
Sextech Use as a Potential Mental Health Reprieve: The Role of Anxiety, Depression, and Loneliness in Seeking Sex Online


 and
and
Abstract
:1. Introduction
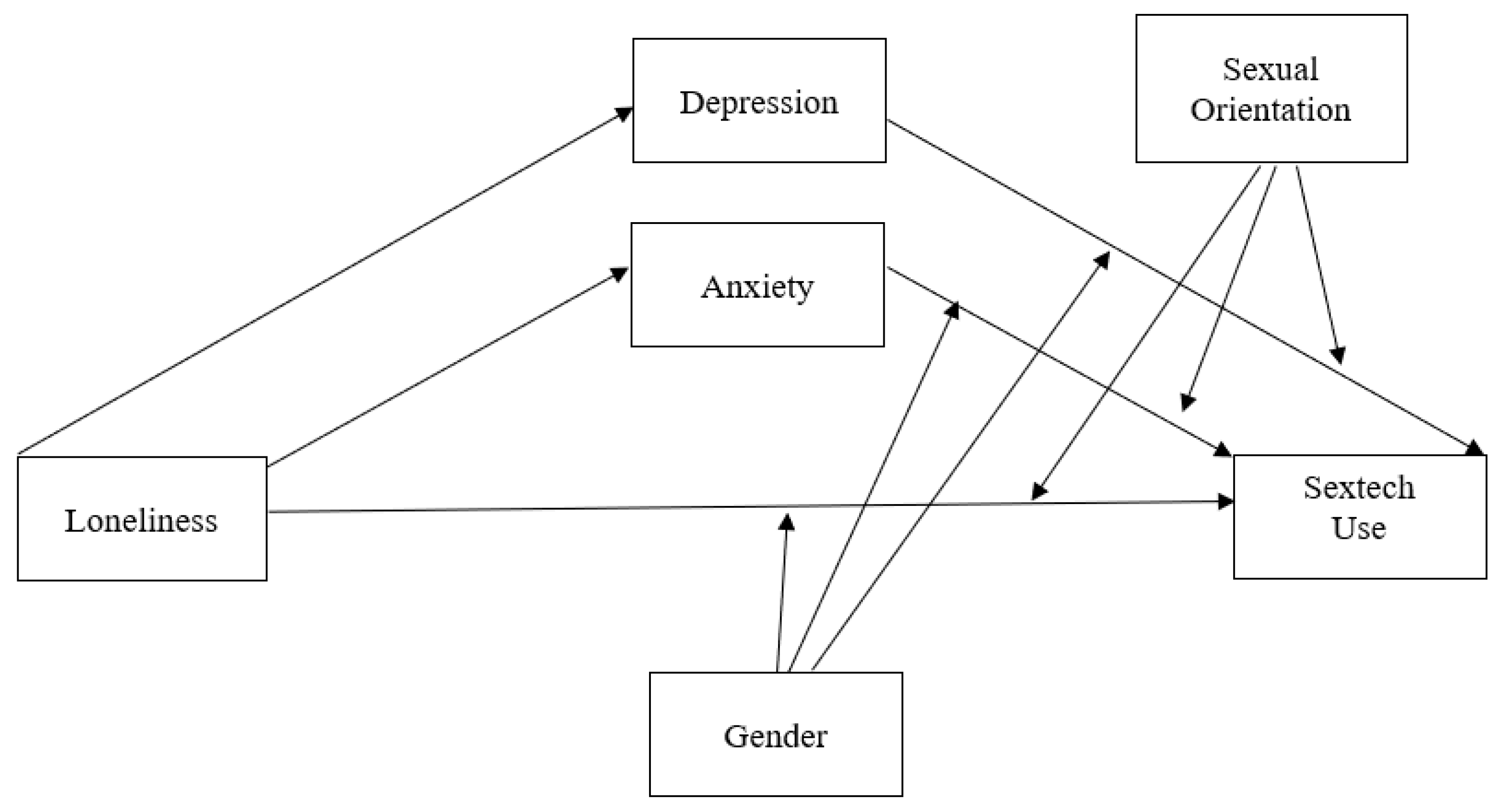
- RQ1. Are higher levels of loneliness, anxiety, and/or depression associated with sextech engagement?
- RQ2. Do anxiety and depression mediate the association between loneliness and sextech engagement?
- RQ3. How do gender and sexual orientation moderate each of the aforementioned associations in RQ1 and RQ2?
2. Materials and Methods
2.1. Procedure
2.2. Ethical Considerations
2.3. Participants
2.4. Measures
2.4.1. Sociodemographics
2.4.2. Mental Health
2.4.3. Sexual Desire
2.4.4. Types of Sextech
3. Data Analysis
4. Results
4.1. Descriptive Statistics: Frequency of Sextech Use
4.2. Moderated Mediation
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. The World Health Report 2001: Mental Disorders Affect One in Four People. 2001. Available online: https://www.who.int/news/item/28-09-2001-the-world-health-report-2001-mental-disorders-affect-one-in-four-people (accessed on 1 May 2021).
- Hyman, S.; Chisholm, D.; Kessler, R.; Patel, V.; Whiteford, H. Mental Disorders. In Disease Control Policies in Developing Countries, 2nd ed.; Jamison, D.T., Breman, J.G., Measham, A.R., Alleyne, G., Claeson, M., Evans, D.B., Musgrove, P., Eds.; Oxford University Press: New York, NY, USA, 2006. [Google Scholar]
- UK Prime Minister’s Office. PM Launches Government’s First Loneliness Strategy. 2018. Available online: https://www.gov.uk/government/news/pm-launches-governments-first-loneliness-strategy (accessed on 15 June 2021).
- GBD 2017 Disease and Injury Incidence and Prevalence Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 354 diseases and injuries for 195 countries and territories, 1990–2017: A systematic analysis for the Global Burden of Disease Study 2017. Lancet 2018, 392, 1789–1858. [Google Scholar] [CrossRef] [Green Version]
- Lamers, F.; Van Oppen, P.; Comijs, H.C.; Smit, J.H.; Spinhoven, P.; van Balkom, A.J.L.M.; Nolen, W.A.; Zitman, F.G.; Beekman, A.T.F.; Penninx, B.W.J.H. Comorbidity Patterns of Anxiety and Depressive Disorders in a Large Cohort Study: The Netherlands Study of Depression and Anxiety (NESDA). J. Clin. Psychiatry 2011, 72, 341–348. [Google Scholar] [CrossRef]
- Hirschfeld, R.M.A. The comorbidity of major depression and anxiety disorders: Recognition and management in primary care. Prim. Care Companion J. Clin. Psychiatry 2001, 3, 244–254. [Google Scholar] [CrossRef]
- Mushtaq, R.; Shoib, S.; Shah, T.; Mushtaq, S. Relationship between Loneliness, Psychiatric Disorders and Physical Health? A Review on the Psychological Aspects of Loneliness. J. Clin. Diagn. Res. 2014, 8, WE01. [Google Scholar] [CrossRef]
- Cacioppo, J.T.; Patrick, W. Loneliness: Human Nature and the Need for Social Connection; 1. publ. as a Norton paperback; Norton: New York, NY, USA, 2009. [Google Scholar]
- Erzen, E.; Çikrikci, O. The effect of loneliness on depression: A meta-analysis. Int. J. Soc. Psychiatry 2018, 64, 427–435. [Google Scholar] [CrossRef]
- Beutel, M.E.; Klein, E.M.; Brähler, E.; Reiner, I.; Jünger, C.; Michal, M.; Wiltink, J.; Wild, P.S.; Münzel, T.; Lackner, K.J.; et al. Loneliness in the general population: Prevalence, determinants and relations to mental health. BMC Psychiatry 2017, 17, 97. [Google Scholar] [CrossRef] [Green Version]
- Richardson, T.; Elliott, P.; Roberts, R. Relationship between loneliness and mental health in students. J. Public Ment. Health 2017, 16, 48–54. [Google Scholar] [CrossRef] [Green Version]
- Cross, S.E.; Madson, L. Models of the self: Self-Construals and gender. Psychol. Bull. 1997, 122, 5–37. [Google Scholar] [CrossRef]
- Cambron, M.J.; Acitelli, L.K.; Pettit, J.W. Explaining Gender Differences in Depression: An Interpersonal Contingent Self-Esteem Perspective. Sex Roles 2009, 61, 751–761. [Google Scholar] [CrossRef]
- Chang, E.C. Relationship between loneliness and symptoms of anxiety and depression in African American men and women: Evidence for gender as a moderator. Pers. Individ. Differ. 2018, 120, 138–143. [Google Scholar] [CrossRef]
- Fitzpatrick, K.M.; Piko, B.F.; Wright, D.R.; LaGory, M. Depressive Symptomatology, Exposure to Violence, and the Role of Social Capital Among African American Adolescents. Am. J. Orthopsychiatr. 2005, 75, 262–274. [Google Scholar] [CrossRef] [PubMed]
- Liu, R.T.; Alloy, L.B. Stress generation in depression: A systematic review of the empirical literature and recommendations for future study. Clin. Psychol. Rev. 2010, 30, 582–593. [Google Scholar] [CrossRef] [Green Version]
- Mannes, Z.L.; Burrell, L.E.; Bryant, V.E.; Dunne, E.M.; Hearn, L.E.; Whitehead, N.E. Loneliness and substance use: The influence of gender among HIV+ Black/African American adults 50+. AIDS Care 2015, 28, 598–602. [Google Scholar] [CrossRef] [Green Version]
- Bolton, S.-L.; Sareen, J. Sexual Orientation and its Relation to Mental Disorders and Suicide Attempts: Findings from a Nationally Representative Sample. Can. J. Psychiatry 2011, 56, 35–43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rimes, K.A.; Ion, D.; Wingrove, J.; Carter, B. Sexual orientation differences in psychological treatment outcomes for depression and anxiety: National cohort study. J. Consult. Clin. Psychol. 2019, 87, 577–589. [Google Scholar] [CrossRef] [Green Version]
- Hatzenbuehler, M.L. How does sexual minority stigma “get under the skin”? A psychological mediation framework. Psychol. Bull. 2009, 135, 707–730. [Google Scholar] [CrossRef]
- Meyer, I.H. Prejudice, social stress, and mental health in lesbian, gay, and bisexual populations: Conceptual issues and research evidence. Psychol. Bull. 2003, 129, 674–697. [Google Scholar] [CrossRef]
- Nam, B.; Jun, H.-J.; Fedina, L.; Shah, R.; DeVylder, J.E. Sexual orientation and mental health among adults in four U.S. cities. Psychiatry Res. 2018, 273, 134–140. [Google Scholar] [CrossRef]
- Ross, L.E.; Salway, T.; Tarasoff, L.A.; Mackay, J.M.; Hawkins, B.; Fehr, C.P. Prevalence of Depression and Anxiety Among Bisexual People Compared to Gay, Lesbian, and Heterosexual Individuals: A Systematic Review and Meta-Analysis. J. Sex Res. 2017, 55, 435–456. [Google Scholar] [CrossRef] [Green Version]
- Mereish, E.H.; Poteat, V.P. A relational model of sexual minority mental and physical health: The negative effects of shame on relationships, loneliness, and health. J. Couns. Psychol. 2015, 62, 425–437. [Google Scholar] [CrossRef]
- Li, M.J.; Hubach, R.D.; Dodge, B. Social Milieu and Mediators of Loneliness Among Gay and Bisexual Men in Rural Indiana. J. Gay Lesbian Ment. Health 2015, 19, 331–346. [Google Scholar] [CrossRef]
- Perone, A.; Ingersoll-Dayton, B.; Watkins-Dukhie, K. Social isolation among LGBT older Adults: Lessons learned from a pilot friendly-caller program. Innov. Aging 2019, 3, S742–S743. [Google Scholar] [CrossRef]
- Goldman, R.N.; Greenberg, L.S. Self-Soothing and Other-Soothing in Emotion-Focused Therapy for Couples. In Clinical Casebook of Couple Therapy; Gurman, A.S., Ed.; Guilford Publications: New York, NY, USA, 2010; pp. 255–280. [Google Scholar]
- Bolton, J.; Cox, B.; Clara, I.; Sareen, J. Use of Alcohol and Drugs to Self-Medicate Anxiety Disorders in a Nationally Representative Sample. J. Nerv. Ment. Dis. 2006, 194, 818–825. [Google Scholar] [CrossRef]
- Robinson, J.; Sareen, J.; Cox, B.J.; Bolton, J. Self-medication of anxiety disorders with alcohol and drugs: Results from a nationally representative sample. J. Anxiety Disord. 2009, 23, 38–45. [Google Scholar] [CrossRef] [PubMed]
- Bolton, J.M.; Robinson, J.; Sareen, J. Self-medication of mood disorders with alcohol and drugs in the National Epidemiologic Survey on Alcohol and Related Conditions. J. Affect. Disord. 2009, 115, 367–375. [Google Scholar] [CrossRef]
- Chekroud, S.R.; Gueorguieva, R.; Zheutlin, A.B.; Paulus, M.; Krumholz, H.M.; Krystal, J.H.; Chekroud, A. Association between physical exercise and mental health in 1·2 million individuals in the USA between 2011 and 2015: A cross-sectional study. Lancet Psychiatry 2018, 5, 739–746. [Google Scholar] [CrossRef]
- Nabkasorn, C.; Miyai, N.; Sootmongkol, A.; Junprasert, S.; Yamamoto, H.; Arita, M.; Miyashita, K. Effects of physical exercise on depression, neuroendocrine stress hormones and physiological fitness in adolescent females with depressive symptoms. Eur. J. Public Health 2005, 16, 179–184. [Google Scholar] [CrossRef] [PubMed]
- Lamis, D.A.; Ballard, E.; May, A.M.; Dvorak, R.D. Depressive Symptoms and Suicidal Ideation in College Students: The Mediating and Moderating Roles of Hopelessness, Alcohol Problems, and Social Support. J. Clin. Psychol. 2016, 72, 919–932. [Google Scholar] [CrossRef]
- Gowen, K.; Deschaine, M.; Gruttadara, D.; Markey, D. Young adults with mental health conditions and social networking websites: Seeking tools to build community. Psychiatr. Rehabil. J. 2012, 35, 245–250. [Google Scholar] [CrossRef]
- Baumeister, R.F.; Leary, M.R. The need to belong: Desire for interpersonal attachments as a fundamental human motivation. Psychol. Bull. 1995, 117, 497–529. [Google Scholar] [CrossRef]
- Mikulincer, M.; Shaver, P.R. An attachment and behavioral systems perspective on social support. J. Soc. Pers. Relatsh. 2009, 26, 7–19. [Google Scholar] [CrossRef]
- Deters, F.G.; Mehl, M.R. Does Posting Facebook Status Updates Increase or Decrease Loneliness? An Online Social Networking Experiment. Soc. Psychol. Pers. Sci. 2012, 4, 579–586. [Google Scholar] [CrossRef] [Green Version]
- Dolev-Cohen, M.; Barak, A. Adolescents’ use of Instant Messaging as a means of emotional relief. Comput. Hum. Behav. 2013, 29, 58–63. [Google Scholar] [CrossRef]
- Panova, T.; Lleras, A. Avoidance or boredom: Negative mental health outcomes associated with use of Information and Communication Technologies depend on users’ motivations. Comput. Hum. Behav. 2016, 58, 249–258. [Google Scholar] [CrossRef]
- Cooper, A. Sexuality and the Internet: Surfing into the New Millennium. Cyber Psychol. Behav. 1998, 1, 187–193. [Google Scholar] [CrossRef]
- Gross, E.F. Adolescent Internet use: What we expect, what teens report. J. Appl. Dev. Psychol. 2004, 25, 633–649. [Google Scholar] [CrossRef]
- Valkenburg, P.M.; Peter, J. Online Communication and Adolescent Well-Being: Testing the Stimulation Versus the Displacement Hypothesis. J. Comput. Commun. 2007, 12, 1169–1182. [Google Scholar] [CrossRef] [Green Version]
- Morahan-Martin, J.; Schumacher, P. Loneliness and social uses of the Internet. Comput. Hum. Behav. 2003, 19, 659–671. [Google Scholar] [CrossRef]
- Naslund, J.A.; Bondre, A.; Torous, J.; Aschbrenner, K.A. Social Media and Mental Health: Benefits, Risks, and Opportunities for Research and Practice. J. Technol. Behav. Sci. 2020, 5, 245–257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dalbudak, E.; Evren, C.; Aldemir, S.; Taymur, I.; Evren, B.; Topcu, M. The impact of sensation seeking on the relationship between attention deficit/hyperactivity symptoms and severity of Internet addiction risk. Psychiatry Res. 2015, 228, 156–161. [Google Scholar] [CrossRef] [PubMed]
- Giordano, A.L.; Cashwell, C.S. Cybersex Addiction among College Students: A Prevalence Study. Sex. Addict. Compulsivity 2017, 24, 1–11. [Google Scholar] [CrossRef]
- Sánchez-Fuentes, M.D.M.; Santos-Iglesias, P.; Sierra, J.C. A systematic review of sexual satisfaction. Int. J. Clin. Health Psychol. 2014, 14, 67–75. [Google Scholar] [CrossRef] [Green Version]
- Rosen, R.C.; Bachmann, G.A. Sexual Well-Being, Happiness, and Satisfaction, in Women: The Case for a New Conceptual Paradigm. J. Sex Marital. Ther. 2008, 34, 291–297. [Google Scholar] [CrossRef] [PubMed]
- Davison, S.L.; Bell, R.; LaChina, M.; Holden, S.L.; Davis, S.R. The relationship between self-reported sexual satisfaction and general well-being in women. J. Sex. Med. 2009, 6, 2690–2697. [Google Scholar] [CrossRef] [PubMed]
- Hensel, D.J.; Nance, J.; Fortenberry, J.D. The Association between Sexual Health and Physical, Mental, and Social Health in Adolescent Women. J. Adolesc. Health 2016, 59, 416–421. [Google Scholar] [CrossRef] [Green Version]
- Carcedo, R.J.; Fernández-Rouco, N.; Fernández-Fuertes, A.A.; Martínez-Álvarez, J.L. Association between Sexual Satisfaction and Depression and Anxiety in Adolescents and Young Adults. Int. J. Environ. Res. Public Health 2020, 17, 841. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shindel, A.W.; Eisenberg, M.L.; Breyer, B.N.; Sharlip, I.D.; Smith, J.F. Sexual Function and Depressive Symptoms Among Female North American Medical Students. J. Sex. Med. 2011, 8, 391–399. [Google Scholar] [CrossRef] [PubMed]
- Smith, J.F.; Breyer, B.N.; Eisenberg, M.; Sharlip, I.D.; Shindel, A.W. Sexual Function and Depressive Symptoms among Male North American Medical Students. J. Sex. Med. 2010, 7, 3909–3917. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woloski-Wruble, A.C.; Oliel, Y.; Leefsma, M.; Hochner-Celnikier, D. Sexual Activities, Sexual and Life Satisfaction, and Successful Aging in Women. J. Sex. Med. 2010, 7, 2401–2410. [Google Scholar] [CrossRef] [PubMed]
- Laumann, E.O.; Paik, A.; Glasser, D.B.; Kang, J.-H.; Wang, T.; Levinson, B.; Moreira, E.D.; Nicolosi, A.; Gingell, C.; Laumann, E.O.; et al. A Cross-National Study of Subjective Sexual Well-Being among Older Women and Men: Findings from the Global Study of Sexual Attitudes and Behaviors. Arch. Sex. Behav. 2006, 35, 143–159. [Google Scholar] [CrossRef] [PubMed]
- Little, K.C.; McNulty, J.K.; Russell, V.M. Sex Buffers Intimates against the Negative Implications of Attachment Insecurity. Pers. Soc. Psychol. Bull. 2010, 36, 484–498. [Google Scholar] [CrossRef] [Green Version]
- Ott, M.A.; Millstein, S.G.; Ofner, S.; Halpern-Felsher, B.L. Greater Expectations: Adolescents’ Positive Motivations for Sex. Perspect. Sex. Reprod. Health 2006, 38, 84–89. [Google Scholar] [CrossRef]
- Leigh, B.C. Reasons for having and avoiding sex: Gender, sexual orientation, and relationship to sexual behavior. J. Sex Res. 1989, 26, 199–209. [Google Scholar] [CrossRef]
- Davis, D.; Shaver, P.R.; Vernon, M.L. Attachment Styles and Subjective Motivations for Sex. Pers. Soc. Psychol. Bull. 2004, 30, 1076–1090. [Google Scholar] [CrossRef] [PubMed]
- Muñoz-Laboy, M.; Garcia, J. Bisexual Latino Men’s Motivations for Sex. Am. J. Sex. Educ. 2019, 14, 440–465. [Google Scholar] [CrossRef]
- Morrison-Beedy, D.; Grove, L.; Ji, M.; Baker, E. Understanding the “Why” for High-Risk Behavior: Adolescent Girls’ Motivations for Sex. J. Assoc. Nurses AIDS Care 2017, 28, 877–887. [Google Scholar] [CrossRef] [PubMed]
- Mikulincer, M.; Shaver, P.R. The Attachment Behavioral System in Adulthood: Activation, Psychodynamics, and Interpersonal Processes. Adv. Exp. Soc. Psychol. 2003, 35, 53–152. [Google Scholar] [CrossRef]
- Selterman, D.; Gesselman, A.N.; Moors, A.C. Sexuality through the lens of secure base dynamics: Individual differences in Sexploration. Pers. Individ. Differ. 2019, 147, 229–236. [Google Scholar] [CrossRef]
- Mizrahi, M.; Hirschberger, G.; Mikulincer, M.; Szepsenwol, O.; Birnbaum, G. Reassuring sex: Can sexual desire and intimacy reduce relationship-specific attachment insecurities? Eur. J. Soc. Psychol. 2016, 46, 467–480. [Google Scholar] [CrossRef]
- Burke, P.J.; Katz-Wise, S.L.; Spalding, A.; Shrier, L.A. Intimate Relationships and Sexual Behavior in Young Women with Depression. J. Adolesc. Health 2018, 63, 429–434. [Google Scholar] [CrossRef] [PubMed]
- Lykins, A.D.; Janssen, E.; Newhouse, S.; Heiman, J.R.; Rafaeli, E. The Effects of Similarity in Sexual Excitation, Inhibition, and Mood on Sexual Arousal Problems and Sexual Satisfaction in Newlywed Couples. J. Sex. Med. 2012, 9, 1360–1366. [Google Scholar] [CrossRef] [PubMed]
- Mosack, V.; Steinke, E.E.; Wright, D.W.; Walker, C.; Medina, M.; Moser, D.K.; Chung, M.L. Effects of Depression on Sexual Activity and Sexual Satisfaction in Heart Failure. Dimens. Crit. Care Nurs. 2011, 30, 218–225. [Google Scholar] [CrossRef]
- Shifren, J.L.; Monz, B.U.; Russo, P.A.; Segreti, A.; Johannes, C.B. Sexual problems and distress in United States women: Prevalence and correlates. Obs. Gynecol. 2008, 112, 970–978. [Google Scholar] [CrossRef] [Green Version]
- Davison, J.; Huntington, A. “Out of sight”: Sexuality and women with enduring mental illness. Int. J. Ment. Health Nurs. 2010, 19, 240–249. [Google Scholar] [CrossRef]
- Regnerus, M.; Gordon, D.L.; Price, J. Documenting Pornography Use in America: A Comparative Analysis of Methodological Approaches. J. Sex Res. 2015, 53, 873–881. [Google Scholar] [CrossRef] [PubMed]
- Döring, N.; Daneback, K.; Shaughnessy, K.; Grov, C.; Byers, E.S. Online Sexual Activity Experiences among College Students: A Four-Country Comparison. Arch. Sex. Behav. 2015, 46, 1641–1652. [Google Scholar] [CrossRef]
- Jones, A. Camming: Money, Power, and Pleasure in the Sex Work Industry; New York University Press: New York, NY, USA, 2020. [Google Scholar]
- Dekker, A.; Wenzlaff, F.; Biedermann, S.V.; Briken, P.; Fuss, J. VR Porn as “Empathy Machine”? Perception of Self and Others in Virtual Reality Pornography. J. Sex Res. 2020, 58, 273–278. [Google Scholar] [CrossRef]
- Zoledziowski, A. Making Money on OnlyFans is a Lot Harder than You Think. Vice. Available online: https://www.vice.com/en/article/wxeavm/making-money-on-onlyfans-is-a-lot-harder-than-you-think (accessed on 2 April 2020).
- Drolet, G.; O’Neill, S. The Year Sex Work Came Home. New York Times. Available online: www.nytimes.com/2020/04/10/style/camsoda-onlyfans-streaming-sex-coronavirus.html (accessed on 10 April 2020).
- Butler, M.H.; Pereyra, S.A.; Draper, T.W.; Leonhardt, N.D.; Skinner, K.B. Pornography Use and Loneliness: A Bidirectional Recursive Model and Pilot Investigation. J. Sex Marital. Ther. 2017, 44, 127–137. [Google Scholar] [CrossRef] [PubMed]
- Hesse, C.; Floyd, K. Affection substitution: The effect of pornography consumption on close relationships. J. Soc. Pers. Relatsh. 2019, 36, 3887–3907. [Google Scholar] [CrossRef]
- Borgogna, N.C.; Duncan, J.; McDermott, R.C. Is scrupulosity behind the relationship between problematic pornography viewing and depression, anxiety, and stress? Sex. Addict. Compulsivity 2018, 25, 293–318. [Google Scholar] [CrossRef]
- Grubbs, J.; Volk, F.; Exline, J.J.; Pargament, K.I. Internet Pornography Use: Perceived Addiction, Psychological Distress, and the Validation of a Brief Measure. J. Sex Marital. Ther. 2013, 41, 83–106. [Google Scholar] [CrossRef]
- Vanwesenbeeck, I. Psychosexual correlates of viewing sexually explicit sex on television among women in the Netherlands. J. Sex Res. 2001, 38, 361–368. [Google Scholar] [CrossRef]
- Black, D.; Kehrberg, L.L.; Flumerfelt, D.L.; Schlosser, S.S. Characteristics of 36 subjects reporting compulsive sexual behavior. Am. J. Psychiatry 1997, 154, 243–249. [Google Scholar] [CrossRef]
- Kafka, M.P. Update on Paraphilias and Paraphilia-Related Disorders. Curr. Affect. Illn. 1993, 12, 5–13. [Google Scholar]
- Zillmann, D. Transfer of Excitation in Emotional Behavior. In Social Psychophysiology: A Sourcebook; Cacioppo, J.T., Petty, R.E., Eds.; The Guildford Press: New York, NY, USA, 1983. [Google Scholar]
- Bancroft, J.; Janssen, E.; Strong, D.; Carnes, L.; Vukadinovic, Z.; Long, J.S. The Relation between Mood and Sexuality in Heterosexual Men. Arch. Sex. Behav. 2003, 32, 217–230. [Google Scholar] [CrossRef] [PubMed]
- Bancroft, J.; Vukadinovic, Z. Sexual addiction, sexual compulsivity, sexual impulsivity, or what? Toward a theoretical model. J. Sex Res. 2004, 41, 225–234. [Google Scholar] [CrossRef]
- Pilkonis, P.A.; Choi, S.W.; Reise, S.P.; Stover, A.; Riley, W.T.; Cella, D. Item Banks for Measuring Emotional Distress from the Patient-Reported Outcomes Measurement Information System (PROMIS®): Depression, Anxiety, and Anger. Assessment 2011, 18, 263–283. [Google Scholar] [CrossRef] [PubMed]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B.W. Validity of a Brief Depression Severity Measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef]
- MacKinnon, D.P.; Krull, J.L.; Lockwood, C.M. Equivalence of the Mediation, Confounding and Suppression Effect. Prev. Sci. 2000, 1, 173–181. [Google Scholar] [CrossRef]
- Liberati, N. Teledildonics and New Ways of “Being in Touch”. Sci. Eng. Ethics 2016, 23, 801–823. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayes, A.F. Introduction to Mediation, Moderation, and Conditional Process Analysis: A Regression-Based Approach, 2nd ed.; Methodology in the Social Sciences; Guilford Press: New York, NY, USA, 2018. [Google Scholar]
- Cohen, J.; Cohen, P.; West, S.; Aiken, L. Applied Multiple Regression/Correlation Analysis for the Behavioral Sciences, 3rd ed.; Psychology Press: London, UK, 2013. [Google Scholar]
- Eichenberg, C.; Khamis, M.; Hübner, L. The Attitudes of Therapists and Physicians on the Use of Sex Robots in Sexual Therapy: Online Survey and Interview Study. J. Med. Internet Res. 2019, 21, e13853. [Google Scholar] [CrossRef] [Green Version]
- Love, T. Oxytocin, motivation and the role of dopamine. Pharmacol. Biochem. Behav. 2014, 119, 49–60. [Google Scholar] [CrossRef] [Green Version]
- Smith, A.S.; Wang, Z. Hypothalamic Oxytocin Mediates Social Buffering of the Stress Response. Biol. Psychiatry 2013, 76, 281–288. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guidry, R.; Floyd, C.G.; Volk, F.; Moen, C.E. The Exacerbating Impact of Moral Disapproval on the Relationship between Pornography Use and Depression, Anxiety, and Relationship Satisfaction. J. Sex Marital. Ther. 2019, 46, 103–121. [Google Scholar] [CrossRef] [PubMed]
- Perry, S.L. Pornography Use and Depressive Symptoms: Examining the Role of Moral Incongruence. Soc. Ment. Health 2017, 8, 195–213. [Google Scholar] [CrossRef]
- Czeisler, M.; Lane, R.I.; Petrosky, E.; Wiley, J.F.; Christensen, A.; Njai, R.; Weaver, M.D.; Robbins, R.; Facer-Childs, E.R.; Barger, L.K.; et al. Mental Health, Substance Use, and Suicidal Ideation during the COVID-19 Pandemic—United States, June 24–30, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 1049–1057. [Google Scholar] [CrossRef] [PubMed]
- Horigian, V.E.; Schmidt, R.D.; Feaster, D.J. Loneliness, Mental Health, and Substance Use among US Young Adults during COVID-19. J. Psychoact. Drugs 2020, 53, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Müller, F.; Röhr, S.; Reininghaus, U.; Riedel-Heller, S. Social Isolation and Loneliness during COVID-19 Lockdown: Associations with Depressive Symptoms in the German Old-Age Population. Int. J. Environ. Res. Public Health 2021, 18, 3615. [Google Scholar] [CrossRef]

{kind=link}
| Have Used Sextech (n = 5192) | Have Not Used Sextech (n = 2812) | Total Sample (n = 8004) | |
|---|---|---|---|
| Age (Years) | |||
| Mean (SD) | 41.05 (12.5) | 49.68 (11.9) | 44.08 (13.0) |
| Gender identity n (%) | |||
| Male | 3035 (58.5%) | 792 (28.2%) | 3827 (47.8%) |
| Female | 2084 (40.1%) | 2013 (71.6%) | 4097 (51.2%) |
| Non-binary | 60 (1.2%) | 3 (0.1%) | 63 (0.8%) |
| Agender | 6 (0.1%) | 3 (0.1%) | 9 (0.1%) |
| Another Identity | 6 (0.1%) | 1 (0.0%) | 7 (0.1%) |
| Don’t Know | 1 (0.0%) | 0 (0.0%) | 1 (0.0%) |
| Sexual orientation n (%) | |||
| Heterosexual | 4180 (80.5%) | 2675 (95.1%) | 6855 (85.6%) |
| Homosexual/Gay/Lesbian | 432 (8.3%) | 90 (3.2%) | 522 (6.5%) |
| Bisexual | 506 (9.7%) | 33 (1.2%) | 539 (6.7%) |
| Other | 74 (1.4%) | 14 (0.5%) | 88 (1.1%) |
| Race/Ethnicity n (%) | |||
| White | 3195 (61.5%) | 1915 (68.1%) | 5110 (63.8%) |
| Black/African American | 748 (14.4%) | 319 (11.3%) | 1067 (13.3%) |
| South Asian | 92 (1.8%) | 26 (0.9%) | 118 (1.5%) |
| East Asian | 258 (5.0%) | 139 (4.9%) | 397 (5.0%) |
| North American Indian or Alaskan Native or Pacific Islander | 63 (1.2%) | 39 (1.4%) | 102 (1.3%) |
| Hispanic or Latino | 726 (14.0%) | 296 (10.5%) | 1022 (12.8%) |
| Other | 110 (2.1%) | 78 (2.8%) | 188 (2.3%) |
| Current relationship status n (%) | |||
| Single and not seeing anyone | 1479 (28.5%) | 814 (28.9%) | 2293 (28.6%) |
| Casually dating one or more people | 528 (10.2%) | 66 (2.3%) | 594 (7.4%) |
| In a committed relationship | 796 (15.3%) | 258 (9.2%) | 1054 (13.2%) |
| Engaged | 119 (2.3%) | 32 (1.1%) | 151 (1.9%) |
| Married | 2270 (43.7%) | 1642 (58.4%) | 3912 (48.9%) |
| Have Used Sextech (n = 5192) | Have Not Used Sextech (n = 2812) | Total Sample (n = 8004) | |
|---|---|---|---|
| Gender identity and Sexual orientation N (%) | |||
| Heterosexual Male | 2527 (48.7%) | 763 (27.1%) | 3290 (41.1%) |
| Heterosexual Female | 1650 (31.8%) | 1910 (67.9%) | 3536 (44.5%) |
| Homosexual Male | 239 (4.6%) | 11 (0.4%) | 250 (3.1%) |
| Homosexual Female | 171 (3.3%) | 79 (2.8%) | 250 (3.1%) |
| Variable | M1 | SD2 | Minimum | Maximum | α | Frequency (%) |
|---|---|---|---|---|---|---|
| Loneliness 3 | 2.50 | 0.86 | 1 | 5 | 0.87 | |
| Depression 4 | 0.70 | 0.71 | 0 | 3 | 0.91 | |
| Anxiety | 2.10 | 1.05 | 1 | 5 | 0.92 | |
| Sextech use 5 | 1.03 | 1.82 | 1 | 7 | 0.91 | |
| Sexual desire 6 | 4.51 | 1.54 | 1 | 7 | ||
| Sending sexually explicit images or videos 7 | 1.52 | 0.94 | 1 | 5 | 2368 (29.6%) 8 | |
| Visiting a camming site | 1.36 | 0.87 | 1 | 5 | 1481 (18.5%) | |
| Participating in a live camming stream | 1.23 | 0.71 | 1 | 5 | 930 (11.6%) | |
| Coordinated teledildonic accessory usage | 1.20 | 0.68 | 1 | 5 | 756 (9.4%) | |
| Accessing virtual reality (VR) pornography | 1.21 | 0.70 | 1 | 5 | 875 (10.9%) | |
| Playing sexually-explicit role-playing games (RPG) | 1.26 | 0.75 | 1 | 5 | 1108 (13.8%) | |
| Exchanging sexually explicit messages with a chatbot/AI | 1.18 | 0.64 | 1 | 5 | 704 (8.8%) |
| Coefficient | SE | t | p | 95% CI | |
|---|---|---|---|---|---|
| IV to mediators (a paths): | |||||
| Depression (a1) | 0.50 | 0.01 | 67.54 | <0.001 | 0.49, 0.52 |
| Anxiety (a2) | 0.73 | 0.01 | 64.54 | <0.001 | 0.70, 0.75 |
| Mediators to DV (b paths): | |||||
| Depression (b1) | 0.27 | 0.06 | 4.37 | <0.001 | 0.15, 0.39 |
| Anxiety (b2) | 0.03 | 0.04 | 0.77 | 0.44 | −0.05, 0.11 |
| IV to DV (c′ path): | |||||
| Loneliness (c1′) | −0.02 | 0.04 | −0.60 | 0.55 | −0.10, 0.05 |
| Moderators to DV (c′ paths): | |||||
| Sexual Orientation (c2′) | 0.47 | 0.06 | 8.09 | <0.001 | 0.36, 0.58 |
| Gender (c3′) | 0.81 | 0.04 | 20.86 | <0.001 | 0.73, 0.88 |
| Interactions: | |||||
| Depression (M1) × Sexual orientation (V) (b2i) | −0.11 | 0.11 | −0.95 | 0.34 | −0.33, 0.12 |
| Anxiety (M2) × Sexual orientation (V) (b2i) | 0.17 | 0.08 | 2.22 | 0.03 | 0.02, 0.32 |
| Depression (M1) × Gender (Q) (b3i) | 0.34 | 0.08 | 4.09 | <0.001 | 0.18, 0.50 |
| Anxiety (M2) × Gender (Q) (b3i) | 0.28 | 0.05 | 5.17 | <0.001 | 0.17, 0.39 |
| Loneliness (IV) × Sexual orientation (V) (c4′) | −0.25 | 0.08 | −3.07 | <0.001 | −0.41, −0.09 |
| Loneliness (IV) × Gender (Q) (c5′) | −0.15 | 0.06 | −2.70 | 0.01 | −0.26, −0.04 |
| Control Variables: | |||||
| Sexual Desire | 0.12 | 0.01 | 9.25 | <0.001 | 0.09, 0.14 |
| Relationship Status | 0.00 | 0.04 | 0.01 | 0.99 | −0.08, 0.08 |
| Age | −0.03 | 0.00 | −19.00 | <0.001 | −0.03, −0.02 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Marcotte, A.S.; Kaufman, E.M.; Campbell, J.T.; Reynolds, T.A.; Garcia, J.R.; Gesselman, A.N. Sextech Use as a Potential Mental Health Reprieve: The Role of Anxiety, Depression, and Loneliness in Seeking Sex Online. Int. J. Environ. Res. Public Health 2021, 18, 8924. https://doi.org/10.3390/ijerph18178924
Marcotte AS, Kaufman EM, Campbell JT, Reynolds TA, Garcia JR, Gesselman AN. Sextech Use as a Potential Mental Health Reprieve: The Role of Anxiety, Depression, and Loneliness in Seeking Sex Online. International Journal of Environmental Research and Public Health. 2021; 18(17):8924. https://doi.org/10.3390/ijerph18178924
Chicago/Turabian StyleMarcotte, Alexandra S., Ellen M. Kaufman, Jessica T. Campbell, Tania A. Reynolds, Justin R. Garcia, and Amanda N. Gesselman. 2021. "Sextech Use as a Potential Mental Health Reprieve: The Role of Anxiety, Depression, and Loneliness in Seeking Sex Online" International Journal of Environmental Research and Public Health 18, no. 17: 8924. https://doi.org/10.3390/ijerph18178924
APA StyleMarcotte, A. S., Kaufman, E. M., Campbell, J. T., Reynolds, T. A., Garcia, J. R., & Gesselman, A. N. (2021). Sextech Use as a Potential Mental Health Reprieve: The Role of Anxiety, Depression, and Loneliness in Seeking Sex Online. International Journal of Environmental Research and Public Health, 18(17), 8924. https://doi.org/10.3390/ijerph18178924