
Immunological Traits of Patients with Coexistent Inflammatory Bowel Disease and Periodontal Disease: A Systematic Review




Abstract
1. Introduction
2. Materials and Methods
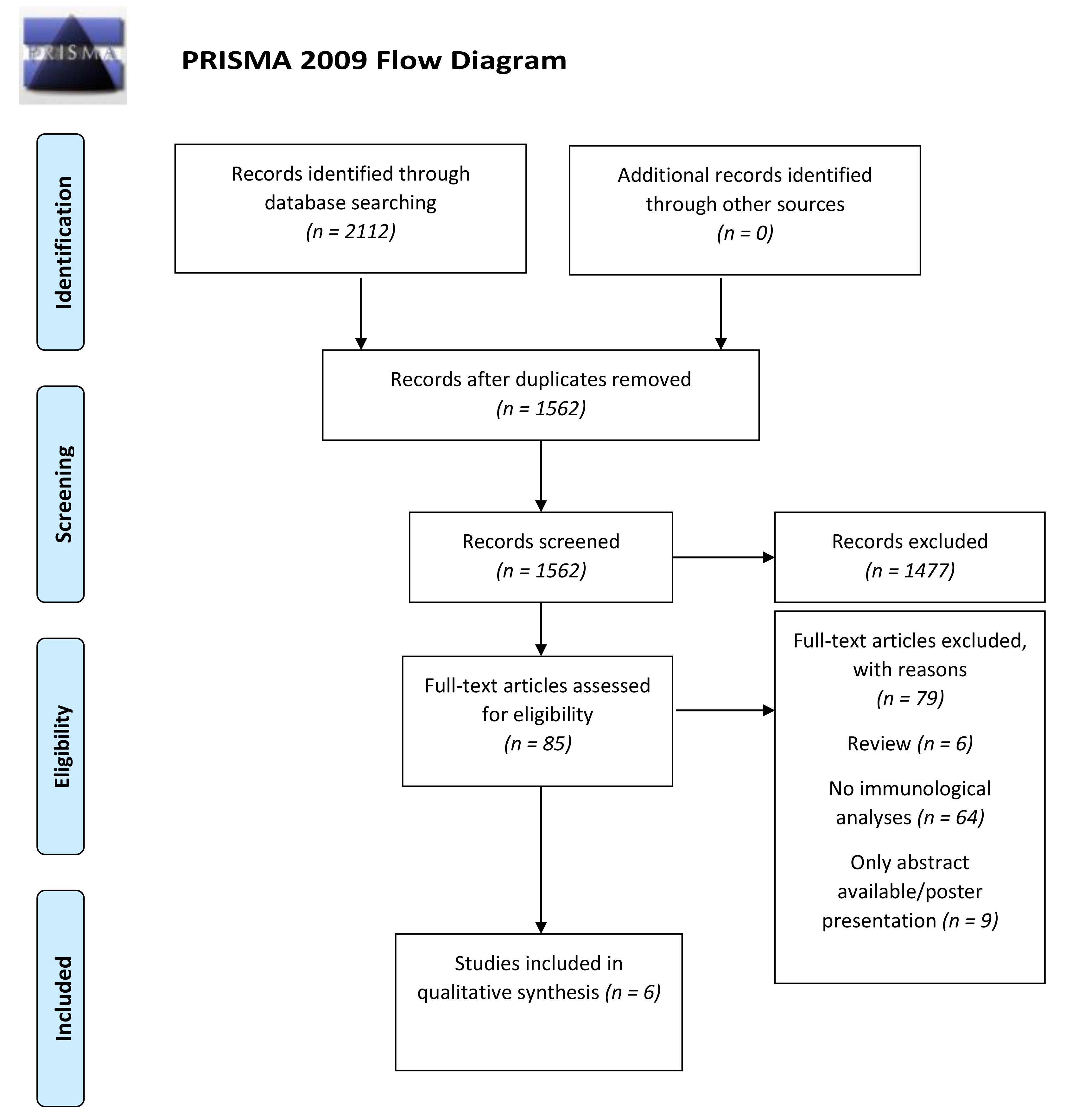
2.1. Literature Search Strategy
2.2. Focus Question
- Population: IBD patients, periodontal disease patients and patients with both diseases
- Exposure/Intervention: Coexistence of periodontal disease and IBD
- Comparison: Subjects with solely IBD or periodontal disease or healthy controls
- Outcomes: Immunological evaluation
2.3. Inclusion Criteria
2.4. Exclusion Criteria
2.5. Assessment of Bias within Studies
3. Results
3.1. Background Characteristics of the Included Studies
3.2. Results from Individual Studies
- Immunological changes in GCF
- Systemic Immunological changes
- Salivary changes in patients with IBD and periodontitis
- Subdivision of IBD patients with periodontitis into Ulcerative colitis and Crohn’s disease
- Immunological changes in gingival and intestinal tissues
3.3. Risk of Bias (Quality Assessment)
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- de Souza, H.S.; Fiocchi, C. Immunopathogenesis of IBD: Current state of the art. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 13–27. [Google Scholar] [CrossRef]
- Fróes, R.S.B.; Carvalho, A.T.P.; Carneiro, A.J.d.V.; de Barros Moreira, A.M.D.; Moreira, J.L.P.; de Souza, H.S. The socio-economic impact of work disability due to inflammatory bowel disease in Brazil. Eur. J. Health Econ. 2018, 19, 463–470. [Google Scholar] [CrossRef]
- Froes, R.d.S.B.; Carvalho, A.T.P.; Carneiro, A.J.d.V.; de Barros Moreira, A.M.D.; Moreira, J.L.P.; de Souza, H.S. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: A systematic review of population-based studies. Lancet 2017, 390, 2769–2778. [Google Scholar]
- Zhang, Y.; Qiao, D.; Chen, R.; Zhu, F.; Gong, J.; Yan, F. The Association between Periodontitis and Inflammatory Bowel Disease: A Systematic Review and Meta-analysis. BioMed Res. Int. 2021, 2021, 1–8. [Google Scholar] [CrossRef]
- Tan, C.X.W.; Brand, H.S.; Kalender, B.; De Boer, N.K.H.; Forouzanfar, T.; de Visscher, J.G.A.M. Dental and periodontal disease in patients with inflammatory bowel disease. Clin. Oral Investig. 2021, 25, 5273–5280. [Google Scholar] [CrossRef] [PubMed]
- Lorenzo-Pouso, A.I.; Castelo-Baz, P.; Rodriguez-Zorrilla, S.; Perez-Sayans, M.; Vega, P. Association between periodontal disease and inflammatory bowel disease: A systematic review and me-ta-analysis. Acta Odontol. Scand. 2021, 79, 344–353. [Google Scholar] [CrossRef]
- Papageorgiou, S.N.; Hagner, M.; Nogueira, A.V.B.; Franke, A.; Jäger, A.; Deschner, J. Inflammatory bowel disease and oral health: Systematic review and a meta-analysis. J. Clin. Periodontol. 2017, 44, 382–393. [Google Scholar] [CrossRef] [PubMed]
- Agossa, K.; Roman, L.; Gosset, M.; Yzet, C.; Fumery, M. Periodontal and dental health in inflammatory bowel diseases: A systematic review. Expert Rev. Gastroenterol. Hepatol. 2021, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Papapanou, P.N.; Sanz, P.; Buduneli, N.; Dietrich, T.; Feres, M.; Fine, D.H.; Flemming, T.F.; Garcia, R.; Giannobile, W.V.; Graziani, F.; et al. Periodontitis: Consensus report of workgroup 2 of the 2017 World Workshop on the Classification of Periodontal and Peri-Implant Diseases and Conditions. J. Periodontol. 2018, 89, S173–S182. [Google Scholar] [CrossRef] [PubMed]
- Bernabe, E.; Marcenes, W.; Hernandez, C.; Bailey, J.; Abreu, L.; Alipour, V.; Amini, S.; Arabloo, J.; Arefi, Z.; Arora, A.; et al. Global, Regional, and National Levels and Trends in Burden of Oral Conditions from 1990 to 2017: A Systematic Analysis for the Global Burden of Disease 2017 Study. J. Dent. Res. 2020, 99, 362–373. [Google Scholar] [CrossRef]
- Vos, T.; Abajobir, A.A.; Abate, K.H.; Abbafati, C.; Abbas, K.M.; Abd-Allah, F.; Abdulkader, R.S.; Abdulle, A.M.; Abebo, T.A.; Abera, S.F.; et al. Global, regional, and national incidence, prevalence, and years lived with disability for 328 diseases and injuries for 195 countries, 1990–2016: A systematic analysis for the Global Burden of Disease Study 2016. Lancet 2017, 390, 1211–1259. [Google Scholar] [CrossRef]
- Cekici, A.; Kantarci, A.; Hasturk, H.; Van Dyke, T.E. Inflammatory and immune pathways in the pathogenesis of periodontal disease. Periodontology 2000 2013, 64, 57–80. [Google Scholar] [CrossRef]
- Van Dyke, T.E.; Bartold, P.M.; Reynolds, E.C. The Nexus between Periodontal Inflammation and Dysbiosis. Front. Immunol. 2020, 11, 511. [Google Scholar] [CrossRef]
- Byrd, K.M.; Gulati, A.S. The Gum-Gut Axis in Inflammatory Bowel Diseases: A Hypothesis-Driven Review of Associations and Advances. Front. Immunol. 2021, 12, 620124. [Google Scholar] [CrossRef]
- Fujino, S.; Andoh, A.; Bamba, S.; Ogawa, A.; Hata, K.; Araki, Y.; Bamba, T.; Fujiyama, Y. Increased expression of interleukin 17 in inflammatory bowel disease. Gut 2003, 52, 65–70. [Google Scholar] [CrossRef] [PubMed]
- Garber, A.; Regueiro, M. Extraintestinal Manifestations of Inflammatory Bowel Disease: Epidemiology, Etiopathogenesis, and Management. Curr. Gastroenterol. Rep. 2019, 21, 31. [Google Scholar] [CrossRef] [PubMed]
- Komatsu, M.; Kobayashi, D.; Saito, K.; Furuya, D.; Yagihashi, A.; Araake, H.; Tsuji, N.; Sakamaki, S.; Niitsu, Y.; Watanabe, N. Tumor necrosis factor-alpha in serum of patients with inflammatory bowel disease as measured by a highly sensitive immuno-PCR. Clin. Chem. 2001, 47, 1297–1301. [Google Scholar] [CrossRef] [PubMed]
- Hajishengallis, G.; Chavakis, T. Local and systemic mechanisms linking periodontal disease and inflammatory comorbidities. Nat. Rev. Immunol. 2021, 21, 426–440. [Google Scholar] [CrossRef]
- Loos, B.G. Systemic Markers of Inflammation in Periodontitis. J. Periodontol. 2005, 76, 2106–2115. [Google Scholar] [CrossRef]
- Paraskevas, S.; Huizinga, J.D.; Loos, B.G. A systematic review and meta-analyses on C-reactive protein in relation to periodontitis. J. Clin. Periodontol. 2008, 35, 277–290. [Google Scholar] [CrossRef] [PubMed]
- Lira-Junior, R.; Figueredo, C.M. Periodontal and inflammatory bowel diseases: Is there evidence of complex pathogenic interactions? World J. Gastroenterol. 2016, 22, 7963–7972. [Google Scholar] [CrossRef]
- Kitamoto, S.; Nagao-Kitamoto, H.; Jiao, Y.; Gillilland, M.G.; Hayashi, A.; Imai, J.; Sugihara, K.; Miyoshi, M.; Brazil, J.C.; Kuffa, P.; et al. The Intermucosal Connection between the Mouth and Gut in Commensal Pathobiont-Driven Colitis. Cell 2020, 182, 447–462.e14. [Google Scholar] [CrossRef]
- Baima, G.; Massano, A.; Squillace, E.; Caviglia, G.P.; Buduneli, N.; Ribaldone, D.G.; Aimetti, M. Shared microbiological and immunological patterns in periodontitis and IBD: A scoping review. Oral Dis. 2021. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. The PRISMA Group Preferred Reporting Items for Systematic Reviews and Meta-Analyses: The PRISMA Statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Zhao, D.; Khawaja, A.T.; Jin, L.; Li, K.-Y.; Tonetti, M.; Pelekos, G. The directional and non-directional associations of periodontitis with chronic kidney disease: A systematic review and meta-analysis of observational studies. J. Periodontal Res. 2018, 53, 682–704. [Google Scholar] [CrossRef] [PubMed]
- Chambrone, L.; Guglielmetti, M.R.; Pannuti, C.M.; Chambrone, L.A. Evidence grade associating periodontitis to preterm birth and/or low birth weight: I. A systematic review of prospective cohort studies. J. Clin. Periodontol. 2011, 38, 795–808. [Google Scholar] [CrossRef]
- Van Dyke, T.E.; Dowell, V.R.; Offenbacher, S.; Snyder, W.; Hersh, T. Potential role of microorganisms isolated from periodontal lesions in the pathogenesis of inflammatory bowel disease. Infect. Immun. 1986, 53, 671–677. [Google Scholar] [CrossRef] [PubMed]
- Figueredo, C.M.; Brito, F.; Barros, F.C.; Menegat, J.S.B.; Pedreira, R.R.; Fischer, R.G.; Gustafsson, A. Expression of cytokines in the gingival crevicular fluid and serum from patients with inflammatory bowel disease and untreated chronic periodontitis. J. Periodontal Res. 2011, 46, 141–146. [Google Scholar] [CrossRef]
- Schmidt, J.; Weigert, C.; Leuschner, H.; Raddatz, R.; Haak, R.F.; Mauseberg, T.; Kottman, G.; Schmaltz, D.; Ziebolz, D. Active matrix metalloproteinase-8 and periodontal bacteria-interlink between periodontitis and inflammatory bowel disease? J. Periodontol. 2018, 89, 699–707. [Google Scholar] [CrossRef]
- Figueredo, C.M.; Nunes, J.G.; Mello-Neto, J.M.; Carvalho, A.T.; Ipe, D.S. Higher salivary expression of S100A12 in patients with ulcerative colitis and chronic periodontitis. Eur. J. Gastroenterol. Hepatol. 2021, 33, 116–117. [Google Scholar] [CrossRef]
- Figueredo, C.; Martins, A.; Lira-Junior, R.; Menegat, J.; Carvalho, A.T.P.; Fischer, R.; Gustafsson, A. Activity of inflammatory bowel disease influences the expression of cytokines in gingival tissue. Cytokine 2017, 95, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Menegat, J.S.B.; Lira-Junior, R.; Siqueira, M.A.; Brito, F.; Carvalho, A.T.P.; Fischer, R.G.; Figueredo, C.M. Cytokine expression in gingival and intestinal tissues of patients with periodontitis and inflammatory bowel disease: An exploratory study. Arch. Oral Biol. 2016, 66, 141–146. [Google Scholar] [CrossRef]
- Deng, J.; Yu, X.-Q.; Wang, P.-H. Inflammasome activation and Th17 responses. Mol. Immunol. 2019, 107, 142–164. [Google Scholar] [CrossRef] [PubMed]
- Ludwiczek, O.; Kaser, A.; Novick, D.; Dinarello, C.A.; Rubeisten, M.; Tilg, H. Elevated systemic levels of free interleukin-18 (IL-18) in patients with Crohn’s disease. Eur. Cytokine Net. 2005, 16, 27–33. [Google Scholar]
- Roberts, H.M.; Ling, M.R.; Insall, R.; Kalna, G.; Spengler, J.; Grant, M.; Chapple, I.L. Impaired neutrophil directional chemotactic accuracy in chronic periodontitis patients. J. Clin. Periodontol. 2015, 42, 1–11. [Google Scholar] [CrossRef]
- Gui, X.; Li, J.; Ueno, A.; Iacucci, M.; Qian, J.; Ghosh, S. Histopathological Features of Inflammatory Bowel Disease are Associated with Different CD4+ T Cell Subsets in Colonic Mucosal Lamina Propria. J. Crohn’s Coliti 2018, 12, 1448–1458. [Google Scholar] [CrossRef]
- Bastos, M.; Lima, J.; Vieira, P.; Mestnik, M.; Faveri, M.; Duarte, P. TNF-α and IL-4 levels in generalized aggressive periodontitis subjects. Oral Dis. 2009, 15, 82–87. [Google Scholar] [CrossRef] [PubMed]
- Holmström, S.B.; Lira-Junior, R.; Zwicker, S.; Majster, M.; Gustafsson, A.; Åkerman, S.; Klinge, B.; Svensson, M.; Boström, E.A. MMP-12 and S100s in saliva reflect different aspects of periodontal inflammation. Cytokine 2018, 113, 155–161. [Google Scholar] [CrossRef]
- Leibur, E.; Tuhkanen, A.; Pintson, U.; Söder, P.O. Prostaglandin E2 levels in blood plasma and in crevicular fluid of advanced periodontitis patients before and after surgical therapy. Oral Dis. 2008, 5, 223–228. [Google Scholar] [CrossRef]
- Zhang, L.; Li, X.; Yan, H.; Huang, L. Salivary matrix metalloproteinase (MMP)-8 as a biomarker for periodontitis: A PRISMA-compliant systematic review and meta-analysis. Medicine 2018, 97, e9642. [Google Scholar] [CrossRef]
- Luzina, I.G.; Keegan, A.D.; Hellen, N.M.; Rook, G.A.W.; Shea-Donohue, T.; Atamas, S.P. Regulation of inflammation by interleukin-4: A review of alternatives. J. Leukoc. Biol. 2012, 92, 753–764. [Google Scholar] [CrossRef] [PubMed]
- Lazarski, C.A.; Ford, J.; Katzman, S.D.; Rosenberg, A.F.; Fowell, D.J. IL-4 Attenuates Th1-Associated Chemokine Expression and Th1 Trafficking to Inflamed Tissues and Limits Pathogen Clearance. PLoS ONE 2013, 8, e71949. [Google Scholar] [CrossRef]
- Karttunnen, R.; Breese, E.J.; Walker-Smith, J.A.; Macdonald, T.T. Decreased mucosal interleukin-4 (IL-4) production in gut inflammation. J. Clin. Pathol. 1994, 47, 1015–1018. [Google Scholar] [CrossRef][Green Version]
- Dey, I.; Lejeune, M.; Chadee, K. Prostaglandin E2receptor distribution and function in the gastrointestinal tract. Br. J. Pharmacol. 2006, 149, 611–623. [Google Scholar] [CrossRef] [PubMed]
- Koelink, P.J.; Overbeek, S.A.; Braber, S.; Morgan, M.E.; Henricks, P.A.J.; Roda, M.A.; Verspaget, H.W.; Wolfkamp, S.C.; Velde, A.A.T.; Jones, C.W.; et al. Collagen degradation and neutrophilic infiltration: A vicious circle in inflammatory bowel disease. Gut 2013, 63, 578–587. [Google Scholar] [CrossRef] [PubMed]
- Kaiser, T.; Langhorst, J.; Wittkowski, H.; Becker, K.; Friedrich, A.W.; Rueffer, A.; Dobos, G.J.; Roth, J.; Foell, D. Faecal S100A12 as a non-invasive marker distinguishing inflammatory bowel disease from irritable bowel syndrome. Gut 2007, 56, 1706–1713. [Google Scholar] [CrossRef]
- Leach, S.; Yang, Z.; Messina, I.; Song, C.; Geczy, C.L.; Cunningham, A.M.; Day, A.S. Serum and mucosal S100 proteins, calprotectin (S100A8/S100A9) and S100A12, are elevated at diagnosis in children with inflammatory bowel disease. Scand. J. Gastroenterol. 2007, 42, 1321–1331. [Google Scholar] [CrossRef]
- Naber, A.H.J.; De Jong, D.J. Assessment of disease activity in inflammatory bowel disease; relevance for clinical trials. Neth. J. Med. 2003, 61, 105–110. [Google Scholar]
- Lo, C.-H.; Nguyen, L.H.; Wu, K.; Ogino, S.; Chan, A.T.; Giovannucci, E.L.; Song, M. Periodontal Disease, Tooth Loss, and Risk of Serrated Polyps and Conventional Adenomas. Cancer Prev. Res. 2020, 13, 699–706. [Google Scholar] [CrossRef]
- Nwizu, N.; Wactawski-Wende, J.; Genco, R.J. Periodontal disease and cancer: Epidemiologic studies and possible mechanisms. Periodontology 2000 2020, 83, 213–233. [Google Scholar] [CrossRef]
- Michaud, D.S.; Fu, Z.; Shi, J.; Chung, M. Periodontal Disease, Tooth Loss, and Cancer Risk. Epidemiol. Rev. 2017, 39, 49–58. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Allavena, P.; Sica, A.; Balkwill, F. Cancer-related inflammation. Nature 2008, 454, 436–444. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Author (Year) | Matched Variables | Participants | Medicaments/Smoking Habits/Disease Activity | Periodontal and IBD Diagnose | Type of Essay | Sample | Main Immunological Outcomes |
|---|---|---|---|---|---|---|---|
| Van Dyke et al., 1986 | Age and gender. | IBD patients with (n = 10) and without (n = 10) periodontal disease Patients with periodontitis (n = 8) Healthy controls (n = 8) | Steroid therapy Subjects were not included if they smoked ≤ 10 cigarettes daily. No disease activity information | Gingival erythema, edema, suppuration, BOP, pain upon probing, Ramfijord attachment levels and Periapical X-ray. IBD: combination of symptoms, including diarrhea, abdominal pain, bleeding, weight loss, perianal disease, and arthritis. Control: healthy individuals who had no bone loss or no/mild gingivitis. | Radioimmunoassay: PGE2 Phagocytosis: Van Furth method Boyden chamber assay. Neutrophils Chemotaxis assay. | GCF Serum | PGE2 sig. > in GCF of IBD patients with periodontitis compared to matched adult periodontitis. Chemotactic response sig < in UC patients with periodontal disease compared to healthy patients. The chemotactic response of normal neutrophils was significantly inhibited by all serum from patients with IBD and periodontal disease. The chemotactic response of normal neutrophils was not affected by serum from normal donors. IBD patients without the periodontal disease had mixed results. Neutrophil phagocytosis was similar between the groups. |
| Figueredo et al., 2011 | Age, gender. | CD patients with periodontitis (n = 15) UC patients with periodontitis (n = 15) Periodontitis patients (n = 15) | CD: immunomodulators (n = 7), aminosalicylates (n = 4) and immunomodulators + aminosalicylates (n = 2). UC: immunomodulators (n = 1), aminosalicylates (n = 9) and immunomodulators + aminosalicylates (n = 5). CD (n = 3), UC (n = 1) and controls (n = 2) were smokers. UC: active disease (n = 3) and 12 in remission. CD: active disease (n = 5) remission (n = 10). | At least five inflamed sites with PD of ≥5 mm and CAL of ≥3 mm in different teeth and diagnosed with chronic untreated Periodontitis. CD and UC: outpatients already diagnosed with IBD attending the Gastroenterology clinics. | ELISA for IL-18. Multiplex assay for IL-1β, IL-4, IL-6, IL-10, IL-12p40, IL-12p70, TNF-α and IFN-γ. | GCF Serum | IL-4 sig. < in deep sites of patients with CD and periodontitis compared to periodontitis only. UC patient < total amount of IL-4 in the GCF in the shallow site and a > IL-6 in deep sites, when compared with periodontitis only. Serum levels of IL-18 sig. > in patients with the coexistence of IBD and periodontitis. Positive correlation between IL-6 in GCF and IFN-γ in serum of CD patients. Positive correlation between IL-1β in gingival crevicular fluid and IL-18 in serum of UC patients. No correlation was observed in periodontitis only. |
| Figueredo et al., 2017 | Age and gender. | DC patients with periodontitis (n = 10) UC patients with periodontitis (n = 11) No control group without IBD. | Mesalazine (n = 7), mesalazine + azathioprine (n = 8), mesalazine, azathioprine + TNF-α inhibitor (n = 4) and mesalazine + steroid (n = 2). Smoking habits not reported CD (n = 4) and UC (n = 4) had active disease and CD (n = 6) and UC (n = 7) were in remission. | At least 10 teeth with PD ≥ 5 mm and CAL ≥ 4 mm in at least 4 sites, in different teeth. IBD: clinical, endoscopic, radiologic, and histological parameters. | Multiplex assay for IL-1β, IL-4, IL-6, IL-10, IL-21, IL-22, IL-23, IL-25, IL-31, IL-33, IL-17A, IL-17F, IFN-γ, sCD40L, and TNF-α. | Gingival and Intestinal tissues | Cytokine levels were similar in intestinal tissue between CD and UC patients. IL-23 in gingival tissue in CD sig. > compared to UC patients with periodontitis. IL-4, IL-10, and IL-21 levels in gingival tissue sig. > inactive IBD. Furthermore, a trend towards > IL-1β levels. IL-1β, IL-4, IL-6, IL-17A, IL17F, IL-21, IL-31, IL-33, and sCD40L were sig. > in intestinal tissue from patients with active disease. Furthermore, a trend towards increased levels of TNF-α inactive IBD. |
| Schmidt et al., 2018 | Age and gender. | CD patients with periodontal disease (n= 30) UC patients with periodontal disease (n= 29) Controls (n = 59) | Aminosalicylates and azathioprine (14%), aminosalicylates and anti-TNF (5%), immunomodulators and anti-TNF (3%), corticosteroids and anti-TNF (5%). Corticosteroids and aminosalicylates and corticosteroids and immunomodulator (methotrexate) (2%). Immunomodulators (22% azathioprine/6-mercaptopurine, 2% methotrexate, 2% cyclosporine). No information available IBD (n = 5). CD (n = 14) and 20 periodontal disease (n = 20) were smokers. Disease activity information available (n = 33), UC (n = 3) active and n = 30 on remission | Periodontal condition was classified into healthy/mild, moderate or severe Periodontitis. No assessment of bleeding on probing (BOP). Papilla bleeding index (PBI). IBD: outpatients recruited within a private gastroenterological clinic. | ELISA assay for aMMP-8 | GCF | aMMP-8 in IBD sig. > compared to control. No sig. difference between CD and UC. aMMP-8 in CD sig. > with increasing severity of periodontitis. Periodontitis severity had no influence on aMMP-8 in UC and controls. aMMP-8 > in patients with severe periodontitis and CD compared to UC and HC also with severe periodontitis. aMMP-8 in CD patients with no or mild periodontitis was < than in the case of UC. |
| Manegat et al., 2016 | Age and gender. | DC patients with periodontitis (n = 18) UC patients with periodontitis (n = 10) No control group without IBD. | CD: immunomodulators (n = 13), 5-aminosalicylate derivatives (n = 11), corticosteroids (n = 1), immunomodulatory derivatives + 5-aminosalicylate (n = 10) no medication (n = 4). UC: 5-aminosalicylate derivatives (n = 8), immunomodulators (n = 5), corticosteroids (n = 1) and immunomodulatory derivatives + 5-aminosalicylate acid derivatives (n = 4) no medication (n = 1). CD group had two smokers and one ex-smoker and UC had three ex-smokers. CD (n = 1) and UC (n = 2) with disease active. | At least 8 teeth with PD ≥ 5 mm and CAL ≥ 4 mm in at least 4 sites, in different teeth. IBD: clinical, endoscopic, radiologic, and histological parameters. | LUMINEX for IFN-γ, IL-1β, IL-4, IL-6, IL-10, IL-21, IL-22, IL-23, IL-25, IL-31, IL-33, IL-17A, IL-17F, sCD40L, and TNF-α | Gingival and intestinal tissues | No differences in cytokine levels between CD and UC patients in the gingival tissue. IL-17A, IL-17F, IL-22, IL-25, IL-33, INF-g, and IL-10 sig. > in gingival tissue. IL-6, IL-31 and IL-21 in gingival tissue showed a tendency to > levels compared to intestinal tissue. |
| Figueredo et al., 2021 | Age, gender. | CD patients with periodontitis (n = 9) UC patients with periodontitis (n = 9). Periodontitis patients (n = 5). | Not reported | Not reported | ELISA for S100A12 | Saliva | S100A12 sig. > in patients with UC patients with periodontitis compared to CD and non-IBD patients also with periodontitis. |
| Author (Year) | Periodontal Findings |
|---|---|
| Van Dyke et al., 1986 | Comparison of IBD periodontitis and periodontitis groups revealed no significant differences in CAL. Periodontal health of the IBD patient is one of moderate to severe periodontitis with extreme inflammation compared with periodontitis only. Redness Bleeding, CAL and PPD were significant > in IBD with periodontitis and adult periodontitis compared to IBD with no periodontitis and controls. |
| Figueredo et al., 2011 | CAL, BOP, PI and GCF volume did not differ between the groups. |
| Figueredo et al., 2017 | PI, BOP, PD, CAL did not differ between the groups. |
| Schmidt et al., 2018 | Significant higher CAL was found in IBD compared to HC, but no significant difference was found for PPD. The PBI was significantly higher in IBD than in HC. IBD group significantly had more participants with severe periodontitis compared to HC. Periodontal parameters did not significantly differ between CD and UC. |
| Figueredo et al., 2021 | Not reported |
| Menegat et al., 2016 | CD patients presented higher % PD significant > 7 mm compared to UC patients also with periodontitis. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
de Mello-Neto, J.M.; Nunes, J.G.R.; Tadakamadla, S.K.; da Silva Figueredo, C.M. Immunological Traits of Patients with Coexistent Inflammatory Bowel Disease and Periodontal Disease: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 8958. https://doi.org/10.3390/ijerph18178958
de Mello-Neto JM, Nunes JGR, Tadakamadla SK, da Silva Figueredo CM. Immunological Traits of Patients with Coexistent Inflammatory Bowel Disease and Periodontal Disease: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(17):8958. https://doi.org/10.3390/ijerph18178958
Chicago/Turabian Stylede Mello-Neto, João Martins, Jessica Gomes Rodrigues Nunes, Santosh Kumar Tadakamadla, and Carlos Marcelo da Silva Figueredo. 2021. "Immunological Traits of Patients with Coexistent Inflammatory Bowel Disease and Periodontal Disease: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 17: 8958. https://doi.org/10.3390/ijerph18178958
APA Stylede Mello-Neto, J. M., Nunes, J. G. R., Tadakamadla, S. K., & da Silva Figueredo, C. M. (2021). Immunological Traits of Patients with Coexistent Inflammatory Bowel Disease and Periodontal Disease: A Systematic Review. International Journal of Environmental Research and Public Health, 18(17), 8958. https://doi.org/10.3390/ijerph18178958