
Cost-Utility Analysis of Oxybutynin vs. OnabotulinumtoxinA (Botox) in the Treatment of Overactive Bladder Syndrome

 , , , , and
, , , , and
Abstract
1. Introduction
1.1. Background
1.2. Motivation and Rationale
1.3. Study Objectives
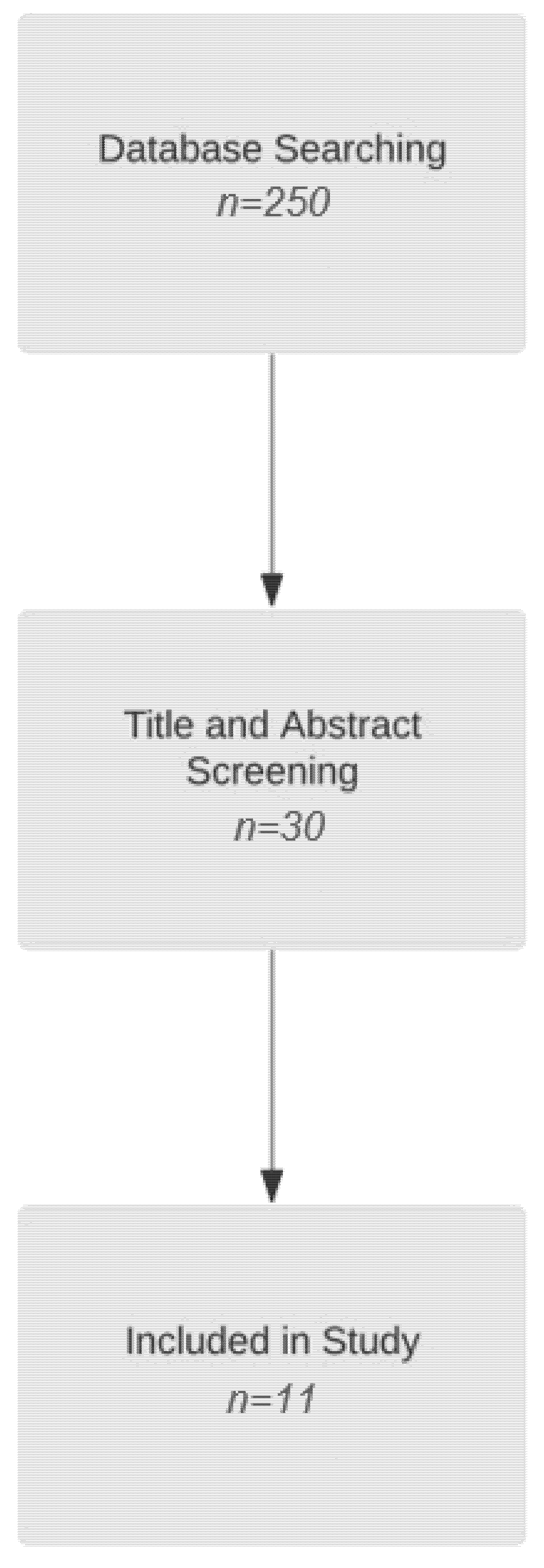
1.4. Literature Review
2. Methods
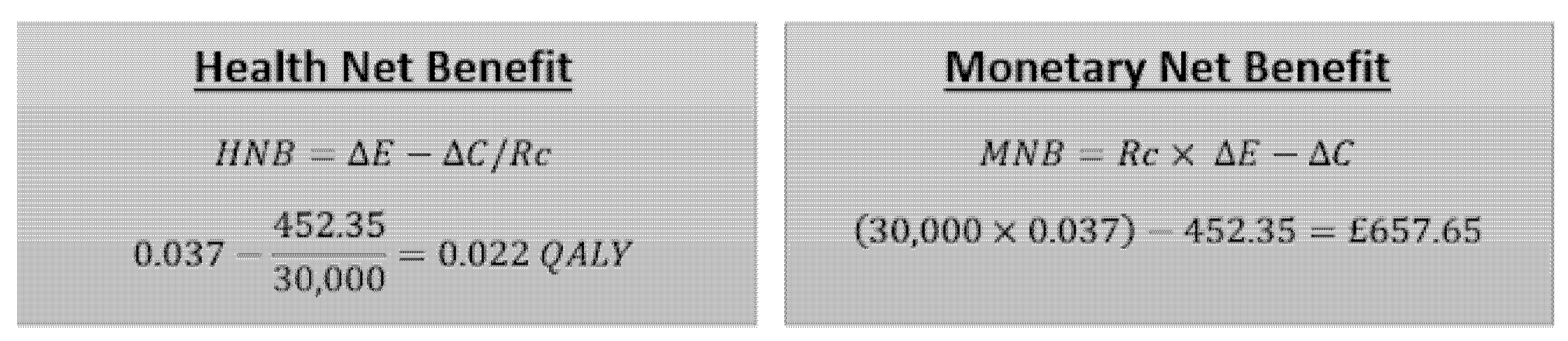
2.1. Choice of Analysis
2.2. Choice of Perspective
2.3. Costs
2.3.1. Medication Costs
2.3.2. Physiotherapy
2.4. Benefits
2.5. Modelling
3. Results
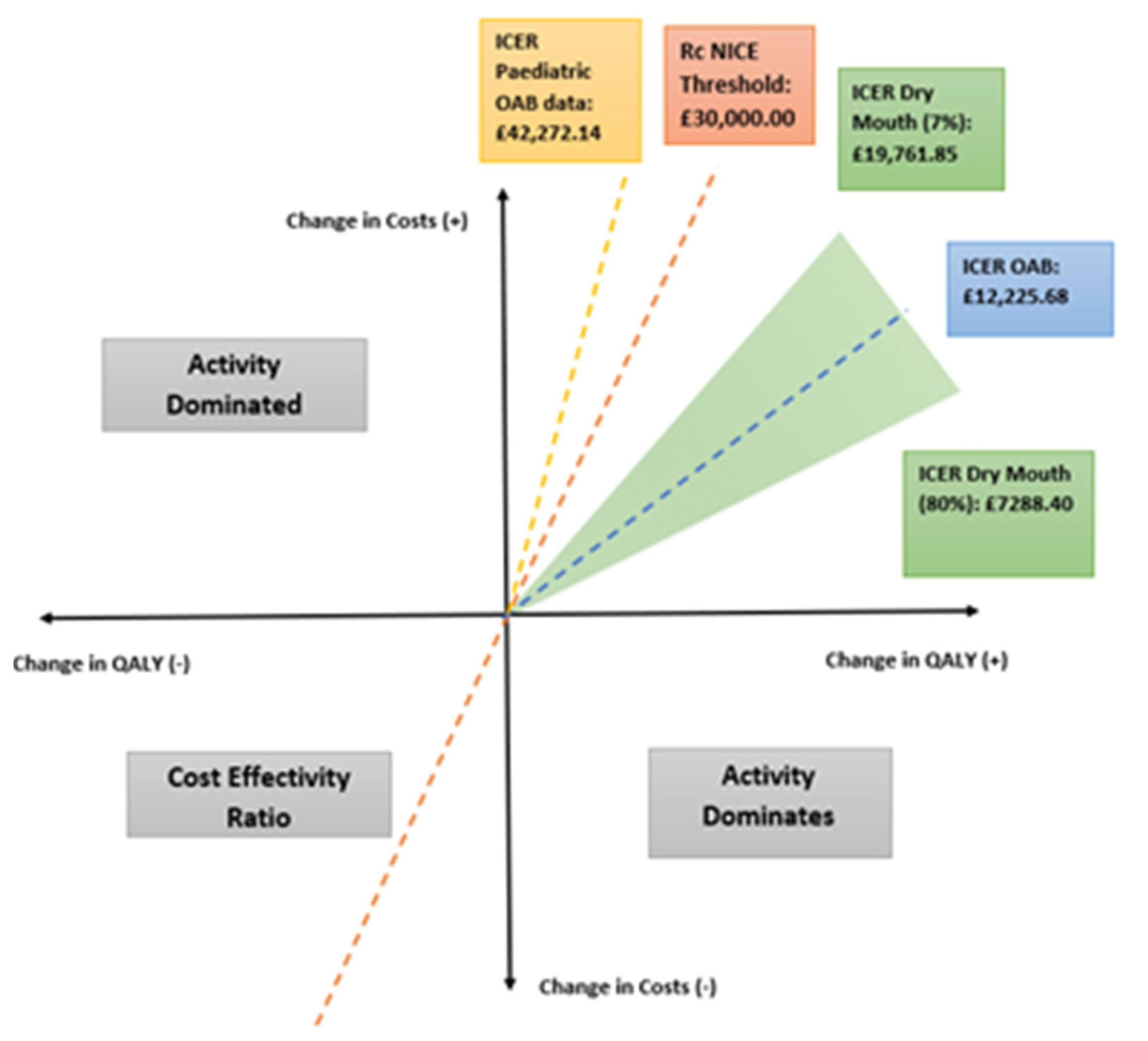
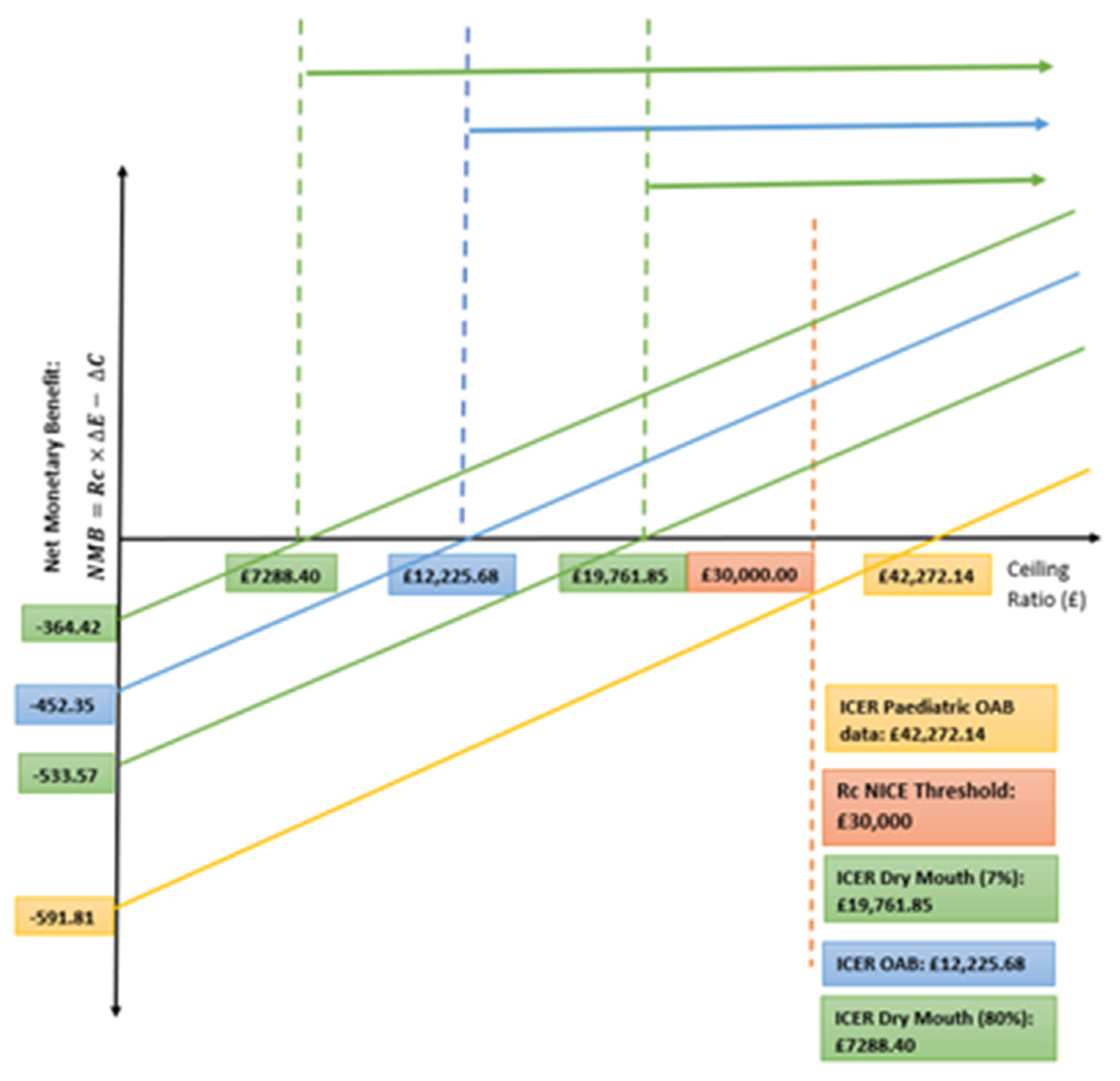
Sensitivity Analysis
4. Discussion
4.1. Limitations
4.2. Contribution to the Literature
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Component | Cost | Discount Rate | Cost with Discount | Reference |
|---|---|---|---|---|
| Botox Vial | £138.20 | N/A | £138.20 | (NICE BNF, 2021a [26]) |
| Botox administration | £219.00 | 1.0356 | (£219.00 × 1.0356) = £269.20 | OnabotulinumtoxinA in the treatment of overactive bladder (Freemantle et al., 2016 [22]) |
| GP Visit | £62.70 | 1.0355 | (62.70 × 1.0355) = £74.47 | Unit Costs of Health and Social Care 2016 (PSSRU, 2016 [30]) |
| Urology outpatient visit | 108 | 1.0352 | (108 × 1.0352) = £115.69 | 2018/2019 National cost collection data of NHS (NHS England, 2018 [45]) |
| TOTAL | £138.20 + 269.20 + 74.47 + £115.69 = £597.56 | £597.56 | ||
| Component | Cost | Discount Rate | Cost with Discount | Reference |
|---|---|---|---|---|
| Botox Vial | £138.20 | N/A | £138.20 | (NICE BNF, 2021a [26]) |
| Botox administration | £219.00 | 1.0356 | (£219.00 × 1.0356) = £269.20 | OnabotulinumtoxinA in the treatment of overactive bladder (Freemantle et al. N, 2016 [22]) |
| TOTAL | £138.20 + 269.20 = £407.40 | £407.40 | ||
| Component | Cost | Discount Rate | Cost with Discount | Reference |
|---|---|---|---|---|
| Oxybutynin treatment | £3.00 per month | N/A | (3.00 × 12) = £36.00 | (NICE BNF, 2021b [27]) |
| GP Visit | £62.70 | 1.0355 | (62.70 × 1.0355) = £74.47 | Unit Costs of Health and Social Care 2016 (PSSRU, 2016 [30]) |
| GP maintenance visits | £42.60 | 1.0353 | (£42.60 × 1.0353) = £47.23 | Cost-effectiveness of solifenacin compared with oral antimuscarinic agents (Hakimi et al., 2018 [32]) |
| Urology outpatient visit | 108 | 1.0352 | (108 × 1.0352) = £115.69 | 2018/2019 National cost collection data of NHS (NHS England, 2018 [45]) |
| TOTAL | £36.00 + £115.69 + £74.47 + £47.23 = £273.39 | £273.39 | ||
| Component | Cost | Discount Rate | Cost with Discount | Reference |
|---|---|---|---|---|
| Incontinence Pads: Dry | £0.17 | 1.0356 | 365 × 0.17 × 1.0356 = £76.28 | OnabotulinumtoxinA in the treatment of overactive bladder (Freemantle et al., 2016 [22]) |
| Incontinence Pads: 0–2 | £0.17 × 2 | 1.0356 | 365 × 0.17 × 2 × 1.0356 = £152.55 | |
| Incontinence Pads: 3–5 | £0.17 × 3 | 1.0356 | 365 × 0.17 × 3 × 1.0356 = £228.83 | |
| Incontinence Pads: 5+ | £0.17 × 7 | 1.0356 | 365 × 0.17 × 7 × 1.0356 = £533.92 |
Appendix B
| Component | Cost | Discount Rate | Cost with Discount | Reference |
|---|---|---|---|---|
| Urinalysis | £19 | N/A | £19 | (NIHR, 2020 [45]) |
| UTI treatment: physician time | £62.70 | 1.0355 | (62.70 × 1.0355) = £74.47(10) | Unit Costs of Health and Social Care 2016 (PSSRU, 2016 [30]) |
| UTI treatment: Trimethoprim 200 mg | £1.27 14 pills | N/A | £1.27/14 × 10 = £0.91 200 mg BD 5 days | (NICE BNF, 2021d [28]) |
| TOTAL UTI PRICE: | £74.47 + £0.91 + £19 = £94.38 | £94.38 | ||
| Constipation: Senna tablets | £2.20/60 tablets 25 packs a year->4 tablets a day | N/A | 2.20 × 25 = £55.00 | (NICE BNF, 2021c [29]) |
| Constipation: Physician time | £62.70 | 1.0355 | (62.70 × 1.0355) = £74.47(10) | Unit Costs of Health and Social Care 2016 (NHS England, 2016 [45]) |
| Constipation: Total Cost | £55.00 + £74.47 = £129.47 | £129.47 | ||
| Dry Mouth: Total Cost | £0 | N/A | N/A | There is no prescription treatment for dry mouth. |
| Urinary retention Catheter cost22 | £0.75 | 1.0356 | £0.75 × 1.0356 = £0.92 | OnabotulinumtoxinA in the treatment of overactive bladder (Freemantle et al., 2016 [22]) |
| Urinary retention: GP appointment | £62.70 | 1.0355 | (62.70 × 1.0355) = £74.47(10) | Unit Costs of Health and Social Care 2016 (PSSRU, 2016 [30]) |
| Urinary retention: Total Cost | £74.47 + £0.92 = £75.39 | £75.39 | ||
Appendix C
| Component | Probability | Reference | Comments/Limitations |
|---|---|---|---|
| Reinjection of Botox | Yes: 0.667 No:0.333 | OnabotulinumtoxinA in the treatment of overactive bladder (Freemantle et al., 2016 [22]) | |
| Treatment Switch to Botox: with no adverse effects | No: 0.982 Yes: 0.018 | Patterns of use of antimuscarinic drugs to treat overactive bladder (Margulis et al., 2018 [31]) | |
| Treatment Switch to Botox: with adverse effects | No:0.766 Yes: 0.234 | Patterns of use of antimuscarinic drugs to treat overactive bladder (Margulis et al., 2018 [31]) | |
| Treatment Discontinuation with adverse effects | Yes:0.9 No:0.1 | Cost-effectiveness of solifenacin compared with oral antimuscarinic agents (Hakimi et al., 2018 [32]) | |
| Treatment Discontinuation without adverse effects | Yes:0.064 No:0.936 | Cost-effectiveness of solifenacin compared with oral antimuscarinic agents (Hakimi et al., 2018 [32]) | |
| Urinary Tract Infection | Yes: 0.204 No: 0.796 | OnabotulinumtoxinA in the treatment of overactive bladder (Freemantle, 2016 [22]) | |
| Urinary Retention | Yes: 0.069 No: 0.931 | OnabotulinumtoxinA in the treatment of overactive bladder (Freemantle, 2016 [22]) | |
| Dry Mouth | Yes: 0.37 No: 0.63 | Cost-effectiveness of solifenacin compared with oral antimuscarinic agents (Hakimi et al., 2018 [32]) | Extreme values were found for this point e.g., 80%, and 7%. Which is why we conducted a sensitivity analysis. |
| Constipation | Yes: 0.037 No:0.963 | Cost-effectiveness of solifenacin compared with oral antimuscarinic agents (Hakimi et al., 2018 [32]) | |
| Probability of Level 1–4 UIE for discontinued oxybutynin | (1) 0.0 (2) 0.178 (3) 0.351 (4) 0.356 | OnabotulinumtoxinA in the treatment of overactive bladder (Freemantle el 2016 [22]) | The probabilities of people having UIE episodes after failed anticholinergic use, without further treatment. |
| Probability of Level 1–4 for oxybutynin | (1) 0.23 (2) 0.367 (3) 0.191 (4) 0.212 | A Comparative Review of Oxybutynin Chloride Formulations (Kennelly, 2010 [33]) | The probability of 23% was found from this article. The remaining probabilities of levels 2–4 were calculated on the assumption that they followed the same proportions as the Botox data. |
| Probability of Level 1–4 for Botox | (1) 0.289 (2) 0.339 (3) 0.176 (4) 0.196 | OnabotulinumtoxinA in the treatment of overactive bladder (Freemantle et al., 2016 [22]) | |
| Probability of Level 1–4 for reinjected Botox | (1) 0.654 (2) 0.166 (3) 0.085 (4) 0.095 | Interstim Sacral Neuromodulation and Botox Botulinum-A Toxin Intradetrusor Injections for Refractory Urge Urinary Incontinence (Shepherd, 2011 [23]) | The probability of 65% was found from this article. The remaining probabilities of levels 2–4 were calculated on the assumption that they followed the same proportions as the Botox probabilities. |
Appendix D
| Component | Utility | Reference | Comments |
|---|---|---|---|
| Level 1: Dry | 0.915 | OnabotulinumtoxinA in the treatment of overactive bladder (Freemantle et al., 2016 [22]) | These utilities are the standardized utilities at the EQ5D for that number of UIE’s for 1 year. The antimuscarinic trials output was measured in 5 incontinence levels which could be converted to this more intuitive level system. Therefore, we did this and made the assumption that the utilities would be the same. |
| Level 2: 1–2 | 0.853 | ||
| Level 3: 3–5 | 0.796 | ||
| Level 4: 5+ | 0.767 | ||
| Disutility per side effect | −0.036 | Cost-effectiveness of solifenacin compared with oral antimuscarinic agents (Hakimi et al., 2018 [32]) | This was based on dry mouth and constipation. We assumed the same disutility could be applied to urinary retention and urinary tract infection. |
Appendix E
| Level | Number of Urinary Incontinence Episodes | Probability of Each Level for Oxybutynin-Adult | Probability of Each Level for Oxybutynin-Children. |
|---|---|---|---|
| 1/Dry | 0 | 0.23 | 0.61 |
| 2 | 1–2 | 0.367 | 0.185 |
| 3 | 3–5 | 0.191 | 0.097 |
| 4 | 5+ | 0.212 | 0.108 |
Appendix F
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Written in English | Written in language other than English |
| Articles specifically referring to overactive bladder syndrome | Articles referring to non-OAB conditions e.g., UTIs |
| Articles focusing on antimuscarinic/anticholinergic/Botox treatments | Articles focusing on treatment plans that do not include antimuscarinics/anticholinergics/Botox |
| 5+ Systematic reviews, RCTs, meta-analysis, CEA, CUA, CBA | Qualitative studies |
References
- Wein, A.J.; Rovner, E.S. Definition and epidemiology of overactive bladder. Urology 2002, 60, 7–12. [Google Scholar] [CrossRef]
- Bartoli, S.; Aguzzi, G.; Tarricone, R. Impact on Quality of Life of Urinary Incontinence and Overactive Bladder: A Systematic Literature Review. Urology 2010, 75, 491–500. [Google Scholar] [CrossRef]
- Moon, S.-J.; Kim, Y.T.; Lee, T.Y.; Moon, H.; Kim, M.J.; Kim, S.A.; Choi, B.Y. The Influence of an Overactive Bladder on Falling: A Study of Females Aged 40 and Older in the Community. Int. Neurourol. J. 2011, 15, 41–47. [Google Scholar] [CrossRef]
- Eapen, R.; Radomski, S. Review of the epidemiology of overactive bladder. Res. Rep. Urol. 2016, 8, 71–76. [Google Scholar] [CrossRef]
- Franco, I. Pediatric Overactive Bladder Syndrome. Pediatr. Drugs 2007, 9, 379–390. [Google Scholar] [CrossRef]
- Banakhar, M.A.; Al-Shaiji, T.F.; Hassouna, M.M. Pathophysiology of overactive bladder. Int. Urogynecol. J. 2012, 23, 975–982. [Google Scholar] [CrossRef] [PubMed]
- National Institute for Health and Care Excellence (NICE). Scenario: Overactive Bladder. 2019. Available online: https://cks.nice.org.uk/topics/luts-in-men/management/overactive-bladder/ (accessed on 29 January 2021).
- National Institute for Health and Care Excellence (NICE). Invasive Procedures for Overactive Bladder in Women. 2020. Available online: https://pathways.nice.org.uk/pathways/urinary-incontinence-and-pelvic-organ-prolapse-in-women/invasive-procedures-for-overactive-bladder-in-women.pdf (accessed on 29 January 2021).
- Duthie, J.B.; Vincent, M.; Herbison, G.P.; Wilson, D.I.; Wilson, D. Botulinum toxin injections for adults with overactive bladder syndrome. Cochrane Database Syst. Rev. 2011, CD005493. [Google Scholar] [CrossRef]
- Karsenty, G.; Denys, P.; Amarenco, G.; De Seze, M.; Gamé, X.; Haab, F.; Kerdraon, J.; Perrouin-Verbe, B.; Ruffion, A.; Saussine, C.; et al. Botulinum Toxin A (Botox®) Intradetrusor Injections in Adults with Neurogenic Detrusor Overactivity/Neurogenic Overactive Bladder: A Systematic Literature Review. Eur. Urol. 2008, 53, 275–287. [Google Scholar] [CrossRef]
- NHS Dorset Clinical Commissioning Group. Botulinum Toxin Type A for Overactive Bladder. 2017. Available online: https://www.dorsetccg.nhs.uk/wp-content/uploads/2018/04/Botulinum-Toxin-Type-A-for-Overactive-Bladder.pdf?UNLID= (accessed on 1 February 2021).
- Benner, J.S.; Nichol, M.; Rovner, E.S.; Jumadilova, Z.; Alvir, J.; Hussein, M.; Fanning, K.; Trocio, J.N.; Brubaker, L. Patient-reported reasons for discontinuing overactive bladder medication. BJU Int. 2010, 105, 1276–1282. [Google Scholar] [CrossRef]
- Irwin, D.E.; Mungapen, L.; Milsom, I.; Kopp, Z.; Reeves, P.; Kelleher, C. The economic impact of overactive bladder syndrome in six Western countries. BJU Int. 2009, 103, 202–209. [Google Scholar] [CrossRef]
- Basra, R.K.; Wagg, A.; Chapple, C.; Cardozo, L.; Castro-Diaz, D.; Pons, M.E.; Kirby, M.; Milsom, I.; Vierhout, M.; Van Kerrebroeck, P.; et al. A review of adherence to drug therapy in patients with overactive bladder. BJU Int. 2008, 102, 774–779. [Google Scholar] [CrossRef] [PubMed]
- Coupland, C.A.C.; Hill, T.; Dening, T.; Morriss, R.; Moore, M.; Hippisley-Cox, J. Anticholinergic Drug Exposure and the Risk of Dementia. JAMA Intern. Med. 2019, 179, 1084–1093. [Google Scholar] [CrossRef] [PubMed]
- Murray, B.; Hessami, S.H.; Gultyaev, D.; Lister, J.; Dmochowski, R.; Gillard, K.K.; Stanisic, S.; Tung, A.; Boer, R.; Kaplan, S. Cost–effectiveness of overactive bladder treatments: From the US payer perspective. J. Comp. Eff. Res. 2019, 8, 61–71. [Google Scholar] [CrossRef] [PubMed]
- Andersson, K.E.; Chapple, C.R. Oxybutynin and the overactive bladder. World J. Urol. 2001, 19, 319–323. [Google Scholar] [CrossRef]
- Cruz, F.; Herschorn, S.; Aliotta, P.; Brin, M.; Thompson, C.; Lam, W.; Daniell, G.; Heesakkers, J.; Haag-Molkenteller, C. Efficacy and Safety of OnabotulinumtoxinA in Patients with Urinary Incontinence Due to Neurogenic Detrusor Overactivity: A Randomised, Double-Blind, Placebo-Controlled Trial. Eur. Urol. 2011, 60, 742–750. [Google Scholar] [CrossRef]
- Dmochowski, R.; Chapple, C.; Nitti, V.; Chancellor, M.; Everaert, K.; Thompson, C.; Daniell, G.; Zhou, J.; Haag-Molkenteller, C. Efficacy and Safety of OnabotulinumtoxinA for Idiopathic Overactive Bladder: A Double-Blind, Placebo Controlled, Randomized, Dose Ranging Trial. J. Urol. 2010, 184, 2416–2422. [Google Scholar] [CrossRef]
- Drake, M.J.; Nitti, V.; Ginsberg, D.A.; Brucker, B.; Hepp, Z.; McCool, R.; Glanville, J.M.; Fleetwood, K.; James, D.; Chapple, C.R. Comparative assessment of the efficacy of onabotulinumtoxinA and oral therapies (anticholinergics and mirabegron) for overactive bladder: A systematic review and network meta-analysis. BJU Int. 2017, 120, 611–622. [Google Scholar] [CrossRef]
- Carlson, J.J.; Hansen, R.N.; Dmochowski, R.R.; Globe, D.R.; Colayco, D.C.; Sullivan, S.D. Estimating the Cost-Effectiveness of OnabotulinumtoxinA for Neurogenic Detrusor Overactivity in the United States. Clin. Ther. 2013, 35, 414–424. [Google Scholar] [CrossRef]
- Freemantle, N.; Khalaf, K.; Loveman, C.; Stanisic, S.; Gultyaev, D.; Lister, J.; Drake, M. OnabotulinumtoxinA in the treatment of overactive bladder: A cost-effectiveness analysis versus best supportive care in England and Wales. Eur. J. Health Econ. 2015, 17, 911–921. [Google Scholar] [CrossRef][Green Version]
- Shepherd, J.P.; Carter-Brooks, C.; Chermanksy, C. A cost-effectiveness analysis of Onabotulinumtoxin A as first-line treatment for overactive bladder. Int. Urogynecol. J. 2018, 29, 1213–1219. [Google Scholar] [CrossRef]
- Siddiqui, N.Y.; Amundsen, C.L.; Visco, A.G.; Myers, E.R.; Wu, J. Cost-Effectiveness of Sacral Neuromodulation Versus Intravesical Botulinum A Toxin for Treatment of Refractory Urge Incontinence. J. Urol. 2009, 182, 2799–2804. [Google Scholar] [CrossRef]
- National Cost Collection 2019. NHS England and NHS Improvement. 2020. Available online: https://www.england.nhs.uk/wp-content/uploads/2020/08/1_-_NCC_Report_FINAL_002.pdf (accessed on 9 February 2021).
- Botulinum Toxin Type A. British National Formulary. 2021. Available online: https://bnf.nice.org.uk/medicinal-forms/botulinum-toxin-type-a.html (accessed on 9 February 2021).
- Oxybutynin Hydrochloride. British National Formulary. 2021. Available online: https://bnf.nice.org.uk/medicinal-forms/oxybutynin-hydrochloride.html (accessed on 9 February 2021).
- Trimethoprim British National Formulary. 2021. Available online: https://bnf.nice.org.uk/medicinal-forms/trimethoprim.html (accessed on 9 February 2021).
- Senna British National Formulary. 2021. Available online: https://bnf.nice.org.uk/medicinal-forms/senna.html (accessed on 9 February 2021).
- Curtis, L.; Burns, A. Unit Costs of Health and Social Care. Personal Social Services Research Unit, University of Kent, Canterbury. 2016. Available online: https://www.pssru.ac.uk/project-pages/unit-costs/unit-costs-2016/ (accessed on 9 February 2021).
- Margulis, A.V.; Linder, M.; Arana, A.; Pottegård, A.; Berglind, I.A.; Bui, C.; Kristiansen, N.S.; Bahmanyar, S.; McQuay, L.J.; Atsma, W.J.; et al. Patterns of use of antimuscarinic drugs to treat overactive bladder in Denmark, Sweden, and the United Kingdom. PLoS ONE 2018, 13, e0204456. [Google Scholar] [CrossRef] [PubMed]
- Hakimi, Z.; Kelleher, C.; Aballéa, S.; Maman, K.; Nazir, J.; Mankowski, C.; Odeyemi, I. Cost-effectiveness of solifenacin compared with oral antimuscarinic agents for the treatment of patients with overactive bladder in the UK. J. Mark. Access Health Policy 2018, 6, 1438721. [Google Scholar] [CrossRef] [PubMed]
- Kennelly, M.J. A comparative review of oxybutynin chloride formulations: Pharmacokinetics and therapeutic efficacy in over-active bladder. Rev. Urol. 2010, 12, 12–19. Available online: https://pubmed.ncbi.nlm.nih.gov/20428289/ (accessed on 10 February 2021).
- Brazier, J. Is the EQ–5D fit for purpose in mental health? Br. J. Psychiatry 2010, 197, 348–349. [Google Scholar] [CrossRef]
- NICE’s 2019/2020 methods review: Challenges and opportunities. Pharm. Outcomes News 2020, 846, 2–8. [CrossRef]
- NHS.UK. Overview: Laxatives. Available online: https://www.nhs.uk/conditions/laxatives/ (accessed on 10 February 2021).
- Pharmaceutical Services Negotiating Committee. New Measures to Support Safe Use of Stimulant Laxatives Available over-the-Counter. Available online: https://psnc.org.uk/our-news/new-measures-to-support-safe-use-of-stimulant-laxatives-available-over-the-counter/ (accessed on 8 February 2021).
- NHS.UK. Dry Mouth. Available online: https://www.nhs.uk/conditions/dry-mouth/ (accessed on 14 February 2021).
- Kay, S.; Tolley, K.; Colayco, D.; Khalaf, K.; Anderson, P.; Globe, D. Mapping EQ-5D Utility Scores from the Incontinence Quality of Life Questionnaire among Patients with Neurogenic and Idiopathic Overactive Bladder. Value Health 2013, 16, 394–402. [Google Scholar] [CrossRef] [PubMed]
- Di Rosa, M.; Lamura, G. The impact of incontinence management on informal caregivers’ quality of life. Aging Clin. Exp. Res. 2015, 28, 89–97. [Google Scholar] [CrossRef]
- Visco, A.G.; Zyczynski, H.; Brubaker, L.; Nygaard, I.; Xu, X.; Lukacz, E.S.; Paraiso, M.F.; Greer, J.; Rahn, D.D.; Meikle, S.F.; et al. Cost-Effectiveness Analysis of Anticholinergics Versus Botox for Urgency Urinary Incontinence. Female Pelvic Med. Reconstr. Surg. 2016, 22, 311–316. [Google Scholar] [CrossRef]
- Lee, J.H.; Kim, K.R.; Lee, Y.S.; Han, S.W.; Kim, K.S.; Song, S.H.; Baek, M.; Park, K. Efficacy, Tolerability, and Safety of Oxybutynin Chloride in Pediatric Neurogenic Bladder With Spinal Dysraphism: A Retrospective, Multicenter, Observational Study. Korean J. Urol. 2014, 55, 828–833. [Google Scholar] [CrossRef]
- Warde, N. Solifenacin causes less dry mouth than oxybutynin in OAB. Nat. Rev. Urol. 2010, 7, 303. [Google Scholar] [CrossRef] [PubMed]
- Lai, H.H.; Boone, T.B.; Appell, R.A. Selecting a Medical Therapy for Overactive Bladder. Rev. Urol. 2002, 4, S28–S37. [Google Scholar] [PubMed]
- NHS England. Available online: https://www.england.nhs.uk/national-cost-collection/ (accessed on 10 February 2021).




| Treatment | Cost |
|---|---|
| Botox | £597.56 |
| Botox Reinjection | £407.40 |
| Oxybutynin | £273.39 |
| Constipation | £129.47 |
| Dry Mouth | £0.00 |
| UTI | £94.38 |
| Urinary Retention | £75.39 |
| Level 1 Pad Use | £76.28 |
| Level 2 Pad Use | £152.55 |
| Level 3 Pad Use | £228.83 |
| Level 4 Pad Use | £533.92 |
| Level | Number of Urinary Incontinence Episodes | Utilities |
|---|---|---|
| 1/Dry | 0 | 0.915 |
| 2 | 1–2 | 0.853 |
| 3 | 3–5 | 0.796 |
| 4 | 5+ | 0.767 |
| Botox | Oxybutynin | |
|---|---|---|
| Total Cost (£) | £1063.54 | £611.19 |
| Total Utility (QALY) | 0.859 | 0.822 |
| ICER | ||
| SENSITIVITY: | Botox | Oxybutynin |
|---|---|---|
| Total Cost (£) | £1063.54 | £471.73 |
| Total Utility (QALY) | 0.859 | 0.845 |
| ICER | ||
| SENSITIVITY at 80%: | Botox | Oxybutynin |
|---|---|---|
| Total Cost (£) | £1063.54 | £699.12 |
| Total Utility (QALY) | 0.859 | 0.809 |
| ICER | ||
| SENSITIVITY at 7%: | Botox | Oxybutynin |
|---|---|---|
| Total Cost (£) | £1063.54 | £529.97 |
| Total Utility (QALY) | 0.859 | 0.832 |
| ICER | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Shabir, H.; Hashemi, S.; Al-Rufayie, M.; Adelowo, T.; Riaz, U.; Ullah, U.; Alam, B.; Anwar, M.; de Preux, L. Cost-Utility Analysis of Oxybutynin vs. OnabotulinumtoxinA (Botox) in the Treatment of Overactive Bladder Syndrome. Int. J. Environ. Res. Public Health 2021, 18, 8743. https://doi.org/10.3390/ijerph18168743
Shabir H, Hashemi S, Al-Rufayie M, Adelowo T, Riaz U, Ullah U, Alam B, Anwar M, de Preux L. Cost-Utility Analysis of Oxybutynin vs. OnabotulinumtoxinA (Botox) in the Treatment of Overactive Bladder Syndrome. International Journal of Environmental Research and Public Health. 2021; 18(16):8743. https://doi.org/10.3390/ijerph18168743
Chicago/Turabian StyleShabir, Habiba, Sana Hashemi, Moussa Al-Rufayie, Tayo Adelowo, Umar Riaz, Umayair Ullah, Benyamin Alam, Mehreen Anwar, and Laure de Preux. 2021. "Cost-Utility Analysis of Oxybutynin vs. OnabotulinumtoxinA (Botox) in the Treatment of Overactive Bladder Syndrome" International Journal of Environmental Research and Public Health 18, no. 16: 8743. https://doi.org/10.3390/ijerph18168743
APA StyleShabir, H., Hashemi, S., Al-Rufayie, M., Adelowo, T., Riaz, U., Ullah, U., Alam, B., Anwar, M., & de Preux, L. (2021). Cost-Utility Analysis of Oxybutynin vs. OnabotulinumtoxinA (Botox) in the Treatment of Overactive Bladder Syndrome. International Journal of Environmental Research and Public Health, 18(16), 8743. https://doi.org/10.3390/ijerph18168743