, INTV groups more likely to use condoms 100% (p = 0.04), more likely to avoid sex (p = 0.05), had fewer incidences of unprotected sex and a greater percentage of protected sex (p = 0.01) than C. SW: Family INTV improved parent-teen sexual communication (p < 0.01). |
| Brown et al., 2017; Chicago IL, Providence RI, USA | Mental ill-health–high school students with emotional or behavioural problems | 13–19 | School | 377 (128 vs. 130 vs. 119) | 6 | HIV prevention plus affect management (AM) vs. skills-based HIV prevention (SB) | 12 × 45 min sessions, delivered once or twice per week in mixed gender groups. | General health promotion (HP) intervention delivered in same format at INTV | K + A: HIV knowledge, condom attitudes B: Sexual activity, condom use, intercourse with concurrent substance use | K + A: At FU, HIV knowledge and condom attitudes were both sig better in AM or SB (p < 0.05) than C. B: At FU, sexual activity sig lower in AM vs. C (OR = 0.28), but SB vs. C ns. Condom use more consistent in AM vs. C (OR = 3.42), SB vs. C ns. Substance use ns. |
| Out-of-Home Care | ||||||||||
| Green et al., 2017; CA, MD and OK, USA | Out-of-home care; justice-involved youth | 13–18 | Group homes | 1037 (517 vs. 520) | 6, 12 | Pregnancy/HIV/STI prevention skills training (Power Through Choices) | 10 × 90 min group sessions, twice a week for 5 weeks | TAU | K + A: Knowledge about sex and HIV, attitudes toward protection, self-efficacy to practice safe sex, intentions re: sex and condom use B: sexual behaviours SW: ability to communicate with partner | K + A: At 6 m and 12 m, INTV sig better knowledge about anatomy and fertility, HIV and STIs, and methods of protection (all p < 0.001). INTV showed more support for methods of protection (p < 0.03) and better knowledge of where to get birth control (p < 0.003). B: All ns SW: INTV sig higher ability to communicate with partner (p < 0.001). |
| Oman et al., 2018; CA, MD and OK, USA | Out-of-home care; justice-involved youth | 13–18 | Group homes | 1037 (517 vs. 520) Note: Same sample as Green et al. (2017) | 6, 12 | Pregnancy/HIV/STI prevention skills training (Power Through Choices) | 10 × 90 min group sessions, twice a week for 5 weeks | TAU | B: Sex without condoms/birth control, ever been pregnant/gotten someone pregnant | B: At 12 m, INTV participants were less likely than control to have been, or have gotten somebody, pregnant, AOR = 0.67. |
| Slonim-Nevo, et al., 1996; St Louis, MO, USA | Out-of-home care; justice-involved youth; mental ill-health | 12–18 | Residential centres | 268 (group sizes not reported) | 9, 12 | HIV risk reduction skills training vs. HIV discussion groups | 9 × 90–120 min group sessions over 3 weeks | TAU | K + A: knowledge, attitudes and intentions to cope with AIDS-risk situations B: Engagement in unsafe sexual activities | K + I: At 9 and 12 m, AIDS related attitudes ns. Discussion group had greater knowledge about AIDS (p = 0.02) and intentions to cope with AIDS-risk situations knowledge (p = 0.02). B: All ns |
Appendix B
MEDLINE (Ovid) Search Terms
- ((“safe sex” or “unsafe sex” or “sexual risk taking” or “sex* risk behavio*r” or STI or HIV or chlamydia or gonorrhoea or hepatitis or syphilis or “acquired immunodeficiency syndrome” or condom* or “barrier contraception” or “unwanted pregnancy”).ti,ab. or exp *Sexually Transmitted Diseases/or exp *Sexual Health/or exp *Sexual Behavior/or exp *Sex Education/or exp *Sex Education/mt or exp *Health Knowledge, Attitudes, Practice/or exp *Contraception, Barrier/or exp *Contraception Behavior/or exp *Contraception/or exp *Long-Acting Reversible Contraception/or exp *Hormonal Contraception/or exp *Pregnancy, Unwanted/) and ((“behavio* therapy” or “cognitive therapy” or “psychosocial intervention” or “skills training” or “sex education” or “motivational interview*”).ti,ab. or exp *Psychosocial Intervention/or exp *Behavior Therapy/or exp *Cognitive Behavioral Therapy/or exp *Motivational Interviewing/) and ((youth or “young adult*” or teenage* or “high school student*” or adolescen* or “university student*”.ti,ab.) or exp *Adolescent/or exp *Young Adult/or exp *Child/or exp *Students/or exp *Adolescent Behavior/)
- (alcohol* or binge or ethanol or drink* or “drug use” or “recreational drug*” or “substance use”).ti,ab. or exp *Alcohol Drinking/or exp *Substance-Related Disorders/or exp *Alcoholism/or exp *Illicit Drugs/
- (“minority group*” OR “ethnic minorit*” OR “ethnic group*” OR immigrant* OR “racial group*” OR black OR hispanic OR latin* OR asian OR indigenous OR “native American” OR aboriginal OR “first nations” OR african OR vietnamese OR “hawaii* native” OR asian OR indian OR inuit OR “pacific islander*” OR “american indian*”).ti,ab. or exp *Ethnic Groups/or exp *Minority Groups/or exp *Indigenous Canadians/or exp *Health Services, Indigenous/or exp *Indigenous Peoples/
- (homeless* or “street youth” or “runaway youth”).ti,ab. or exp *Homeless Youth/
- (“juvenile justice” or probation or court* or “law enforcement” or “diversion program” or “juvenile detention”).ti,ab. or exp *Juvenile Delinquency/
- (gay or lesbian* or genderqueer or transgender* or homosexual* or bisexual or bicurious or “female to male” or “male to female” or trans or “men who have sex with men” or MSM or intersex or LGBT or LGBTQ or LGBTQI or “gender transition” or “gender dysphoria” or “gender identity” or “same sex attracted” or “same sex couple” or “same sex couples” or “sexual and gender minorities” or “sexual orientation” or “sexual preference” or “trans wom#n” or “trans m#n” or “trans people” or “women loving women” or “women who have sex with women” or WSW).ti,ab. or exp *”Sexual and Gender Minorities”/
- (“severe mental illness” or “serious mental illness” or “chronic mental illness” or schizophrenia or bipolar or mania or psychosis or schizoaffective or “major depressive disorder” or MDD).ti,ab. or exp *Mental Disorders/
- (“foster care” or “group home*” or “out-of-home care” or “residential care”).ti,ab. or exp *Foster Home Care/
- 2 or 3 or 4 or 5 or 6 or 7 or 8
- 1 and 9
References
- World Health Organization. Defining Sexual Health: Report of a Technical Consultation on Sexual Health, 28–31 January 2002, Geneva; World Health Organization: Geneva, Switzerland, 2006. [Google Scholar]
- Duberg, A.-S.; Törner, A.; Daviðsdóttir, L.; Aleman, S.; Blaxhult, A.; Svensson, A.; Hultcrantz, R.; Bäck, E.; Ekdahl, K. Cause of death in individuals with chronic HBV and/or HCV infection, a nationwide community-based register study. J. Viral Hepat. 2008, 15, 538–550. [Google Scholar] [CrossRef] [Green Version]
- Trickey, A.; May, M.T.; Vehreschild, J.-J.; Obel, N.; Gill, M.J.; Crane, H.M.; Boesecke, C.; Patterson, S.; Grabar, S.; Cazanave, C.; et al. Survival of HIV-positive patients starting antiretroviral therapy between 1996 and 2013: A collaborative analysis of cohort studies. Lancet HIV 2017, 4, e349–e356. [Google Scholar] [CrossRef] [Green Version]
- Munoz, N.; Castellsagué, X.; De González, A.B.; Gissmann, L. HPV in the etiology of human cancer. Vaccine 2006, 24, S1–S10. [Google Scholar] [CrossRef] [PubMed]
- Campbell, R.; Dworkin, E.; Cabral, G. An Ecological Model of the Impact of Sexual Assault On Women’s Mental Health. Trauma Violence Abus. 2009, 10, 225–246. [Google Scholar] [CrossRef] [PubMed]
- Field, N.; Prah, P.; Mercer, C.H.; Rait, G.; King, M.; Cassell, J.A.; Tanton, C.; Heath, L.; Mitchell, K.R.; Clifton, S. Are depression and poor sexual health neglected comorbidities? Evidence from a population sample. BMJ Open 2016, 6, e010521. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Adan Sanchez, A.Y.; McMillan, E.; Bhaduri, A.; Pehlivan, N.; Monson, K.; Badcock, P.; Thompson, K.; Killackey, E.; Chanen, A.; O’Donoghue, B. High-risk sexual behaviour in young people with mental health disorders. Early Interv. Psychiatry 2018, 13, 867–873. [Google Scholar] [CrossRef]
- Idele, P.; Gillespie, A.; Porth, T.; Suzuki, C.; Mahy, M.; Kasedde, S.; Luo, C. Epidemiology of HIV and AIDS Among Adolescents: Current Status, Inequities, and Data Gaps. J. Acquir. Immune Defic. Syndr. 2014, 66, S144–S153. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chawla, N.; Sarkar, S. Defining “High-risk Sexual Behavior” in the Context of Substance Use. J. Psychosex. Health 2019, 1, 26–31. [Google Scholar] [CrossRef]
- Weinstock, H.; Berman, S.; Cates, W., Jr. Sexually transmitted diseases among American youth: Incidence and prevalence estimates, 2000. Perspect. Sex. Reprod. Health 2004, 36, 6–10. [Google Scholar] [CrossRef] [PubMed]
- Satterwhite, C.L.; Torrone, E.; Meites, E.; Dunne, E.F.; Mahajan, R.; Ocfemia, M.C.B.; Su, J.; Xu, F.; Weinstock, H. Sexually Transmitted Infections Among US Women and Men: Prevalence and Incidence Estimates, 2008. Sex. Transm. Dis. 2013, 40, 187–193. [Google Scholar] [CrossRef]
- Cook, S.M.C.; Cameron, S.T. Social issues of teenage pregnancy. Obstet. Gynaecol. Reprod. Med. 2015, 25, 243–248. [Google Scholar] [CrossRef]
- Haberland, N.; Rogow, D. Sexuality education: Emerging trends in evidence and practice. J. Adolesc. Health 2015, 56, S15–S21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Evans, R.; Widman, L.; Stokes, M.N.; Javidi, H.; Hope, E.C.; Brasileiro, J. Association of Sexual Health Interventions With Sexual Health Outcomes in Black Adolescents: A Systematic Review and Meta-analysis. JAMA Pediatr. 2020, 174, 676–689. [Google Scholar] [CrossRef]
- Shoveller, J.A.; Johnson, J.L. Risky groups, risky behaviour, and risky persons: Dominating discourses on youth sexual health. Crit. Public Health 2006, 16, 47–60. [Google Scholar] [CrossRef]
- Australian Department of Health: Canberra, Australia. 2004. Available online: https://www1.health.gov.au/internet/publications/publishing.nsf/Content/drugtreat-pubs-front3-wk-toc~drugtreat-pubs-front3-wk-secb~drugtreat-pubs-front3-wk-secb-2~drugtreat-pubs-front3-wk-secb-2-1 (accessed on 15 June 2021).
- Centers for Disease Control Prevention. HIV Surveillance in Men Who Have Sex with Men (MSM); Centers for Disease Control Prevention: Atlanta, GA, USA, 2016.
- Kubicek, K.; Beyer, W.J.; Weiss, G.; Iverson, E.; Kipke, M.D. In the dark: Young men’s stories of sexual initiation in the absence of relevant sexual health information. Health Educ. Behav. 2010, 37, 243–263. [Google Scholar] [CrossRef]
- Maxwell, S.; Shahmanesh, M.; Gafos, M. Chemsex behaviours among men who have sex with men: A systematic review of the literature. Int. J. Drug Policy 2019, 63, 74–89. [Google Scholar] [CrossRef]
- Mojola, S.A.; Everett, B. STD and HIV risk factors among US young adults: Variations by gender, race, ethnicity and sexual orientation. Perspect. Sex. Reprod. Health 2012, 44, 125–133. [Google Scholar] [CrossRef]
- Herrick, A.; Kuhns, L.; Kinsky, S.; Johnson, A.; Garofalo, R. Demographic, psychosocial, and contextual factors associated with sexual risk behaviors among young sexual minority women. J. Am. Psychiatr. Nurses Assoc. 2013, 19, 345–355. [Google Scholar] [CrossRef]
- Cook, R.L.; Comer, D.M.; Wiesenfeld, H.C.; Chang, C.-C.H.; Tarter, R.; Lave, J.R.; Clark, D.B. Alcohol and drug use and related disorders: An underrecognized health issue among adolescents and young adults attending sexually transmitted disease clinics. Sex. Transm. Dis. 2006, 33, 565–570. [Google Scholar] [CrossRef] [PubMed]
- Barnert, E.S.; Perry, R.; Morris, R.E. Juvenile incarceration and health. Acad. Pediatr. 2016, 16, 99–109. [Google Scholar] [CrossRef] [PubMed]
- Gramkowski, B.; Kools, S.; Paul, S.; Boyer, C.B.; Monasterio, E.; Robbins, N. Health risk behavior of youth in foster care. J. Child Adolesc. Psychiatr. Nurs. 2009, 22, 77–85. [Google Scholar] [CrossRef] [Green Version]
- Testa, A.; Coleman, L. Sexual health knowledge, attitudes and behaviours among black and minority ethnic youth in London. Brighton Trust Study Adolesc. 2007, 66, 68–81. [Google Scholar]
- Centres for Disease Control and Prevention. HIV/AIDS Prevention Research Synthesis Project. Compendium of Evidence-Based Interventions and Best Practices for HIV Prevention. Centers for Disease Control and Prevention. Available online: https://www.cdc.gov/hiv/dhap/prb/prs/index.html (accessed on 15 June 2021).
- Walsh, C.; McCann, E.; Gilbody, S.; Hughes, E. Promoting HIV and sexual safety behaviour in people with severe mental illness: A systematic review of behavioural interventions. Int. J. Mental Health Nurs. 2014, 23, 344–354. [Google Scholar] [CrossRef] [Green Version]
- Pandor, A.; Kaltenthaler, E.; Higgins, A.; Lorimer, K.; Smith, S.; Wylie, K.; Wong, R. Sexual health risk reduction interventions for people with severe mental illness: A systematic review. BMC Public Health 2015, 15, 138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wright, N.; Walker, J. Homelessness and drug use—A narrative systematic review of interventions to promote sexual health. AIDS Care 2006, 18, 467–478. [Google Scholar] [CrossRef] [PubMed]
- Underhill, K.; Dumont, D.; Operario, D. HIV Prevention for Adults With Criminal Justice Involvement: A Systematic Review of HIV Risk-Reduction Interventions in Incarceration and Community Settings. Am. J. Public Health 2014, 104, e27–e53. [Google Scholar] [CrossRef] [PubMed]
- Herbst, J.H.; Beeker, C.; Mathew, A.; McNally, T.; Passin, W.F.; Kay, L.S.; Crepaz, N.; Lyles, C.M.; Briss, P.; Chattopadhyay, S. The effectiveness of individual-, group-, and community-level HIV behavioral risk-reduction interventions for adult men who have sex with men: A systematic review. Am. J. Prev. Med. 2007, 32, 38–67. [Google Scholar] [CrossRef] [PubMed]
- St. Lawrence, J.; Jefferson, K.; Alleyne, E.; Brasfield, T. Comparison of Education Versus Behavioral Skills Training Interventions in Lowering Sexual HIV-Risk Behavior of Substance-Dependent Adolescents. J. Consult. Clin. Psychol. 1995, 63, 154–157. [Google Scholar] [CrossRef]
- St. Lawrence, J.S.; Crosby, R.A.; Brasfield, T.L.; O Bannon, R.E. Reducing STD and HIV Risk Behavior of Substance-Dependent Adolescents: A Randomized Controlled Trial. J. Consult. Clin. Psychol. 2002, 70, 1010–1021. [Google Scholar] [CrossRef]
- Letourneau, E.J.; McCart, M.R.; Sheidow, A.J.; Mauro, P.M. First Evaluation of a Contingency Management Intervention Addressing Adolescent Substance Use and Sexual Risk Behaviors: Risk Reduction Therapy for Adolescents. J. Subst. Abus. Treat. 2017, 72, 56–65. [Google Scholar] [CrossRef] [Green Version]
- Suffoletto, B.; Akers, A.; McGinnis, K.A.; Calabria, J.; Wiesenfeld, H.C.; Clark, D.B. A Sex Risk Reduction Text-Message Program for Young Adult Females Discharged From the Emergency Department. J. Adolesc. Health 2013, 53, 387–393. [Google Scholar] [CrossRef]
- Bryan, A.D.; Magnan, R.E.; Gillman, A.S.; Yeater, E.A.; Feldstein Ewing, S.W.; Kong, A.S.; Schmiege, S.J. Effect of including alcohol and cannabis content in a sexual risk-reduction intervention on the incidence of sexually transmitted infections in adolescents: A cluster randomized clinical trial. JAMA Pediatr. 2018, 172. [Google Scholar] [CrossRef]
- Bryan, A.D.; Schmiege, S.J.; Broaddus, M.R. HIV risk reduction among detained adolescents: A randomized, controlled trial. Pediatrics 2009, 124, e1180–e1188. [Google Scholar] [CrossRef]
- Slesnick, N.; Kang, M.J. The impact of an integrated treatment on HIV risk behavior among homeless youth: A randomized controlled trial. J. Behav. Med. 2008, 31, 45–59. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tucker, J.S.; D’Amico, E.J.; Ewing, B.A.; Miles, J.N.; Pedersen, E.R. A group-based motivational interviewing brief intervention to reduce substance use and sexual risk behavior among homeless young adults. J. Subst. Abus. Treat. 2017, 76, 20–27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tolou-Shams, M.; Houck, C.; Conrad, S.M.; Tarantino, N.; Stein, L.A.R.; Brown, L.K. HIV Prevention for Juvenile Drug Court Offenders: A Randomized Controlled Trial Focusing on Affect Management. J. Correct. Health Care 2011, 17, 226–232. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tingey, L.; Mullany, B.; Chambers, R.; Hastings, R.; Lee, A.; Parker, A.; Barlow, A.; Rompalo, A. Respecting the circle of life: One year outcomes from a randomized controlled comparison of an HIV risk reduction intervention for American Indian adolescents. AIDS Care 2015, 27, 1087–1097. [Google Scholar] [CrossRef]
- Smith, M.L.; Wilson, K.L.; Bergeron, C.D. Condom Use for Sexually Transmitted Infection Prevention Among Hispanic Teenage Mothers: A Community-Based Randomized Trial. J. Women’s Health 2020, 29, 534–540. [Google Scholar] [CrossRef] [PubMed]
- Kipke, M.; Boyer, C.; Hein, K. An evaluation of an AIDS risk reduction education and skills training (Arrest) program. J. Adolesc. Health 1993, 14, 533–539. [Google Scholar] [CrossRef]
- Villarruel, A.M.; Jemmott, J.B.; Jemmott, L.S. A Randomized Controlled Trial Testing an HIV Prevention Intervention for Latino Youth. Arch. Pediatr. Adolesc. Med. 2006, 160, 772–777. [Google Scholar] [CrossRef] [Green Version]
- Mustanski, B.; Garofalo, R.; Monahan, C.; Gratzer, B.; Andrews, R. Feasibility, acceptability, and preliminary efficacy of an online HIV prevention program for diverse young men who have sex with men: The keep it up! intervention. AIDS Behav. 2013, 17, 2999–3012. [Google Scholar] [CrossRef]
- Thompson, R.G.; Aivadyan, C.; Stohl, M.; Aharonovich, E.; Hasin, D.S. Smartphone application plus brief motivational intervention reduces substance use and sexual risk behaviors among homeless young adults: Results from a randomized controlled trial. Psychol. Addict. Behav. 2020, 34, 641–649. [Google Scholar] [CrossRef]
- Kerr, D.C.R.; Leve, L.D.; Chamberlain, P. Pregnancy Rates Among Juvenile Justice Girls in Two Randomized Controlled Trials of Multidimensional Treatment Foster Care. J. Consult. Clin. Psychol. 2009, 77, 588–593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- St. Lawrence, J.S.; Crosby, R.A.; Belcher, L.; Yazdani, N.; Brasfield, T.L. Sexual Risk Reduction and Anger Management Interventions for Incarcerated Male Adolescents: A Randomized Controlled Trial of Two Interventions. J. Sex Educ. Ther. 1999, 24, 9–17. [Google Scholar] [CrossRef]
- Goldberg, E.; Millson, P.; Rivers, S.; Manning, S.J.; Leslie, K.; Read, S.; Shipley, C.; Victor, J.C. A Human Immunodeficiency Virus Risk Reduction Intervention for Incarcerated Youth: A Randomized Controlled Trial. J. Adolesc. Health 2009, 44, 136–145. [Google Scholar] [CrossRef] [PubMed]
- Green, J.; Oman, R.F.; Lu, M.; Clements-Nolle, K.D. Long-Term Improvements in Knowledge and Psychosocial Factors of a Teen Pregnancy Prevention Intervention Implemented in Group Homes. J. Adolesc. Health 2017, 60, 698–705. [Google Scholar] [CrossRef] [PubMed]
- Slonim-Nevo, V.; Auslander, W.F.; Ozawa, M.N.; Jung, K.G. The Long-Term Impact of AIDS-Preventive Interventions for Delinquent and Abused Adolescents. Adolescence 1996, 31, 409–421. [Google Scholar]
- Oman, R.F.; Vesely, S.K.; Green, J.; Clements-Nolle, K.; Lu, M. Adolescent Pregnancy Prevention Among Youths Living in Group Care Homes: A Cluster Randomized Controlled Trial. Am. J. Public Health 2018, 108, S38–S44. [Google Scholar] [CrossRef]
- Chen, X.; Murphy, D.A.; Naar-King, S.; Parsons, J.T. A clinic-based motivational intervention improves condom use among subgroups of youth living with HIV. J. Adolesc. Health 2011, 49, 193–198. [Google Scholar] [CrossRef] [Green Version]
- Hidalgo, M.A.; Kuhns, L.M.; Hotton, A.L.; Johnson, A.K.; Mustanski, B.; Garofalo, R. The MyPEEPS Randomized Controlled Trial: A Pilot of Preliminary Efficacy, Feasibility, and Acceptability of a Group-Level, HIV Risk Reduction Intervention for Young Men Who Have Sex with Men. Arch. Sex. Behav. 2015, 44, 475–485. [Google Scholar] [CrossRef]
- Ybarra, M.L.; Liu, W.; Prescott, T.L.; Phillips, G.; Mustanski, B. The Effect of a Text Messaging Based HIV Prevention Program on Sexual Minority Male Youths: A National Evaluation of Information, Motivation and Behavioral Skills in a Randomized Controlled Trial of Guy2Guy. AIDS Behav. 2018, 22, 3335–3344. [Google Scholar] [CrossRef] [PubMed]
- Rongkavilit, C.; Wang, B.; Naar-King, S.; Bunupuradah, T.; Parsons, J.T.; Panthong, A.; Koken, J.A.; Saengcharnchai, P.; Phanuphak, P. Motivational interviewing targeting risky sex in HIV-positive young Thai men who have sex with men. Arch. Sex. Behav. 2015, 44, 329–340. [Google Scholar] [CrossRef] [Green Version]
- Philliber, A. The IN·clued Program: A Randomized Control Trial of an Effective Sex Education Program for Lesbian, Gay, Bisexual, Transgender, Queer, and Questioning Youths. J. Adolesc. Health 2021. [Google Scholar] [CrossRef]
- Brown, L.M.D.; Wendy Hadley, P.D.; Geri, R.; Donenberg, P.D.; Ralph, J.; Di Clemente, P.D.; Celia Lescano, P.D.; Delia, M.; Lang, P.D.; Richard Crosby, P.D.; et al. Project STYLE: A Multisite RCT for HIV Prevention Among Youths in Mental Health Treatment. Psychiatr. Serv. 2014, 65, 338–344. [Google Scholar] [CrossRef] [PubMed]
- Brown, L.K.; Whiteley, L.; Houck, C.D.; Craker, L.K.; Lowery, A.; Beausoleil, N.; Donenberg, G. The Role of Affect Management for HIV Risk Reduction for Youth in Alternative Schools. J. Am. Acad. Child Adolesc. Psychiatry 2017, 56, 524–531. [Google Scholar] [CrossRef] [PubMed]
- Champion, J.D.; Collins, J.L. Comparison of a theory-based (AIDS Risk Reduction Model) cognitive behavioral intervention versus enhanced counseling for abused ethnic minority adolescent women on infection with sexually transmitted infection: Results of a randomized controlled trial. Int. J. Nurs. Stud. 2012, 49, 138–150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- John, S.A.; Walsh, J.L.; Weinhardt, L.S. The Information-Motivation-Behavioral Skills Model Revisited: A Network-Perspective Structural Equation Model Within a Public Sexually Transmitted Infection Clinic Sample of Hazardous Alcohol Users. AIDS Behav. 2017, 21, 1208–1218. [Google Scholar] [CrossRef] [Green Version]
- Fisher, E.B.; Fitzgibbon, M.L.; Glasgow, R.E.; Haire-Joshu, D.; Hayman, L.L.; Kaplan, R.M.; Nanney, M.S.; Ockene, J.K. Behavior Matters. Am. J. Prev. Med. 2011, 40, e15–e30. [Google Scholar] [CrossRef] [PubMed]
- Starrs, A.M.; Ezeh, A.C.; Barker, G.; Basu, A.; Bertrand, J.T.; Blum, R.; Coll-Seck, A.M.; Grover, A.; Laski, L.; Roa, M.; et al. Accelerate progress—Sexual and reproductive health and rights for all: Report of the Guttmacher– Lancet Commission. Lancet 2018, 391, 2642–2692. [Google Scholar] [CrossRef]
- Slater, C.; Robinson, A.J. Sexual health in adolescents. Clin. Dermatol. 2014, 32, 189–195. [Google Scholar] [CrossRef]
- Ford, J.V.; Corona Vargas, E.; Finotelli, I., Jr.; Fortenberry, J.D.; Kismödi, E.; Philpott, A.; Rubio-Aurioles, E.; Coleman, E. Why Pleasure Matters: Its Global Relevance for Sexual Health, Sexual Rights and Wellbeing. Int. J. Sex. Health 2019, 31, 217–230. [Google Scholar] [CrossRef]
- Edwards, W.M.; Coleman, E. Defining sexual health: A descriptive overview. Arch. Sex. Behav. 2004, 33, 189–195. [Google Scholar] [CrossRef]
- Hogben, M.; Ford, J.; Becasen, J.S.; Brown, K.F. A Systematic Review of Sexual Health Interventions for Adults: Narrative Evidence. J. Sex Res. 2015, 52, 444–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Scott-Sheldon, L.A.; Johnson, B.T. Eroticizing creates safer sex: A research synthesis. J. Prim. Prev. 2006, 27, 619–640. [Google Scholar] [CrossRef] [PubMed]
- Hanbury, A.; Eastham, R. Keep calm and contracept! Addressing young women’s pleasure in sexual health and contraception consultations. Sex Educ. 2016, 16, 255–265. [Google Scholar] [CrossRef]
- Bryant, J.; Ellard, J. Hope as a form of agency in the future thinking of disenfranchised young people. J. Youth Stud. 2015, 18, 485–499. [Google Scholar] [CrossRef]
- Adler, J.M.; Chin, E.D.; Kolisetty, A.P.; Oltmanns, T.F. The distinguishing characteristics of narrative identity in adults with features of borderline personality disorder: An empirical investigation. J. Pers. Disord. 2012, 26, 498–512. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- David, N.; Newen, A.; Vogeley, K. The “sense of agency” and its underlying cognitive and neural mechanisms. Conscious. Cogn. 2008, 17, 523–534. [Google Scholar] [CrossRef]
- Rickwood, D.; Paraskakis, M.; Quin, D.; Hobbs, N.; Ryall, V.; Trethowan, J.; McGorry, P. Australia’s innovation in youth mental health care: The headspace centre model. Early Interv. Psychiatry 2019, 13, 159–166. [Google Scholar] [CrossRef]
- Sweeney, S.; Obure, C.D.; Maier, C.B.; Greener, R.; Dehne, K.; Vassall, A. Costs and efficiency of integrating HIV/AIDS services with other health services: A systematic review of evidence and experience. Sex. Transm. Infect. 2012, 88, 85. [Google Scholar] [CrossRef] [Green Version]
- Public Health England. Teenage Pregnancy Prevention Framework; Supporting Young People to Prevent Unplanned Pregnancy and Develop Healthy Relationships. Available online: https://www.gov.uk/government/publications/teenage-pregnancy-prevention-framework (accessed on 15 June 2021).
- Kpokiri, E.E.; Wu, D.; Srinivas, M.L.; Anderson, J.; Say, L.; Kontula, O.; Ahmad, N.A.; Morroni, C.; Izugbara, C.; de Visser, R.; et al. Development of an international sexual and reproductive health survey instrument: Results from a pilot WHO/HRP consultative Delphi process. Sex. Transm. Infect. 2021. [Google Scholar] [CrossRef] [PubMed]

| PICO Element | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Population | Young people ≤25 years old, of any gender, who are members of one of the following high-risk groups:
| Samples including participants >25 years old at start of trial If the trial targeted black American youth as the only ‘high-risk’ criteria given previously completed review in this population. |
| Intervention | Any psychosocial or behavioural intervention aimed at promoting sexual health and/or sexual safety-taking behaviours | Any intervention that targets parents of young people rather than the young people directly, or any intervention that is focused solely on promoting abstinence |
| Comparison | Any non-pharmacological comparator (e.g., waitlist control) | A pharmacological comparator |
| Outcome | Sexual health or safety-taking behaviours, e.g., condom use; Biological indicators of sexual safety-taking behaviour, e.g., STI incidence, unwanted pregnancy; Changes in knowledge of, or attitudes toward, sexual health and safety. Measures of sexual wellbeing e.g., communication skills or relationship satisfaction | Abstinence |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Brown, E.; Lo Monaco, S.; O’Donoghue, B.; Nolan, H.; Hughes, E.; Graham, M.; Simmons, M.; Gray, R. Improving the Sexual Health of Young People (under 25) in High-Risk Populations: A Systematic Review of Behavioural and Psychosocial Interventions. Int. J. Environ. Res. Public Health 2021, 18, 9063. https://doi.org/10.3390/ijerph18179063
Brown E, Lo Monaco S, O’Donoghue B, Nolan H, Hughes E, Graham M, Simmons M, Gray R. Improving the Sexual Health of Young People (under 25) in High-Risk Populations: A Systematic Review of Behavioural and Psychosocial Interventions. International Journal of Environmental Research and Public Health. 2021; 18(17):9063. https://doi.org/10.3390/ijerph18179063
Chicago/Turabian StyleBrown, Ellie, Samantha Lo Monaco, Brian O’Donoghue, Hayley Nolan, Elizabeth Hughes, Melissa Graham, Magenta Simmons, and Richard Gray. 2021. "Improving the Sexual Health of Young People (under 25) in High-Risk Populations: A Systematic Review of Behavioural and Psychosocial Interventions" International Journal of Environmental Research and Public Health 18, no. 17: 9063. https://doi.org/10.3390/ijerph18179063
APA StyleBrown, E., Lo Monaco, S., O’Donoghue, B., Nolan, H., Hughes, E., Graham, M., Simmons, M., & Gray, R. (2021). Improving the Sexual Health of Young People (under 25) in High-Risk Populations: A Systematic Review of Behavioural and Psychosocial Interventions. International Journal of Environmental Research and Public Health, 18(17), 9063. https://doi.org/10.3390/ijerph18179063