
Multicomponent Physical Exercise Training in Multimorbid and Palliative Oldest Adults



Abstract
:1. Introduction
2. Materials and Methods
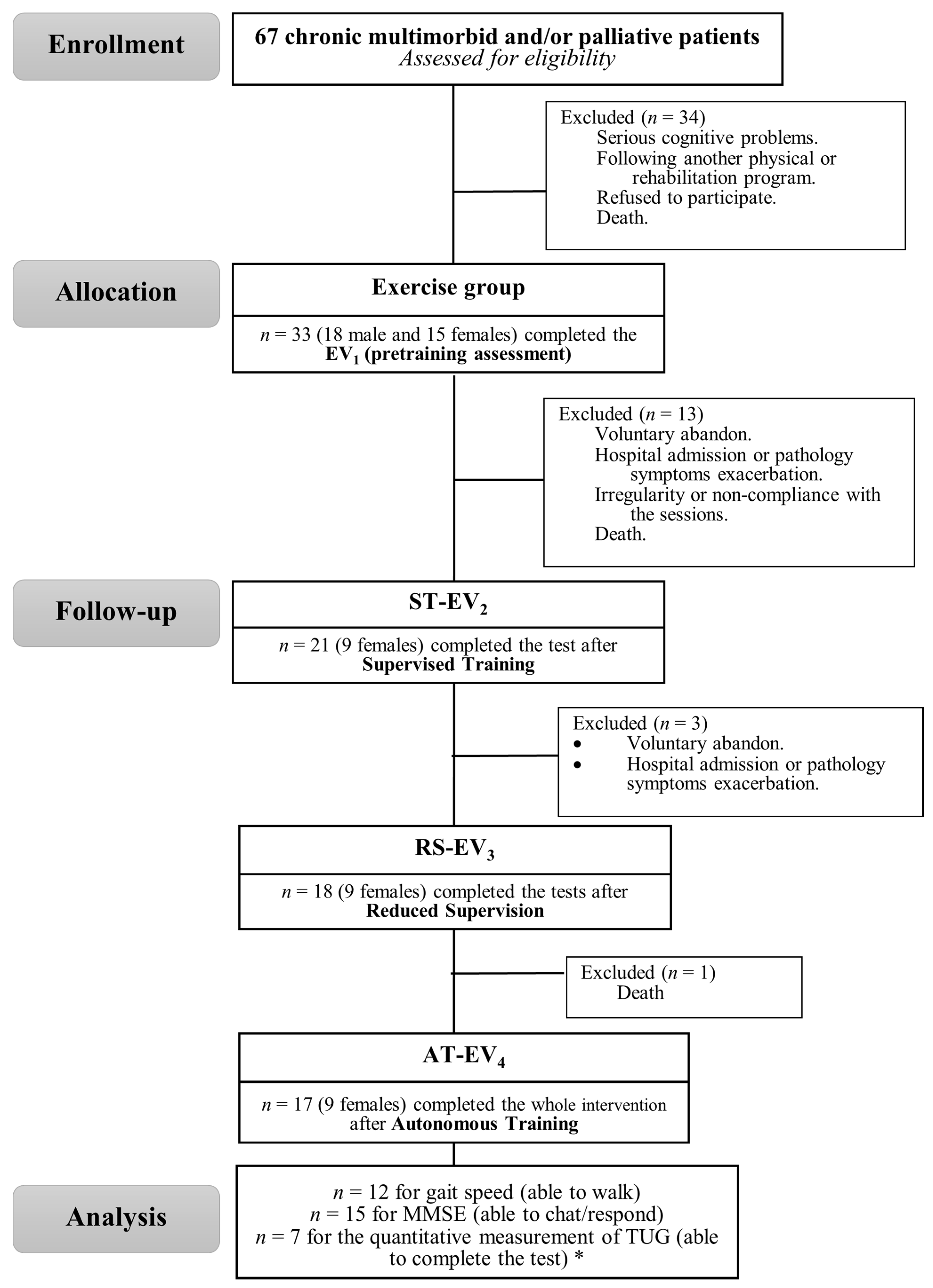
2.1. Participants
2.2. Experimental Procedure
2.3. Functional Capacity Assessment
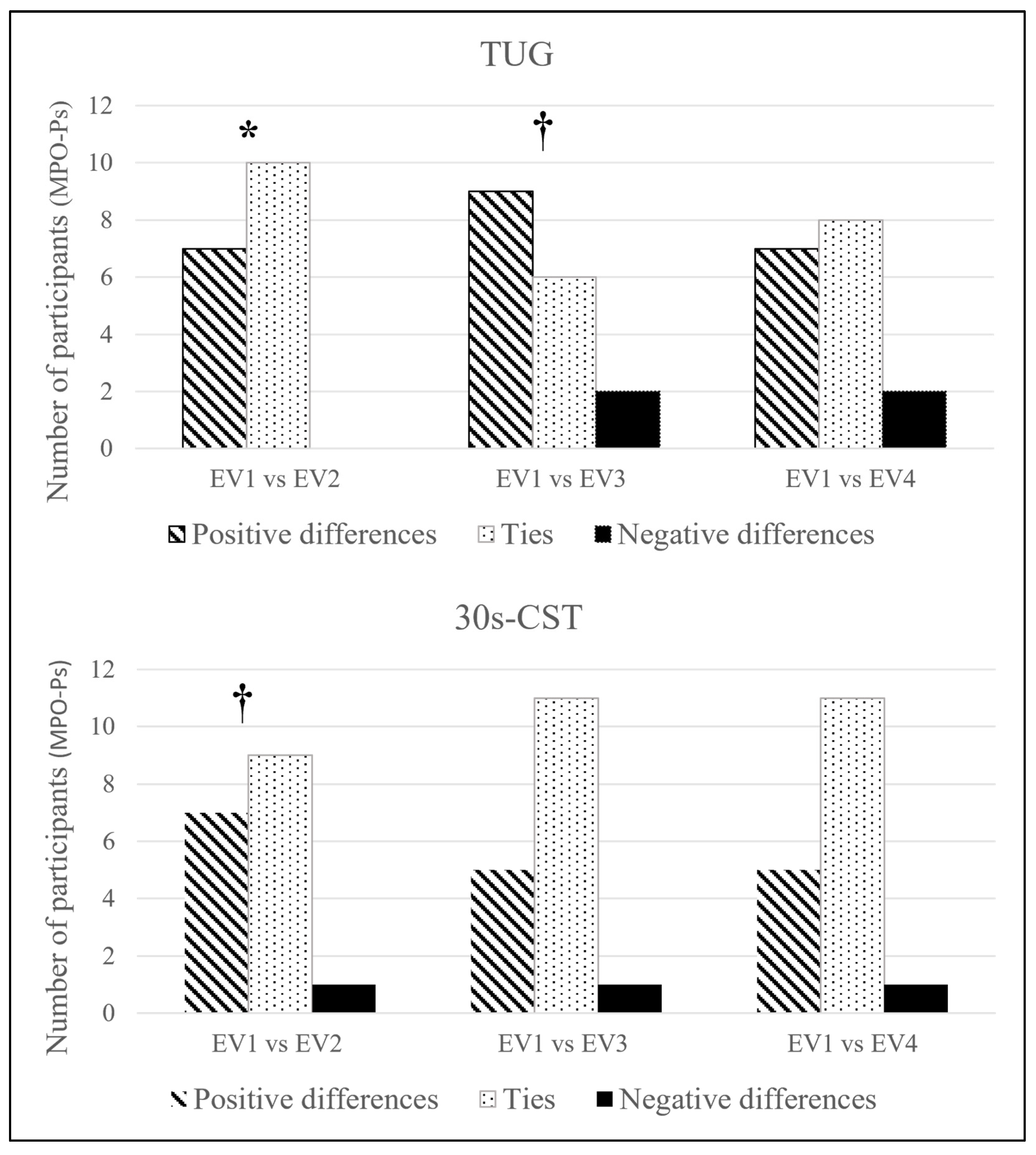
2.4. Categorical Analysis of the 8-Foot Timed Up-and-Go Test and the 30-s Chair Stand Test
2.5. Cognitive Function, Daily Living Autonomy and Health Variables Assessment
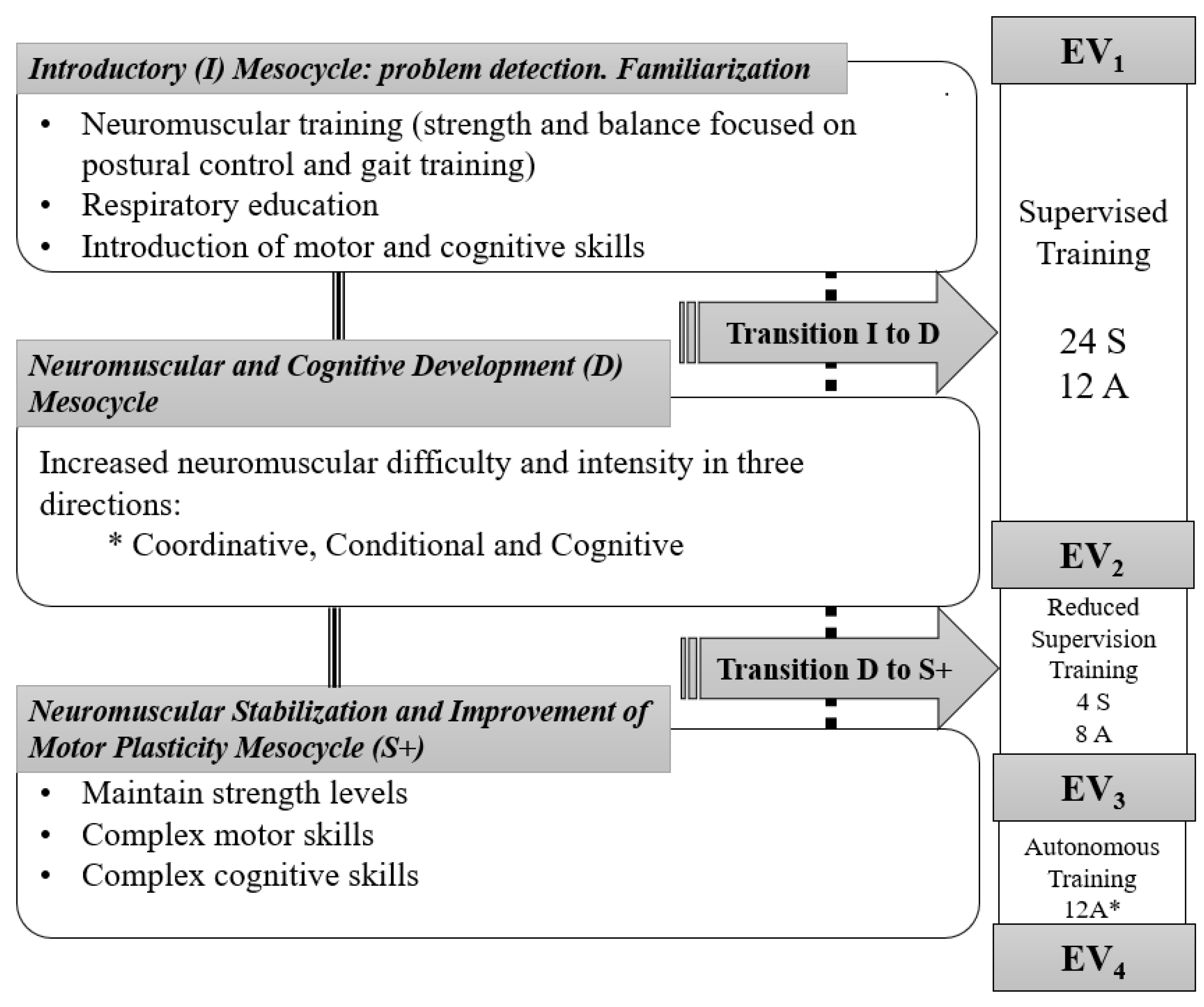
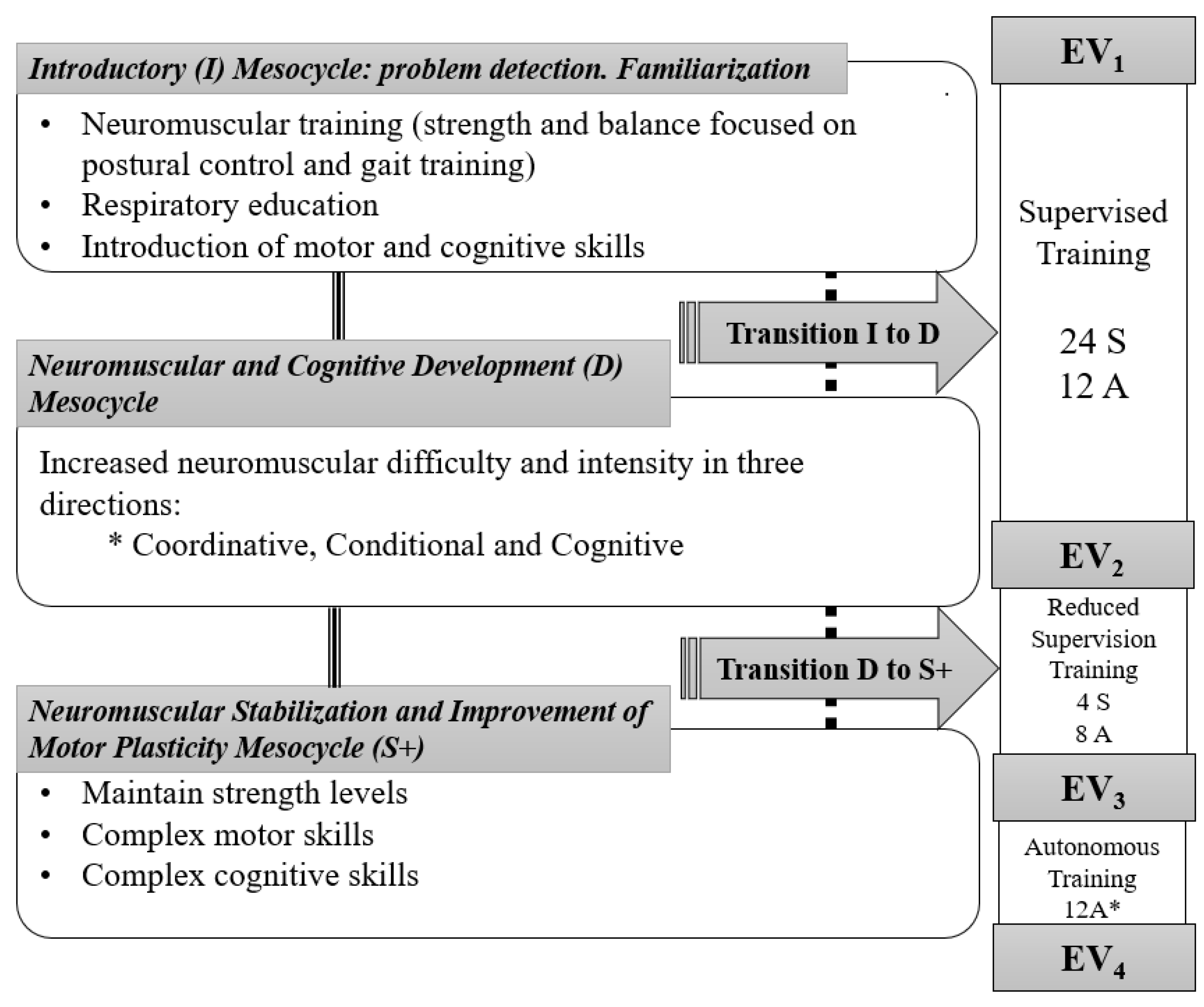
2.6. Intervention
2.7. Data Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cunningham, C.; O’Sullivan, R.; Caserotti, P.; Tully, M.A. Consequences of physical inactivity in older adults: A systematic review of reviews and meta-analyses. Scand. J. Med. Sci. Sports 2020, 30, 816–827. [Google Scholar] [CrossRef]
- Kandola, A.; Stubbs, B.; Koyanagi, A. Physical multimorbidity and sedentary behavior in older adults: Findings from the Irish longitudinal study on ageing (TILDA). Maturitas 2020, 134, 1–7. [Google Scholar] [CrossRef]
- Jayasinghe, S.; Byrne, N.M.; Patterson, K.A.; Ahuja, K.D.; Hills, A.P. The current global state of movement and physical activity-the health and economic costs of the inactive phenotype. Prog. Cardiovasc. Dis. 2020, 64, 9–16. [Google Scholar] [CrossRef]
- Lazarus, N.R.; Lord, J.M.; Harridge, S.D. The relationships and interactions between age, exercise and physiological function. J. Physiol. 2019, 597, 1299–1309. [Google Scholar] [CrossRef] [Green Version]
- Rebelo-Marques, A.; De Sousa Lages, A.; Andrade, R.; Ribeiro, C.F.; Mota-Pinto, A.; Carrilho, F.; Espregueira-Mendes, J. Aging hallmarks: The benefits of physical exercise. Front. Endocrinol. 2018, 9, 258. [Google Scholar] [CrossRef]
- Balan, E.; Decottignies, A.; Deldicque, L. Physical activity and nutrition: Two promising strategies for telomere maintenance? Nutrients 2018, 10, 1942. [Google Scholar] [CrossRef] [Green Version]
- Garland, S.N.; Johnson, B.; Palmer, C.; Speck, R.M.; Donelson, M.; Xie, S.X.; DeMichele, A.; Mao, J.J. Physical activity and telomere length in early stage breast cancer survivors. Breast Cancer Res. 2014, 16, 413. [Google Scholar] [CrossRef]
- López-Otín, C.; Blasco, M.A.; Partridge, L.; Serrano, M.; Kroemer, G. The hallmarks of aging. Cell 2013, 153, 1194–1217. [Google Scholar] [CrossRef] [Green Version]
- MacNee, W.; Rabinovich, R.A.; Choudhury, G. Ageing and the border between health and disease. Eur. Respir. 2014, 44, 1332–1352. [Google Scholar] [CrossRef] [Green Version]
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef] [Green Version]
- Fragala, M.S.; Cadore, E.L.; Dorgo, S.; Izquierdo, M.; Kraemer, W.J.; Peterson, M.D.; Ryan, E.D. Resistance training for older adults: Position statement from the national strength and conditioning association. J. Strength Cond. Res. 2019, 33, 2019–2050. [Google Scholar] [CrossRef]
- Angulo, J.; El Assar, M.; Álvarez-Bustos, A.; Rodríguez-Mañas, L. Physical activity and exercise: Strategies to manage frailty. Redox Biol. 2020, 35, 101513. [Google Scholar] [CrossRef]
- Sellami, M.; Gasmi, M.; Denham, J.; Hayes, L.D.; Stratton, D.; Padulo, J.; Bragazzi, N. Effects of acute and chronic exercise on immunological parameters in the elderly aged: Can physical activity counteract the effects of aging? Front. Immunol. 2018, 9, 2187. [Google Scholar] [CrossRef] [Green Version]
- Fried, L.P.; Tangen, C.M.; Walston, J.; Newman, A.B.; Hirsch, C.; Gottdiener, J.; Seeman, T.; Tracy, R.; Kop, W.J.; Burke, G. Frailty in older adults: Evidence for a phenotype. J. Gerontol. A Biol. Sci. Med. Sci. 2001, 56, M146–M157. [Google Scholar] [CrossRef]
- Clegg, A.; Young, J. The frailty syndrome. Clin. Med. 2011, 11, 72–75. [Google Scholar] [CrossRef]
- Fabrício-Wehbe, S.C.C.; Rodrigues, R.A.P.; Haas, V.J.; Fhon, J.R.S.; Diniz, M.A. Association of frailty in hospitalized and institutionalized elderly in the community-dwelling. Rev. Bras. Enferm. 2016, 69, 691–696. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- WHO. Centro de Prensa. Actividad Física. Datos y Cifras. Available online: http://www.who.int/mediacentre/factsheets/fs385/es/ (accessed on 25 March 2021).
- Veronese, N.; Stubbs, B.; Noale, M.; Solmi, M.; Pilotto, A.; Vaona, A.; Demurtas, J.; Mueller, C.; Huntley, J.; Crepaldi, G. Polypharmacy is associated with higher frailty risk in older people: An 8-year longitudinal cohort study. J. Am. Med. Dir. Assoc. 2017, 18, 624–628. [Google Scholar] [CrossRef]
- Powell, V.D.; Silveira, M.J.J. Palliative Care for Older Adults with Multimorbidity in the Time of COVID 19. J. Aging Soc. Policy 2021, 1–9. [Google Scholar] [CrossRef]
- Dempsey, P.C.; Owen, N.; Biddle, S.J.; Dunstan, D.W. Managing sedentary behavior to reduce the risk of diabetes and cardiovascular disease. Curr. Diab Rep. 2014, 14, 522. [Google Scholar] [CrossRef] [Green Version]
- Kosaki, K.; Tanahashi, K.; Matsui, M.; Akazawa, N.; Osuka, Y.; Tanaka, K.; Dunstan, D.W.; Owen, N.; Shibata, A.; Oka, K. Sedentary behaviour, physical activity, and renal function in older adults: Isotemporal substitution modelling. BMC Nephrol. 2020, 21, 1–10. [Google Scholar] [CrossRef]
- Gremeaux, V.; Gayda, M.; Lepers, R.; Sosner, P.; Juneau, M.; Nigam, A. Exercise and longevity. Maturitas 2012, 73, 312–317. [Google Scholar] [CrossRef]
- Paterson, D.H.; Jones, G.R.; Rice, C.L. Ageing and physical activity: Evidence to develop exercise recommendations for older adults. Appl. Physiol. Nutr. Metab. 2007, 32, S69–S108. [Google Scholar] [CrossRef] [Green Version]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef]
- Freiberger, E.; Kemmler, W.; Siegrist, M.; Sieber, C. Frailty and exercise interventions. J. Gerontol. Geriatr. 2016, 49, 606–611. [Google Scholar] [CrossRef]
- Dunstan, D.W.; Healy, G.N.; Sugiyama, T.; Owen, N. Too much sitting’and metabolic risk—Has modern technology caught up with us. Eur. Endocrinol. 2010, 6, 19–23. [Google Scholar] [CrossRef] [Green Version]
- Sartini, C.; Wannamethee, S.G.; Iliffe, S.; Morris, R.W.; Ash, S.; Lennon, L.; Whincup, P.H.; Jefferis, B. Diurnal patterns of objectively measured physical activity and sedentary behaviour in older men. BMC Public Health 2015, 15, 609. [Google Scholar] [CrossRef] [Green Version]
- Askim, T.; Bernhardt, J.; Salvesen, O.; Indredavik, B. Physical activity early after stroke and its association to functional outcome 3 months later. J. Stroke Cerebrovasc. Dis. 2014, 23, e305–e312. [Google Scholar] [CrossRef]
- ACSM. ACSM’s Guidelines for Exercise Testing and Prescription; Lippincott Williams & Wilkins: Philadelphia, PA, USA, 2013. [Google Scholar]
- Sherrington, C.; Fairhall, N.; Kwok, W.; Wallbank, G.; Tiedemann, A.; Michaleff, Z.A.; Ng, C.A.; Bauman, A. Evidence on physical activity and falls prevention for people aged 65+ years: Systematic review to inform the WHO guidelines on physical activity and sedentary behaviour. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 1–9. [Google Scholar] [CrossRef]
- Blasco-Lafarga, C.; Sanchis-Sanchis, R.; Sanchis-Soler, G.; San Inocencio-Cuenca, D.; Llorens-Soriano, P. Entrenamiento Neuromotor en pacientes ancianos pluripatológicos en las Unidades de Hospitalización a Domicilio: Estudio piloto. Cuad. Psicol. Deporte 2019, 19, 95–105. [Google Scholar] [CrossRef] [Green Version]
- Sanchis-Soler, G.; Saninocencio, D.; Llorens, P.; Blasco-Lafarga, C. Reducción de la sobrecarga del cuidador tras entrenamiento supervisado en ancianos pluripatológicos y paliativos. Cuad. Psicol. Deporte 2021, 21, 271–281. [Google Scholar] [CrossRef]
- Blasco-Lafarga, C.; Cordellat, A.; Forte, A.; Roldán, A.; Monteagudo, P. Short and Long-Term Trainability in Older Adults: Training and Detraining Following Two Years of Multicomponent Cognitive—Physical Exercise Training. Int. J. Environ. Res. Public Health 2020, 17, 5984. [Google Scholar] [CrossRef]
- Izquierdo, M.; Merchant, R.; Morley, J.; Anker, S.; Aprahamian, I.; Arai, H.; Aubertin-Leheudre, M.; Bernabei, R.; Cadore, E.; Cesari, M.J. International Exercise Recommendations in Older Adults (ICFSR): Expert Consensus Guidelines. J. Nutr. Health Aging 2021, 25, 824–853. [Google Scholar] [CrossRef]
- Lewsey, S.C.; Weiss, K.; Schär, M.; Zhang, Y.; Bottomley, P.A.; Samuel, T.J.; Xue, Q.-L.; Steinberg, A.; Walston, J.D.; Gerstenblith, G. Exercise intolerance and rapid skeletal muscle energetic decline in human age-associated frailty. JCI Insight 2020, 5, e141246. [Google Scholar] [CrossRef] [PubMed]
- Blasco-Lafarga, C.; Sanchis-Sanchis, R.; Sanchis-Soler, G.; Llorens-Soriano, P. Physical and functional improvements after 4 weeks of a functional training program for home hospitalization unit patients. In Proceedings of the Physiology 2014 Congress, London, UK, 22–24 August 2014. [Google Scholar]
- Blasco-Lafarga, C.; Martinez-Navarro, I.; Cordellat, A.; Roldán, A.; Monteagudo, P.; Sanchis-Soler, G.; Sanchis-Sanchis, R. Método de Entrenamiento Funcional Cognitivo Neuromotor. España Patent 156,069, 24 October 2016. [Google Scholar]
- Cordellat Marzal, A.; Roldán Aliaga, A.; Monteagudo Chiner, P.; Forte Deltell, A.; Blasco-Lafarga, C. Pruebas T vs análisis categorial: Evolución de la agilidad en los adultos mayores tras dos años de entrenamiento. Retos Nuevas Tend. En Educ. Física Deporte Y Recreación 2021, 39, 5. [Google Scholar]
- Roldán, A.; Cordellat, A.; Monteagudo, P.; García-Lucerga, C.; Blasco-Lafarga, N.M.; Gomez-Cabrera, M.C.; Blasco-Lafarga, C. Beneficial effects of inspiratory muscle training combined with multicomponent training in elderly active women. Res. Q. Exerc. Sports Med. 2019, 90, 547–554. [Google Scholar] [CrossRef]
- Silsupadol, P.; Shumway-Cook, A.; Lugade, V.; van Donkelaar, P.; Chou, L.-S.; Mayr, U.; Woollacott, M.H. Effects of Single-Task Versus Dual-Task Training on Balance Performance in Older Adults: A Double-Blind, Randomi. Arch. Phys. Med. Rehabil. 2009, 90, 381–387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rikli, R.; Jones, J. Development and validation of a functional fitness test for community-residing older adults. J. Aging Phys. Act. 1999, 7, 129–161. [Google Scholar] [CrossRef]
- Rikli, R.; Jones, J. Senior Fitness Test Manual; Human Kinetics: Champaign, IL, USA, 2013. [Google Scholar]
- Galindo-Ciocon, D.J.; Ciocon, J.O.; Galindo, D.J. Gait training and falls in the elderly. J. Gerontol. Nurs. 1995, 21, 10–17. [Google Scholar] [CrossRef]
- Berg, K.; Wood-Dauphine, S.; Williams, J.; Gayton, D. Measuring balance in the elderly: Preliminary development of an instrument. Physiother Can. 1989, 41, 304–311. [Google Scholar] [CrossRef]
- Roberts, H.C.; Denison, H.J.; Martin, H.J.; Patel, H.P.; Syddall, H.; Cooper, C.; Sayer, A.A. A review of the measurement of grip strength in clinical and epidemiological studies: Towards a standardised approach. Age Ageing 2011, 40, 423–429. [Google Scholar] [CrossRef] [Green Version]
- Shah, S.; Vanclay, F.; Cooper, B. Improving the sensitivity of the Barthel Index for stroke rehabilitation. J. Clin. Epidemiol. 1989, 42, 703–709. [Google Scholar] [CrossRef]
- Lobo, A.; Saz, P.; Marcos, G.; ZARADEMP Workgroup. MMSE Examen Cognoscitivo Mini-Mental; TEA Ediciones: Madrid, Spain, 2002. [Google Scholar]
- Morishita, S.; Tsubaki, A.; Nakamura, M.; Nashimoto, S.; Fu, J.B.; Onishi, H. Rating of perceived exertion on resistance training in elderly subjects. Expert Rev. Cardiovasc. Ther. 2019, 17, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Fritz, C.O.; Morris, P.E.; Richler, J.J. Effect size estimates: Current use, calculations, and interpretation. J. Exp. Psychol. Gen. 2012, 141, 2–18. [Google Scholar] [CrossRef] [Green Version]
- Rosner, B. Fundamentals of Biostatistics; Cengage Learning: Boston, MA, USA, 2015. [Google Scholar]
- Applebaum, E.V.; Breton, D.; Feng, Z.W.; Ta, A.-T.; Walsh, K.; Chassé, K.; Robbins, S.M. Modified 30-second Sit to Stand test predicts falls in a cohort of institutionalized older veterans. PLoS ONE 2017, 12, e0176946. [Google Scholar] [CrossRef] [Green Version]
- McAllister, L.S.; Palombaro, K.M. Modified 30-second Sit-to-Stand test: Reliability and validity in older adults unable to complete traditional Sit-to-Stand testing. J. Geriatr. Phys. Ther. 2020, 43, 153–158. [Google Scholar] [CrossRef]
- Bohannon, R.W. Reference Values for the Timed Up and Go Test: A Descriptive Meta-Analysis. J. Geriatr. Phys. Ther. 2006, 29, 64–68. [Google Scholar] [CrossRef] [Green Version]
- Bohannon, R.W.; Peolsson, A.; Massy-Westropp, N.; Desrosiers, J.; Bear-Lehman, J. Reference values for adult grip strength measured with a Jamar dynamometer: A descriptive meta-analysis. Physiotherapy 2006, 92, 11–15. [Google Scholar] [CrossRef]
- del Nogal, M.L.; González-Ramírez, A.; Palomo-Iloro, A. Evaluación del riesgo de caídas. Protocolos de valoración clínica. Rev. Española Geriatría Y Gerontol. 2005, 40, 54–63. [Google Scholar] [CrossRef]
- Studenski, S.; Perera, S.; Patel, K.; Rosano, C.; Faulkner, K.; Inzitari, M.; Brach, J.; Chandler, J.; Cawthon, P.; Connor, E.B. Gait speed and survival in older adults. JAMA 2011, 305, 50–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perera, S.; Patel, K.V.; Rosano, C.; Rubin, S.M.; Satterfield, S.; Harris, T.; Ensrud, K.; Orwoll, E.; Lee, C.G.; Chandler, J.M. Gait speed predicts incident disability: A pooled analysis. J. Gerontol. Ser. A Biomed. Sci. Med. Sci. 2016, 71, 63–71. [Google Scholar] [CrossRef]
- Cadore, E.L.; de Asteasu, M.L.S.; Izquierdo, M. Multicomponent exercise and the hallmarks of frailty: Considerations on cognitive impairment and acute hospitalization. Exp. Gerontol. 2019, 122, 10–14. [Google Scholar] [CrossRef] [PubMed]
- Hughes, K.J.; Salmon, N.; Galvin, R.; Casey, B.; Clifford, A.M. Interventions to improve adherence to exercise therapy for falls prevention in community-dwelling older adults: Systematic review and meta-analysis. Age Ageing 2019, 48, 185–195. [Google Scholar] [CrossRef]
- Amboni, M.; Barone, P.; Hausdorff, J.M. Cognitive contributions to gait and falls: Evidence and implications. Mov. Disord. 2013, 28, 1520–1533. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
| Mn ± SD | CV% | |
| Age | 81.6 ± 5.6 | 6.9% |
| SBP (mmHg) | 133.0 ± 15.07 | 11.3% |
| DBP (mmHg) | 71.5 ± 9.5 | 13.3% |
| Weight (Kg) a | 69.5 ± 13.8 | 19.9% |
| Height (cm) b | 154.1 ± 12.6 | 8.2% |
| BMI | 30.1 ± 5.2 | 17.3% |
| SaO2 (%) | 92.7 ± 5.3 | 5.68% |
| Frequency | Percentage | |
| Gender | ||
| Male | 8 | 47.1% |
| Female | 9 | 52.9% |
| Walk initially | ||
| Yes | 12 | 70.6% |
| No | 5 | 29.4% |
| Pathological condition | ||
| Chronic-Pluripathological | 15 | 88.2% |
| Palliative-Oncological | 2 | 11.8% |
| Test | N | EV1 | EV2 | EV3 | EV4 | p |
|---|---|---|---|---|---|---|
| Gait speed (m/s) | 12 | 0.33 (0.22) | 0.34 (0.22) | 0.31 (0.25) | 0.33 (0.25) | 0.42 |
| 30 s-CST (Rep) | 17 | 1.65 (2.87) | 2.94 (2.91) * | 2.59 (3.10) * | 2.56 (2.86) | 0.07 † |
| Berg (s) | 17 | 16.00 (14.25) | 22.35 (17.00) * | 21.18 (15.24) | 18.00 (13.91) | 0.05 * |
| Tinetti Balance (s) | 17 | 5.71 (5.23) | 7.47 (5.41) † | 6.76 (4.53) | 6.41 (4.65) | 0.24 |
| Tinetti Gait (s) | 17 | 3.53 (3.50) | 4.94 (3.73) † | 4.65 (3.97) | 4.47 (3.76) | 0.45 |
| Total Tinetti (s) | 17 | 9.24 (8.10) | 12.41 (8.87) * | 11.41 (8.23) | 10.88 (8.28) | 0.13 |
| Barthel Index (s) | 17 | 30.88 (29.85) | 40.59 (31.61) * | 41.18 (26.84) * | 38.82 (29.29) | 0.06 † |
| p | ||||||
| Hand Grip Right (kg) | 17 | 12.11 (6.63) | 12.62 (6.31) | 11.97 (6.70) | 11.14 (6.29) | 0.73 |
| Hand Grip Left (kg) | 17 | 10.43 (6.68) | 11.04 (5.80) | 9.78 (5.98) | 9.88 (4.69) | 0.34 |
| MMSE (s) | 15 | 24.60 (3.83) | 25.27 (3.63) | 24.93 (3.69) | 25.20 (4.39) | 0.93 |
| TUG (s) | 7 | 35.44 (26.45) | 31.52 (12.78) | 51.03 (38.79) | 43.11 (28.59) | 0.36 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Blasco-Lafarga, C.; Sanchis-Soler, G.; Llorens, P. Multicomponent Physical Exercise Training in Multimorbid and Palliative Oldest Adults. Int. J. Environ. Res. Public Health 2021, 18, 8896. https://doi.org/10.3390/ijerph18178896
Blasco-Lafarga C, Sanchis-Soler G, Llorens P. Multicomponent Physical Exercise Training in Multimorbid and Palliative Oldest Adults. International Journal of Environmental Research and Public Health. 2021; 18(17):8896. https://doi.org/10.3390/ijerph18178896
Chicago/Turabian StyleBlasco-Lafarga, Cristina, Gema Sanchis-Soler, and Pere Llorens. 2021. "Multicomponent Physical Exercise Training in Multimorbid and Palliative Oldest Adults" International Journal of Environmental Research and Public Health 18, no. 17: 8896. https://doi.org/10.3390/ijerph18178896
APA StyleBlasco-Lafarga, C., Sanchis-Soler, G., & Llorens, P. (2021). Multicomponent Physical Exercise Training in Multimorbid and Palliative Oldest Adults. International Journal of Environmental Research and Public Health, 18(17), 8896. https://doi.org/10.3390/ijerph18178896