
Process Improvement Approaches for Increasing the Response of Emergency Departments against the COVID-19 Pandemic: A Systematic Review

 , and
, and
Abstract
:1. Introduction
2. Methods
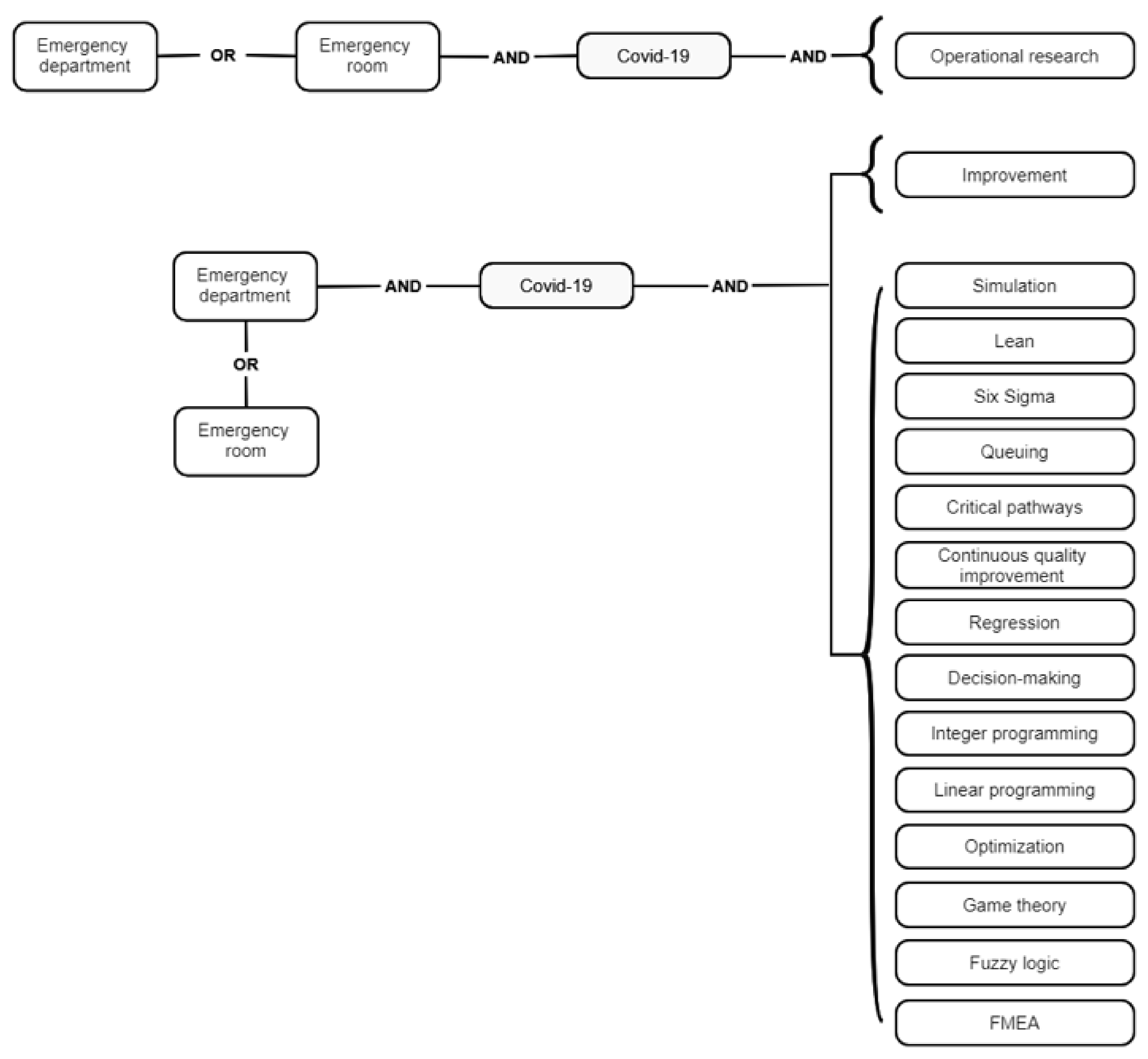
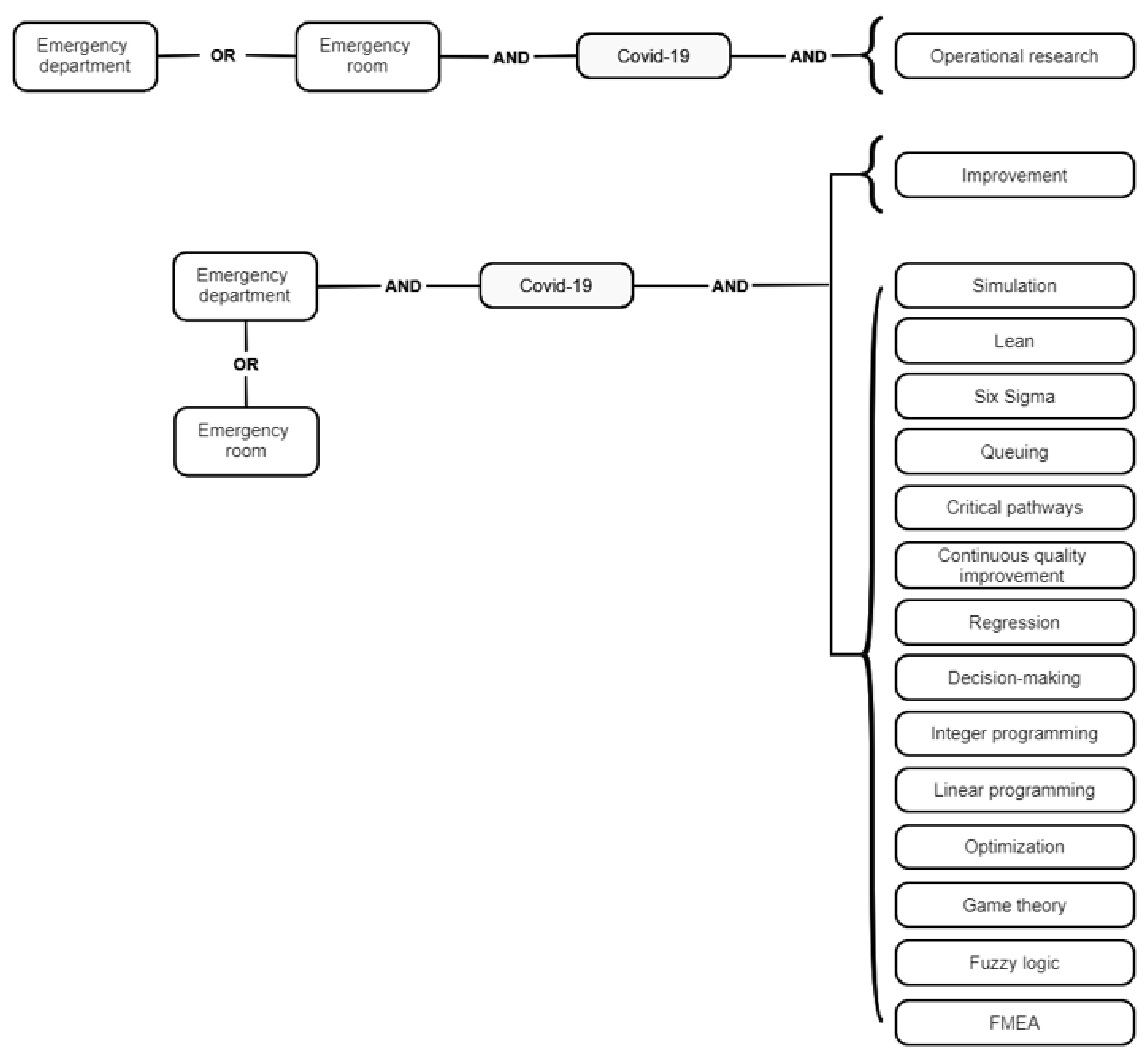
2.1. Search Strategy and Information Sources
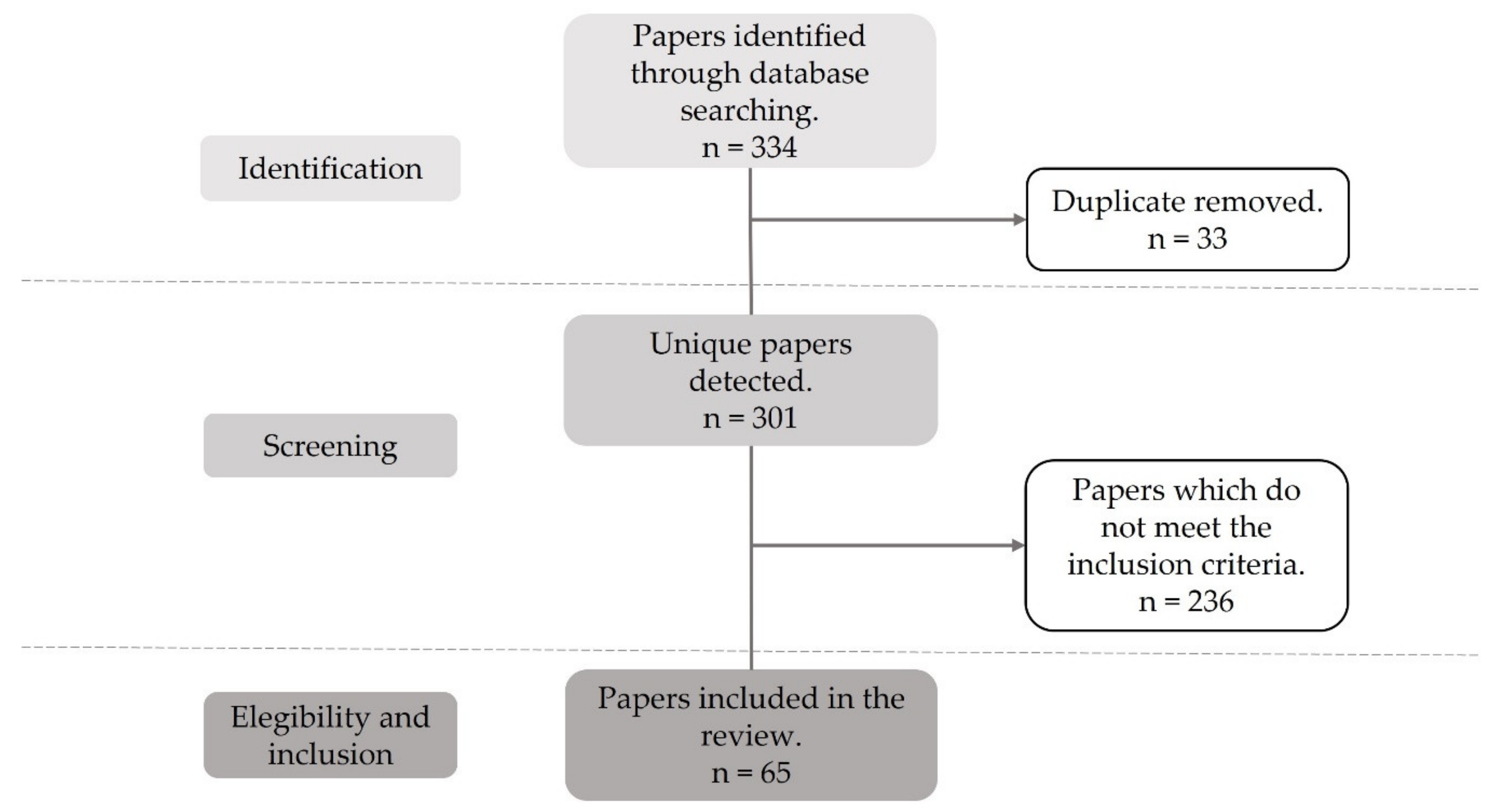
2.2. Selection Process and Data Extraction
2.2.1. Criteria for Including Studies in this Review
Types of Studies
Types of Participants
Types of Interventions
Outcome Measures
- ✓
- Mean length of stay (LOS)
- ✓
- Left-without-being-seen rate (LWBS)
- ✓
- Average flow time
- ✓
- Median time to ED revisit
- ✓
- Median waiting time for consultation
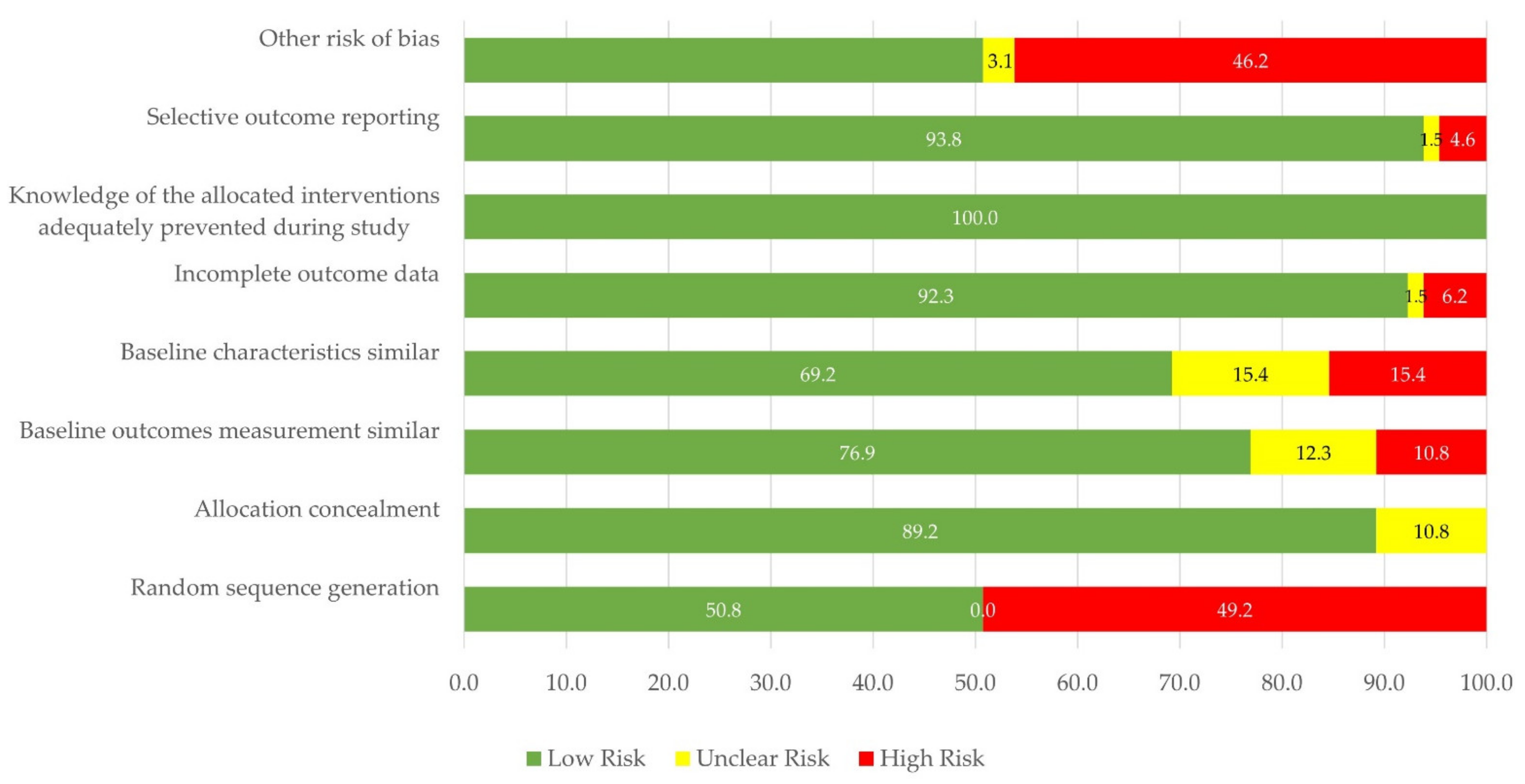
2.3. Risk of Bias Assessment
- ✓
- Low risk: all the factors were graded as “low risk”
- ✓
- Moderate risk: one or two factors were qualified as “unclear risk” or “high risk”
- ✓
- High risk: more than two factors were graded as “unclear risk” or “high risk”
2.4. Effect Measures
- ✓
- Mean length of stay (LOS) (percentage difference; absolute change with 95% confidence interval, inter-quartile range—IQR)
- ✓
- Left-without-being-seen rate (LWBS) (average rate difference)
- ✓
- Average flow time (absolute difference)
- ✓
- Median time to ED revisit (median difference)
- ✓
- Median waiting time for consultation (percentage change)
- ✓
- % of available ventilators (percentage difference)
- ✓
- Number of patients with unfavorable outcomes
- ✓
- Predicted number of COVID-19 patients (percentage difference, absolute change with 95% confidence interval, p-value)
- ✓
- Median time to COVID-19 results (IQR, absolute change with 95% confidence interval)
- ✓
- COVID-19 infection rate within the ED wards (percentage difference)
2.5. Dealing with Missing Data
2.6. Heterogeneity Evaluation
2.7. Data Synthesis, Summary Tables, and Confidence Assessment
3. Results
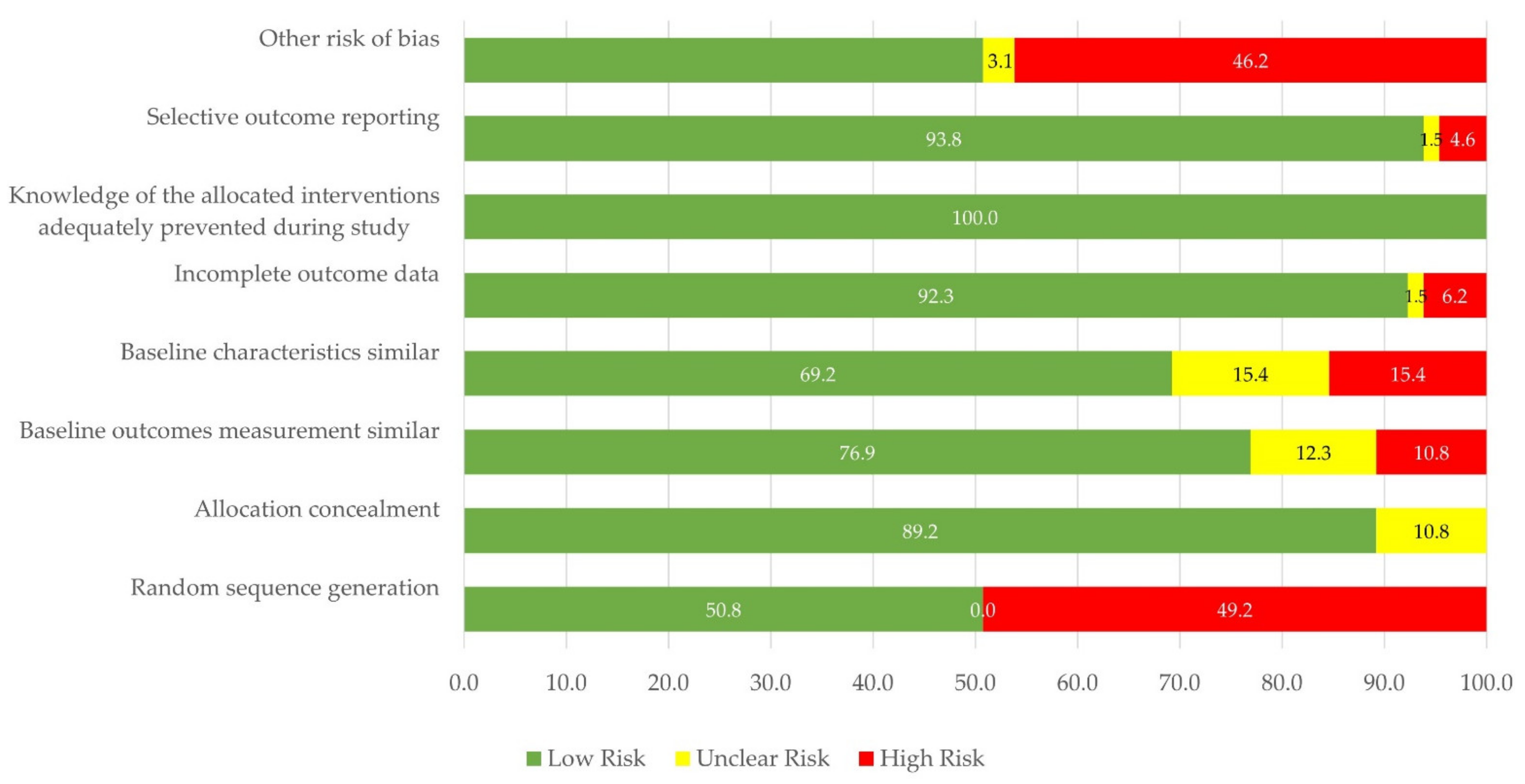
3.1. Study Characteristics, Quality of the Evidence, and Risk of Bias
3.2. Classification Schemes
3.2.1. Classification Based on the Contributing Research Domain
Techniques from the Operational Research Domain
Techniques from the Quality Management Domain
Techniques from the Machine Learning and Data Analytics Domain
Techniques Related to Protocol Design and Implementation
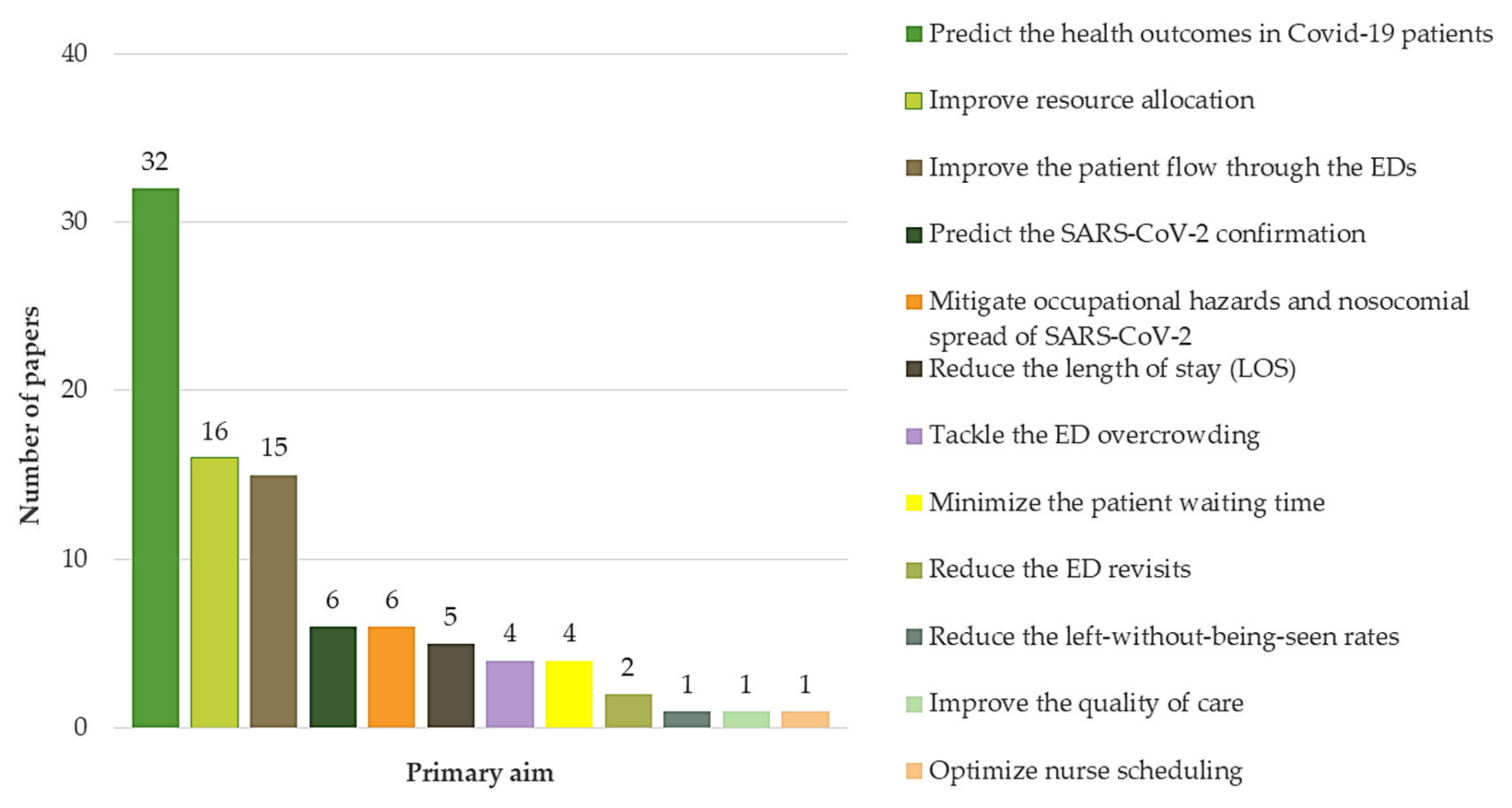
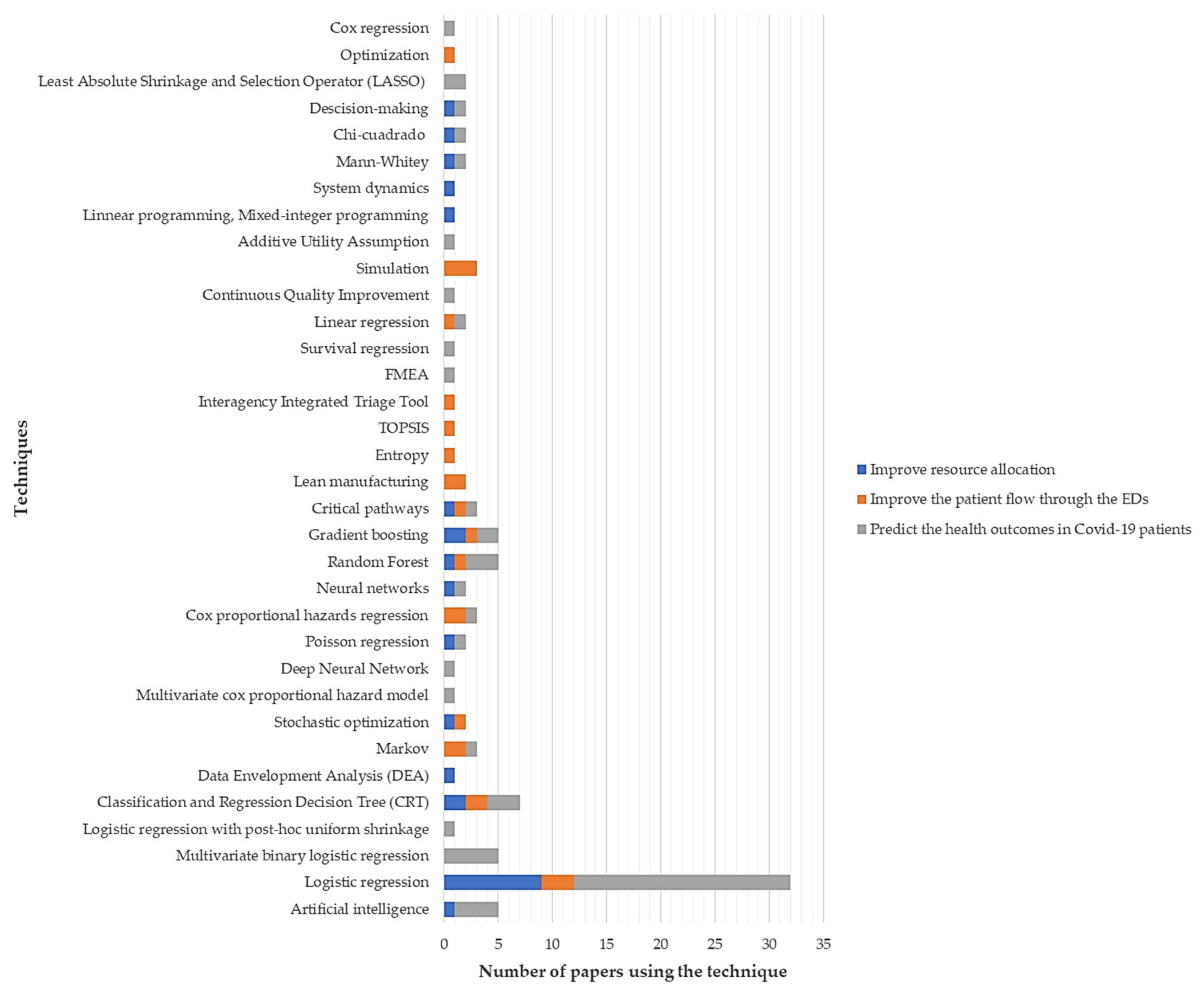
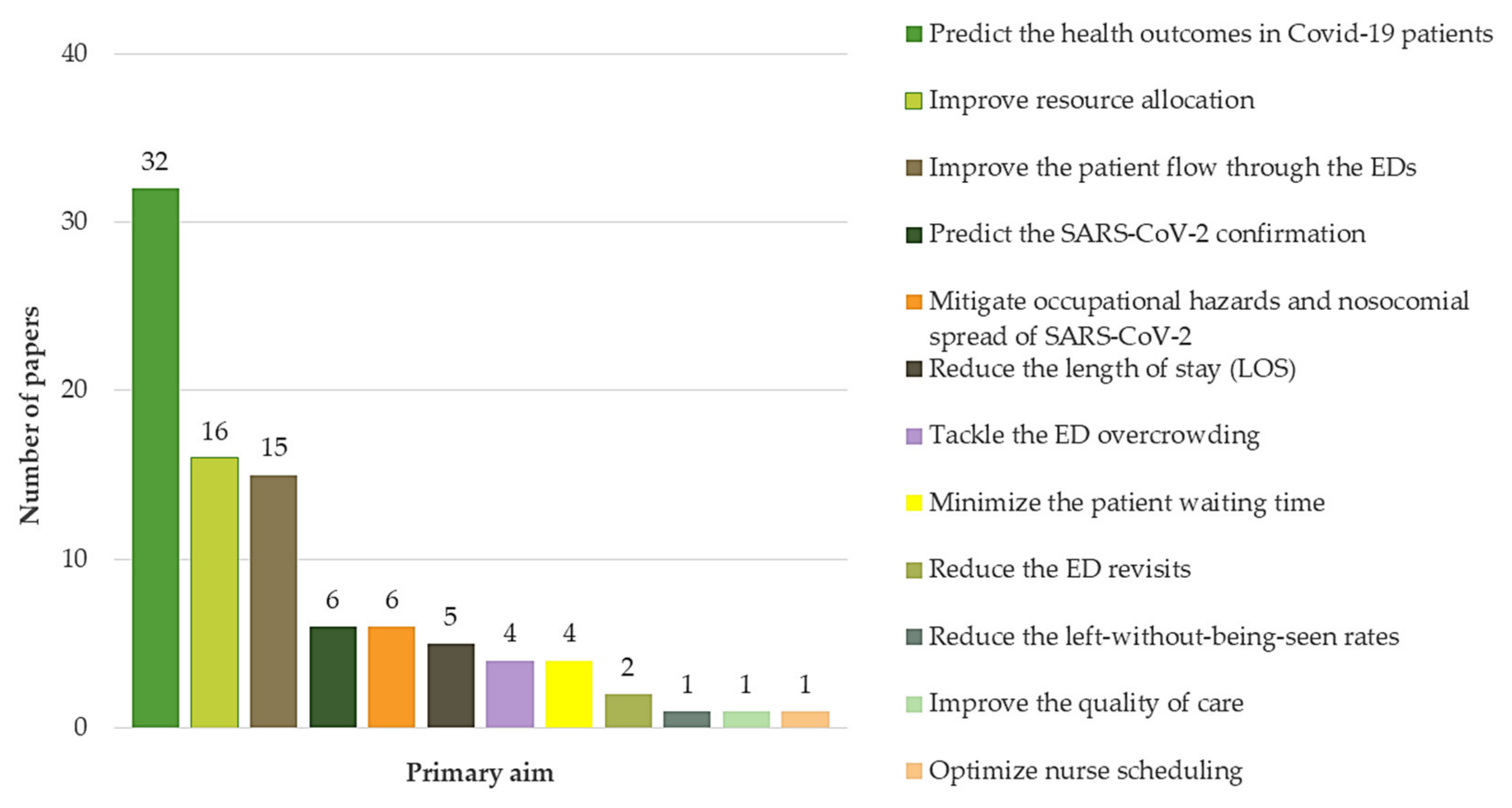
3.2.2. Classification Based on the Primary Aim
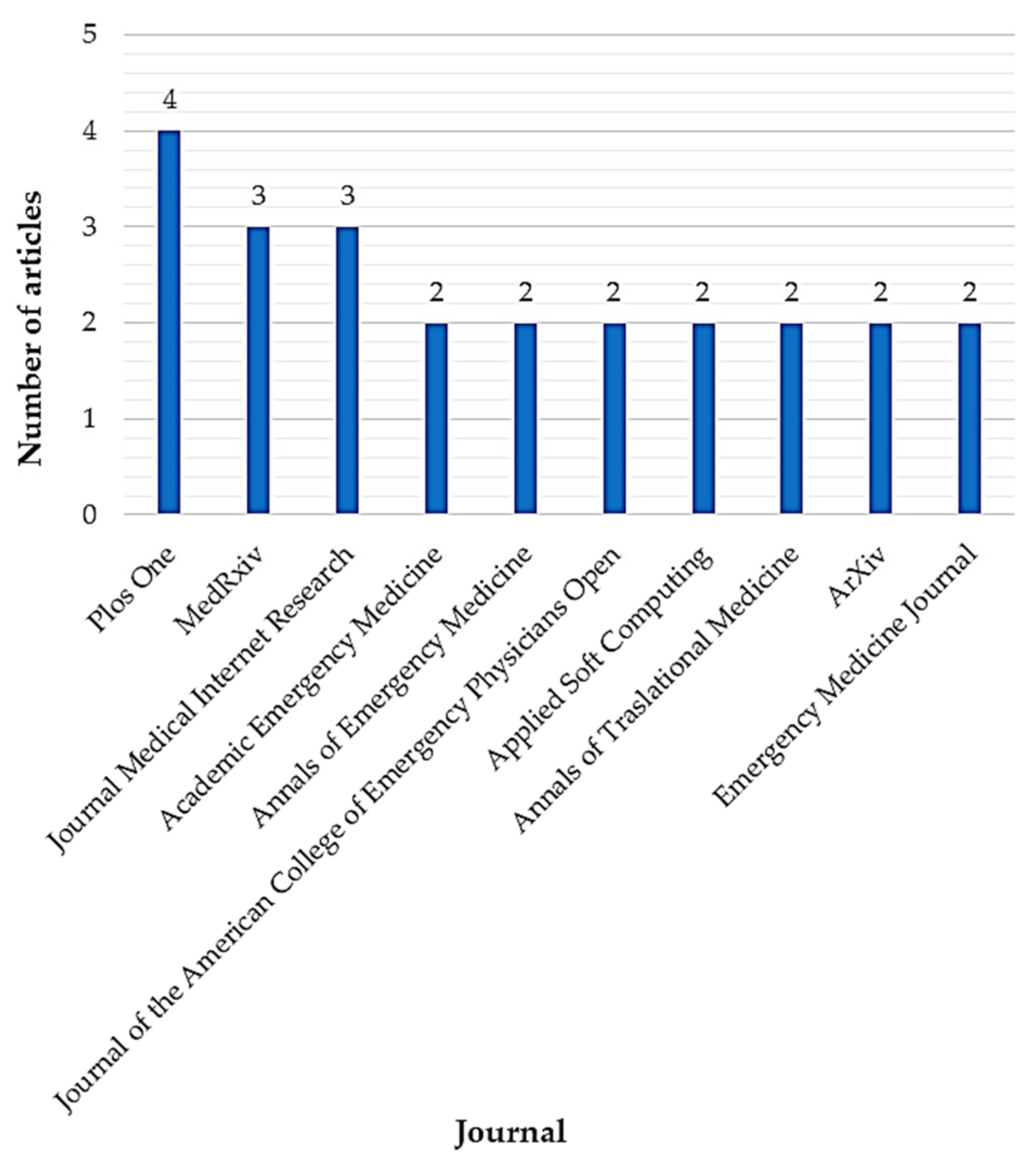
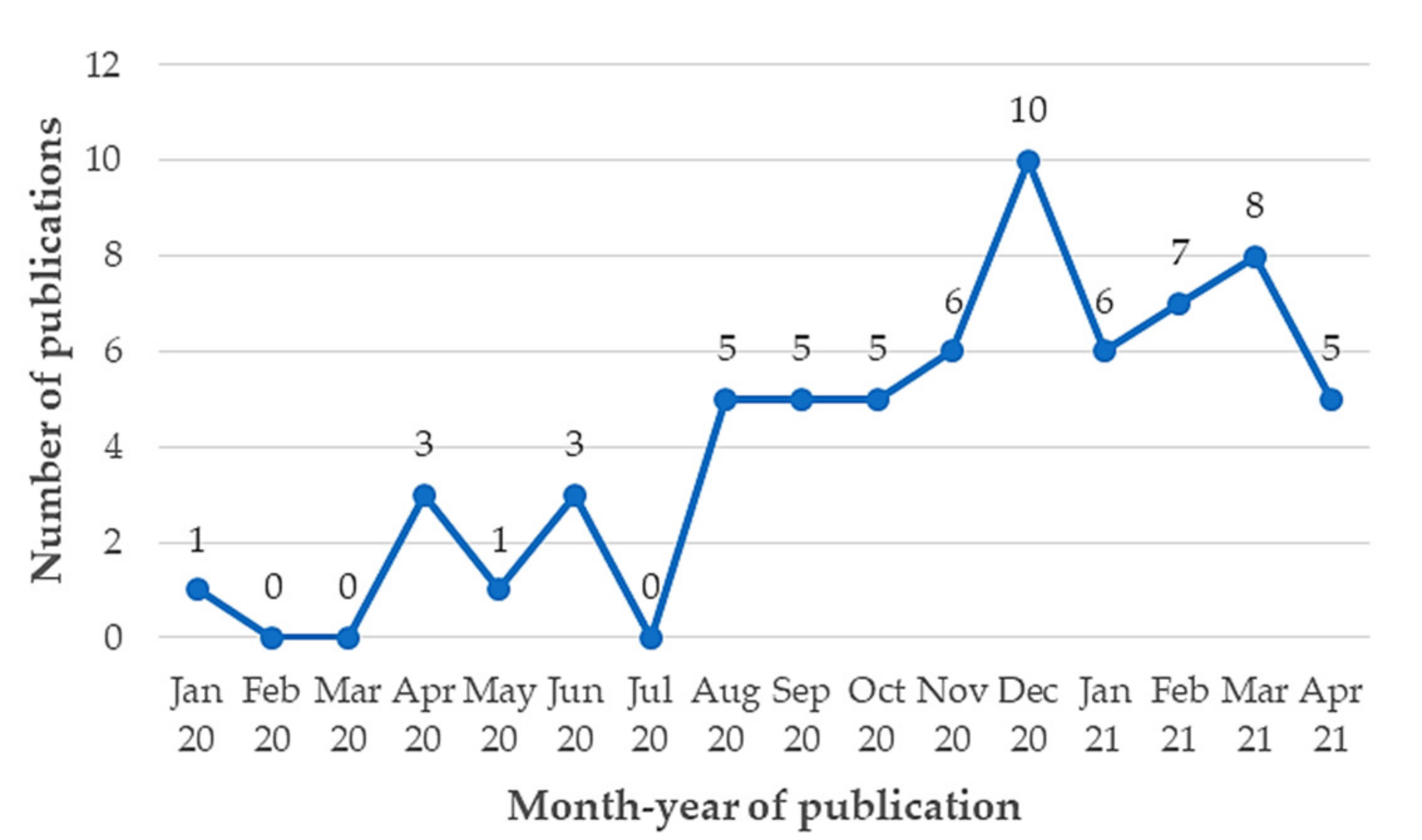
3.2.3. Classification Based on the Publication Period and the Contributing Journal
4. Discussion
5. Concluding Remarks and Future Directions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Anderson, R.M.; Heesterbeek, H.; Klinkenberg, D.; Hollingsworth, T.D. How will country-based mitigation measures influence the course of the COVID-19 epidemic? Lancet 2020, 395, 931–934. [Google Scholar] [CrossRef]
- Sun, X.; Wang, T.; Cai, D.; Hu, Z.; Liao, H.; Zhi, L.; Wei, H.; Zhang, Z.; Qiu, Y.; Wang, J.; et al. Cytokine storm intervention in the early stages of COVID-19 pneumonia. Cytokine Growth Factor Rev. 2020, 53, 38–42. [Google Scholar] [CrossRef]
- Walker, P.G.T.; Whittaker, C.; Watson, O.J.; Baguelin, M.; Winskill, P.; Hamlet, A.; Ghani, A.C. The impact of COVID-19 and strategies for mitigation and suppression in low- and middle-income countries. Science 2020, 369, 413–422. [Google Scholar] [CrossRef]
- World Health Organization. WHO Coronavirus (COVID-19) Dashboard. Available online: https://covid19.who.int/ (accessed on 21 May 2021).
- Singer, D.R. A new pandemic out of China: The Wuhan 2019-nCoV coronavirus syndrome. Health Policy Technol. 2020, 9, 1. [Google Scholar] [CrossRef]
- Ortíz-Barrios, M.A.; Alfaro-Saíz, J.J. Methodological approaches to support process improvement in emergency departments: A systematic review. Int. J. Environ. Res. Public Health 2020, 17, 2664. [Google Scholar] [CrossRef]
- World Health Organization. Coronavirus disease 2019 (COVID-19) Situation Report-93. 2020. Available online: https://www.who.int/docs/default-source/coronaviruse/situation-reports/20200422-sitrep-93-covid-19.pdf?sfvrsn=35cf80d7_4 (accessed on 16 August 2021).
- Mareiniss, D.P. The impending storm: COVID-19, pandemics and our overwhelmed emergency departments. Am. J. Emerg. Med. 2020, 38, 1293–1294. [Google Scholar] [CrossRef]
- Ortiz-Barrios, M.; Lopez-Meza, P.; McClean, S.; Polifroni-Avendaño, G. Discrete-event simulation for performance evaluation and improvement of gynecology outpatient departments: A case study in the public sector. In Lecture Notes in Computer Science; Springer: Cham, Switzerland, 2019; Volume 11582. [Google Scholar] [CrossRef]
- Singh, R.P.; Javaid, M.; Haleem, A.; Suman, R. Internet of things (IoT) applications to fight against COVID-19 pandemic. Diabetes Metab. Syndr. Clin. Res. Rev. 2020, 14, 521–524. [Google Scholar] [CrossRef]
- Hundal, G.S.; Thiyagarajan, S.; Alduraibi, M.; Laux, C.M.; Furterer, S.L.; Cudney, E.A.; Antony, J. Lean Six Sigma as an organizational resilience mechanism in health care during the era of COVID-19. Int. J. Lean Six Sigma 2021, in press. [Google Scholar] [CrossRef]
- Gupta, S.; Starr, M.K.; Farahani, R.Z.; Asgari, N. Pandemics/epidemics: Challenges and opportunities for operations management research. Manuf. Serv. Oper. Manag. 2020, in press. [Google Scholar]
- Munn, Z.; Stern, C.; Aromataris, E.; Lockwood, C.; Jordan, Z. What kind of systematic review should i conduct? A proposed typology and guidance for systematic reviewers in the medical and health sciences. BMC Med Res. Methodol. 2018, 18, 5. [Google Scholar] [CrossRef] [PubMed]
- Elamir, H. Improving patient flow through applying lean concepts to emergency department. Lead. Health Serv. 2018, 31, 293–309. [Google Scholar] [CrossRef]
- Rotteau, L.; Webster, F.; Salkeld, E.; Hellings, C.; Guttmann, A.; Vermeulen, M.J.; Bell, R.S.; Zwarenstein, M.; Rowe, B.H.; Nigam, A.; et al. Ontario’s emergency department process improvement program: The experience of implementation. Acad. Emerg. Med. 2015, 22, 720–729. [Google Scholar] [CrossRef] [PubMed]
- Cheng, I.; Zwarenstein, M.; Kiss, A.; Castren, M.; Brommels, M.; Schull, M. Factors associated with failure of emergency wait-time targets for high acuity discharges and intensive care unit admissions. Can. J. Emerg. Med. 2018, 20, 112–124. [Google Scholar] [CrossRef] [Green Version]
- Ashour, O.M.; Okudan Kremer, G.E. Dynamic patient grouping and prioritization: A new approach to emergency department flow improvement. Health Care Manag. Sci. 2016, 19, 192–205. [Google Scholar] [CrossRef]
- Feng, Y.; Wu, I.; Chen, T. Stochastic resource allocation in emergency departments with a multi-objective simulation optimization algorithm. Health Care Manag. Sci. 2017, 20, 55–75. [Google Scholar] [CrossRef] [PubMed]
- Bellew, S.D.; Collins, S.P.; Barrett, T.W.; Russ, S.E.; Jones, I.D.; Slovis, C.M.; Self, W.H. Implementation of an Opioid Detoxification Management Pathway Reduces Emergency Department Length of Stay. Acad. Emerg. Med. 2018, 25, 1157–1163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yousefi, M.; Ferreira, R.P.M. An agent-based simulation combined with group decision-making technique for improving the performance of an emergency department. Braz. J. Med. Biol. Res. 2017, 50, e5955. [Google Scholar] [CrossRef] [Green Version]
- Nezamoddini, N.; Khasawneh, M.T. Modeling and optimization of resources in multi-emergency department settings with patient transfer. Oper. Res. Health Care 2016, 10, 23–34. [Google Scholar] [CrossRef]
- Bish, P.A.; McCormick, M.A.; Otegbeye, M. Ready-JET-Go: Split Flow Accelerates ED Throughput. J. Emerg. Nurs. 2016, 42, 114–119. [Google Scholar] [CrossRef]
- Blick, K.E. Providing critical laboratory results on time, every time to help reduce emergency department length of stay: How our laboratory achieved a six sigma level of performance. Am. J. Clin. Pathol. 2013, 140, 193–202. [Google Scholar] [CrossRef] [Green Version]
- Azadeh, A.; Rouhollah, F.; Davoudpour, F.; Mohammadfam, I. Fuzzy modelling and simulation of an emergency department for improvement of nursing schedules with noisy and uncertain inputs. Int. J. Serv. Oper. Manag. 2013, 15, 58–77. [Google Scholar] [CrossRef]
- Acuna, J.A.; Zayas-Castro, J.L.; Charkhgard, H. Ambulance allocation optimization model for the overcrowding problem in US emergency departments: A case study in Florida. Socio. Econ. Plan. Sci. 2020, 71, 100747. [Google Scholar] [CrossRef]
- Sorrentino, P. Use of failure mode and effects analysis to improve emergency department handoff processes. Clin. Nurse Spec. 2016, 30, 28–37. [Google Scholar] [CrossRef] [PubMed]
- Saghafian, S.; Austin, G.; Traub, S.J. Operations research/management contributions to emergency department patient flow optimization: Review and research prospects. IIE Trans. Healthc. Syst. Eng. 2015, 5, 101–123. [Google Scholar] [CrossRef]
- Effective Practice and Organisation of Care Group. EPOC Website. Available online: https://epoc.cochrane.org/resources/epoc-resources-review-authors (accessed on 2 August 2021).
- Silal, S.P. Operational research: A multidisciplinary approach for the management of infectious disease in a global context. Eur. J. Oper. Res. 2021, 291, 929–934. [Google Scholar] [CrossRef] [PubMed]
- Gibbs, N.; Kwon, J.; Balen, J.; Dodd, P.J. Operational research to support equitable non-communicable disease policy in low-income and middle-income countries in the sustainable development era: A scoping review. BMJ Glob. Health 2020, 5, e002259. [Google Scholar] [CrossRef] [PubMed]
- Ortiz-Barrios, M.; Alfaro-Saiz, J. A hybrid fuzzy multi-criteria decision-making model to evaluate the overall performance of public emergency departments: A case study. Int. J. Inf. Technol. Decis. Mak. 2020, 19, 1485–1548. [Google Scholar] [CrossRef]
- Mosadeghrad, A.M. Developing and validating a total quality management model for healthcare organisations. TQM J. 2015, 27, 544–564. [Google Scholar] [CrossRef]
- Gambella, C.; Ghaddar, B.; Naoum-Sawaya, J. Optimization Problems for Machine Learning: A Survey. Eur. J. Oper. Res. 2021, 290, 807–828. [Google Scholar] [CrossRef]
- Borges Do Nascimento, I.J.; Marcolino, M.S.; Abdulazeem, H.M.; Weerasekara, I.; Azzopardi-Muscat, N.; Goncalves, M.A.; Novillo-Ortiz, D. Impact of Big Data Analytics on People’s Health: Overview of Systematic Reviews and Recommendations for Future Studies. J. Med Internet Res. 2021, 23, e27275. [Google Scholar] [CrossRef]
- Retzlaff, K.J. COVID-19 Emergency Management Structure and Protocols. AORN J. 2020, 112, 197–203. [Google Scholar] [CrossRef]
- Sangal, R.B.; Scofi, J.E.; Parwani, V.; Pickens, A.T.; Ulrich, A.; Venkatesh, A.K. Less Social Emergency Departments: Implementation of Workplace Contact Reduction during COVID-19. Emerg. Med. J. 2020, 37, 463–466. [Google Scholar] [CrossRef]
- Ballini, L.; Negro, A.; Maltoni, S.; Vignatelli, L.; Flodgren, G.; Simera, I.; Grilli, R. Interventions to reduce waiting times for elective procedures. Cochrane Database Syst. Rev. 2015, CD005610. [Google Scholar] [CrossRef]
- Haidich, A.B. Meta-analysis in medical research. Hippokratia 2010, 14, 29. [Google Scholar] [PubMed]
- Abadi, M.Q.H.; Rahmati, S.; Sharifi, A.; Ahmadi, M. HSSAGA: Designation and Scheduling of Nurses for Taking Care of COVID-19 Patients Using Novel Method of Hybrid Salp Swarm Algorithm and Genetic Algorithm. Appl. Soft Comput. 2021, 108, 107449. [Google Scholar] [CrossRef] [PubMed]
- AbdelAziz, A.M.; Alarabi, L.; Basalamah, S.; Hendawi, A. A Multi-Objective Optimization Method for Hospital Admission Problem—A Case Study on Covid-19 Patients. Algorithms 2021, 14, 38. [Google Scholar] [CrossRef]
- Aggarwal, L.; Goswami, P.; Sachdeva, S. Multi-Criterion Intelligent Decision Support System for COVID-19. Appl. Soft Comput. 2021, 101, 107056. [Google Scholar] [CrossRef]
- Albahri, A.S.; Hamid, R.A.; Albahri, O.S.; Zaidan, A.A. Detection-Based Prioritisation: Framework of Multi-Laboratory Characteristics for Asymptomatic COVID-19 Carriers Based on Integrated Entropy–TOPSIS Methods. Artif. Intell. Med. 2021, 111, 101983. [Google Scholar] [CrossRef]
- Alfaro-Martínez, J.J.; Calbo Mayo, J.; Molina Cifuentes, M.; Abizanda Soler, P.; Guillén Martínez, S.; Rodríguez Marín, Y.; Sirvent Segovia, A.E.; Nuñez Ares, A.; Alcaraz Barcelona, M.; Paterna Mellinas, G.; et al. Generation and Validation of In-Hospital Mortality Prediction Score in COVID-19 Patients: Alba-Score. Curr. Med Res. Opin. 2021, 37, 719–726. [Google Scholar] [CrossRef]
- Angeli, E.; Dalto, S.; Marchese, S.; Setti, L.; Bonacina, M.; Galli, F.; Rulli, E.; Torri, V.; Monti, C.; Meroni, R.; et al. Prognostic Value of CT Integrated with Clinical and Laboratory Data during the First Peak of the COVID-19 Pandemic in Northern Italy: A Nomogram to Predict Unfavorable Outcome. Eur. J. Radiol. 2021, 137, 109612. [Google Scholar] [CrossRef]
- Araz, O.M.; Ramirez-Nafarrate, A.; Jehn, M.; Wilson, F.A. The Importance of Widespread Testing for COVID-19 Pandemic: Systems Thinking for Drive-through Testing Sites. Health Syst. 2020, 9, 119–123. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Assaf, D.; Gutman, Y.; Neuman, Y.; Segal, G.; Amit, S.; Gefen-Halevi, S.; Shilo, N.; Epstein, A.; Mor-Cohen, R.; Biber, A.; et al. Utilization of Machine-Learning Models to Accurately Predict the Risk for Critical COVID-19. Intern. Emerg. Med. 2020, 15, 1435–1443. [Google Scholar] [CrossRef]
- Balbi, M.; Caroli, A.; Corsi, A.; Milanese, G.; Surace, A.; Di Marco, F.; Novelli, L.; Silva, M.; Lorini, F.L.; Duca, A.; et al. Chest X-Ray for Predicting Mortality and the Need for Ventilatory Support in COVID-19 Patients Presenting to the Emergency Department. Eur. Radiol. 2020, 31, 1999–2012. [Google Scholar] [CrossRef] [PubMed]
- Balmaks, R.; Grāmatniece, A.; Vilde, A.; Ļuļļa, M.; Dumpis, U.; Gross, I.; Šlēziņa, I. A Simulation-Based Failure Mode Analysis of SARS-CoV-2 Infection Control and Prevention in Emergency Departments. Simul. Healthc. 2020, in press. [Google Scholar] [CrossRef] [PubMed]
- Brendish, N.J.; Poole, S.; Naidu, V.V.; Mansbridge, C.T.; Norton, N.J.; Wheeler, H.; Presland, L.; Kidd, S.; Cortes, N.J.; Borca, F.; et al. Clinical Impact of Molecular Point-of-Care Testing for Suspected COVID-19 in Hospital (COV-19POC): A Prospective, Interventional, Non-Randomised, Controlled Study. Lancet Respir. Med. 2020, 8, 1192–1200. [Google Scholar] [CrossRef]
- Bolourani, S.; Brenner, M.; Wang, P.; McGinn, T.; Hirsch, J.S.; Barnaby, D.; Zanos, T.P.; Barish, M.; Cohen, S.L.; Coppa, K.; et al. A Machine Learning Prediction Model of Respiratory Failure within 48 Hours of Patient Admission for COVID-19: Model Development and Validation. J. Med Internet Res. 2021, 23, e24246. [Google Scholar] [CrossRef] [PubMed]
- Carlile, M.; Hurt, B.; Hsiao, A.; Hogarth, M.; Longhurst, C.A.; Dameff, C. Deployment of Artificial Intelligence for Radiographic Diagnosis of COVID-19 Pneumonia in the Emergency Department. J. Am. Coll. Emerg. Physicians Open 2020, 1, 1459–1464. [Google Scholar] [CrossRef]
- Casiraghi, E.; Malchiodi, D.; Trucco, G.; Frasca, M.; Cappelletti, L.; Fontana, T.; Esposito, A.A.; Avola, E.; Jachetti, A.; Reese, J.; et al. Explainable Machine Learning for Early Assessment of COVID-19 Risk Prediction in Emergency Departments. IEEE Access 2020, 8, 196299–196325. [Google Scholar] [CrossRef]
- Chen, T.; Ma, X.; Zhou, S.; Wang, H.; Pan, Y.; Chen, L.; Lv, H.; Lu, Y. Establishing a Standardized FUO Emergency Department: Design and Practice in Dealing with COVID-19. Ann. Transl. Med. 2020, 8, 749. [Google Scholar] [CrossRef]
- Chopra, Z.; Holmes, A.R.; Nelson, J.R.; Hirschl, J.R.; Perkins, S.J.; Fung, C.; Medlin, R.P.; Korley, F.K. 63 Incidence and Determinants of COVID-19 Emergency Department Revisits. Ann. Emerg. Med. 2020, 76, S25. [Google Scholar] [CrossRef]
- Chou, E.H.; Wang, C.H.; Hsieh, Y.L.; Namazi, B.; Wolfshohl, J.; Bhakta, T.; Tsai, C.L.; Lien, W.C.; Sankaranarayanan, G.; Lee, C.C.; et al. Clinical Features of Emergency Department Patients from Early COVID-19 Pandemic That Predict SARS-CoV-2 Infection: Machine-Learning Approach. Western J. Emerg. Med. 2021, 22, 244–251. [Google Scholar] [CrossRef] [PubMed]
- Diep, A.N.; Gilbert, A.; Saegerman, C.; Gangolf, M.; D’Orio, V.; Ghuysen, A.; Donneau, A.-F. Development and Validation of a Predictive Model to Determine the Level of Care in Patients Confirmed with COVID-19. Infect. Dis. 2021, 53, 590–599. [Google Scholar] [CrossRef] [PubMed]
- De Moraes, A.F.; Miraglia, J.L.; Rizzi-Donato, T.H.; Porto-Chiavegatto-Filho, A. COVID-19 diagnosis prediction in emergency care patients: A machine learning approach. medRxiv 2020, 20052092. [Google Scholar] [CrossRef] [Green Version]
- De Nardo, P.; Gentilotti, E.; Mazzaferri, F.; Cremonini, E.; Hansen, P.; Goossens, H.; Tacconelli, E. Multi-Criteria Decision Analysis to Prioritize Hospital Admission of Patients Affected by COVID-19 in Low-Resource Settings with Hospital-Bed Shortage. Int. J. Infect. Dis. 2020, 98, 494–500. [Google Scholar] [CrossRef] [PubMed]
- Esposito, A.; Palmisano, A.; Cao, R.; Rancoita, P.; Landoni, G.; Grippaldi, D.; Boccia, E.; Cosenza, M.; Messina, A.; la Marca, S.; et al. Quantitative Assessment of Lung Involvement on Chest CT at Admission: Impact on Hypoxia and Outcome in COVID-19 Patients. Clin. Imaging 2021, 77, 194–201. [Google Scholar] [CrossRef]
- Feng, C.; Wang, L.; Chen, X.; Zhai, Y.; Zhu, F.; Chen, H.; Wang, Y.; Su, X.; Huang, S.; Tian, L.; et al. A Novel Artificial Intelligence-Assisted Triage Tool to Aid in the Diagnosis of Suspected COVID-19 Pneumonia Cases in Fever Clinics. Ann. Transl. Med. 2021, 9, 201. [Google Scholar] [CrossRef]
- Freund, Y.; Drogrey, M.; Miró, Ò.; Marra, A.; Féral-Pierssens, A.L.; Penaloza, A.; Hernandez, B.A.L.; Beaune, S.; Gorlicki, J.; Vaittinada Ayar, P.; et al. Association Between Pulmonary Embolism and COVID-19 in Emergency Department Patients Undergoing Computed Tomography Pulmonary Angiogram: The PEPCOV International Retrospective Study. Acad. Emerg. Med. 2020, 27, 811–820. [Google Scholar] [CrossRef]
- Garbey, M.; Joerger, G.; Furr, S.; Fikfak, V. A Model of Workflow in the Hospital during a Pandemic to Assist Management. PLoS ONE 2020, 15, e0242183. [Google Scholar] [CrossRef]
- García de Guadiana-Romualdo, L.; Calvo Nieves, M.D.; Rodríguez Mulero, M.D.; Calcerrada Alises, I.; Hernández Olivo, M.; Trapiello Fernández, W.; González Morales, M.; Bolado Jiménez, C.; Albaladejo-Otón, M.D.; Fernández Ovalle, H.; et al. MR-ProADM as Marker of Endotheliitis Predicts COVID-19 Severity. European. J. Clin. Investig. 2021, 51, e13511. [Google Scholar] [CrossRef]
- Gavelli, F.; Castello, L.M.; Bellan, M.; Azzolina, D.; Hayden, E.; Beltrame, M.; Galbiati, A.; Gardino, C.A.; Gastaldello, M.L.; Giolitti, F.; et al. Clinical Stability and In-Hospital Mortality Prediction in COVID-19 Patients Presenting to the Emergency Department. Minerva Med. 2020, 112, 118–123. [Google Scholar] [CrossRef]
- Goodacre, S.; Thomas, B.; Sutton, L.; Burnsall, M.; Lee, E.; Bradburn, M.; Loban, A.; Waterhouse, S.; Simmonds, R.; Biggs, K.; et al. Derivation and Validation of a Clinical Severity Score for Acutely Ill Adults with Suspected COVID-19: The PRIEST Observational Cohort Study. PLoS ONE 2021, 16, e0245840. [Google Scholar] [CrossRef] [PubMed]
- Gordon, W.J.; Henderson, D.; Desharone, A.; Fisher, H.N.; Judge, J.; Levine, D.M.; MacLean, L.; Sousa, D.; Su, M.Y.; Boxer, R. Remote Patient Monitoring Program for Hospital Discharged COVID-19 Patients. Appl. Clin. Inform. 2020, 11, 792–801. [Google Scholar] [CrossRef]
- Haddad, Y.; Salonitis, K.; Emmanouilidis, C. Design of Emergency Response Manufacturing Networks: A Decision-Making Framework. Procedia CIRP 2020, 96, 151–156. [Google Scholar] [CrossRef]
- Heldt, F.S.; Vizcaychipi, M.P.; Peacock, S.; Cinelli, M.; McLachlan, L.; Andreotti, F.; Jovanović, S.; Dürichen, R.; Lipunova, N.; Fletcher, R.A.; et al. Early Risk Assessment for COVID-19 Patients from Emergency Department Data Using Machine Learning. Sci. Rep. 2021, 11, 4200. [Google Scholar] [CrossRef]
- Joshi, R.P.; Pejaver, V.; Hammarlund, N.E.; Sung, H.; Lee, S.K.; Furmanchuk, A.; Lee, H.Y.; Scott, G.; Gombar, S.; Shah, N.; et al. A Predictive Tool for Identification of SARS-CoV-2 PCR-Negative Emergency Department Patients Using Routine Test Results. J. Clin. Virol. 2020, 129, 104502. [Google Scholar] [CrossRef] [PubMed]
- Kim, C.; Yeo, I.H.; Kim, J.K.; Cho, Y.; Lee, M.J.; Jung, H.; Cho, J.W.; Ham, J.Y.; Lee, S.H.; Chung, H.S.; et al. Confirmation of COVID-19 in Out-of-Hospital Cardiac Arrest Patients and Postmortem Management in the Emergency Department during the COVID-19 Outbreak. Infect. Chemother. 2020, 52, 572. [Google Scholar] [CrossRef]
- Kirby, J.J.; Shaikh, S.; Bryant, D.P.; Ho, A.F.; d’Etienne, J.P.; Schrader, C.D.; Wang, H. A Simplified Comorbidity Evaluation Predicting Clinical Outcomes Among Patients with Coronavirus Disease 2019. J. Clin. Med. Res. 2021, 13, 237–244. [Google Scholar] [CrossRef]
- Kline, J.A.; Camargo, C.A.; Courtney, D.M.; Kabrhel, C.; Nordenholz, K.E.; Aufderheide, T.; Baugh, J.J.; Beiser, D.G.; Bennett, C.L.; Bledsoe, J.; et al. Clinical Prediction Rule for SARS-CoV-2 Infection from 116 U.S. Emergency Departments. PLoS ONE 2021, 16, e0248438. [Google Scholar] [CrossRef]
- Lancet, E.A.; Gonzalez, D.; Alexandrou, N.A.; Zabar, B.; Lai, P.H.; Hall, C.B.; Braun, J.; Zeig-Owens, R.; Isaacs, D.; Ben-Eli, D.; et al. Prehospital Hypoxemia, Measured by Pulse Oximetry, Predicts Hospital Outcomes during the New York City COVID-19 Pandemic. J. Am. Coll. Emerg. Physicians 2021, 2, e12407. [Google Scholar] [CrossRef]
- Levine, D.M.; Lipsitz, S.R.; Co, Z.; Song, W.; Dykes, P.C.; Samal, L. Derivation of a Clinical Risk Score to Predict 14-Day Occurrence of Hypoxia, ICU Admission, and Death Among Patients with Coronavirus Disease 2019. J. Gen. Intern. Med. 2020, 36, 730–737. [Google Scholar] [CrossRef] [PubMed]
- Liu, P.Y.; Tsai, Y.S.; Chen, P.L.; Tsai, H.P.; Hsu, L.W.; Wang, C.S.; Lee, N.Y.; Huang, M.S.; Wu, Y.C.; Ko, W.C.; et al. Application of an Artificial Intelligence Trilogy to Accelerate Processing of Suspected Patients with SARS-CoV-2 at a Smart Quarantine Station: Observational Study. J. Med Internet Res. 2020, 22, e19878. [Google Scholar] [CrossRef] [PubMed]
- McDonald, S.A.; Medford, R.J.; Basit, M.A.; Diercks, D.B.; Courtney, D.M. Derivation with Internal Validation of a Multivariable Predictive Model to Predict COVID-19 Test Results in Emergency Department Patients. Acad. Emerg. Med. 2021, 28, 206–214. [Google Scholar] [CrossRef] [PubMed]
- Mehrotra, S.; Rahimian, H.; Barah, M.; Luo, F.; Schantz, K. A Model of Supply-chain Decisions for Resource Sharing with an Application to Ventilator Allocation to Combat COVID-19. Nav. Res. Logist. (NRL) 2020, 67, 303–320. [Google Scholar] [CrossRef]
- Mitchell, R.; McKup, J.J.; Bue, O.; Nou, G.; Taumomoa, J.; Banks, C.; O’Reilly, G.; Kandelyo, S.; Bornstein, S.; Cole, T.; et al. Implementation of a Novel Three-Tier Triage Tool in Papua New Guinea: A Model for Resource-Limited Emergency Departments. Lancet Reg. Health West. Pac. 2020, 5, 100051. [Google Scholar] [CrossRef]
- Möckel, M.; Stegemann, M.; Burst, V.; Kümpers, P.; Risse, J.; Koehler, F.; Schunk, D.; Hitzek, J.; Dietrich, T.; Slagman, A. Which parameters support disposition decision in suspected COVID-19 cases in the emergency department (ED): A German clinical cohort study. BMJ Open 2021, 11, 044853. [Google Scholar] [CrossRef]
- Moss, R.; Wood, J.; Brow, D.; Shearer, F.; Black, A.J.; Cheng, A.C.; McCare, J.M.; McVernon, J. Modelling the impact of COVID-19 in Australia to inform transmission reducing measures and health system preparedness. medRxiv 2020, 20056184. [Google Scholar] [CrossRef] [Green Version]
- Nepomuceno, T.C.C.; Silva, W.M.N.; Nepomuceno, K.T.C.; Barros, I.K.F. A DEA-Based Complexity of Needs Approach for Hospital Beds Evacuation during the COVID-19 Outbreak. J. Healthc. Eng. 2020, 2020, 8857553. [Google Scholar] [CrossRef]
- Nguyen, Y.; Corre, F.; Honsel, V.; Curac, S.; Zarrouk, V.; Burtz, C.P.; Weiss, E.; Moyer, J.D.; Gauss, T.; Grégory, J.; et al. A Nomogram to Predict the Risk of Unfavourable Outcome in COVID-19: A Retrospective Cohort of 279 Hospitalized Patients in Paris Area. Ann. Med. 2020, 52, 367–375. [Google Scholar] [CrossRef] [PubMed]
- O′Reilly, G.M.; Mitchell, R.D.; Noonan, M.P.; Hiller, R.; Mitra, B.; Brichko, L.; Luckhoff, C.; Paton, A.; Smit, D.V.; Santamaria, M.J.; et al. Informing Emergency Care for COVID-19 Patients: The COVID-19 Emergency Department Quality Improvement Project Protocol. EMA Emerg. Med. Australas. 2020, 32, 511–514. [Google Scholar] [CrossRef] [Green Version]
- Parker, F.; Sawczuk, H.; Ganjkhanloo, F.; Ahmadi, F.; Ghobadi, K. Optimal Resource and Demand Redistribution for Healthcare Systems Under Stress from COVID-19. arXiv 2020, arXiv:2011.03528. [Google Scholar]
- Peng, Q.; Yang, J.; Strome, T.; Weldon, E.; Chochinov, A. Bottleneck Detection and Reduction Using Simulation Modeling to Reduce Overcrowding of Hospital Emergency Department. J. Modeling Optim. 2020, 12, 100–109. [Google Scholar] [CrossRef]
- Plante, T.B.; Blau, A.M.; Berg, A.N.; Weinberg, A.S.; Jun, I.C.; Tapson, V.F.; Kanigan, T.S.; Adib, A.B. Development and External Validation of a Machine Learning Tool to Rule out COVID-19 among Adults in the Emergency Department Using Routine Blood Tests: A Large, Multicenter, Real-World Study. J. Med Internet Res. 2020, 22, e24048. [Google Scholar] [CrossRef] [PubMed]
- Romero-Gameros, C.A.; Colin-Martínez, T.; Waizel-Haiat, S.; Vargas-Ortega, G.; Ferat-Osorio, E.; Guerrero-Paz, J.A.; Intriago-Alor, M.; López-Moreno, M.A.; Cuevas-García, C.F.; Mendoza-Zubieta, V.; et al. Diagnostic Accuracy of Symptoms as a Diagnostic Tool for SARS-CoV 2 Infection: A Cross-Sectional Study in a Cohort of 2173 Patients. BMC Infect. Dis. 2021, 21, 255. [Google Scholar] [CrossRef]
- Saegerman, C.; Gilbert, A.; Donneau, A.-F.; Gangolf, M.; Diep, A.N.; Meex, C.; Bontems, S.; Hayette, M.-P.; D′Orio, V.; Ghuysen, A. Clinical Decision Support Tool for Diagnosis of COVID-19 in Hospitals. PLoS ONE 2021, 16, e0247773. [Google Scholar] [CrossRef]
- Shamout, F.E.; Shen, Y.; Wu, N.; Kaku, A.; Park, J.; Makino, T.; Jastrzębski, S.; Witowski, J.; Wang, D.; Zhang, B.; et al. An Artificial Intelligence System for Predicting the Deterioration of COVID-19 Patients in the Emergency Department. arXiv 2020, arXiv:2008.01774. [Google Scholar]
- Sherren, P.B.; Camporota, L.; Sanderson, B.; Jones, A.; Shankar-Hari, M.; Meadows, C.I.; Barrett, N.; Ostermann, M.; Hart, N. Outcomes of Critically Ill COVID-19 Patients Managed in a High-Volume Severe Respiratory Failure and ECMO Centre in the United Kingdom. J. Intensive Care Soc. 2020, 175114372097885. [Google Scholar] [CrossRef]
- Suh, E.H.; Bodnar, D.J.; Melville, L.D.; Sharma, M.; Farmer, B.M. Crisis Clinical Pathway for COVID-19. Emerg. Med. J. 2020, 37, 700–704. [Google Scholar] [CrossRef] [PubMed]
- Sung, J.; Choudry, N.; Bachour, R. Development and Validation of a Simple Risk Score for Diagnosing Covid-19 in the Emergency Room. Epidemiol. Infect. 2020, 148, e273. [Google Scholar] [CrossRef]
- Tang, S.; McDonald, S.; Furmaga, J.; Piel, C.; Courtney, M.; Diercks, D.; Rojas Cordova, A. 185 Data-Driven Staffing Decision-Making at an Emergency Department in Response to COVID-19. Ann. Emerg. Med. 2020, 76, S71–S72. [Google Scholar] [CrossRef]
- Teklewold, B.; Anteneh, D.; Kebede, D.; Gezahegn, W. Use of Failure Mode and Effect Analysis to Reduce Admission of Asymptomatic COVID-19 Patients to the Adult Emergency Department: An Institutional Experience. Risk Manag. Healthc. Policy 2021, 14, 273–282. [Google Scholar] [CrossRef] [PubMed]
- Van Klaveren, D.; Rekkas, A.; Alsma, J.; Verdonschot, R.J.; Koning, D.T.; Kamps, M.J.; Dormans, T.; Stassen, R.; Weijer, S.; Arnold, K.-S.; et al. COVID Outcome Prediction in the Emergency Department (COPE): Development and Validation of a Model for Predicting Death and Need for Intensive Care in COVID-19 Patients. medRxiv 2021, 20249023. [Google Scholar] [CrossRef]
- Van Singer, M.; Brahier, T.; Ngai, M.; Wright, J.; Weckman, A.M.; Erice, C.; Meuwly, J.Y.; Hugli, O.; Kain, K.C.; Boillat-Blanco, N. COVID-19 Risk Stratification Algorithms Based on STREM-1 and IL-6 in Emergency Department. J. Allergy Clin. Immunol. 2021, 147, 99–106.e4. [Google Scholar] [CrossRef] [PubMed]
- Wang, A.Z.; Ehrman, R.; Bucca, A.; Croft, A.; Glober, N.; Holt, D.; Lardaro, T.; Musey, P.; Peterson, K.; Schaffer, J.; et al. Can We Predict Which COVID-19 Patients Will Need Transfer to Intensive Care within 24 Hours of Floor Admission? Acad. Emerg. Med 2021, 28, 511–518. [Google Scholar] [CrossRef] [PubMed]
- Zeinalnezhad, M.; Chofreh, A.G.; Goni, F.A.; Klemeš, J.J.; Sari, E. Simulation and Improvement of Patients’ Workflow in Heart Clinics during COVID-19 Pandemic Using Timed Coloured Petri Nets. Int. J. Environ. Res. Public Health 2020, 17, 8577. [Google Scholar] [CrossRef] [PubMed]
- Zhang, W.; Zhang, C.; Bi, Y.; Yuan, L.; Jiang, Y.; Hasi, C.; Zhang, X.; Kong, X. Analysis of COVID-19 Epidemic and Clinical Risk Factors of Patients under Epidemiological Markov Model. Results Phys. 2021, 22, 103881. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Cheng, S.R. Evaluating the Need for Routine COVID-19 Testing of Emergency Department Staff: Quantitative Analysis. JMIR Public Health Surveill. 2020, 6, e20260. [Google Scholar] [CrossRef]
- Zhou, W.; Liu, Y.; Xu, B.; Wang, S.; Li, S.; Liu, H.; Huang, Z.; Luo, Y.; Hu, M.; Wu, W.; et al. Early Identification of Patients with Severe COVID-19 at Increased Risk of in-Hospital Death: A Multicenter Case-Control Study in Wuhan. J. Thorac. Dis. 2021, 13, 1380–1395. [Google Scholar] [CrossRef]
- Medford-Davis, L.; Marcozzi, D.; Agrawal, S.; Carr, B.G.; Carrier, E. Value-based approaches for emergency care in a new era. Ann. Emerg. Med. 2017, 69, 675–683. [Google Scholar] [CrossRef]
- Rocha, T.A.H.; da Silva, N.C.; Amaral, P.V.; Barbosa, A.C.Q.; Rocha, J.V.M.; Alvares, V.; Facchini, L.A. Access to emergency care services: A transversal ecological study about brazilian emergency health care network. Public Health 2017, 153, 9–15. [Google Scholar] [CrossRef]
- Ortiz-Barrios, M.; Alfaro-Saiz, J.J. An integrated approach for designing in-time and economically sustainable emergency care networks: A case study in the public sector. PLoS ONE 2020, 15, e0234984. [Google Scholar] [CrossRef]
- Lemos, D.R.Q.; D’angelo, S.M.; Farias, L.A.B.G.; Almeida, M.M.; Gomes, R.G.; Pinto, G.P.; Cavalcanti, L.P.G. Health system collapse 45 days after the detection of COVID-19 in ceará, northeast brazil: A preliminary analysis. Rev. Soc. Bras. Med. Trop. 2020, 53, 1–6. [Google Scholar] [CrossRef]
- Thornton, J. Covid-19: A&E visits in england fall by 25% in week after lockdown. BMJ (Clin. Res. Ed.) 2020, 369, m1401. [Google Scholar] [CrossRef] [Green Version]
- Perry, R.; Banaras, A.; Werring, D.J.; Simister, R. What has caused the fall in stroke admissions during the COVID-19 pandemic? J. Neurol. 2020, 267, 3457–3458. [Google Scholar] [CrossRef] [PubMed]
- Hartnett, K.P.; Kite-Powell, A.; DeVies, J.; Coletta, M.A.; Boehmer, T.K.; Adjemian, J.; Gundlapalli, A.V. National Syndromic Surveillance Program Community of Practice. Impact of the COVID-19 Pandemic on Emergency Department Visits—United States, January1, 2019–May 30, 2020. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 699–704. [Google Scholar] [CrossRef]
- Pashazadeh, A.; Navimipour, N.J. Big data handling mechanisms in the healthcare applications: A comprehensive and systematic literature review. J. Biomed. Inform. 2018, 82, 47–62. [Google Scholar] [CrossRef] [PubMed]
- Romero-Conrado, A.R.; Castro-Bolaño, L.J.; Montoya-Torres, J.R.; Jiménez-Barros, M.Á. Operations research as a decision-making tool in the health sector: A state of the art. [La utilización de la investigación de operaciones como soporte a la toma de decisiones en el sector salud: Un estado del arte]. DYNA 2017, 84, 129–137. [Google Scholar] [CrossRef]
- Sun, C.; Hong, S.; Song, M.; Li, H.; Wang, Z. Predicting COVID-19 disease progression and patient outcomes based on temporal deep learning. BMC Med Inform. Decis. Mak. 2021, 21, 45. [Google Scholar] [CrossRef]
- Apornak, A. Human resources allocation in the hospital emergency department during COVID-19 pandemic. Int. J. Healthc. Manag. 2021, 14, 264–270. [Google Scholar] [CrossRef]
- Emanuel, E.J.; Persad, G.; Upshur, R.; Thome, B.; Parker, M.; Glickman, A.; Phillips, J.P. Fair allocation of scarce medical resources in the time of covid-19. New Engl. J. Med. 2020, 382, 2049–2055. [Google Scholar] [CrossRef]
- Dinh, M.M.; Berendsen Russell, S. Overcrowding kills: How COVID-19 could reshape emergency department patient flow in the new normal. EMA Emerg. Med. Australas. 2021, 33, 175–177. [Google Scholar] [CrossRef]
- Ortiz-Barrios, M.; Pancardo, P.; Jiménez-Delgado, G.; De Ávila-Villalobos, J. Applying multi-phase DES approach for modelling the patient journey through accident and emergency departments. In Lecture Notes in Computer Science; Springer: Cham, Switzerland, 2019; Volume 11582. [Google Scholar] [CrossRef]
- Nuñez-Perez, N.; Ortíz-Barrios, M.; McClean, S.; Salas-Navarro, K.; Jimenez-Delgado, G.; Castillo-Zea, A. Discrete-event simulation to reduce waiting time in accident and emergency departments: A case study in a district general clinic. In Lecture Notes in Computer Science; Springer: Cham, Switzerland, 2017; Volume 10586. [Google Scholar] [CrossRef]
- Artiga-Sainz, L.M.; Sarria-Santamera, A.; Martínez-Alés, G.; Quintana-Díaz, M. New approach to managing COVID-19 pandemic in a complex tertiary care medical centre in madrid, spain. Disaster Med. Public Health Prep. 2021, 110, 220–228. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| First Author; Year; Country | Sample | Primary Measure of Outcome | Comparator | Key Findings/Conclusion | Quality of the Evidence |
|---|---|---|---|---|---|
| Abadi [39] *; 2021; Iran | 250 | Total deviation from the nurse scheduling constraints | Grasshopper Optimization Algorithm (GOA); Gray Wolf Optimization algorithm (GWO); Cuckoo Optimization Algorithm (COA); Whale Optimization Algorithm (WOA) | HSSAGA outperformed GOA, GWO, COA, and WOA with a total deviation of 561,020. The absolute difference with the above approaches are: 297,722 (GWO), 385,491 (GOA), 388,944 (WOA), and 164,844 (COA). | High |
| AbdelAziz [40] *; 2020; Saudi Arabia | 254 | WT; secondary outcome: accuracy | Lexicographic method | The WT for admission passed from 0.0016217 s to 2.48 × 10−4 s when using Pareto optimization. Likewise, the accuracy increased from 89% to 97% approximately. | High |
| Aggarwal [41] **; 2020; India | 8 states | Precision; F-Score; Receiver Operating Characteristic (ROC); Precision–Recall (PRC); Matthews Correlation Coefficient (MCC) | TreesJ48; logistics; decision table; ZeroR | The precision, recall, and F-score achieved via the MCDM approach were found to be 0.66, 1.0, and 0.795, respectively. On the other hand, the ROC, PRC, and MCC values were calculated to be 0.5, 0.6, and 0 | Moderate |
| Albahri [42] **; 2021 | 56 | Patient priority | Other MCDM approaches | The maximum patient priority derived from Entropy-TOPSIS was 0.80139 (critical condition) while the minimum was 0.11366 (well health condition) | Moderate |
| Alfaro-Martinez [43] **; 2021; | 1470 | Area under curve (AUC) | No intervention | The AUC was found to be 0.8625 and 0.848 for the numerical and categorical scores of the generating cohort, respectively, whereas in the validation cohort, the AUC were 0.8505 and 0.8313 for the same scores. | Moderate |
| Angeli [44] **; 2021; Italy | 301 | Area under curve (AUC) for prognosis | No intervention | Integration of clinical and laboratory data increases the CT prognostic value (AUC = 0.841). | Low |
| Araz [45] ***; 2020; United States | Not specified | Average time for sample collection; availability of testing kits | No intervention | Drive-through COVID-19 testing sites are a strategy to rapidly gather samples from suspected cases with minimal physician-patient contact. | Very low |
| Assaf [46] **; 2020; Israel | 6695 | AUC; sensitivity, Positive Predict Value (PPV); Negative Predict Value (NPP); accuracy; F-Score. All these measures are related to risk for critical disease | APACHE II risk prediction score | Having a sensitivity of 88%, specificity of 92.7%, and accuracy of 92% for the critical state of COVID-19 patients, it is demonstrated that the ML models outperformed the APACHE II risk score | Moderate |
| Balbi [47] **; 2020; Italy | 340 | Median time from symptom onset to ED admission; prevalence of SARS-CoV−2 infection | No intervention | 92% of patients presented in ED obtained a positive RT-PCR while the median time from symptom onset to ED admission was 7 days. | Low |
| Balmaks [48] **; 2020; Latvia | 67 | Percentage of failure modes in medium or high risk | No intervention | 84.4% of failure modes represent medium or high average risk, with 40.7% being related to organizational factors, 40.7% to individual factors, and 18.5% to environmental factors | Low |
| Brendish [49] **; 2020; Germany | 499 | Median time to COVID-19 results | No intervention | Time to results was significantly lower in the testing group than in the control group (hazard ratio 4023 (95% CI 545–29 696), p < 0.0001). | Low |
| Bolourani [50] *; 2021; United States | 11,525 | Mean accuracy; Area under curve (AUC) | Modified Early Warning Score, XGBoost + SMOTEENN, logistic regression | The XGBoost method evidenced the highest mean accuracy (0.919) while the AUC was found to be 0.77 (standard deviation = 0.05). | High |
| Carlile [51] ***; 2020; United States | 1855 | AUC; accuracy; sensitivity; specificity; percentage of healthcare workers agreed on the easiness of AI implementation in their workflow | No intervention | The resulting AUC was 0.854 while the accuracy, sensitivity, and specificity were 81.6%, 82.8%, and 72.6%, respectively. Likewise, 86% of the healthcare workers agreed on the fact the AI model was easy to implement in their workflow. | Very low |
| Casiraghi [52] **; 2021; Italy | 301 | Area under curve (AUC), sensitivity; specificity; F1 score; accuracy | Generalized linear models | The risk prediction results evidenced a reduction in accuracy by an average of 0.06 concerning the five performance measures (AUC from 0.81 to 0.76, sensitivity from 0.72 to 0.66, specificity from 0.76 to 0.71, F1 score from 0.62 to 0.55, accuracy from 0.74 to 0.68). | High |
| Chen [53] **; 2020; China | 2863 | Time from pre-examination to virus screening; hospital visiting time; waiting time for consultation Secondary outcomes: median waiting time for image examination; moving distance | No intervention | The time from pre-examination to virus screening was reduced from 34 to 3 h, the visiting time was decreased from 18 to 8 h, and the WT for a consultation was narrowed from 2 h to 10 min. in Addition, the median WT for image examination was slackened from 40 to 3 min. Finally, the moving distance passed from 800 to 10 min. | Low |
| Chopra [54] **; 2020; United States | 323 | Median time to revisit; median hospital LOS | No intervention | A total of 8 were discharged from the ED during their index visit and 225 were admitted to the hospital. Among those discharged, 25/98 (25.5%) returned within 28 days of index ED presentation | Very low |
| Chou [55] **; 2021; United States | 580 | AUC; AP; accuracy; F1-Score; kappa; recall (sensitivity); specificity; PPV (precision); NPV; ROC. All these measures for confirmed diagnosis of COVID-19 | No intervention | The three methods, Random Forest outperformed the others with an AUC of 0.86, followed by Gradient Boosting with 0.83, and Extra Trees with 0.82. | Low |
| Diep [56] **; 2021; Belgium | 745 | Area under curve (AUC) | No intervention | The AUC for the predictive model was calculated to be 0.931 (95% CI: 0.910–0.953) with a standard error of 0.010 | Low |
| De Moraes [57] *; 2020; Brazil, | 235 | Area under curve (AUC); sensitivity; specificity; Brier score | No intervention | Support Vector Machine was found to produce the best performance (AUC: 0.85; sensitivity: 0.68; specificity: 0.85; Brier score: 0.16) | Moderate |
| De Nardo [58] **; 2020; Italy | 10 | Patient priority | No intervention | The maximum observed score (critical condition) was 69% while the minimum (well health condition) was 15% | Low |
| Esposito [59] *; 2021; Italy | 77 | Area under curve (AUC) | No intervention | Moderate AUC of 0.76, 0.75, and 0.77 for well-aerated lung, semi-consolidation, and consolidation predicted worst hypoxemia during hospitalization correspondingly. | Moderate |
| Feng [60] **; 2021; China | 132 | AUC; F1-Score; specificity; recall; precision (for early identification of COVID-19 in ED admission) | No intervention | The LASSO model performance in the testing set and the validation cohort resulted in AUC (0.841 and 0.938), the F−1 score (0.571 and 0.667), the recall (1.000 and 1.000), the specificity (0.727 and 0.778), and the precision (0.400 and 0.500) | Moderate |
| Freund [61] **; 2020; Italy, Spain, France, Chile, Belgium, and Quebec. | 3358 | AUC; sensitivity | No intervention | Whole population: AUC = 0.79, 95% CI = 0.76 to 0.81. COVID-19 patients: AUC = 0.81, 95% CI = 0.77 to 0.85. | Low |
| Garbey [62] **; 2020; French | 50 per day | Death rate due to COVID-19 | No intervention | After calibrating the Markov model, the death rate was found to be 25% approximately. | Moderate |
| García de Guadiana-Romualdo [63] **; 2021; Spain | 99 | AUC; accuracy; sensitivity; specificity (For predicting 28-day mortality) | No intervention | MR-proDAM showed the highest AUC for predicting mortality and progression to severe disease. 25.3% of the cases developed into serious diseases, and the 28-day mortality rate was 14.1%. | Low |
| Gavelli [64] **; 2021; Italy | 480 | Death adjusted hazard ratio | Multivariable logistic regression; Cox regression hazard model | When in-hospital mortality was assessed, a meaningful gap was evident between scores of 0–1 and 2 vs. 3 and 4–5. Specifically, the death adjusted Hazard Ratio for Novara-COVID scores of 3 and 4–5 were 2.6 (1.4–4.8) and 8.4 (4.7–15.2), correspondingly. | Moderate |
| Goodacre [65] **; 2021; United Kingdom | 11,773 | AUC; ROC; C-Statistic; sensitivity; specificity | NEWS2 Score | C-statistic of 0.80 (95% confidence interval 0.79–0.81), sensitivity 0.98 (0.97–0.98), and specificity 0.34 (0.34–0.35) | Moderate |
| Gordon [66] **; 2020; United States | 295 | Percentage of patients triggering a symptom alert | No intervention | Of the 210 who completed at least one questionnaire, only 72/210 (34%) triggered a symptom alert to the central nursing pool during their monitoring enrollment period, and only 15% (315/2161) of questionnaires across all patients triggered an alert to the central nursing pool | Moderate |
| Haddad [67] ***; 2021; England | 29 hospitals | Mean number of shortages | No intervention | The optimization model led to a 55% reduction in the number of shortages | Moderate |
| Heldt [68] *; 2021; England | 1235 | AUC; sensitivity; specificity; Brier score; precision-recall | No intervention | Logistic regression reaches an AUC of 0.70, the random forest 0.77 and XGBoost reach 0.76. However, all models showed improved accuracy with F1 scores of 0.56–0.61 | High |
| Joshi [69] **; 2020; United States | 390 | C-statistic; sensitivity | No intervention | The C-statistic was found to be 78% with an optimized sensitivity of 93%. By constraining PCR testing to predict COVID-19 patients, it would be possible to achieve a 33% increase in the allocation of testing resources. | Moderate |
| Kim [70] **; 2020; Korea | 184 | Percentage of COVID-19 patients with fever before OHCA; percentage of COVID-19 patients with pneumonic infiltration | No intervention | 55.6% of patients in the COVID-19-positive group had a fever before out-of-hospital cardiac arrest (OHCA) and 16.9% of the COVID-19-negative group had a fever before OHCA (p = 0.018). A total of 88.9% patients in the COVID-19-positive group had a chest X-ray indicating pneumonic infiltration. | Low |
| Kirby [71] *; 2021; United States | 90,549 | C-statistics for in-hospital all-cause mortality; hospital admissions | Charlson Comorbidity Index (CCI) and Elixhauser Comorbidity Index (ECI) | C-statistics of COVID-related high risk chronic condition predicting in-hospital all-cause mortality was 0.73 (0.69–0.76) | Moderate |
| Kline [72] *; 2021; United States | 19,850 | Prevalence of SARS-CoV−2 infection; area under curve (AUC) | No intervention | In the validation sample (n = 9975), the probability from logistic regression score produced an area under the receiver operating characteristic curve of 0.80 (CI: 0.79–0.81). On the other hand, the pooled prevalence of infection among those tested was 34%. | Moderate |
| Lancet [73] **; 2021, United States | 1673 | LOS; in-hospital mortality; likelihood of survival to discharge | No intervention | The median hospital LOS was 6 days (IQR: 2–11 days) while 34.5% of the patients died. In younger patients, the likelihood of survival to discharge was 1.68 (95% CI, 1.49–1.88; p <0.001). | Low |
| Levine [74] *; 2021; United States | 1014 | C-statistic; sensitivity; specificity (for predicting a 14-day period | No intervention | It obtained a sensitivity of 83% and specificity of 82%, counting with C-statistics for derivation 0.8939 (95% CI, 0.8687 to 0.9192) and validation 0.8685 (95% CI, 0.8095 to 0.9275). | High |
| Liu [75] **; 2020; China | 643 | AUC; sensitivity; specificity; accuracy; median survey time | Conventional ED track | AUC of 0.99, sensitivity of 94.1%, specificity of 95.1%, and accuracy of 94.6% using the training data set. The median survey time without the model in the quarantine station was 100.5 min (95% CI 40.3–152.5), vs. 34 min with the model in the quarantine station (95% CI 24–53; p <.001). | Moderate |
| McDonald [76] **; 2020; United States | 1026 | Prevalence of SARS-CoV−2 infection; area under curve (AUC) | No intervention | The COVID-19 prevalence was 9.6% whereas AUC of 0.89 (95% CI = 0.84–0.94) | Moderate |
| Mehrotra [77] **; 2020: United States | Not specified | Number of ventilators in stock | No intervention | If more than 40% of the existing ventilator inventory is available for COVID-19 patients, the national stockpile is approximately enough to satisfy the demand in mild cases. Nevertheless, if less than 25% of the current ventilator inventory is available for COVID-19 patients, the national stockpile and the projected production could not address the peak demands caused by the pandemic. | Moderate |
| Mitchell [78] ***; 2020; Papua New Guinea | 210 per day | Satisfaction level on the new triage and flow system as a way of identifying the most urgent patients | No intervention | A total of 100% of the respondents agreed on the fact that the new triage and flow system has helped in the identification and prioritization of new patients. | Very low |
| Möckel [79] **; 2021; Germany | 1255 | Area under curve (AUC) representing the need for mechanical ventilation during index stay or after readmission; median LOS | No intervention | A sufficient discriminatory power (C-index 0.75) was achieved for predicting the need for artificial ventilation or death within 14-day period after ED admission | Moderate |
| Moss [80] **; 2020; Australia | Not specified | Mean bed time | No intervention | The mean bed time was found to be 8 days | Low |
| Nepomuceno [81] ***; 2020; Brazil | Not specified | Number of beds feasible to be evacuated and reallocated to COVID-19 patients | No intervention | In summary, 3772 beds are feasible to be evacuated and reassigned for new COVID-19 cases in one year considering different interventions on surgery and patient LOS. | Low |
| Nguyen [82] *; 2020; France | 334 | C-statistics (need for artificial ventilation or death within 14-day period after ED admission) | No intervention | A sufficient discriminatory power (C-index 0.75) was achieved for predicting the need for artificial ventilation or death within 14-day period after ED admission | High |
| O’Reilly [83] ***; 2020; Australia | Not specified | Number of ventilator-free days, hospital length of stay and death during hospital admission. | No intervention | The COVED protocol for addressing the operational consequences of the COVID-19 pandemic | Very low |
| Parker [84] *; 2020; United States | 75 hospitals | Surge capacity | No intervention | An 85% reduction in required surge capacity was achieved considering uncertainties inherent to the COVID-19 pandemic. | High |
| Peng [85] **; 2020; Canada | 39,525 | WT; LOS | No intervention | After simulating the proposed alternatives, the maximum reduction percentage in WT and LOS were 76.33% and 31.16%. | High |
| Plante [86] *; 2020; United States | 192,779 | Area under curve (AUC) | No intervention | AUC was found to be 0.91 (95% CI 0.90–0.92). | Moderate |
| Retzlaff [35] ***; 2020; United States | Not specified | Number of COVID-19 tests processed per day | No intervention | The laboratory was calculated to process 30 tests per day. | Very low |
| Romero-Gameros [87] ***; 2021; Mexico | 2173 | Prevalence of SARS-CoV−2 infection; sensitivity; specificity | No intervention | A prevalence of 53.72% of SARS-CoV−2 infection was detected. The symptom with the highest sensitivity was cough 71%, and a specificity of 52.68% | Low |
| Saegerman [88] **; 2021; Belgium | 2152 | Area under curve (AUC) | No intervention | The resulting area under curve was 0.71 (95% CI: 0.68–0.73) | Low |
| Sangal [36] ***; 2020; United States | 190,000 | Number of provider shifts; contact time between physician and COVID-19 patients | No intervention | The provider shifts decreased by 42% whereas the contact time between physician and COVID-19 patient was reduced by 66% | Low |
| Shamout [89] *; 2020; United States | 19,957 | AUC; sensitivity; specificity; PPV; NPV; F1-score (for predicting deterioration within 96 h) | Imaging reading via two experienced chest radiologists | AUC of 0.786 (95% CI: 0.745–0.830) for prediction of deterioration within 96 h | High |
| Sherren [90] ***; 2020; United Kingdom | 316 | Percentage of patients survived to critical care discharge | No intervention | Of the 201 patients received in the ED with a completed critical care status, 71.1% survived to critical care discharge. | Low |
| Suh [91] ***; 2020; United States | 1832 | Number of patients discharged with oxygen concentrators for use at home (period: 2 months); number of patients discharged with pulse oximeters | No intervention | In this case, 1040 patients were discharged with pulse oximeters and 792 patients were discharged at home with portable oxygen concentrators. | Low |
| Sung [92] **; 2020; United States | 656 | AUC; sensitivity; specificity; PPV; NPV | No intervention | Risk score of ≥3 in the development cohort (sensitivity = 85.1%; specificity of 75.0%; PPV = 71.8% and NPV = 87.0%); in the validation cohort (sensitivity = 79.6%; specificity = 70.9%). AUC = 0.87 (95% confidence interval (CI) 0.82–0.92) in the development cohort and 0.85 (95% CI 0.78–0.92) in the validation cohort. | Moderate |
| Tang [93] **; 2020; United States | 28,454 standard patients and 1693 COVID-19-like illness | Left-without-being-seen rates (LWBSR); LOS | No intervention | After adopting a one-floating provider configuration, the average LOS was reduced by 24.34% for discharged patients and 13.91% for hospitalized patients while LWBSR was slackened by 84.57% | High |
| Teklewold [94] ***; 2020; Ethiopia | Not specified | Number of failure modes associated with no transmission-based precautions | No intervention | A total of 12 out of 22 failure modes were found to be related to non-adherence to transmission-based precautions. | Low |
| Van Klaveren [95] *; 2020; Netherlands | 5912 | AUC; sensitivity; specificity; accuracy; PPV; NPV (for the COVID-19 outcome prediction in the ED) | No intervention | AUC in 4 hospitals: 0.82 (0.78; 0.86); 0.82 (0.74; 0.90); 0.79 (0.70; 0.88); 0.83 (0.79; 0.86) | Moderate |
| Van Singer [96] **; 2021; Switzerland | 76 | 30-day intubation/mortality, and oxygen requirement via AUC | No intervention | The highest accuracy for 30-day oxygen requirement (AUC 0.84; 95% CI, 0.74–0.94). | Low |
| Wang [97] **; 2021; United States | 542 | Percentage and AUC of COVID-19 patients with need for transfer to ICU within 24 h of ED admission | No intervention | A total of 10% of COVID-19 patients required transfer to ICU within 24 h of ED admission. On the other hand, the AUC was found to be 0.54 (standard error 0.02, CI 0.50–0.59) | Low |
| Zeinalnezhad [98] **; 2020; Iran | Not specified | WT | No intervention | The second simulated scenario (hiring more reception staff while assigning free human resources in other wards) led to a 62.3% reduction in patient waiting time. | Moderate |
| Zhang [99] **; 2021; China | 500 | Median time; average LOS; transfer density | No intervention | The median time for each state were the following: state 1 (pre-infection period): 0.26 days, state 2 (acute infection period): 6.13 days, state 3 (pre new coronary pneumonia): 1.05 days. On the other hand, the average LOS for each state were as follows: state 1: 2.14 days, state 2: 5.22 days, and state 3: 6.64 days. Finally, the transfer densities were: state 1: 5.54, state 2: 0.13, and state 3: 0.57. | Moderate |
| Zhang & Cheng [100] ***; 2020; United States | 42,309 | Weekly infection rate in healthcare workers and patients | No intervention | The weekly infection rate in healthcare workers and patients was reduced from 3–5.9%, to 1–2.1%. | Moderate |
| Zhou [101] **; 2021; China | 174 | Time from illness onset to hospital admission | No intervention | In non-survivors, the time from illness onset to hospital admission was 10.0 (7.0–14.0) days whereas in survivors was 10.0 (7.0–13.0) days | Low |
| Authors | Technique Type |
|---|---|
| Single | |
| Tang et al. [93] | Discrete event simulation |
| Nepomuceno et al. [81] | Data envelopment analysis (DEA) |
| Mehrotra et al. [77] | Stochastic optimization |
| AbdelAziz et al. [40] | Multi-objective pareto optimization |
| Peng et al. [85]; Moss et al. [80] | Simulation |
| Aggarwal et al. [41] | Additive utility assumption |
| Araz et al. [45] | System dynamics |
| Hybrid | |
| Garbey et al. [62] | Markov chains, stochastic optimization |
| Albahri et al. [42] | Entropy, TOPSIS |
| De Nardo et al. [58] | Potentially all pairwise ranking of all possible alternatives (PAPRIKA), multi-criteria decision making (MCDM) |
| Parker et al. [84] | Linear programming, mixed-integer programming |
| Zeinalnezhad et al. [98] | Colored petri nets, discrete event simulation |
| Zhang & Cheng. [100] | Logistic regression, Markov chains |
| Abadi et al. [39] | Hybrid salp swarm algorithm and genetic algorithm (HSSAGA) |
| Haddad et al. [67] | Simulation, optimization |
| Authors | Technique Type |
|---|---|
| Single | |
| Chen et al. [53] | Lean Manufacturing |
| Casiraghi et al. [52]; Teklewold et al. [94]; Balmaks et al. [48] | FMEA |
| Hybrid | |
| Retzlaff [35] | Critical pathways, lean manufacturing |
| O’Reilly et al. [83] | Logistic regression, survival regression, linear regression, continuous quality improvement |
| Authors | Technique Type |
|---|---|
| Single | |
| Chopra et al. [54]; Sung et al. [92]; Alfaro-Martinez et al. [43]; Kirby et al. [71]; Lancet et al. [73] | Multivariate logistic regression |
| Nguyen et al. [82] | Multivariate cox proportional hazard model |
| Joshi et al. [69]; Kim et al. [70]; Levine et al. [74]; Wang et al. [97]; Angeli et al. [44]; Zhou et al. [101] | Logistic regression |
| Liu et al. [75] | Artificial intelligence |
| Freund et al. [61] | Multivariate binary logistic regression |
| Brendish et al. [49]; Esposito et al. [59] | Cox proportional hazards regression |
| Gordon et al. [66] | Mixed-effect logistic regression |
| García de Guadiana-Romualdo et al. [63] | Multivariate regression |
| Kline et al. [72] | Stepwise forward logistic regression |
| Carlile et al. [51] | Deep learning |
| Plante et al. [86] | Gradient boosting |
| Hybrid | |
| Shamout et al. [89] | Deep neural network, gradient boosting |
| Balbi et al. [47] | Poisson regression, logistic regression |
| Van Klaveren et al. [95] | Logistic regression with post hoc uniform shrinkage |
| De Moraes et al. [57] | Neural networks, random forest, gradient boosting, logistic regression, support vector machine (SVM) |
| McDonald et al. [76]; Heldt et al. [68] | Logistic regression, random forest, and gradient-boosted decision tree |
| Zhang & Cheng [100]; Zhang et al. [99] | Logistic regression, Markov |
| O’Reilly et al. [83] | Logistic regression, survival regression, Linear regression, continuous quality improvement |
| Assaf et al. [46]; Chou et al. [55] | Neural network, random forest, classification and regression decision tree (CRT) |
| Van Singer et al. [96]; Möckel et al. [79] | Logistic regression and CRT |
| Diep et al. [56] | Logistic regression, Mann–Whitey, chi-cuadrado |
| Saegerman et al. [88] | Binary logistic regression and bootstrapped quantile regression, classification and regression tree analysis. |
| Romero-Gameros et al. [87] | Logistic regression, Mantel–Haenszel |
| Bolourani et al. [50] | Artificial intelligence, logistic regression, XGBoost combines a recursive gradient-boosting method called Newton boosting, with a decision-tree model, decision making |
| Goodacre et al. [65]; Feng et al. [46] | Multivariable regression with least absolute shrinkage and selection operator (LASSO) |
| Gavelli et al. [64] | logistic regression and cox regression |
| Authors | Technique Type |
|---|---|
| Single | |
| Suh et al. [91]; Sangal et al. [36]; Sherren et al. [90] | Critical pathways |
| Mitchell et al. [78] | Intelligent integrated triage tool |
| Hybrid | |
| Retzlaff [35] | Critical pathways, lean manufacturing |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ortíz-Barrios, M.A.; Coba-Blanco, D.M.; Alfaro-Saíz, J.-J.; Stand-González, D. Process Improvement Approaches for Increasing the Response of Emergency Departments against the COVID-19 Pandemic: A Systematic Review. Int. J. Environ. Res. Public Health 2021, 18, 8814. https://doi.org/10.3390/ijerph18168814
Ortíz-Barrios MA, Coba-Blanco DM, Alfaro-Saíz J-J, Stand-González D. Process Improvement Approaches for Increasing the Response of Emergency Departments against the COVID-19 Pandemic: A Systematic Review. International Journal of Environmental Research and Public Health. 2021; 18(16):8814. https://doi.org/10.3390/ijerph18168814
Chicago/Turabian StyleOrtíz-Barrios, Miguel Angel, Dayana Milena Coba-Blanco, Juan-José Alfaro-Saíz, and Daniela Stand-González. 2021. "Process Improvement Approaches for Increasing the Response of Emergency Departments against the COVID-19 Pandemic: A Systematic Review" International Journal of Environmental Research and Public Health 18, no. 16: 8814. https://doi.org/10.3390/ijerph18168814
APA StyleOrtíz-Barrios, M. A., Coba-Blanco, D. M., Alfaro-Saíz, J.-J., & Stand-González, D. (2021). Process Improvement Approaches for Increasing the Response of Emergency Departments against the COVID-19 Pandemic: A Systematic Review. International Journal of Environmental Research and Public Health, 18(16), 8814. https://doi.org/10.3390/ijerph18168814