
The Role of Coping Strategies in Post-Traumatic Growth among Syrian Refugees: A Structural Equation Model

 ,
,  ,
,  ,
,
Abstract
:1. Introduction
- Post-traumatic growth would be positively associated with past traumatic experiences, but negatively associated with post-migration stressors.
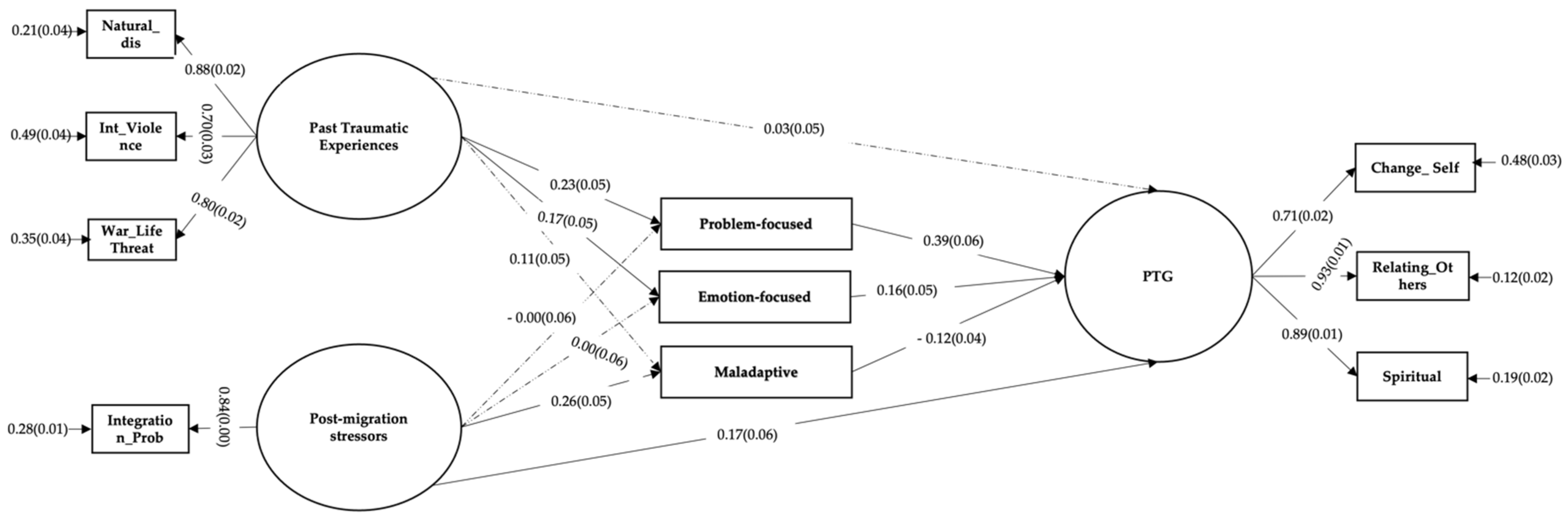
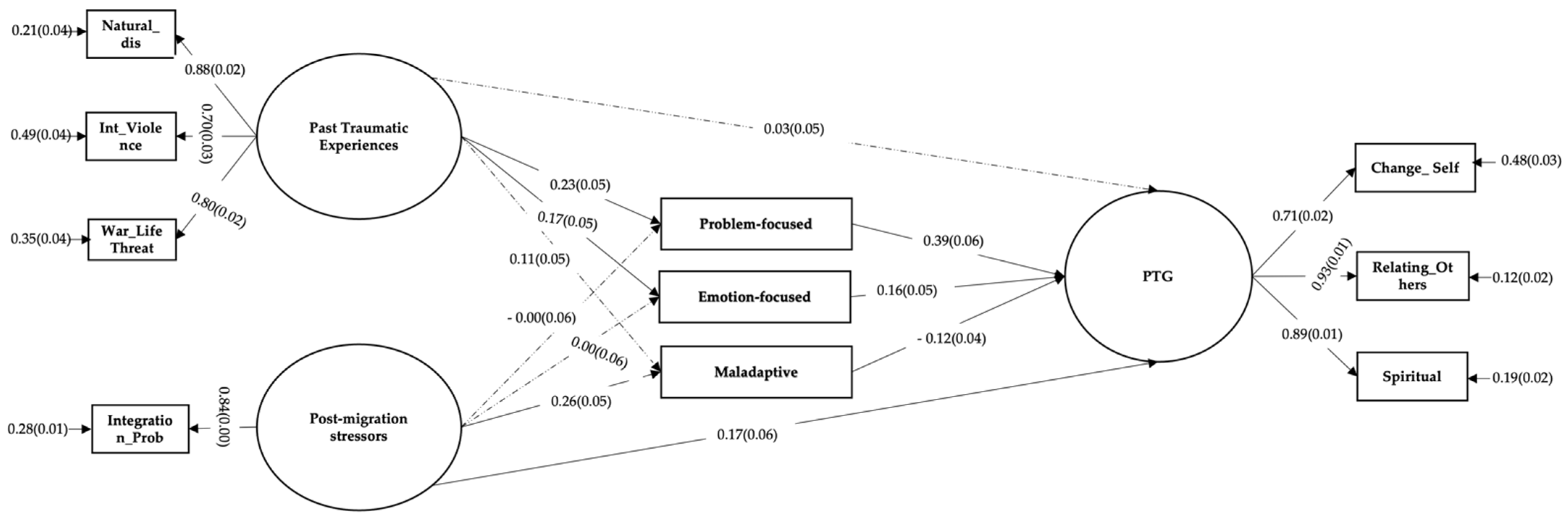
- Coping strategies would mediate the association between multiple past traumatic experiences and PTG such that past traumatic experiences would be associated with higher use of problem-focused and emotion-focused coping strategies which would predict higher PTG and higher use of maladaptive coping strategies which would predict lower PTG.
- Coping strategies would mediate the association between post-migration stressors and PTG such that post-migration stressors would be associated with lower use of problem-focused and emotion-focused and higher use of maladaptive coping strategies which would predict lower PTG.
2. Materials and Methods
2.1. Participants and Procedure
2.2. Measurements
2.2.1. Past Traumatic Experiences
2.2.2. Post-Traumatic Growth
2.2.3. Coping Strategies
2.2.4. Post-Migration Stressors
2.3. Statistical Analyses
3. Results
3.1. Preliminary Analyses
3.2. Direct and Indirect Associations
4. Discussion
4.1. Traumatic Experiences, Post-Migration Stressors and Post-Traumatic Growth
4.2. Coping Strategies as a Mediator between Traumatic Experiences, Post-Migration Stressors and, Post-Traumatic Growth
4.3. Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- United Nations High Commissioner for Refugees (UNHCR). Refugee Data Finder. Available online: https://www.unhcr.org/refugee-statistics/ (accessed on 14 May 2021).
- Kılıç, C.; Magruder, K.M.; Koryürek, M.M. Does Trauma Type Relate to Posttraumatic Growth after War? A Pilot Study of Young Iraqi War Survivors Living in Turkey. Transcult. Psychiatry 2016, 53, 110–123. [Google Scholar] [CrossRef] [PubMed]
- Teodorescu, D.-S.; Siqveland, J.; Heir, T.; Hauff, E.; Wentzel-Larsen, T.; Lien, L. Posttraumatic Growth, Depressive Symptoms, Posttraumatic Stress Symptoms, Post-Migration Stressors and Quality of Life in Multi-Traumatized Psychiatric Outpatients with a Refugee Background in Norway. Health Qual. Life Outcomes 2012, 10, 84. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Carlsson, J.; Sonne, C. Mental Health, Pre-migratory Trauma and Post-migratory Stressors Among Adult Refugees. In Mental Health of Refugee and Conflict-Affected Populations: Theory, Research and Clinical Practice; Morina, N., Nickerson, A., Eds.; Springer International Publishing: Cham, Switzerland, 2018; pp. 15–35. ISBN 978-3-319-97045-5. [Google Scholar]
- Giacco, D.; Laxhman, N.; Priebe, S. Prevalence of and Risk Factors for Mental Disorders in Refugees. Semin. Cell Dev. Biol. 2018, 77, 144–152. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, H.; Hassan, C.Q. Post-Traumatic Stress Disorder Symptoms Resulting from Torture and Other Traumatic Events among Syrian Kurdish Refugees in Kurdistan Region, Iraq. Front. Psychol. 2017, 8, 241. [Google Scholar] [CrossRef] [PubMed]
- Young, M.Y.; Chan, K.J. The psychological experience of refugees: A gender and cultural analysis. In Psychology of Gender through the Lens of Culture: Theories and Applications; Springer International Publishing: Cham, Switzerland, 2015; pp. 17–36. ISBN 978-3-319-14004-9. [Google Scholar]
- Acarturk, C.; Cetinkaya, M.; Senay, I.; Gulen, B.; Aker, T.; Hinton, D. Prevalence and Predictors of Posttraumatic Stress and Depression Symptoms Among Syrian Refugees in a Refugee Camp. J. Nerv. Ment. Dis. 2018, 206, 40–45. [Google Scholar] [CrossRef]
- Chu, T.; Keller, A.S.; Rasmussen, A. Effects of Post-Migration Factors on PTSD Outcomes among Immigrant Survivors of Political Violence. J. Immigr. Minor. Health 2013, 15, 890–897. [Google Scholar] [CrossRef] [PubMed]
- Georgiadou, E.; Zbidat, A.; Schmitt, G.M.; Erim, Y. Prevalence of Mental Distress Among Syrian Refugees With Residence Permission in Germany: A Registry-Based Study. Front. Psychiatry 2018, 9, 393. [Google Scholar] [CrossRef] [Green Version]
- Porter, M.; Haslam, N. Predisplacement and Postdisplacement Factors Associated with Mental Health of Refugees and Internally Displaced Persons: A Meta-Analysis. JAMA 2005, 294, 602–612. [Google Scholar] [CrossRef] [PubMed]
- Schweitzer, R.D.; Brough, M.; Vromans, L.; Asic-Kobe, M. Mental Health of Newly Arrived Burmese Refugees in Australia: Contributions of Pre-Migration and Post-Migration Experience. Aust. N. Z. J. Psychiatry 2011, 45, 299–307. [Google Scholar] [CrossRef] [Green Version]
- Joseph, S.; Linley, P.A. Positive Adjustment to Threatening Events: An Organismic Valuing Theory of Growth through Adversity. Rev. Gen. Psychol. 2005, 9, 262–280. [Google Scholar] [CrossRef]
- Rizkalla, N.; Segal, S.P. Well-Being and Posttraumatic Growth Among Syrian Refugees in Jordan. J. Trauma. Stress 2018, 31, 213–222. [Google Scholar] [CrossRef]
- Waysman, M.; Schwarzwald, J.; Solomon, Z. Hardiness: An Examination of Its Relationship with Positive and Negative Long Term Changes Following Trauma. J. Trauma. Stress 2001, 14, 531–548. [Google Scholar] [CrossRef]
- Tedeschi, R.G.; Calhoun, L.G. A Clinical Approach to Posttraumatic Growth. In Positive Psychology in Practice; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2004; pp. 405–419. ISBN 978-0-471-45906-4. [Google Scholar]
- Bhat, R.M.; Rangaiah, B. The Impact of Conflict Exposure and Social Support on Posttraumatic Growth among the Young Adults in Kashmir. Cogent Psychol. 2015, 2, 1000077. [Google Scholar] [CrossRef]
- Hussain, D.; Bhushan, B. Posttraumatic Stress and Growth among Tibetan Refugees: The Mediating Role of Cognitive-Emotional Regulation Strategies. J. Clin. Psychol. 2011, 67, 720–735. [Google Scholar] [CrossRef]
- Powell, S.; Rosner, R.; Butollo, W.; Tedeschi, R.G.; Calhoun, L.G. Posttraumatic Growth after War: A Study with Former Refugees and Displaced People in Sarajevo. J. Clin. Psychol. 2003, 59, 71–83. [Google Scholar] [CrossRef]
- Sleijpen, M.; Haagen, J.; Mooren, T.; Kleber, R.J. Growing from Experience: An Exploratory Study of Posttraumatic Growth in Adolescent Refugees. Eur. J. Psychotraumatol. 2016, 7, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Bayer-Topilsky, T.; Itzhaky, H.; Dekel, R.; Marmor, Y.N. Mental Health and Posttraumatic Growth in Civilians Exposed to Ongoing Terror. J. Loss Trauma 2013, 18, 227–247. [Google Scholar] [CrossRef]
- Kira, I.A.; Aboumediene, S.; Ashby, J.S.; Odenat, L.; Mohanesh, J.; Alamia, H. The Dynamics of Posttraumatic Growth Across Different Trauma Types in a Palestinian Sample. J. Loss Trauma 2013, 18, 120–139. [Google Scholar] [CrossRef]
- Kroo, A.; Nagy, H. Posttraumatic Growth Among Traumatized Somali Refugees in Hungary. J. Loss Trauma 2011, 16, 440–458. [Google Scholar] [CrossRef]
- Ersahin, Z. Post-Traumatic Growth among Syrian Refugees in Turkey: The Role of Coping Strategies and Religiosity. Curr. Psychol. 2020, 1–10. [Google Scholar] [CrossRef]
- Wen, K.; McGrath, M.; Acarturk, C.; Ilkkursun, Z.; Fuhr, D.C.; Sondorp, E.; Cuijpers, P.; Sijbrandij, M.; Roberts, B. Post-Traumatic Growth and Its Predictors among Syrian Refugees in Istanbul: A Mental Health Population Survey. J. Migr. Health 2020, 1–2, 100010. [Google Scholar] [CrossRef] [PubMed]
- Tedeschi, R.G.; Calhoun, L. Posttraumatic growth: A new perspective on psychotraumatology. Psychiatr. Times 2004, 21, 58–60. [Google Scholar]
- Helgeson, V.S.; Reynolds, K.A.; Tomich, P.L. A Meta-Analytic Review of Benefit Finding and Growth. J. Consult. Clin. Psychol. 2006, 74, 797–816. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ickovics, J.R.; Meade, C.S.; Kershaw, T.S.; Milan, S.; Lewis, J.B.; Ethier, K.A. Urban Teens: Trauma, Posttraumatic Growth, and Emotional Distress among Female Adolescents. J. Consult. Clin. Psychol. 2006, 74, 841–850. [Google Scholar] [CrossRef]
- Shakespeare-Finch, J.; Armstrong, D. Trauma Type and Posttrauma Outcomes: Differences Between Survivors of Motor Vehicle Accidents, Sexual Assault, and Bereavement. J. Loss Trauma 2010, 15, 69–82. [Google Scholar] [CrossRef] [Green Version]
- Brooks, M.; Graham-Kevan, N.; Robinson, S.; Lowe, M. Trauma Characteristics and Posttraumatic Growth: The Mediating Role of Avoidance Coping, Intrusive Thoughts, and Social Support. Psychol. Trauma Theory Res. Pract. Policy 2019, 11, 232–238. [Google Scholar] [CrossRef] [Green Version]
- Kira, I.; Lewandowski, L.; Somers, C.L.; Yoon, J.S.; Chiodo, L. The Effects of Trauma Types, Cumulative Trauma, and PTSD on IQ in Two Highly Traumatized Adolescent Groups. Psychol. Trauma Theory Res. Pract. Policy 2012, 4, 128–139. [Google Scholar] [CrossRef]
- Peterson, C.; Park, N.; Pole, N.; D’Andrea, W.; Seligman, M.E.P. Strengths of Character and Posttraumatic Growth. J. Trauma Stress 2008, 21, 214–217. [Google Scholar] [CrossRef]
- Shigemoto, Y.; Poyrazli, S. Factors Related to Posttraumatic Growth in U.S. and Japanese College Students. Psychol. Trauma Theory Res. Pract. Policy 2013, 5, 128–134. [Google Scholar] [CrossRef]
- Mollica, R.F.; McInnes, K.; Poole, C.; Tor, S. Dose-Effect Relationships of Trauma to Symptoms of Depression and Post-Traumatic Stress Disorder among Cambodian Survivors of Mass Violence. Br. J. Psychiatry 1998, 173, 482–488. [Google Scholar] [CrossRef]
- Steel, Z.; Chey, T.; Silove, D.; Marnane, C.; Bryant, R.A.; van Ommeren, M. Association of Torture and Other Potentially Traumatic Events with Mental Health Outcomes among Populations Exposed to Mass Conflict and Displacement: A Systematic Review and Meta-Analysis. JAMA 2009, 302, 537–549. [Google Scholar] [CrossRef]
- Berger, R.; Weiss, T. Immigration and Posttraumatic Growth-A Missing Link. J. Immigr. Refug. Serv. 2003, 1, 21–39. [Google Scholar] [CrossRef]
- Lindencrona, F.; Ekblad, S.; Hauff, E. Mental health of recently resettled refugees from the Middle East in Sweden: The impact of pre-resettlement trauma, resettlement stress and capacity to handle stress. Soc. Psychiatry Psychiatr. Epidemiol. 2008, 43, 121–131. [Google Scholar] [CrossRef] [PubMed]
- Aragona, M.; Pucci, D.; Mazzetti, M.; Maisano, B.; Geraci, S. Traumatic events, post-migration living difficulties and post-traumatic symptoms in first generation immigrants: A primary care study. Ann. Dell’Istituto Super. di Sanita 2013, 49, 169–175. [Google Scholar]
- Hecker, T.; Huber, S.; Maier, T.; Maercker, A. Differential associations among PTSD and complex PTSD symptoms and traumatic experiences and postmigration difficulties in a culturally diverse refugee sample. J. Trauma. Stress 2018, 31, 795–804. [Google Scholar] [CrossRef]
- Park, C.L.; Fenster, J.R. Stress-Related Growth: Predictors of Occurrence and Correlates with Psychological Adjustment. J. Soc. Clin. Psychol. 2004, 23, 195–215. [Google Scholar] [CrossRef]
- Prati, G.; Pietrantoni, L. Optimism, Social Support, and Coping Strategies As Factors Contributing to Posttraumatic Growth: A Meta-Analysis. J. Loss Trauma 2009, 14, 364–388. [Google Scholar] [CrossRef] [Green Version]
- Lazarus, R.S.; Folkman, S. Transactional Theory and Research on Emotions and Coping. Eur. J. Personal. 1987, 1, 141–169. [Google Scholar] [CrossRef]
- Carver, C.S.; Scheier, M.F.; Weintraub, J.K. Assessing Coping Strategies: A Theoretically Based Approach. J. Personal. Soc. Psychol. 1989, 56, 267–283. [Google Scholar] [CrossRef]
- Littleton, H.; Horsley, S.; John, S.; Nelson, D.V. Trauma coping strategies and psychological distress: A meta-analysis. J. Trauma. Stress: Off. Publ. Int. Soc. Trauma. Stress Stud. 2007, 20, 977–988. [Google Scholar] [CrossRef]
- Folkman, S.; Moskowitz, J.T. Coping: Pitfalls and promise. Annu. Rev. Psychol. 2004, 4, 745–774. [Google Scholar] [CrossRef] [PubMed]
- Masel, C.N.; Terry, D.J.; Gribble, M. The effects of coping on adjustment: Re-examining the goodness of fit model of coping effectiveness. Anxiety Stress Coping 1996, 9, 279–300. [Google Scholar] [CrossRef]
- Kurt, G.; Acar, İ.H.; Ilkkursun, Z.; Yurtbakan, T.; Acar, B.; Uygun, E.; Acarturk, C. Traumatic Experiences, Acculturation, and Psychological Distress among Syrian Refugees in Turkey: The Mediating Role of Coping Strategies. Int. J. Intercult. Relat. 2021, 81, 214–225. [Google Scholar] [CrossRef]
- Woltin, K.A.; Sassenberg, K.; Albayrak, N. Regulatory Focus, Coping Strategies and Symptoms of Anxiety and Depression: A Comparison between Syrian Refugees in Turkey and Germany. PLoS ONE 2018, 13, e0206522. [Google Scholar] [CrossRef] [Green Version]
- Amir, M.; Kaplan, Z.; Efroni, R.; Levine, Y.; Benjamin, J.; Kotler, M. Coping Styles in Post-Traumatic Stress Disorder (PTSD) Patients. Personal. Individ. Differ. 1997, 23, 399–405. [Google Scholar] [CrossRef]
- Emmelkamp, J.; Komproe, I.H.; Van Ommeren, M.; Schagen, S. The relation between coping, social support and psychological and somatic symptoms among torture survivors in Nepal. Psychol. Med. 2002, 32, 1465–1470. [Google Scholar] [CrossRef] [PubMed]
- Araya, M.; Chotai, J.; Komproe, I.H.; de Jong, J.T. Gender differences in traumatic life events, coping strategies, perceived social support and sociodemographics among postconflict displaced persons in Ethiopia. Soc. Psychiatry Psychiatr. Epidemiol. 2007, 42, 307–315. [Google Scholar] [CrossRef]
- Litman, J.A. The COPE Inventory: Dimensionality and Relationships with Approach- and Avoidance-Motives and Positive and Negative Traits. Personal. Individ. Differ. 2006, 41, 273–284. [Google Scholar] [CrossRef]
- Low, C.A.; Stanton, A.L.; Thompson, N.; Kwan, L.; Ganz, P.A. Contextual Life Stress and Coping Strategies as Predictors of Adjustment to Breast Cancer Survivorship. Ann. Behav. Med. 2006, 32, 235–244. [Google Scholar] [CrossRef] [PubMed]
- Larsen, S.E.; Berenbaum, H. Are Specific Emotion Regulation Strategies Differentially Associated with Posttraumatic Growth versus Stress? Journal of Aggression. Maltreatment Trauma 2015, 24, 794–808. [Google Scholar] [CrossRef]
- Hagenaars, M.A.; Fisch, I.; van Minnen, A. The Effect of Trauma Onset and Frequency on PTSD-Associated Symptoms. J. Affect Disord. 2011, 132, 192–199. [Google Scholar] [CrossRef] [Green Version]
- London, M.J.; Mercer, M.C.; Lilly, M.M. Considering the Impact of Early Trauma on Coping and Pathology to Predict Posttraumatic Growth Among 9-1-1 Telecommunicators. J. Interpers. Violence 2020, 35, 4709–4731. [Google Scholar] [CrossRef] [PubMed]
- Zoellner, T.; Maercker, A. Posttraumatic Growth in Clinical Psychology—A Critical Review and Introduction of a Two Component Model. Clin. Psychol. Rev. 2006, 26, 626–653. [Google Scholar] [CrossRef]
- Butler, L.D.; Blasey, C.M.; Garlan, R.W.; McCaslin, S.E.; Azarow, J.; Chen, X.-H.; Desjardins, J.C.; DiMiceli, S.; Seagraves, D.A.; Hastings, T.A.; et al. Posttraumatic Growth Following the Terrorist Attacks of September 11, 2001: Cognitive, Coping, and Trauma Symptom Predictors in an Internet Convenience Sample. Traumatology 2005, 11, 247–267. [Google Scholar] [CrossRef]
- Kato, T. Development of the Coping Flexibility Scale: Evidence for the Coping Flexibility Hypothesis. J. Couns. Psychol. 2012, 59, 262–273. [Google Scholar] [CrossRef] [PubMed]
- Ai, A.L.; Tice, T.N.; Whitsett, D.D.; Ishisaka, T.; Chim, M. Posttraumatic Symptoms and Growth of Kosovar War Refugees: The Influence of Hope and Cognitive Coping. J. Posit. Psychol. 2007, 2, 55–65. [Google Scholar] [CrossRef]
- Penrod, J.; Preston, D.B.; Cain, R.E.; Starks, M.T. A discussion of chain referral as a method of sampling hard-to-reach populations. J. Transcult. Nurs. 2003, 14, 100–107. [Google Scholar] [CrossRef] [PubMed]
- Weathers, F.W.; Blake, D.D.; Schnurr, P.P.; Kaloupek, D.G.; Marx, B.P.; Keane, T.M. The Life Events Checklist for DSM-5 (LEC-5) 2013. Instrument Available from the National Center for PTSD. Available online: www.ptsd.va.go (accessed on 20 September 2018).
- Gray, M.J.; Litz, B.T.; Hsu, J.L.; Lombardo, T.W. Psychometric Properties of the Life Events Checklist. Assessment 2004, 11, 330–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sezgin, A.U.; Punamäki, R.-L. Type of Traumatic Events, Mental Health Problems, and Posttraumatic Cognitions Among Eastern Anatolian Women. J. Interpers. Violence 2019. [Google Scholar] [CrossRef]
- Kira, I.; Abou-Median, S.; Ashby, J.; Lewandowski, L.; Mohanesh, J.; Odenat, L. Post-Traumatic Growth Inventory: Psychometric Properties of the Arabic Version in Palestinian Adults. Int. J. Educ. Psychol. Assess. 2012, 11, 120–137. [Google Scholar]
- Salo, J.A.; Qouta, S.; Punamäki, R.-L. Adult Attachment, Posttraumatic Growth and Negative Emotions among Former Political Prisoners. Anxiety. Stress Coping 2005, 18, 361–378. [Google Scholar] [CrossRef]
- Schick, M.; Zumwald, A.; Knöpfli, B.; Nickerson, A.; Bryant, R.A.; Schnyder, U.; Müller, J.; Morina, N. Challenging Future, Challenging Past: The Relationship of Social Integration and Psychological Impairment in Traumatized Refugees. Eur. J. Psychotraumatol. 2016, 7, 28057. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- IBM Corp. IBM SPSS Statistics for Windows, Version 23.0; IBM Corp: Armonk, NY, USA, 2015. [Google Scholar]
- Muthén, L.K.; Muthén, B.O. Mplus User’s Guide, 8th ed.; Muthén & Muthén: Los Angeles, CA, USA, 2017. [Google Scholar]
- Kline, R.B. Principles and Practice of Structural Equation Modeling, 3rd ed.; Guilford Press: New York, NY, USA, 2011; ISBN 978-1-60623-877-6. [Google Scholar]
- Enders, C. Applied Missing Data Analysis; The Guilford Press: New York, NY, USA, 2010. [Google Scholar]
- Durlak, J.A. How to Select, Calculate, and Interpret Effect Sizes. J. Pediatric Psychol. 2009, 34, 917–928. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayduk, L.A. Structural Equation Modeling with LISREL: Essentials and Advances; Johns Hopkins University Press: Baltimore, MD, USA, 1987; ISBN 978-0-8018-3478-3. [Google Scholar]
- Wang, J.; Wang, X. Structural Equation Modeling: Applications Using Mplus; John Wiley & Sons: Hoboken, NJ, USA, 2019; ISBN 978-1-119-42271-6. [Google Scholar]
- Sangalang, C.C.; Becerra, D.; Mitchell, F.M.; Lechuga-Peña, S.; Lopez, K.; Kim, I. Trauma, Post-Migration Stress, and Mental Health: A Comparative Analysis of Refugees and Immigrants in the United States. J. Immigr. Minor. Health 2019, 21, 909–919. [Google Scholar] [CrossRef] [Green Version]
- Chan, K.J.; Young, M.Y.; Sharif, N. Well-Being after Trauma: A Review of Posttraumatic Growth among Refugees. Can. Psychol. Psychol. Can. 2016, 57, 291–299. [Google Scholar] [CrossRef]
- MacKinnon, D.P.; Fairchild, A.J.; Fritz, M.S. Mediation Analysis. Annu. Rev. Psychol. 2007, 58, 593. [Google Scholar] [CrossRef]
- Brown, T.A. Confirmatory Factor Analysis for Applied Research; The Guilford Press: New York, NY, USA, 2006; ISBN 978-1-59385-274-0. [Google Scholar]
- Frazier, P.A.; Burnett, J.W. Immediate Coping Strategies Among Rape Victims. J. Couns. Dev. 1994, 72, 633–639. [Google Scholar] [CrossRef]
- McMillen, C.; Zuravin, S.; Rideout, G. Perceived Benefit from Child Sexual Abuse. J. Consult. Clin. Psychol. 1995, 63, 1037–1043. [Google Scholar] [CrossRef]
- Tedeschi, R.G.; Park, C.L.; Calhoun, L.G. (Eds.) Posttraumatic Growth: Positive Changes in the Aftermath of Crisis; Lawrence Erlbaum Associates Publishers: Mahwah, NJ, USA, 1998; ISBN 978-0-8058-2319-6. [Google Scholar]
- Tinghög, P.; Malm, A.; Arwidson, C.; Sigvardsdotter, E.; Lundin, A.; Saboonchi, F. Prevalence of mental ill health, traumas and postmigration stress among refugees from Syria resettled in Sweden after 2011: A population-based survey. BMJ Open 2017, 7, e018899. [Google Scholar] [CrossRef] [Green Version]
- Borho, A.; Viazminsky, A.; Morawa, E.; Schmitt, G.M.; Georgiadou, E.; Erim, Y. The prevalence and risk factors for mental distress among Syrian refugees in Germany: A register-based follow-up study. BMC Psychiatry 2020, 20, 1–3. [Google Scholar] [CrossRef]
- Lazarus, R.S. Hope: An Emotion and a Vital Coping Resource Against Despair. Soc. Res. 1999, 66, 653–678. [Google Scholar]
- Kuo, B.C.H. Coping, Acculturation, and Psychological Adaptation among Migrants: A Theoretical and Empirical Review and Synthesis of the Literature. Health Psychol. Behav. Med. 2014, 2, 16–33. [Google Scholar] [CrossRef]
- Li, S.S.Y.; Liddell, B.J.; Nickerson, A. The Relationship Between Post-Migration Stress and Psychological Disorders in Refugees and Asylum Seekers. Curr. Psychiatry Rep. 2016, 18, 82. [Google Scholar] [CrossRef] [PubMed]
- Solberg, M.A.; Gridley, M.K.; Peters, R.M. The Factor Structure of the Brief Cope: A Systematic Review. West. J. Nurs. Res. 2021, 4, 01939459211012044. [Google Scholar]
- Hammen, C.; Marks, T.; Mayol, A.; DeMayo, R. Depressive self-schemas, life stress, and vulnerability to depression. J. Abnorm. Psychol. 1985, 94, 308. [Google Scholar] [CrossRef] [PubMed]
- Holahan, C.J.; Moos, R.H.; Holahan, C.K.; Brennan, P.L.; Schutte, K.K. Stress generation, avoidance coping, and depressive symptoms: A 10-year model. J. Consult. Clin. Psychol. 2005, 73, 658. [Google Scholar] [CrossRef] [Green Version]
- Jenzer, T.; Meisel, S.N.; Blayney, J.A.; Colder, C.R.; Read, J.P. Reciprocal processes in trauma and coping: Bidirectional effects over a four-year period. Psychol. Trauma Theory Res. Pract. Policy 2020, 12, 207. [Google Scholar] [CrossRef]
- Moos, R.H.; Holahan, C.J. Dispositional and contextual perspectives on coping: Toward an integrative framework. J. Clin. Psychol. 2003, 59, 1387–1403. [Google Scholar] [CrossRef]
- Dekel, S.; Ein-Dor, T.; Solomon, Z. Posttraumatic Growth and Posttraumatic Distress: A Longitudinal Study. Psychol. Trauma Theory Res. Pract. Policy 2012, 4, 94–101. [Google Scholar] [CrossRef] [Green Version]
- Stockton, H.; Hunt, N.; Joseph, S. Cognitive Processing, Rumination, and Posttraumatic Growth. J. Trauma Stress 2011, 24, 85–92. [Google Scholar] [CrossRef]
- Trenado, C.; Pedroarena-Leal, N.; Ruge, D. Considering the role of neurodidactics in medical education as inspired by learning studies and music education. Med. Sci. Educ. 2021, 31, 267–272. [Google Scholar] [CrossRef]
- Pinzón-Espinosa, J.; Valdés-Florido, M.J.; Riboldi, I.; Baysak, E.; Vieta, E.; EFPT Psychiatry Across Borders Working Group. The COVID-19 pandemic and mental health of refugees, asylum seekers, and migrants. J. Affect. Disord. 2020, 10, 407–408. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variable | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. PTG-self | - | ||||||||||||
| 2. PTG-spiritual | 0.84 ** | - | |||||||||||
| 3. PTG-relation | 0.66 ** | 0.62 ** | - | ||||||||||
| 4. Natural_dis | 0.14 ** | 0.19 ** | 0.13 ** | - | |||||||||
| 5. Int_Violence | 0.02 | 0.04 | 0.12 ** | 0.62 ** | - | ||||||||
| 6. War_lifethreat | 0.13 ** | 0.19 ** | 0.08 | 0.71 ** | 0.57 ** | - | |||||||
| 7. Integration prob | 0.08 * | 0.21 ** | 0.12 ** | 0.22 ** | 0.19 ** | 0.17 ** | - | ||||||
| 8. Problemfocus | 0.46 ** | 0.46 ** | 0.41 ** | 0.21 ** | 0.16 ** | 0.22 ** | 0.04 | - | |||||
| 9. Emotionfocus | 0.36 ** | 0.35 ** | 0.42 ** | 0.17 ** | 0.12 ** | 0.15 ** | 0.03 | 0.70 ** | - | ||||
| 10. Maladaptive | 0.01 | 0.02 | 0.20 ** | 0.16 ** | 0.19 ** | 0.05 | 0.23 ** | 0.17 ** | 0.27 ** | - | |||
| 11. Age | −0.13 ** | −0.08 * | 0.02 | 0.02 | 0.06 | 0.02 | 0.04 | −0.01 | 0.06 | −0.04 | - | ||
| 12. LOS | 0.01 | −0.08 | 0.07 | −0.14 ** | −0.03 | −0.15 ** | −0.04 | 0.0 | 0.02 | 0.0 | 0.08 * | - | |
| 13. Sex (1:F 2:M) | 0.07 | 0.0 | 0.12 ** | −0.12 ** | −0.17 ** | −0.08 | 0.0 | 0.0 | 0.01 | −0.04 | −0.20 ** | −0.09 * | - |
| n | 528 | 528 | 528 | 528 | 528 | 528 | 528 | 528 | 528 | 528 | 525 | 515 | |
| M | 3.05 | 3.05 | 2.39 | 1.97 | 1.62 | 1.93 | 1.78 | 2.97 | 3.01 | 2.19 | 35.6 | 65.98 | |
| SD | 1.14 | 1.11 | 1.16 | 0.68 | 0.67 | 0.75 | 0.89 | 0.61 | 0.5 | 0.64 | 11.65 | 24.04 | |
| Range | 0–5 | 0–5 | 0–5 | 1–4 | 1–4 | 1–4 | 0–4 | 1–4 | 1–4 | 1–4 | 18–77 | 2–144 | |
| Skewness | 0.02 | −0.47 | −0.43 | 0.51 | 1.12 | 0.44 | 0.16 | −0.47 | −0.58 | 0.07 | 0.83 | −0.154 | |
| Kurtosis | −0.66 | −0.23 | −0.47 | −0.24 | 0.98 | −0.77 | −0.44 | 0.11 | 0.69 | −0.76 | 0.27 | −0.118 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Acar, B.; Acar, İ.H.; Alhiraki, O.A.; Fahham, O.; Erim, Y.; Acarturk, C. The Role of Coping Strategies in Post-Traumatic Growth among Syrian Refugees: A Structural Equation Model. Int. J. Environ. Res. Public Health 2021, 18, 8829. https://doi.org/10.3390/ijerph18168829
Acar B, Acar İH, Alhiraki OA, Fahham O, Erim Y, Acarturk C. The Role of Coping Strategies in Post-Traumatic Growth among Syrian Refugees: A Structural Equation Model. International Journal of Environmental Research and Public Health. 2021; 18(16):8829. https://doi.org/10.3390/ijerph18168829
Chicago/Turabian StyleAcar, Busra, İbrahim H. Acar, Omar A. Alhiraki, Ola Fahham, Yesim Erim, and Ceren Acarturk. 2021. "The Role of Coping Strategies in Post-Traumatic Growth among Syrian Refugees: A Structural Equation Model" International Journal of Environmental Research and Public Health 18, no. 16: 8829. https://doi.org/10.3390/ijerph18168829
APA StyleAcar, B., Acar, İ. H., Alhiraki, O. A., Fahham, O., Erim, Y., & Acarturk, C. (2021). The Role of Coping Strategies in Post-Traumatic Growth among Syrian Refugees: A Structural Equation Model. International Journal of Environmental Research and Public Health, 18(16), 8829. https://doi.org/10.3390/ijerph18168829