
Investing in Public Health Infrastructure to Address the Complexities of Homelessness



{kind=link}
Abstract
:1. Introduction
2. The Structural Determinants of Homelessness
3. Infrastructure Failures and their Public Health Impacts
- In 2005, Hurricane Katrina, a category 5 hurricane, devastated New Orleans, Louisiana, leaving 1800 people dead and estimated thousands more temporarily displaced from their homes and businesses as a consequence of fatal flaws of engineering in the city’s system of levees and the flood protection that the system was supposed to afford homeowners and businesses [14].
- In August of 2007, an eight-lane steel bridge structure that connected Interstate 35 W across the Saint Anthony Falls of the Mississippi River in Minneapolis, Minnesota, collapsed—resulting in the deaths of 13 motorists and injuring over 140 others. According to the National Public Radio, “The bridge collapse sparked immediate calls in Minnesota and across the country [sic] invest big in repairing and replacing the nation’s aging and crumbling infrastructure” [15].
- In one of the most catastrophic failures of state and municipal governments to protect the health of its citizens, the Flint, Michigan, water supply was discovered in 2015 to be contaminated with lead and other toxic chemical wastes, corrosive industrial byproducts, and sewage that were in the Flint River—which became the city’s water supply source when state and local government officials stopped pumping water from a Detroit source in a cost-saving measure and began pumping water from the Flint River into the homes of Flint residents. Since then, one in six of the city’s homes has been abandoned, Flint’s population has plummeted from 125,000 in 2000 to under 100,000 people, and almost half of its residents—most of whom are African American—live below the poverty line [16].
- In February 2021—in the midst of the COVID-19 pandemic—large bands of Texas communities were hit with a power outage that resulted from several severe winter storms that converged and swept across the nation. The outage, which was the consequence of an outdated [17], deregulated and privatized power grid operated by the Electric Reliability Council of Texas (ERCOT) that failed because it had not been weatherized, resulted in severe shortages of food, water, and heat for 4.5 million Texas businesses and homes, and led to the destruction of thousands of homeowner and business properties due to water pipes that froze and burst. The outage killed at least 151 people [18], demonstrating the growing impact of climate change on the built environment.
4. The Impact of COVID-19 and the Response of Public Health Systems
“the COVID-19 pandemic has exposed the vulnerability of our public health infrastructure and its relationship to housing. During this pandemic, the ability to shelter in place has been key to protecting ourselves and others from the spread of COVID-19. Those who are homeless lack a place to shelter, which puts them not only at higher risk of contracting the coronavirus, but also of spreading it to other vulnerable community members” [7].
5. Policy Interventions to Improve Infrastructure
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- National Law Center on Homelessness and Poverty. Homelessness in America: Overview of Data and Causes. Available online: https://www.nlchp.org/wp-content/uploads/2018/10/Homeless_Stats_Fact_Sheet.pdf (accessed on 19 May 2021).
- U.S. Department of Housing and Urban Development. The 2020 Annual Homeless Assessment Report (AHAR) to Congress (Part 1: Point-in-Time-Estimates of Homelessness). 2021. Available online: https://www.huduser.gov/portal/sites/default/files/pdf/2020-AHAR-Part-1.pdf (accessed on 16 May 2021).
- Hopper, K.; Shinn, M.; Laska, E.; Meisner, M.; Wanderling, J. Estimating numbers of unsheltered homeless people through plant-capture and postcount survey methods. Am. J. Public Health 2008, 98, 1438–1442. [Google Scholar] [CrossRef] [PubMed]
- Foscarinis, M. Homeless Problem Bigger than Our Leaders Think: Column. USA Today. 16 January 2014. Available online: https://www.usatoday.com/story/opinion/2014/01/16/homeless-problem-obama-america-recession-column/4539917/ (accessed on 19 May 2021).
- Tsai, J.; O’Toole, T.; Kearney, L.K. Homelessness as a public mental health and social problem: New knowledge and solutions. Psychol. Serv. 2017, 14, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Wong, A.; Chen, J.; Dicipulo, R.; Weiss, D.; Sleet, D.A.; Francescutti, L.H. Combatting homelessness in Canada: Applying lessons learned from six tiny villages to the Edmonton Bridge Healing Program. Int. J. Environ. Res. Public Health 2020, 17, 6279. [Google Scholar] [CrossRef] [PubMed]
- Community Solutions. Understanding Public Health and Homelessness. Available online: https://www.community.solutions/understanding-public-health-and-homelessness/ (accessed on 16 May 2021).
- World Health Organization (WHO). Social Determinants of Health. Available online: https://www.who.int/health-topics/social-determinants-of-health#tab=tab_1 (accessed on 19 May 2021).
- Centers for Disease Control and Prevention (CDC). About Social Determinants of Health. Available online: https://www.cdc.gov/socialdeterminants/about.html (accessed on 16 May 2021).
- Castañeda, E.; Smith, E.; Vetter, B. Hispanic health disparities and housing: Comparing measured and self-reported health metrics among housed and homeless Latin individuals. J. Migr. Health 2020, 1, 100008. [Google Scholar] [CrossRef] [PubMed]
- Joint Center for Housing Studies of Harvard University. State of the Nation’s Housing 2020. 2020. Available online: https://www.jchs.harvard.edu/sites/default/files/reports/files/Harvard_JCHS_The_State_of_the_Nations_Housing_2020_Report_Revised_120720.pdf (accessed on 18 July 2021).
- Center on Budget and Policy Priorities. Federal Housing Assistance Funding Remains Well Below 2010 Level. Available online: https://www.cbpp.org/federal-housing-assistance-funding-remains-well-below-2010-level (accessed on 19 July 2021).
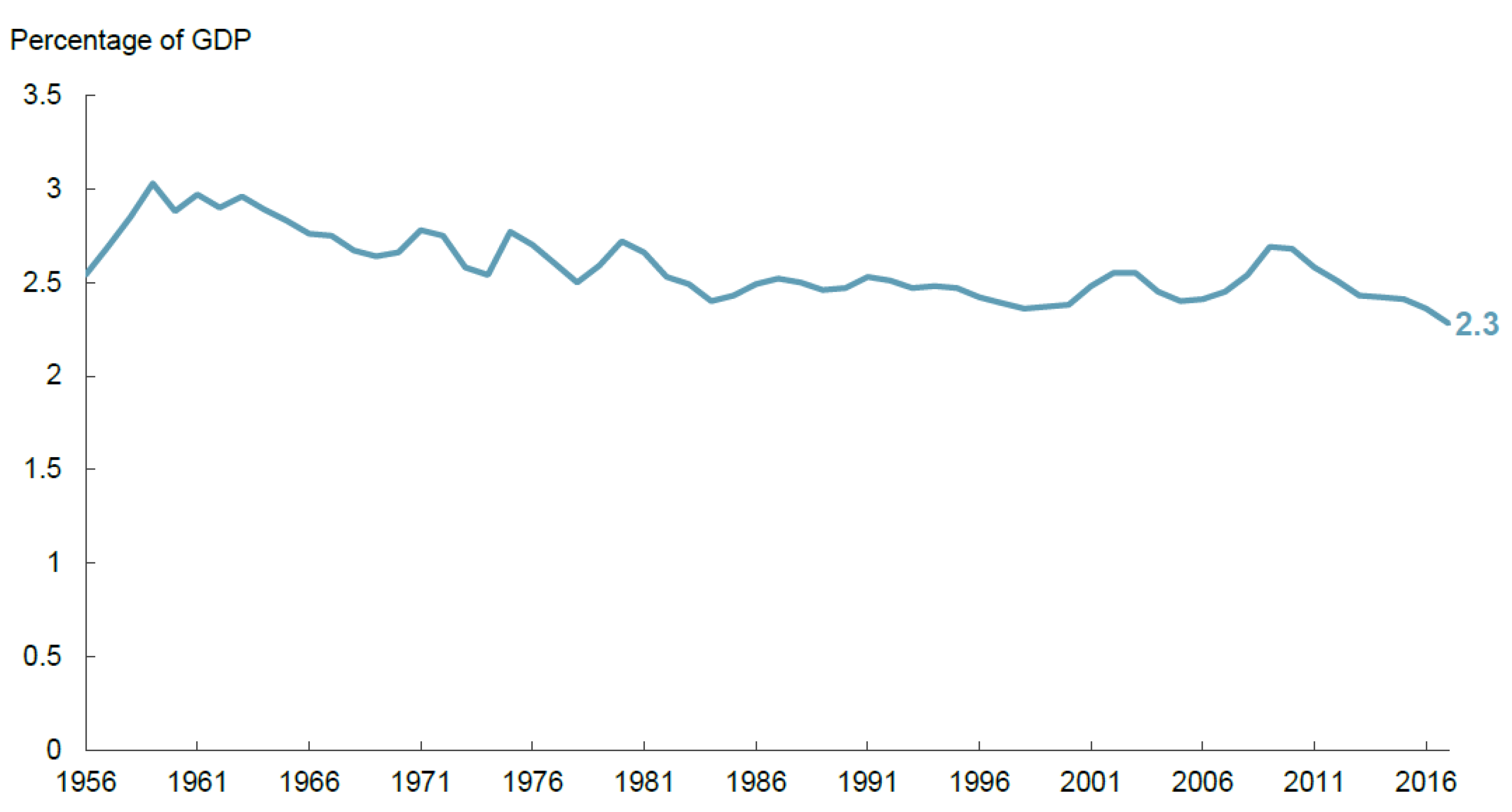
- Congressional Budget Office. October 2018. Public Spending on Transportation and Water Infrastructure, 1956 to 2017. Available online: https://www.cbo.gov/system/files/2018-10/54539-Infrastructure.pdf (accessed on 19 August 2021).
- National Public Radio (NPR). 10 Years After Bridge Collapse, America Is Still Crumbling. Available online: https://www.npr.org/2017/08/01/540669701/10-years-after-bridge-collapse-america-is-still-crumbling (accessed on 19 May 2021).
- National Public Radio (NPR). Hurricane Katrina: 10 Years of Recovery and Reflection. Available online: https://www.npr.org/series/429056277/hurricane-katrina-10-years-of-recovery-and-reflection (accessed on 19 May 2021).
- National Resources Defense Council (NRDC). Flint Water Crisis: Everything you Need to Know. Available online: https://www.nrdc.org/stories/flint-water-crisis-everything-you-need-know (accessed on 18 May 2021).
- Chrobak, U. The US Has More Power Outages Than Any Other Developed Country. Here’s Why. Popular Science. 17 August 2020. Available online: https://www.popsci.com/story/environment/why-us-lose-power-storms/ (accessed on 16 August 2021).
- National Public Radio (NPR). Growing Power Outages Pose Grave Threat to People Who Need Medical Equipment To Live. Available online: https://www.npr.org/sections/health-shots/2021/05/15/996872685/growing-power-outages-pose-grave-threat-to-people-who-need-medical-equipment-to- (accessed on 19 May 2021).
- Haviland, L. Op-ed: COVID-19 Homelessness Is a Public Health Problem—It’s about to Get Worse. Available online: https://www.sph.cuny.edu/life-at-sph/news/2021/03/24/op-ed-homeless/ (accessed on 22 May 2021).
- Johns Hopkins University & Medicine. Coronavirus Resource Center. Available online: https://coronavirus.jhu.edu/map.html (accessed on 14 August 2021).
- Allegrante, J.P.; Auld, M.E.; Natarajan, S. Preventing COVID-19 and its sequela: "There is no magic bullet… It’s just behaviors". Am. J. Prev. Med. 2020, 59, 288–292. [Google Scholar] [CrossRef] [PubMed]
- Koh, H. We Need One Response—Not 50—To Fight COVID-19. Available online: https://www.statnews.com/2020/05/22/we-need-one-response-to-fight-covid-19-not-50/ (accessed on 16 May 2021).
- Mays, G.P.; Smith, S.A. Evidence links increases in public health spending to declines in preventable deaths. Health Aff. 2011, 30, 1585–1593. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mays, G.P.; Marmaril, C.B.; Timsina, L.R. Preventable death rates fell where communities expanded population health activities through multisector networks. Health Aff. 2016, 35, 2005–2013. [Google Scholar] [CrossRef] [PubMed]
- IOM. For the Public’s Health: Investing in a Healthier Future; National Academy Press: Washington, DC, USA, 2012. [Google Scholar]
- Bradley, E.H.; Canavan, M.; Rogan, E. Variation in health outcomes: The role of spending on social services, public health, and health care, 2000–2009. Health Aff. 2016, 35, 760–768. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harvard, T.H. Robert Wood Johnson Foundation. Chan School of Public Health. The Public’s Perspective on the United States Public Health System. May 2021. Available online: https://www.rwjf.org/en/library/research/2021/05/the-publics-perspective-on-the-united-states-public-health-system.html?rid=003E000000yZwitIAC&et_cid=2459858 (accessed on 16 May 2021).
- McKillop, M.; Ilakkuvan, V. The Impact of Chronic Underfunding on America’s Public Health System: Trends, Risks, and Recommendations. 2021. Available online: https://www.resource.nlm.nih.gov/101751510 (accessed on 16 May 2021).
- HUD Nominee Marcia Fudge to Push for Financial Assistance, Affordable Housing Amid Coronavirus Crisis. The Washington Post. Available online: https://www.washingtonpost.com/business/2021/01/28/hud-fudge-confirmation-hearing/ (accessed on 22 May 2021).
- American Rescue Plan Act HOME Supplemental Allocations. Available online: https://www.hud.gov/sites/dfiles/CPD/documents/HOME-ARP.pdf (accessed on 22 May 2021).
- Stein, J.; Jan, T. Fears Mount about Impact of Coronavirus on Homeless. Available online: https://www.washingtonpost.com/business/2020/03/15/fears-mount-about-impact-coronavirus-homeless/ (accessed on 22 May 2021).
- Lowe, J. Los Angeles Goes to War with Itself over Homelessness. 2021. Available online: https://www.nytimes.com/2021/07/13/magazine/los-angeles-homelessness.html (accessed on 18 July 2021).
- Bassuk, E.L.; Hart, J.A.; Donovan, E. Resetting policies to end family homelessness. Ann. Rev. Public Health 2020, 41, 247–263. [Google Scholar] [CrossRef] [PubMed]
- Kim, K.; Garcia, I. Why do homeless families exit and return the homeless shelter? Factors affecting the risk of family homelessness in Salt Lake County (Utah, United States) as a case study. Int. J. Environ. Res. Public Health 2019, 16, 4328. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Francescutti, L.H.; Sleet, D.A. Homelessness and Public Health; Special Issue; MDPI: Basel, Switzerland, 2021. [Google Scholar]
- Kiesler, C.A. Homelessness and public policy priorities. Am. Psychol. 1991, 46, 1245–1252. [Google Scholar] [CrossRef] [PubMed]
- Saegert, S.C.; Klitzman, S.; Freudenberg, N.; Cooperman-Mroczek, J.; Nassar, S. Healthy housing: A structured review of published evaluations of US interventions to improve health by modifying housing in the United States, 1990–2001. Am. J. Public Health 2003, 93, 1471–1477. [Google Scholar] [CrossRef] [PubMed]
- Fowler, P.J.; Hovmand, P.S.; Marcal, K.E.; Das, S. Solving homelessness from a complex systems perspective: Insights for prevention responses. Ann. Rev. Public Health 2019, 40, 465–486. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Livingood, W.C.; Allegrante, J.P.; Airhihenbuwa, C.O.; Clark, N.M.; Windsor, R.C.; Zimmerman, M.A.; Green, L.W. Applied social and behavioral science to address complex health problems. Am. J. Prev. Med. 2011, 41, 525–531. [Google Scholar] [CrossRef] [PubMed]
- Dourado, E. We Must Build Our Way Out of This Mess: Guest Essay. The New York Times, 11 August 2021. Available online: https://www.nytimes.com/2021/08/11/opinion/politics/we-need-to-build-our-way-out-of-this-mess.html(accessed on 16 August 2021).

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Allegrante, J.P.; Sleet, D.A. Investing in Public Health Infrastructure to Address the Complexities of Homelessness. Int. J. Environ. Res. Public Health 2021, 18, 8887. https://doi.org/10.3390/ijerph18168887
Allegrante JP, Sleet DA. Investing in Public Health Infrastructure to Address the Complexities of Homelessness. International Journal of Environmental Research and Public Health. 2021; 18(16):8887. https://doi.org/10.3390/ijerph18168887
Chicago/Turabian StyleAllegrante, John P., and David A. Sleet. 2021. "Investing in Public Health Infrastructure to Address the Complexities of Homelessness" International Journal of Environmental Research and Public Health 18, no. 16: 8887. https://doi.org/10.3390/ijerph18168887
APA StyleAllegrante, J. P., & Sleet, D. A. (2021). Investing in Public Health Infrastructure to Address the Complexities of Homelessness. International Journal of Environmental Research and Public Health, 18(16), 8887. https://doi.org/10.3390/ijerph18168887