
Current Update on the Clinical Utility of MMSE and MoCA for Stroke Patients in Asia: A Systematic Review


 ,
,
Abstract
:1. Introduction
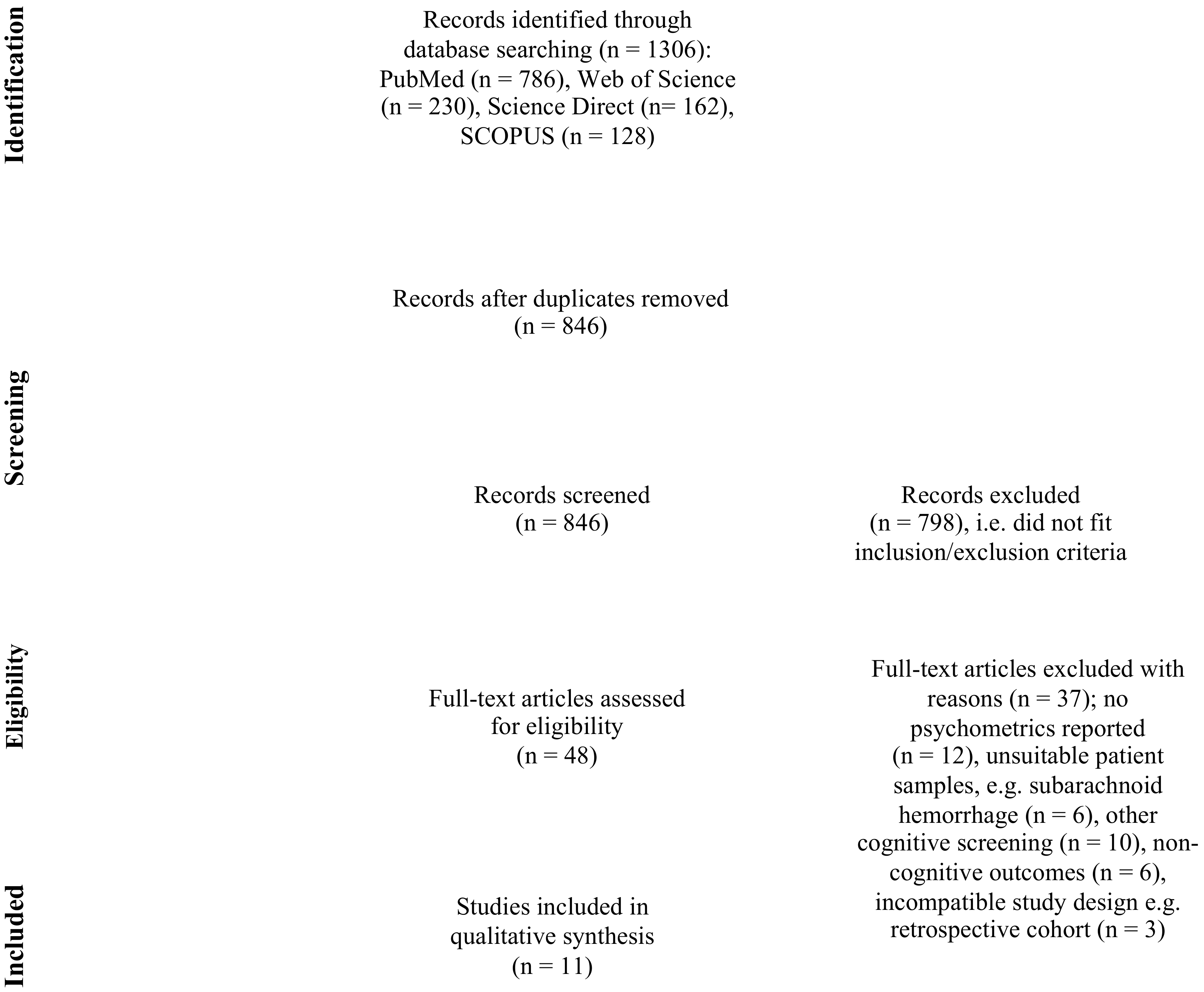
2. Methods
2.1. Brief Description of the MMSE and MoCA
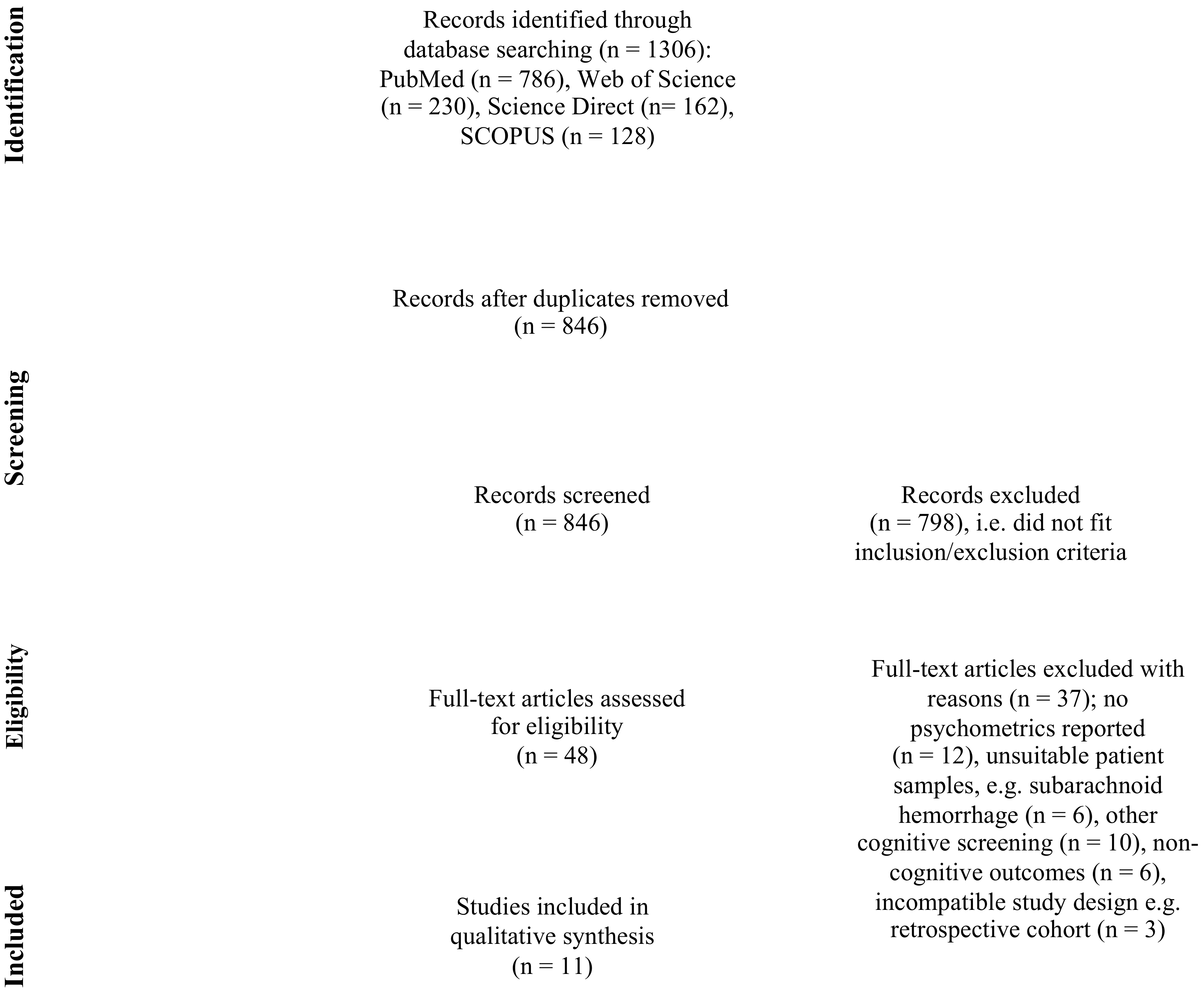
2.2. Search Strategy
2.3. Eligibility Criteria
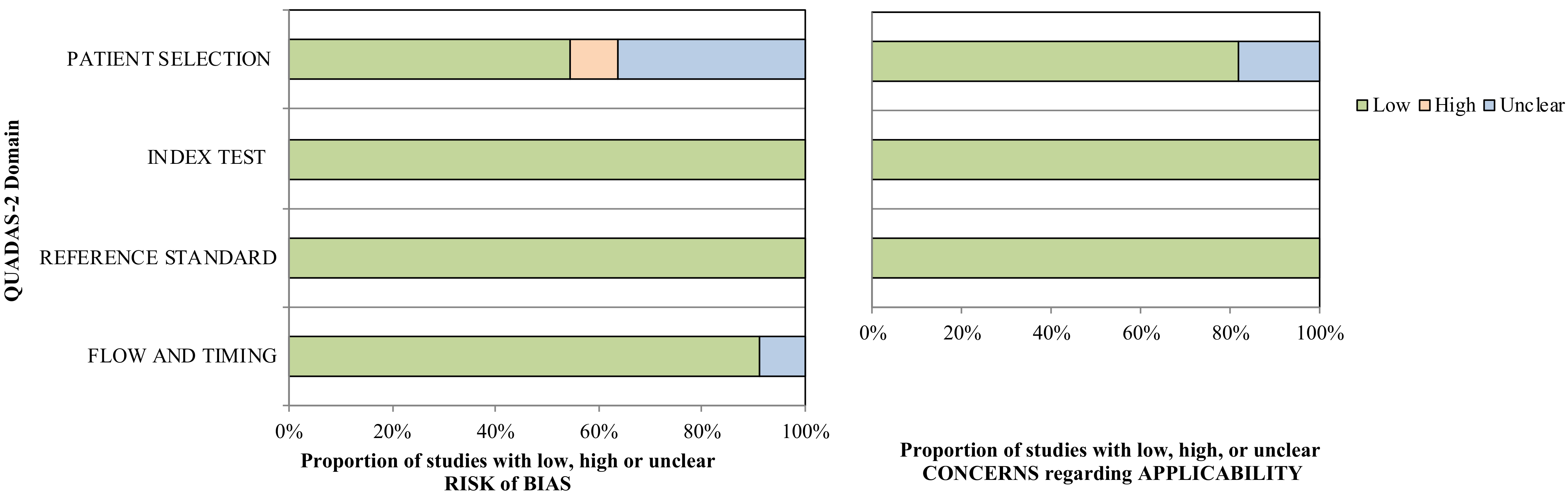
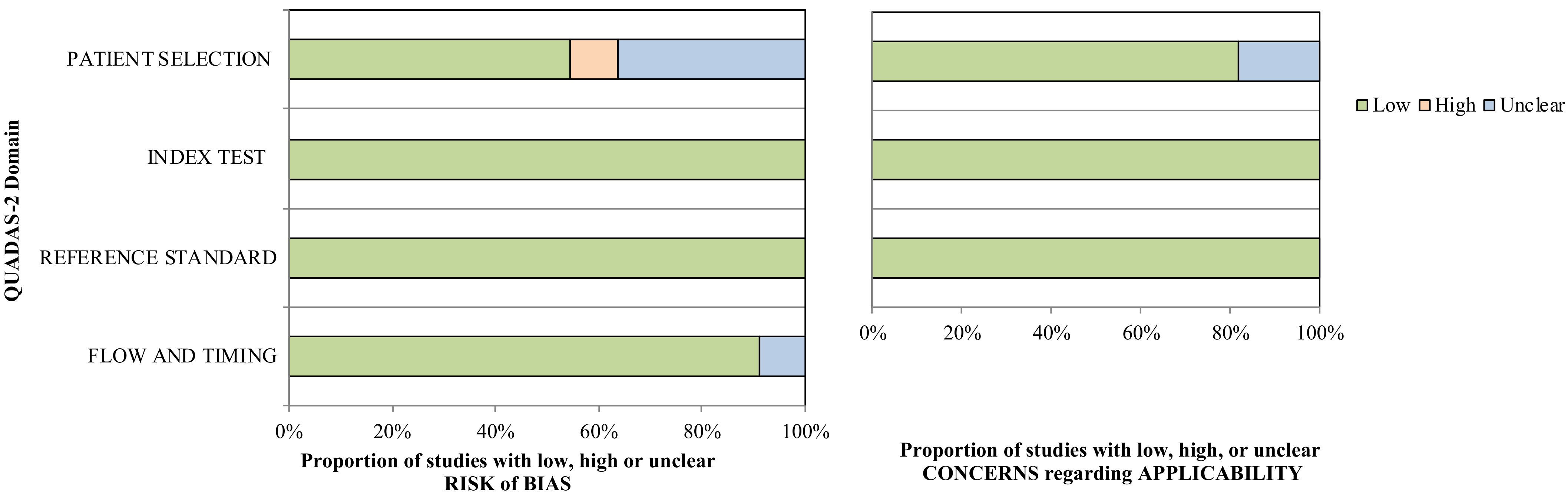
2.4. Quality Assessment
2.5. Data Synthesis
3. Results
3.1. Risk of Bias
3.2. Sample Characteristics
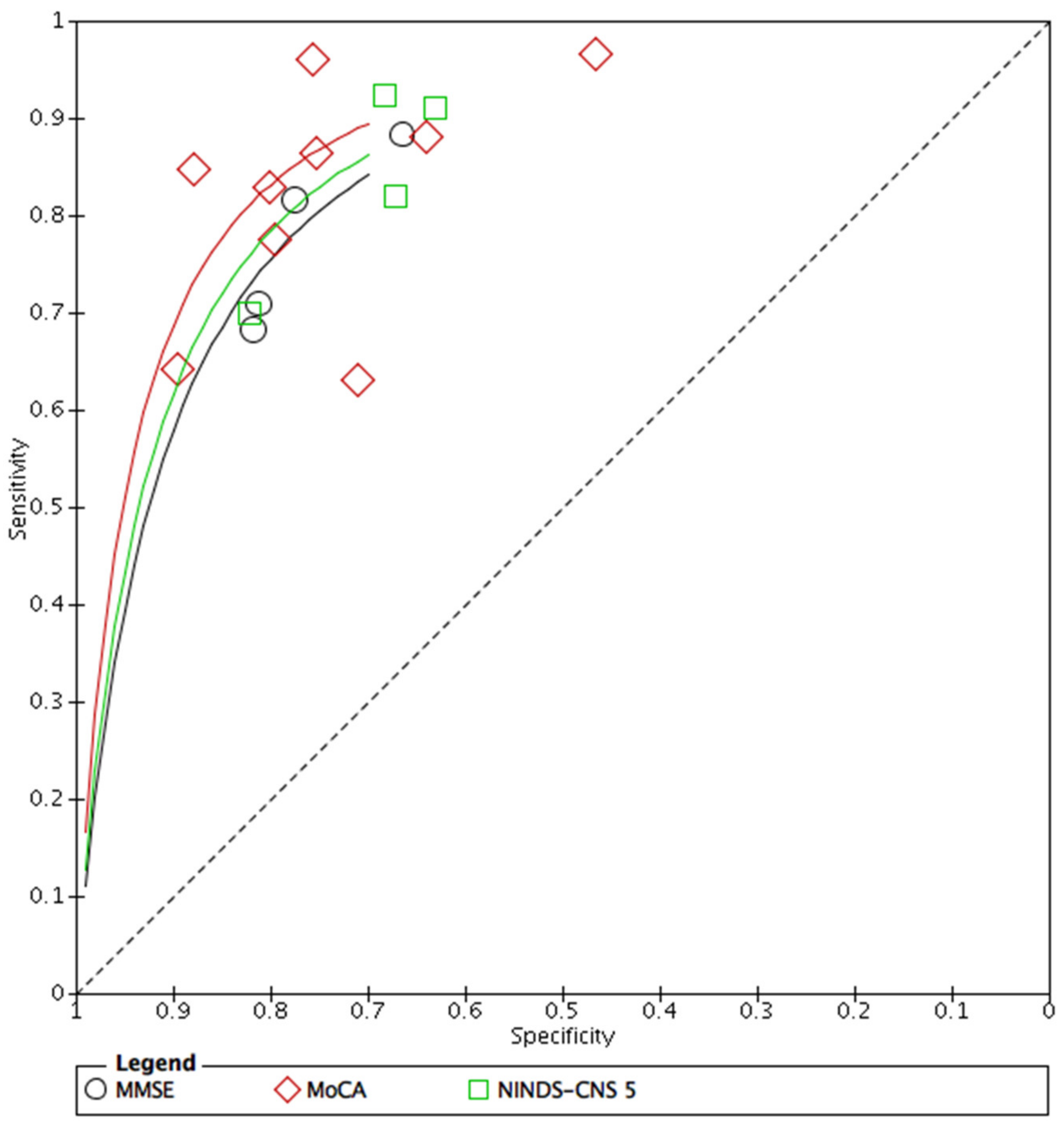
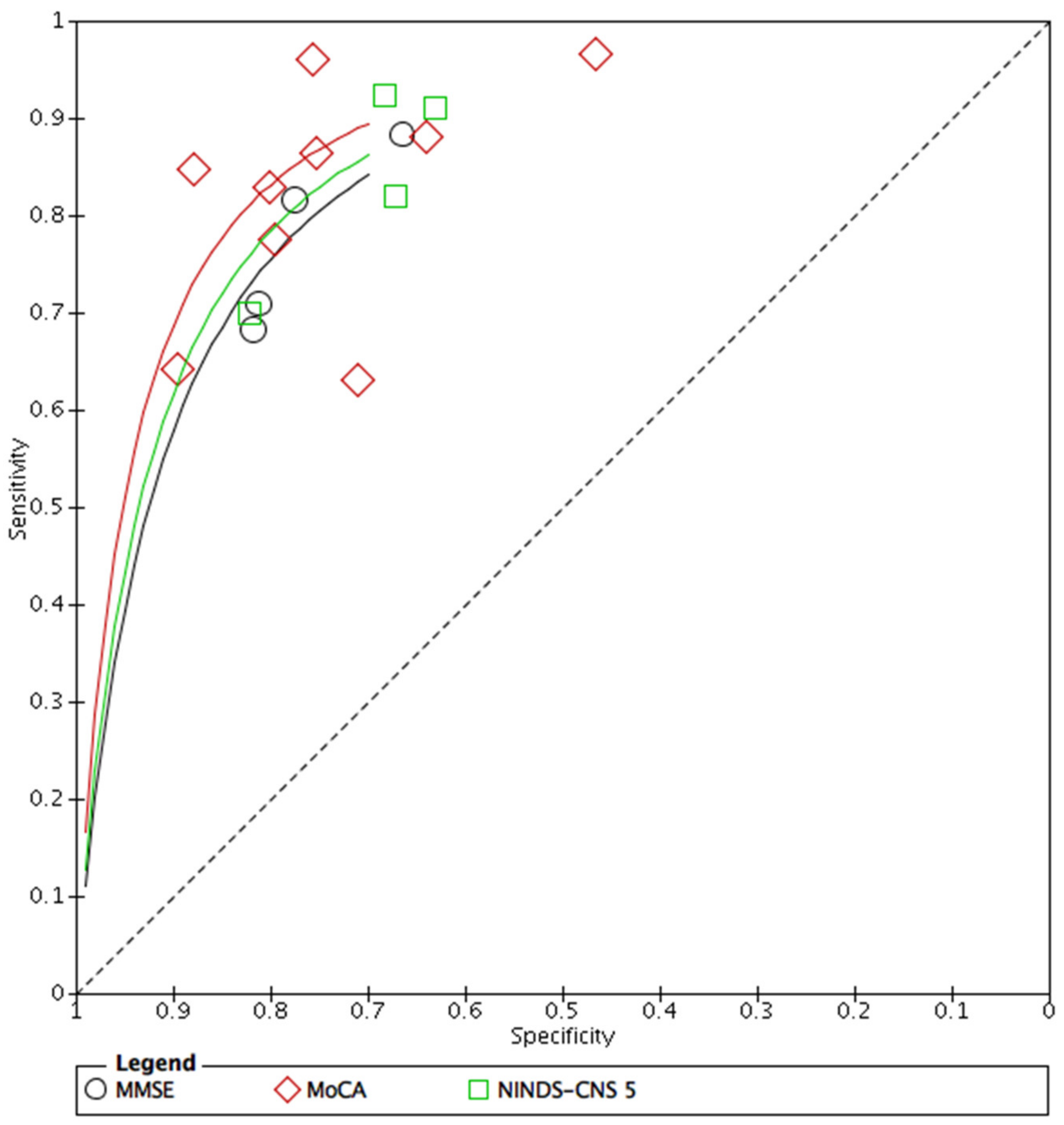
3.3. Analysis
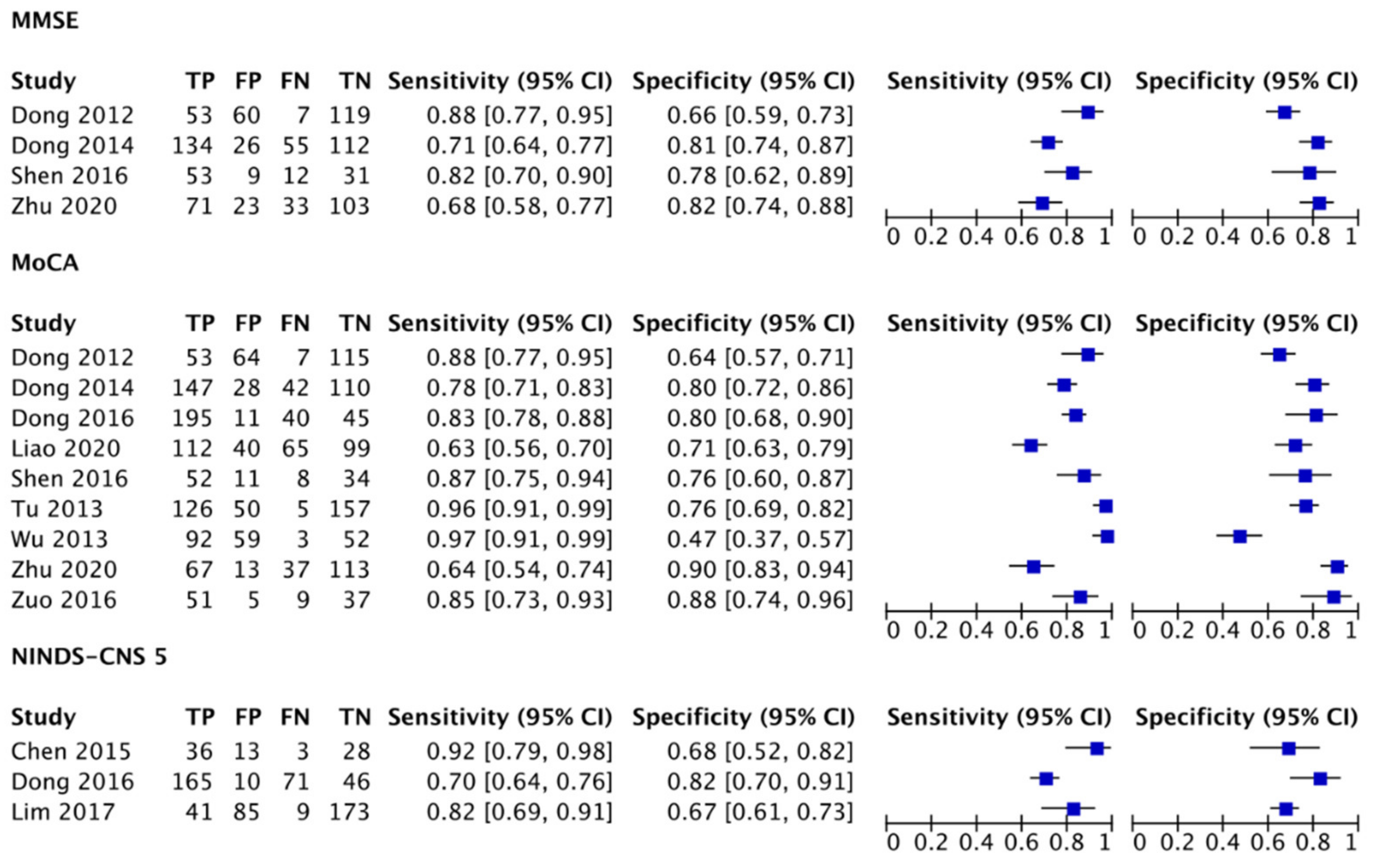
3.4. Detection Accuracy of the MMSE and MoCA
3.5. Covariates
3.5.1. Education
3.5.2. Age
3.5.3. Stroke Characteristics
3.5.4. Time since Stroke
3.5.5. Cognitive Domains
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Pendlebury, S.T.; Rothwell, P.M. Incidence and prevalence of dementia associated with transient ischaemic attack and stroke: Analysis of the population-based Oxford Vascular Study. Lancet Neurol. 2019, 18, 248–258. [Google Scholar] [CrossRef] [Green Version]
- Sexton, E.; McLoughlin, A.; Williams, D.J.; Merriman, N.A.; Donnelly, N.; Rohde, D.; Hickey, A.; Wren, M.A.; Bennett, K. Systematic review and meta-analysis of the prevalence of cognitive impairment no dementia in the first year post-stroke. Eur. Stroke J. 2019, 4, 160–171. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Folstein, M.F.; Folstein, S.E.; McHugh, P.R. "Mini-mental state": A practical method for grading the cognitive state of patients for the clinician. J. Psychiatr. Res. 1975, 12, 189–198. [Google Scholar] [CrossRef]
- Nasreddine, Z.S.; Phillips, N.A.; Bédirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H. The Montreal Cognitive Assessment, MoCA: A brief screening tool for mild cognitive impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef]
- Quinn, T.J.; Elliott, E.; Langhorne, P. Cognitive and mood assessment tools for use in stroke. Stroke 2018, 49, 483–490. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, J.T.; Erkinjuntti, T.; Reisberg, B.; Roman, G.; Sawada, T.; Pantoni, L.; Bowler, J.V.; Ballard, C.; DeCarli, C.; Gorelick, P.B.; et al. Vascular cognitive impairment. Lancet Neurol. 2003, 2, 89–98. [Google Scholar] [CrossRef]
- Sachdev, P.; Kalaria, R.; O’Brien, J.; Skoog, I.; Alladi, S.; Black, S.E.; Blacker, D.; Blazer, D.G.; Chen, C.; Chui, H. Diagnostic criteria for vascular cognitive disorders: A VASCOG statement. Alzheimer Dis. Assoc. Disord. 2014, 28, 206–218. [Google Scholar] [CrossRef] [Green Version]
- Sachdev, P.S.; Brodaty, H.; Valenzuela, M.J.; Lorentz, L.; Looi, J.C.; Wen, W.; Zagami, A.S. The neuropsychological profile of vascular cognitive impairment in stroke and TIA patients. Neurology 2004, 62, 912–919. [Google Scholar] [CrossRef] [PubMed]
- American Psychiatric Association. Diagnostic and Statistical Manual, 5th ed.; DSM-APA: Washington, DC, USA, 2013; pp. 621–624. [Google Scholar]
- Mijajlović, M.D.; Pavlović, A.; Brainin, M.; Heiss, W.D.; Quinn, T.J.; Ihle-Hansen, H.B.; Hermann, D.M.; Assayag, E.B.; Richard, E.; Thiel, A.; et al. Post-stroke dementia a comprehensive review. BMC Med. 2017, 15, 11. [Google Scholar] [CrossRef] [Green Version]
- Demeyere, N.; Riddoch, M.J.; Slavkova, E.D.; Bickerton, W.L.; Humphreys, G.W. The Oxford Cognitive Screen (OCS): Validation of a stroke-specific short cognitive screening tool. Psychol. Ass. 2015, 27, 883–894. [Google Scholar] [CrossRef]
- Demeyere, N.; Riddoch, M.J.; Slavkova, E.D.; Jones, K.; Reckless, I.; Mathieson, P.; Humphreys, G.W. Domain-specific versus generalized cognitive screening in acute stroke. J. Neurol. 2016, 263, 306–315. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rodrigues, J.C.; Becker, N.; Beckenkamp, C.L.; Miná, C.S.; de Salles, J.F.; Bandeira, D.R. Psychometric properties of cognitive screening for patients with cerebrovasculardiseases A systematic review. Dement. Neuropsychol. 2019, 13, 31–43. [Google Scholar] [CrossRef] [Green Version]
- Stolwyk, R.J.; O’Neill, M.H.; McKay, A.J.; Wong, D.K. Are cognitive screening tools sensitive and specific enough for use after stroke? A systematic literature review. Stroke 2014, 45, 3129–3134. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Heugten, C.M.; Walton, L.; Hentschel, U. Can we forget the Mini-Mental State Examination? A systematic review of the validity of cognitive screening instruments within one month after stroke. Clin. Rehab. 2015, 29, 694–704. [Google Scholar] [CrossRef] [PubMed]
- Razali, R.; Jean-Li, L.; Jaffar, A.; Ahmad, M.; Shah, S.A.; Ibrahim, N.; Din, N.C.; Nik Jaafar, N.R.; Midin, M.; Sidi, H. Is the Bahasa Malaysia version of the Montreal Cognitive Assessment (MoCA-BM) a better instrument than the Malay version of the Mini Mental State Examination (M-MMSE) in screening for mild cognitive impairment (MCI) in the elderly? Compr. Psychiatr. 2014, 55, S70–S75. [Google Scholar] [CrossRef]
- Rosli, R.; Tan, M.P.; Gray, W.K.; Subramanian, P.; Chin, A.V. Cognitive assessment tools in Asia: A systematic review. Int. Psychogeriatr. 2016, 28, 189–210. [Google Scholar] [CrossRef]
- Chan, E.; Altendorff, S.; Healy, C.; Werring, D.J.; Cipolotti, L. The test accuracy of the Montreal Cognitive Assessment (MoCA) by stroke lateralisation. J. Neurol. Sci. 2017, 373, 100–104. [Google Scholar] [CrossRef] [PubMed]
- Nys, G.M.; van Zandvoort, M.J.; de Kort, P.L.; Jansen, B.P.; Kappelle, L.J.; de Haan, E.H. Restrictions of the Mini-Mental State Examination in acute stroke. Arch. Clin. Neuropsychol. 2005, 20, 623–629. [Google Scholar] [CrossRef] [Green Version]
- Shim, Y.S.; Yang, D.W.; Kim, H.J.; Park, Y.H.; Kim, S. Characteristic differences in the Mini-Mental State Examination used in Asian countries. BMC Neurol. 2017, 17, 141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, Y.; Zhang, W.; Chen, K.; Feng, S.; Ji, Y.; Shen, J.; Reiman, E.M.; Liu, Y. Arithmetic processing in the brain shaped by cultures. Proc. Natl. Acad. Sci. USA 2006, 103, 10775–10780. [Google Scholar] [CrossRef] [Green Version]
- Chiti, G.; Pantoni, L. Use of Montreal Cognitive Assessment in patients with stroke. Stroke 2014, 45, 3135–3140. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Godefroy, O.; Fickl, A.; Roussel, M.; Auribault, C.; Bugnicourt, J.M.; Lamy, C.; Canaple, S.; Petitnicolas, G. Is the Montreal Cognitive Assessment superior to the Mini-Mental State Examination to detect poststroke cognitive impairment? A study with neuropsychological evaluation. Stroke 2011, 42, 1712–1716. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Suda, S.; Muraga, K.; Ishiwata, A.; Nishimura, T.; Aoki, J.; Kanamaru, T.; Suzuki, K.; Sakamoto, Y.; Katano, T.; Nagai, K.; et al. Early cognitive assessment following acute stroke: Feasibility and comparison between Mini-Mental State Examination and Montreal Cognitive Assessment. J. Stroke Cerebrovasc. Dis. 2020, 29, 104688. [Google Scholar] [CrossRef]
- Tan, H.H.; Xu, J.; Teoh, H.L.; Chan, B.P.; Seet, R.C.; Venketasubramanian, N.; Sharma, V.K.; Chen, C.L.; Dong, Y. Decline in changing Montreal Cognitive Assessment (MoCA) scores is associated with post-stroke cognitive decline determined by a formal neuropsychological evaluation. PLoS ONE 2017, 12, e0173291. [Google Scholar] [CrossRef] [Green Version]
- Xu, Q.; Cao, W.W.; Mi, J.H.; Yu, L.; Lin, Y.; Li, Y.S. Brief screening for mild cognitive impairment in subcortical ischemic vascular disease: A comparison study of the Montreal Cognitive Assessment with the Mini-Mental State Examination. Eur. Neurol. 2014, 71, 106–114. [Google Scholar] [CrossRef]
- Zhang, H.; Zhang, X.N.; Zhang, H.L.; Huang, L.; Chi, Q.Q.; Zhang, X.; Yun, X.P. Differences in cognitive profiles between traumatic brain injury and stroke: A comparison ofthe Montreal Cognitive Assessment and Mini-Mental State Examination. CJT 2016, 19, 271–274. [Google Scholar] [CrossRef]
- Dong, Y.; Sharma, V.K.; Chan, B.P.; Venketasubramanian, N.; Teoh, H.L.; Seet, R.C.; Tanicala, S.; Chan, Y.H.; Chen, C. The Montreal Cognitive Assessment (MoCA) is superior to the Mini-Mental State Examination (MMSE) for the detection of vascular cognitive impairment after acute stroke. J. Neurol. Sci. 2010, 299, 15–18. [Google Scholar] [CrossRef]
- Julayanont, P.; Tangwongchai, S.; Hemrungrojn, S.; Tunvirachaisakul, C.; Phanthumchinda, K.; Hongsawat, J.; Suwichanarakul, P.; Thanasirorat, S.; Nasreddine, Z.S. The Montreal Cognitive Assessment-Basic: A screening tool for mild cognitive impairment in illiterate and low-educated elderly adults. J. Am. Geriatr. Soc. 2015, 63, 2550–2554. [Google Scholar] [CrossRef]
- Ng, T.P.; Feng, L.; Lim, W.S.; Chong, M.S.; Lee, T.S.; Yap, K.B.; Tsoi, T.; Liew, T.M.; Gao, Q.; Collinson, S.; et al. Montreal Cognitive Assessment for screening mild cognitive impairment: Variations in test performance and scores by education in Singapore. Dement. Geriatr. Cogn. Disord. 2015, 39, 176–185. [Google Scholar] [CrossRef]
- Tu, Q.Y.; Jin, H.; Ding, B.R.; Yang, X.; Lei, Z.H.; Bai, S.; Zhang, Y.D.; Tang, X.Q. Reliability, validity, and optimal cutoff score of the montreal cognitive assessment (Changsha version) in ischemic cerebrovascular disease patients of Hunan Province, China. Dement. Geriatr. Cogn. Disord. 2013, 3, 25–36. [Google Scholar] [CrossRef] [PubMed]
- Gómez, F.; Zunzunegui, M.; Lord, C.; Alvarado, B.; García, A. Applicability of the MoCA-S test in populations with little education in Colombia. Int. J. Geriatr. Psychiatr. 2013, 28, 813–820. [Google Scholar] [CrossRef]
- Rossetti, H.C.; Lacritz, L.H.; Hynan, L.S.; Cullum, C.M.; Van Wright, A.; Weiner, M.F. Montreal Cognitive Assessment performance among community-dwelling African Americans. Arch. Clin. Neuropsychol. 2017, 32, 238–244. [Google Scholar] [CrossRef] [Green Version]
- Santoso, L.; Erkkinen, E.; Adon, C. The Montreal Cognitive Assessment may not be and effective screening tool in low income countries with education inequality (P1.278). Neurology 2016, 86, P1. [Google Scholar]
- Wolters, F.J.; Ikram, M.A. Epidemiology of Vascular Dementia. Arterioscler. Thromb. Vasc. Biol. 2019, 39, 1542–1549. [Google Scholar] [CrossRef] [PubMed]
- Hsieh, S.; Schubert, S.; Hoon, C.; Mioshi, E.; Hodges, J.R. Validation of the Addenbrooke’s Cognitive Examination III in frontotemporal dementia and Alzheimer’s disease. Dement. Geriatr. Cogn. Disord. 2013, 36, 242–250. [Google Scholar] [CrossRef] [PubMed]
- Fuh, J.L.; Teng, E.L.; Lin, K.N.; Larson, E.B.; Wang, S.J.; Liu, C.Y.; Chou, P.; Kuo, B.I.; Liu, H.C. The Informant Questionnaire on Cognitive Decline in the Elderly (IQCODE) as a screening tool for dementia for a predominantly illiterate Chinese population. Neurology 1995, 45, 92–96. [Google Scholar] [CrossRef]
- Creavin, S.T.; Wisniewski, S.; Noel-Storr, A.H.; Trevelyan, C.M.; Hampton, T.; Rayment, D.; Thom, V.M.; Nash, K.J.; Elhamoui, H.; Milligan, R.; et al. Mini-Mental State Examination (MMSE) for the detection of dementia in clinically unevaluated people aged 65 and over in community and primary care populations. Cochrane Database Syst. Rev. 2016, 1, CD011145. [Google Scholar] [CrossRef] [Green Version]
- Mancuso, M.; Demeyere, N.; Abbruzzese, L.; Damora, A.; Varalta, V.; Pirrotta, F.; Antonucci, G.; Matano, A.; Caputo, M.; Caruso, M.G.; et al. Using the Oxford Cognitive Screen to Detect Cognitive Impairment in Stroke Patients: A Comparison with the Mini-Mental State Examination. Front. Neurol. 2018, 9, 101. [Google Scholar] [CrossRef] [Green Version]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. PRISMA Group Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef] [Green Version]
- Whiting, P.F.; Rutjes, A.W.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.; Sterne, J.A.; Bossuyt, P.M.; QUADAS-2 Group. QUADAS-2: A revised tool for the quality assessment of diagnostic accuracy studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- The Cochrane Collaboration. Review Manager (RevMan) [Computer Program], Version 5; The Nordic Cochrane Centre, The Cochrane Collaboration: Copenhagen, Denmark, 2014.
- Hachinski, V.; Iadecola, C.; Petersen, R.C.; Breteler, M.M.; Nyenhuis, D.L.; Black, S.E.; Powers, W.J.; De Carli, C.; Merino, J.G.; Kalaria, R.N.; et al. National Institute of Neurological Disorders and Stroke-Canadian Stroke Network vascular cognitive impairment harmonization standards. Stroke 2006, 37, 2220–2241. [Google Scholar] [CrossRef]
- Dong, Y.; Xu, J.; Chan, B.P.; Seet, R.C.; Venketasubramanian, N.; Teoh, H.L.; Sharma, V.K.; Chen, C.L. The Montreal Cognitive Assessment is superior to National Institute of Neurological Disease and Stroke-Canadian Stroke Network 5-minute protocol in predicting vascular cognitive impairment at 1 year. BMC Neurol. 2016, 16, 46. [Google Scholar] [CrossRef] [Green Version]
- Lim, J.S.; Oh, M.S.; Lee, J.H.; Jung, S.; Kim, C.; Jang, M.U.; Lee, S.H.; Kim, Y.J.; Kim, Y.; Park, J.; et al. Prediction of post-stroke dementia using NINDS-CSN 5-minute neuropsychology protocol in acute stroke. Int. Psychogeriatr. 2017, 29, 777–784. [Google Scholar] [CrossRef]
- Jones, C.M.; Athanasiou, T. Summary receiver operating characteristic curve analysis techniques in the evaluation of diagnostic tests. Ann. Thorac. Surg. 2005, 79, 16–20. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Venketasubramanian, N.; Chan, B.P.; Sharma, V.K.; Slavin, M.J.; Collinson, S.L.; Sachdev, P.; Chan, Y.H.; Chen, C.L. Brief screening tests during acute admission in patients with mild stroke are predictive of vascular cognitive impairment 3-6 months after stroke. J. Neurol. Neurosurg. Psychiatr. 2012, 83, 580–585. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dong, Y.; Slavin, M.J.; Chan, B.P.; Venketasubramanian, N.; Sharma, V.K.; Collinson, S.L.; Sachdev, P.S.; Chen, C.L. Improving screening for vascular cognitive impairment at three to six months after mild ischemic stroke and transient ischemic attack. Int. Psychogeriatr. 2014, 26, 787–793. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shen, Y.J.; Wang, W.A.; Huang, F.D.; Chen, J.; Liu, H.Y.; Xia, Y.L.; Han, M.; Zhang, L. The use of MMSE and MoCA in patients with acute ischemic stroke in clinical. Int. J. Neurosci. 2016, 126, 442–447. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Zhao, S.; Fan, Z.; Li, Z.; He, F.; Lin, C.; Topatana, W.; Yan, Y.; Liu, Z.; Chen, Y.; et al. Evaluation of the Mini-Mental State Examination and the Montreal Cognitive Assessment for predicting post-stroke cognitive impairment during the acute phase in Chinese minor stroke patients. Front. Aging Neurosci. 2020, 12, 236. [Google Scholar] [CrossRef]
- Wu, Y.; Wang, M.; Ren, M.; Xu, W. The effects of educational background on Montreal Cognitive Assessment screening for vascular cognitive impairment, no dementia, caused by ischemic stroke. J. Clin. Neurosci. 2013, 20, 1406–1410. [Google Scholar] [CrossRef] [PubMed]
- Chen, X.; Fan, X.; Zhao, L.; Duan, L.; Wang, Z.; Han, Y.; Dai, Q.; Liu, D.; Zhang, X.; Chen, Z.; et al. Telephone-based cognitive screening for stroke patients in China. Int. Psychogeriatr. 2015, 27, 2079–2085. [Google Scholar] [CrossRef]
- Zuo, L.; Dong, Y.; Zhu, R.; Jin, Z.; Li, Z.; Wang, Y.; Zhao, X.; Sachdev, P.; Zhang, W.; Wang, Y. Screening for cognitive impairment with the Montreal Cognitive Assessment in Chinese patients with acute mild stroke and transient ischaemic attack: A validation study. BMJ Open 2016, 6, e011310. [Google Scholar] [CrossRef] [Green Version]
- Brott, T.; Adams, H.P., Jr.; Olinger, C.P.; Marler, J.R.; Barsan, W.G.; Biller, J.; Spilker, J.; Holleran, R.; Eberle, R.; Hertzberg, V. Measurements of acute cerebral infarction: A clinical examination scale. Stroke 1989, 20, 864–870. [Google Scholar] [CrossRef] [Green Version]
- Liao, X.; Zuo, L.; Pan, Y.; Xiang, X.; Meng, X.; Li, H.; Zhao, X.; Wang, Y.; Shi, J.; Wang, Y. Screening for cognitive impairment with the Montreal Cognitive assessment at six months after stroke and transient ischemic attack. Neurol. Res. 2021, 43, 15–21. [Google Scholar] [CrossRef]
- Glymour, M.M.; Chêne, G.; Tzourio, C.; Dufouil, C. Brain MRI markers and dropout in a longitudinal study of cognitive aging: The Three-City Dijon Study. Neurology 2012, 79, 1340–1348. [Google Scholar] [CrossRef] [Green Version]
- Khaligh-Razavi, S.M.; Habibi, S.; Sadeghi, M.; Marefat, H.; Khanbagi, M.; Nabavi, S.M.; Sadeghi, E.; Kalafatis, C. Integrated cognitive sssessment: Speed and accuracy of visual processing as a reliable proxy to cognitive performance. Sci. Rep. 2019, 9, 1102. [Google Scholar] [CrossRef] [Green Version]
- Su, C.Y.; Wuang, Y.P.; Lin, Y.H.; Su, J.H. The role of processing speed in post-stroke cognitive dysfunction. Arch. Clin. Neuropsychol. 2014, 30, 148–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- O’Driscoll, C.; Shaikh, M. Cross-cultural applicability of the Montreal Cognitive Assessment (MoCA): A systematic review. J. Alzheimer’s Dis. 2017, 58, 789–801. [Google Scholar] [CrossRef] [PubMed]
- Elkana, O.; Tal, N.; Oren, N.; Soffer, S.; Ash, E.L. Is the cutoff of the MoCA too high? Longitudinal data from highly educated older adults. J. Geriatr. Psychiatr. Neurol. 2020, 33, 155–160. [Google Scholar] [CrossRef] [PubMed]
- Din, N.C.; Shahar, S.; Zulkifli, B.H.; Razali, R.; Vryn, C.A.; Omar, A. Validation and optimal cut-off scores of the Bahasa Malaysia version of the Montreal Cognitive Assessment (MoCA-BM) for mild cognitive impairment among community dwelling older adults in Malaysia. Sains Malaysiana 2016, 45, 1337–1343. [Google Scholar]
- Gottesman, R.F.; Hillis, A.E. Predictors and assessment of cognitive dysfunction resulting from ischaemic stroke. Lancet Neurol. 2010, 9, 895–905. [Google Scholar] [CrossRef] [Green Version]
- Robotham, R.J.; Riis, J.O.; Demeyere, N. A Danish version of the Oxford cognitive screen: A stroke-specific screening test as an alternative to the MoCA. Neuropsychol. Dev. Cogn. 2020, 27, 52–65. [Google Scholar] [CrossRef]
- Levine, D.A.; Wadley, V.G.; Langa, K.M.; Unverzagt, F.W.; Kabeto, M.U.; Giordani, B.; Howard, G.; Howard, V.J.; Cushman, M.; Judd, S.E.; et al. Risk factors for poststroke cognitive decline: The REGARDS study (Reasons for Geographic and Racial Differences in Stroke). Stroke 2018, 49, 987–994. [Google Scholar] [CrossRef] [PubMed]
- Freitas, S.; Simões, M.R.; Alves, L.; Santana, I. Montreal Cognitive Assessment: Influence of sociodemographic and health variables. Archv. Clin. Neuropsych. 2012, 27, 165–175. [Google Scholar] [CrossRef]
- Pendlebury, S.T.; Mariz, J.; Bull, L.; Mehta, Z.; Rothwell, P.M. MoCA, ACE-R, and MMSE versus the National Institute of Neurological Disorders and Stroke-Canadian Stroke Network Vascular Cognitive Impairment Harmonization Standards Neuropsychological Battery after TIA and stroke. Stroke 2012, 43, 464–469. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tang, W.K.; Chan, S.S.; Chiu, H.F.; Wong, K.S.; Kwok, T.C.; Mok, V.; Ungvari, G.S. Can IQCODE detect poststroke dementia? Int. J. Geriatr. Psychiatr. 2003, 18, 706–710. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, R.E.; Wadley, V.G.; McClure, L.A.; Letter, A.J.; Unverzagt, F.W.; Crowe, M.; Nyenhius, D.; Kelley, B.J.; Kana, B.; Marceaux, J.; et al. Performance of the NINDS-CSN 5-minute protocol in a national population-based sample. JINS 2014, 20, 856–867. [Google Scholar] [CrossRef] [Green Version]
- Hong, W.J.; Tao, J.; Wong, A.; Yang, S.L.; Leung, M.T.; Lee, T.; Demeyere, N.; Lau, S.; Chien, C.W.; Chan, C.; et al. Psychometric Properties of the Chinese (Putonghua) Version of the Oxford Cognitive Screen (OCS-P) in Subacute Poststroke Patients without Neglect. BioMed Res. Int. 2018, 6827854. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kong, A.P.; Lam, P.H.; Ho, D.W.; Lau, J.K.; Humphreys, G.W.; Riddoch, J.; Weekes, B. The Hong Kong version of the Oxford Cognitive Screen (HK-OCS): Validation study for Cantonese-speaking chronic stroke survivors. Neuropsych. Dev. Cogn. B Aging Neuropsychol. Cogn. 2016, 23, 530–548. [Google Scholar] [CrossRef]
- Khaw, J.; Subramaniam, P.; Abdul Aziz, N.A.; Wan Asyraf, W.Z.; Raymond, A.A.; Ghazali, S.E. The Oxford Cognitive Screen Malay: Validation of Stroke-Specific Cognitive Screening Test Pilot Study. Master’s Thesis, The National University of Malaysia (UKM), Kuala Lumpur, Malaysia, 2021. Manuscript in Preparation. [Google Scholar]
- Desmond, D.W. The neuropsychology of vascular cognitive impairment: Is there a specific cognitive deficit? J. Neurol. Sci. 2004, 226, 3–7. [Google Scholar] [CrossRef] [PubMed]
- Lees, R.; Broomfield, N.M. Post-stroke cognitive screening: The good, the bad and the unknown. Int. J. Ther. Rehab. 2014, 21, 8–9. [Google Scholar] [CrossRef]
- Cramer, S.C. Repairing the human brain after stroke: I. Mechanisms of spontaneous recovery. Ann. Neurol. 2008, 63, 272–287. [Google Scholar] [CrossRef]
- Alladi, S.; Bak, T.H.; Duggirala, V.; Surampudi, B.; Shailaja, M.; Shukla, A.K.; Chaudhuri, J.R.; Kaul, S. Bilingualism delays age at onset of dementia, independent of education and immigration status. Neurology 2013, 81, 1938–1944. [Google Scholar] [CrossRef]
- Alladi, S.; Bak, T.H.; Mekala, S.; Rajan, A.; Chaudhuri, J.R.; Mioshi, E.; Krovvidi, R.; Surampudi, B.; Duggirala, V.; Kaul, S. Impact of bilingualism on cognitive outcome after stroke. Stroke 2016, 47, 258–261. [Google Scholar] [CrossRef] [Green Version]
- Bialystok, E.; Craik, F.I.; Luk, G. Bilingualism: Consequences for mind and brain. Trends Cogn. Sci. 2012, 16, 240–250. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.; Jeon, S.G.; Nam, Y.; Kim, H.S.; Yoo, D.H.; Moon, M. Bilingualism for dementia: Neurological mechanisms associated with functional and structural changes in the brain. Front. Neurosci. 2019, 13, 1224. [Google Scholar] [CrossRef] [PubMed]
- Perani, D.; Abutalebi, J. Bilingualism, dementia, cognitive and neural reserve. Curr. Opin. Neurol. 2015, 28, 618–625. [Google Scholar] [CrossRef] [PubMed]
- Qiu, C.; Fratiglioni, L. A major role for cardiovascular burden in age-related cognitive decline. Nat. Rev. Cardiol. 2015, 12, 267–277. [Google Scholar] [CrossRef]
- Larner, A.J. Screening utility of the Montreal Cognitive Assessment (MoCA): In place of or as well as the MMSE? Int. Psychogeriatr. 2012, 24, 391–396. [Google Scholar] [CrossRef] [PubMed]
- Trevethan, R. Sensitivity, Specificity, and Predictive Values: Foundations, Pliabilities, and Pitfalls in Research and Practice. Front. Public Health 2017, 5, 307. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| MMSE | |||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Study | Disease | Language | Study Design | Sample Size | Age | Education | NIHSS | Time Since Stroke | Cutoffs | Sensitivity (95% CI) | Specificity (95% CI) | PPV | NPV |
| (%) | (%) | ||||||||||||
| Dong 2012 | VCI | Preference | Prospective | 239 | 67.9 * | 5.7 * | 1 to 4 | 3 days | ≤25/26 | 0.88 (0.77, 0.95) | 0.66 (0.59, 0.73) | 47 | 94 |
| Dong 2014 | VCI | Preference | Prospective | 400 | 64.3 * | 6.3 * | 0 to 1 | 2.4–3.4 months | ≤26 | 0.71 (0.64, 0.77) | 0.81 (0.74, 0.87) | 84 | 67 |
| Shen 2016 | VCI-ND | Mandarin | Case–control | 104 | 70.6 * | 8.7 | 3.16 | ≤14 days | ≤27/28 | 0.82 (0.70, 0.90) | 0.78 (0.62, 0.89) | 82 | 78 |
| Zhu 2020 | VCI | Mandarin | Prospective | 229 | 63.8 | 6* | 1 | ≤14 days | ≤27 | 0.68 (0.58, 0.77) | 0.82 (0.74, 0.88) | 71 | 23 |
| MoCA | |||||||||||||
| Dong 2012 | VCI | Preference | Prospective | 239 | 67.9 * | 5.7 * | 1 to 4 | 3 days | ≤21/22 | 0.88 (0.77, 0.95) | 0.64 (0.57, 0.71) | 45 | 94 |
| Tu 2013 | VCI-ND, VD | Changsha | Case–control | 470 | 69.4–73.2 | 6.3–8.1 * | ? | ≥3 months? | ≤26/27 | 0.96 (0.91, 0.99) | 0.76 (0.69, 0.82) | 86 | 93 |
| Wu 2013 | VCI-ND | Mandarin | Case-control | 206 | 68.1 | 8.65 | ? | Acute? | 22/23 | 0.97 (0.91, 0.99) | 0.47 (0.37, 0.57) | N/A | N/A |
| Dong 2014 | VCI | Preference | Prospective | 400 | 64.3 * | 6.3 * | 0 to 1 | 2.4–3.4 months | ≤23 | 0.78 (0.71, 0.83) | 0.80 (0.72, 0.86) | 84 | 72 |
| Dong 2016 | VCI-ND | Preference | Prospective | 291 | 68.4 * | 5.5* | 1 to 4 | 2.6–4 days | ≤20/21 | 0.83 (0.78, 0.88) | 0.80 (0.68, 0.90) | 50 | 95 |
| Shen 2016 | VCI-ND | Mandarin | Case–control | 104 | 70.6 * | 8.7 | 3.16 | ≤14 days | ≤23/24 | 0.87 (0.75, 0.94) | 0.76 (0.60, 0.87) | 86 | 75 |
| Zuo 2016 | VCI | Mandarin | Case–control | 102 | 58.3 * | Level * | 1 | 10 days | ≤22/23 | 0.85 (0.73, 0.93) | 0.88 (0.74, 0.96) | 91 | 80 |
| Liao 2021 | VCI | Mandarin | Case–control | 316 | 61.1 * | Level * | 2 | 6 months | ≤24 | 0.63 (0.56, 0.70) | 0.71 (0.63, 0.79) | 74 | 60 |
| Zhu 2020 | VCI | Changsha | Prospective | 229 | 63.8 | 6 * | 1 | ≤14 days | ≤21 | 0.64 (0.54, 0.74) | 0.90 (0.83, 0.94) | N/A | N/A |
| NINDS- | |||||||||||||
| CNS 5 | |||||||||||||
| Chen 2015 | VCI | Mandarin | Case–control | 80 | 62.9 | 7.2 * | 2 | 10 months | 24 | 0.92 (0.79, 0.98) | 0.68 (0.52, 0.82) | 73 | 90 |
| Dong 2016 | VCI-ND | Preference | Prospective | 291 | 68.4 * | 5.5 * | 1 to 4 | 2.6–4 days | ≤7/8 | 0.70 (0.64, 0.76) | 0.82 (0.70, 0.91) | 49 | 92 |
| Lim 2017 | VD | Korean | Prospective | 308 | 69.1 * | Level | 5 | 3 months | ≤6/7 | 0.82 (0.69, 0.91) | 0.67 (0.61, 0.73) | 33 | 95 |
| Wei 2020 | VCI | Mandarin | Case–control | 2989 | 63 | Level | 1.16 | 1–2 months | ≤10 | 0.91 (0.89,0.92) | 0.63 (0.60, 0.65) | 71 | 87 |
| MMSE | ||||
|---|---|---|---|---|
| Study | Adjusted | Additional One Point | Method | Notes |
| Dong 2012 | Yes | < primary level education | Regression | Cutoff scores did not differ between patients with lower (≤6 years) and higher educational levels |
| Dong 2014 | Yes | < primary level education | ROC analysis | Cited lack of education stratification for cutoff as study limitation |
| Shen 2016 | No | <12 years | Due to small sample size | |
| Zhu 2020 | Yes | <6 years | ROC analysis | |
| MoCA | ||||
| Dong 2012 | Yes | < primary level education | ROC analysis | Cutoff scores did not differ between patients with lower (≤6 years) and higher educational levels |
| Tu 2013 | No | Regression analysis showed education’s effect | ||
| Wu 2013 | Yes | <12 years | Cutoff scores stratified by education level | Not education-adjusted MoCA ≤ 22/23 Education ≤ 6 years MoCA ≤ 15 Education 6–12 years MoCA ≤ 22 Education > 12 years MoCA ≤ 23 |
| Dong 2014 | Yes | < primary level education | ROC analysis | Cited lack of education stratification for cutoff as study limitation |
| Dong 2016 | Yes | < primary level education | ROC analysis | Education-adjustment did not affect cutoff scores |
| Shen 2016 | No | <12 years | Cutoff scores not adjusted for education | |
| Zuo 2016 | No | <12 years | Authors recommended education-adjusted cutoff scores for future studies | |
| Liao 2020 | No | <12 years | Authors recommended education-adjusted cutoff scores for future studies | |
| Zhu 2020 | Yes | <6 years | ROC analysis | MoCA is more suitable for educated individuals |
| NINDS-CNS 5 | ||||
| Chen 2015 | Yes | Not applicable | Analysis of variance | Cutoff scores not adjusted for education |
| Dong 2016 | Yes | Not applicable | ROC analysis | Education-adjustment did not affect cutoff scores |
| Lim 2017 | Yes | Not applicable | Logistic regression | Categorized education as ≤6 years vs. >6 years |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Khaw, J.; Subramaniam, P.; Abd Aziz, N.A.; Ali Raymond, A.; Wan Zaidi, W.A.; Ghazali, S.E. Current Update on the Clinical Utility of MMSE and MoCA for Stroke Patients in Asia: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 8962. https://doi.org/10.3390/ijerph18178962
Khaw J, Subramaniam P, Abd Aziz NA, Ali Raymond A, Wan Zaidi WA, Ghazali SE. Current Update on the Clinical Utility of MMSE and MoCA for Stroke Patients in Asia: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(17):8962. https://doi.org/10.3390/ijerph18178962
Chicago/Turabian StyleKhaw, Julia, Ponnusamy Subramaniam, Noor Azah Abd Aziz, Azman Ali Raymond, Wan Asyraf Wan Zaidi, and Shazli Ezzat Ghazali. 2021. "Current Update on the Clinical Utility of MMSE and MoCA for Stroke Patients in Asia: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 17: 8962. https://doi.org/10.3390/ijerph18178962
APA StyleKhaw, J., Subramaniam, P., Abd Aziz, N. A., Ali Raymond, A., Wan Zaidi, W. A., & Ghazali, S. E. (2021). Current Update on the Clinical Utility of MMSE and MoCA for Stroke Patients in Asia: A Systematic Review. International Journal of Environmental Research and Public Health, 18(17), 8962. https://doi.org/10.3390/ijerph18178962