
Impact of Parental Education and Physical Activity on the Long-Term Development of the Physical Fitness of Primary School Children: An Observational Study

 ,
,  ,
, 


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patient and Public Involvement
2.2. Sample
2.3. Measurements in Children
2.4. Questionnaire for Parents
2.5. Statistical Analysis
3. Results
3.1. Parental Variables
3.2. Children’s Characteristics
3.3. Comparison of Parental Education Group and Parental PA Group
3.4. Comparison of Included and Excluded Children to the AN(C)OVA
4. Discussion
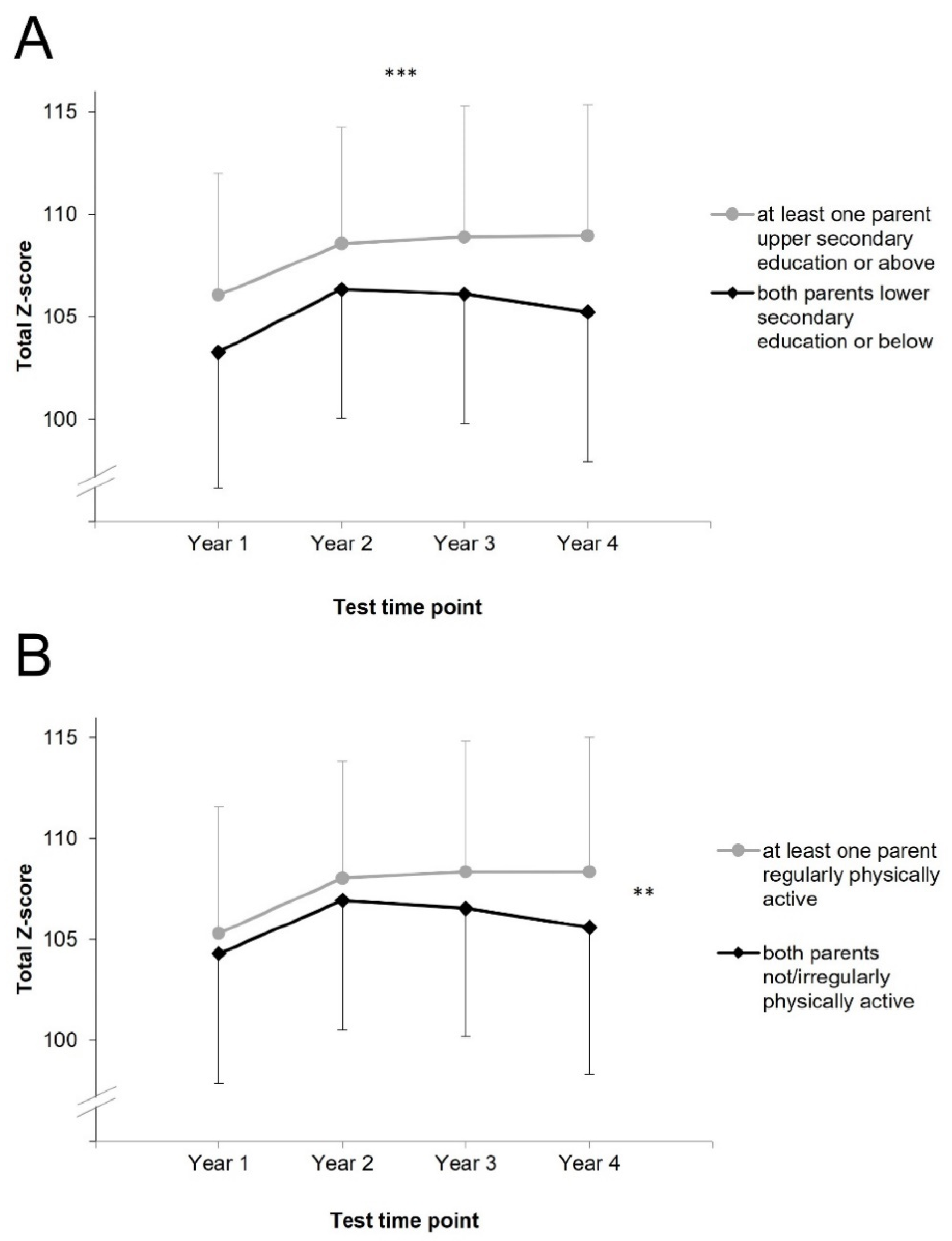
4.1. Parental Education and Children’s Physical Fitness
4.2. Parental Physical Activity and Children’s Physical Fitness
4.3. Comparison of the Statistical Models
4.4. Children’s Physical Fitness and Additional Associating Factors
5. Limitations and Strengths
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Blair, S.N. Physical inactivity: The biggest public health problem of the 21st century. Br. J. Sports Med. 2008, 43, 1–2. [Google Scholar]
- Moore, S.A.; Faulkner, G.; Rhodes, R.E.; Brussoni, M.; Chulak-Bozzer, T.; Ferguson, L.J.; Mitra, R.; O’Reilly, N.; Spence, J.C.; Vanderloo, L.M.; et al. Impact of the Covid-19 virus outbreak on movement and play behaviours of Canadian children and youth: A national survey. Int. J. Behav. Nutr. Phys. Act. 2020, 17, 85. [Google Scholar] [CrossRef] [PubMed]
- Graf, C.; Koch, B.; Kretschmann-Kandel, E.; Falkowski, G.; Christ, H.; Coburger, S.; Lehmacher, W.; Bjarnson-Wehrens, B.; Platen, P.; Tokarski, W.; et al. Correlation between BMI, leisure habits and motor abilities in childhood (CHILT-Project). Int. J. Obes. 2004, 28, 22–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Woll, A.; Worth, A.; Mündermann, A.; Hölling, H.; Jekauc, D.; Bös, K. Age- and sex-dependent disparity in physical fitness between obese and normalweight children and adolescents. J. Sports Med. Phys. Fit. 2013, 53, 48–55. [Google Scholar]
- Daniels, S.R.; Arnett, D.K.; Eckel, R.H.; Gidding, S.S.; Hayman, L.L.; Kumaniyka, S.; Robinson, T.N.; Scott, B.J.; St Jeor, S.; Williams, C.L. Overweight in children and adolescents: Pathophysiology, consequences, prevention, and treatment. Circulation 2005, 111, 1999–2012. [Google Scholar] [CrossRef] [Green Version]
- Ng, M.; Fleming, T.; Robinson, M.; Thomson, B.; Graetz, N.; Margono, C.; Mullany, E.C.; Biryukov, S.; Abbafati, C.; Gakidou, E.; et al. Global, regional, and national prevalence of overweight and obesity in children and adults during 1980–2013: A systematic analysis for the Global Burden of Disease Study 2013. Lancet 2014, 384, 766–781. [Google Scholar] [CrossRef] [Green Version]
- Yao, C.A.; Rhodes, R.E. Parental correlates in child and adolescent physical activity: A meta-analysis. Int. J. Behav. Nutr. Phys. Act. 2015, 12, 10. [Google Scholar] [CrossRef] [Green Version]
- Xu, H.; Wen, L.M.; Rissel, C. Associations of parental influences with physical activity and screen time among young children: A systematic review. J. Obes. 2015, 2015, 546925. [Google Scholar] [CrossRef] [Green Version]
- Garriguet, D.; Colley, R.; Bushinik, T. Parent-child association in physical activity and sedentary behavior. Health Rep. 2017, 28, 3–11. [Google Scholar]
- Wilk, P.; Clark, A.F.; Maltby, A.; Tucker, P.; Gilliland, J.A. Exploring the effect of parental influence on children's physical activity: The mediating role of children's perceptions of parental support. Prev. Med. 2018, 106, 79–85. [Google Scholar] [CrossRef]
- Berge, J.M.; Meyer, C.; MacLehose, R.F.; Esienberg, M.E.; Neumark-Sztainer, D. Nonresident parental influence on adolescent weight and weight-related behaviors: Similar or different from resident parental influence? Int. J. Behav. Nutr. Phys. Act. 2014, 11, 131. [Google Scholar] [CrossRef] [Green Version]
- Sleddens, E.F.C.; Gubbels, J.S.; Kremers, S.P.J.; van der Plas, E.; Thijs, C. Bidirectional associations between activity-related parenting practices, and child physical activity, sedentary screen-based behavior and body mass index: A longitudinal analysis. Int. J. Behav. Nutr. Phys. Act. 2017, 14, 89. [Google Scholar] [CrossRef] [Green Version]
- Furthner, D.; Ehrenmüller, M.; Biebl, A.; Lanzersdorfer, R.; Halmerbauer, G.; Auer-Hackenberg, L.; Schmitt, K. Gender differences and the role of parental education, school types and migration on the body mass index of 2930 Austrian school children: A cross-sectional study. Wien. Klin. Wochenschr. 2017, 129, 786–792. [Google Scholar] [CrossRef]
- Bushnik, T.; Garriguet, D.; Colley, R. Parent-Child association in body weight status. Health Rep. 2017, 28, 12–19. [Google Scholar] [PubMed]
- Buttitta, M.; Iliescu, C.; Rousseau, A.; Guerrien, A. Quality of life in overweight and obese children and adolescents: A literature review. Qual. Life Res. 2014, 23, 1117–1139. [Google Scholar] [CrossRef] [PubMed]
- Jia, H.; Lubetkin, E.I. The impact of obesity on health-related quality-of-life in the general adult US population. J. Public Health 2005, 27, 156–164. [Google Scholar] [CrossRef] [Green Version]
- Olshansky, S.J.; Passaro, D.J.; Hershow, R.C.; Layden, J.; Carnes, B.A.; Brody, J.; Hayflick, L.; Butler, R.N.; Allison, D.B.; Ludwig, D. A potential decline in life expectancy in the United States in the 21st century. N. Engl. J. Med. 2005, 352, 1138–1145. [Google Scholar] [CrossRef] [Green Version]
- Dietz, W. Health consequences of obesity in youth: Childhood predictors of adult disease. Pedeatrics 1998, 101, 518–525. [Google Scholar]
- Ruiz, J.R.; Castro-Pinero, J.; Artero, E.G.; Ortega, F.B.; Sjöström, M.; Suni, J.; Castillo, M.J. Predictive validity of health-related fitness in youth: A systematic review. Br. J. Sports Med. 2009, 43, 909–923. [Google Scholar] [CrossRef]
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J. Physical activity, physical fitness, and overweight in children and adolescents: Evidence from epidemiologic studies. Endocrinol. Nutr. 2013, 60, 458–469. [Google Scholar] [CrossRef]
- Smith, J.J.; Eather, N.; Morgan, P.J.; Plotnikoff, R.C.; Faigenbaum, A.D.; Lubans, D.R. The health benefits of muscular fitness for children and adolescents: A systematic review and meta-analysis. Sports Med. 2014, 44, 1209–1223. [Google Scholar] [CrossRef] [PubMed]
- Caspersen, C.J.; Powell, K.E.; Christenson, G.M. Physical activity, exercise, and physical fitness: Definitions and distinctions for health-related research. Public Health Rep. 1985, 100, 126–131. [Google Scholar] [PubMed]
- Utesch, T.; Dreiskamper, D.; Strauss, B.; Naul, R. The development of the physical fitness construct across childhood. Scand. J. Med. Sci. Sports 2018, 28, 212–219. [Google Scholar] [CrossRef]
- Ortega, F.B.; Labayen, I.; Ruiz, J.R.; Kurvinen, E.; Loit, H.; Harro, J.; Veidebaum, T.; Sjöström, M. Improvements in fitness reduce the risk of becoming overweight across puberty. Med. Sci. Sports Exerc. 2011, 43, 1891–1897. [Google Scholar] [CrossRef] [PubMed]
- García-Hermoso, A.; Ramírez-Campillo, R.; Izquierdo, M. Is muscular fitness associated with future health benefits in children and adolescents? A systematic review and meta-analysis of longitudinal studies. Sports Med. 2019, 49, 1079–1094. [Google Scholar] [CrossRef]
- Ortega, F.B.; Ruiz, J.R.; Castillo, M.J.; Sjöström, M. Physical fitness in childhood and adolescence: A powerful marker of health. Int. J. Obes. (Lond.) 2008, 32, 1–11. [Google Scholar] [CrossRef] [Green Version]
- Lämmle, L.; Worth, A.; Bös, K. Socio-demographic correlates of physical activity and physical fitness in German children and adolescents. Eur. J. Public Health 2012, 22, 880–884. [Google Scholar] [CrossRef] [Green Version]
- Merino-De Haro, I.; Mora-Gonzalez, J.; Cadenas-Sanchez, C.; Vorras, P.A.; Benito, P.J.; Chiva-Bartoll, O.; Torrijos-Niño, C.; Samaniego-Sánchez, C.; Quesada-Granados, J.J.; Sánchez-Delgado, A.; et al. Higher socioeconomic status is related to healthier levels of fatness and fitness already at 3 to 5 years of age: The PREFIT project. J. Sports Sci. 2018, 27, 1–11. [Google Scholar] [CrossRef]
- Lovecchio, N.; Novak, D.; Eid, L.; Casolo, F.; Podnar, H. Urban and rural fitness level: Comparison between Italian and Croatian students. Percept. Mot. Skills 2015, 120, 367–380. [Google Scholar] [CrossRef]
- Klein, M.; Frölich, M.; Pieter, A.; Emrich, E. Socio-economic status and motor performance of children and adolescents. Eur. J. Sport Sci. 2016, 6, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Ruedl, G.; Ewald, P.; Niedermeier, M.; Kirschner, W.; Kopp, M.; Drenowatz, C.; Greier, K. Long-term effect of migration background on the development of physical fitness among primary school children. Scand. J. Med. Sci. Sports 2019, 29, 124–131. [Google Scholar] [CrossRef] [PubMed]
- Bringolf-Isler, B.; Schindler, C.; Kayser, B.; Suggs, L.S.; Probst-Hensch, N.; SOPHYA Study Group. Objectively measured physical activity in population-representative parent-child pairs: Parental modelling matters and is context-specific. BMC Public Health 2018, 18, 1024. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, D.; Padez, C.; Machado-Rodrigues, A.M. Active parents, active children: The importance of parental organized physical activity in children’s extracurricular sport participation. J. Child. Health Care 2018, 22, 159–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bös, K.; Schlenker, L.; Büsch, D.; Lämmle, L.; Müller, H.; Oberger, J.; Seidel, I.; Tittlbach, S. Deutscher Motorik Test. 6–18 (DMT 6–18) [German Motor Performance Test 6–18 (DMT 6-18)]; Czwalina: Hamburg, Germany, 2009. [Google Scholar]
- UNESCO Institute for Statistics. International Standard Classification of Education (ISCED) 2011; UNESCO Institute for Statistics: Montreal, QC, Canada, 2012; Available online: http://uis.unesco.org/sites/default/files/documents/international-standard-classification-of-education-isced-2011-en.pdf (accessed on 14 July 2021).
- Field, A. Discovering Statistics Using IBM SPSS Statistics; SAGE Publications: London, UK, 2013. [Google Scholar]
- Zaqout, M.; Vyncke, K.; Moreno, L.A.; De Miguel-Etayo, P.; Lauria, F.; Molnar, D.; Lissner, L.; Hunsberger, M.; Veidebaum, T.; Tornaritis, M.; et al. Determinant factors of physical fitness in European children. Int. J. Public Health 2016, 61, 573–582. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vermeiren, A.P.; Willeboordse, M.; Oosterhoff, M.; Bartelink, N.; Muris, P.; Bosma, H. Socioeconomic multi-domain health inequalities in Dutch primary school children. Eur. J. Public Health 2018, 28, 610–616. [Google Scholar] [CrossRef]
- Kaseva, K.; Hintsa, T.; Lipsanen, J.; Pulkki-Råback, L.; Hintsanen, M.; Yang, X.; Hirvensalo, M.; Hutri-Kähönen, N.; Raitakari, O.; Keltikangas-Järvinen, L.; et al. Parental physical activity associates with offspring's physical activity until middle age: A 30-year study. J. Phys. Act. Health 2017, 14, 520–531. [Google Scholar] [CrossRef]
- Kriemler, S.; Zahner, L.; Schindler, C.; Meyer, U.; Hartmann, T.; Hebestreit, H.; Brunner-La Rocca, H.P.; van Mechelen, W.; Puder, J.J. Effect of school based physical activity programme (KISS) on fitness and adiposity in primary schoolchildren: Cluster randomised controlled trial. BMJ 2010, 340, c785. [Google Scholar] [CrossRef] [Green Version]
- Lovecchio, N.; Zago, M. Fitness differences according to BMI categories: A new point of view. J. Sports Med. Phys. Fit. 2019, 59, 298–303. [Google Scholar] [CrossRef] [PubMed]
- Ruedl, G.; Franz, D.; Frühauf, A.; Kopp, M.; Niedermeier, M.; Drenowatz, C.; Greier, K. Development of physical fitness among overweight and non-overweight Austrian primary school children: A longitudinal study over 2.5 years. Wien. Klin. Wochenschr. 2018, 130, 321–327. [Google Scholar] [CrossRef] [Green Version]
- Pereira, S.; Bustamante, A.; Santos, C.; Hedeker, D.; Tani, G.; Garganta, R.; Vasconcelos, O.; Baxter-Jones, A.; Katzmarzyk, P.T.; Maia, J. Biological and environmental influences on motor coordination in Peruvian children and adolscents. Sci. Rep. 2021, 11, 15444. [Google Scholar] [CrossRef]
- Craig, C.L.; Marshall, A.L.; Sjostrom, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Oja, P.; et al. International physical activity questionnaire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cocca, A.; Espino, F.; Rodenas, L.; Cocca, M. Effect of a game-based Physical Education program on physical fitness and mental health in elementary school children. Int. J. Environ. Res. Public Health 2020, 17, 4883. [Google Scholar] [CrossRef] [PubMed]
- Cocca, A.; Carbajal-Baca, J.E.; Hernandez Cruz, G.; Cocca, M. Does a Multiple-Sport Intervention based on the TGfU pedagogical model for Physical Education increase physical fitness in primary school children? Int. J. Environ. Res. Public Health 2020, 17, 5532. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Subtest | Time Point | |||||||
|---|---|---|---|---|---|---|---|---|
| Year 1 | Year 2 | Year 3 | Year 4 | |||||
| 20-m sprint [s] | 4.6 | (0.5) | 4.3 | (0.4) | 4.1 | (0.4) | 4.0 | (0.3) |
| Balancing backwards [n steps] | 29 | (10) | 34 | (9) | 38 | (8) | 39 | (8) |
| Jumping sideways [n jumps] | 25 | (6) | 33 | (6) | 37 | (6) | 40 | (7) |
| Stand-and-reach [cm] | 1.0 | (6.7) | 0.8 | (6.7) | 0.4 | (7.2) | 0.8 | (7.9) |
| Push-ups [n] | 13 | (4) | 17 | (3) | 17 | (4) | 18 | (5) |
| Sit ups [n] | 16 | (5) | 20 | (6) | 22 | (6) | 24 | (6) |
| Standing long jump [cm] | 119 | (18) | 124 | (20) | 137 | (20) | 143 | (23) |
| 6-min run [m] | 824 | (247) | 876 | (157) | 919 | (171) | 966 | (190) |
| Missing cases | 64–66 | 49 | 36 | 24 | ||||
| ANOVA | ANCOVA | Multilevel Modelling | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| p | Partial η² | p | Partial η² | p | B | SE B | 95% CI lb | 95% CI ub | ||||
| PEd | <0.001 | *** | 0.06 | 0.001 | ** | 0.04 | 0.040 | * | 1.75 | 0.67 | 0.42 | 3.07 |
| PPh | 0.326 | 0.00 | 0.677 | 0.00 | 0.288 | 1.33 | 0.70 | −0.05 | 2.71 | |||
| PET | 0.231 | 0.01 | 0.261 | 0.01 | 0.269 | 0.31–0.95 | 0.54–0.55 | |||||
| PPT | 0.003 | ** | 0.02 | 0.004 | ** | 0.02 | 0.122 | 0.37–1.16 | 0.58–0.59 | |||
| Time | <0.001 | *** | 0.13 | 0.007 | ** | 0.02 | <0.001 | *** | 0.01–3.80 | 0.35–0.37 | ||
| WS | <0.001 | *** | 0.10 | <0.001 | *** | 3.73 | 0.48 | 2.80 | 4.66 | |||
| MBg | <0.001 | *** | 0.05 | <0.001 | *** | −3.14 | 0.63 | −4.38 | −1.90 | |||
| Time Point | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variable | Year 1 | Year 2 | Year 3 | Year 4 | MC | p | ||||||
| OW, % (n) | 1+ parent USE | 10.3% | (19) | 12.7% | (25) | 12.8% | (26) | 13.3% | (28) | 29–69 | <0.010 | ** |
| 2 parents LSE | 21.2% | (25) | 24.2% | (29) | 26.8% | (34) | 30.3% | (40) | ||||
| MBg, % (n) | 1+ parent USE | 20.6% | (46) | 7 | <0.001 | *** | ||||||
| 2 parents LSE | 46.8% | (66) | ||||||||||
| OW, % (n) | 1+ parent RPA | 11.5% | (30) | 14.6% | (38) | 16.9% | (44) | 16.9% | (44) | 24–64 | 0.285 < p < 0.763 | |
| 2 parents NPA | 12.6% | (14) | 14.4% | (16) | 14.4% | (16) | 21.6% | (24) | ||||
| MBg, % (n) | 1+ parent RPA | 24.6% | (64) | 2 | < 0.001 | *** | ||||||
| 2 parents NPA | 44.1% | (49) | ||||||||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ruedl, G.; Niedermeier, M.; Wimmer, L.; Ploner, V.; Pocecco, E.; Cocca, A.; Greier, K. Impact of Parental Education and Physical Activity on the Long-Term Development of the Physical Fitness of Primary School Children: An Observational Study. Int. J. Environ. Res. Public Health 2021, 18, 8736. https://doi.org/10.3390/ijerph18168736
Ruedl G, Niedermeier M, Wimmer L, Ploner V, Pocecco E, Cocca A, Greier K. Impact of Parental Education and Physical Activity on the Long-Term Development of the Physical Fitness of Primary School Children: An Observational Study. International Journal of Environmental Research and Public Health. 2021; 18(16):8736. https://doi.org/10.3390/ijerph18168736
Chicago/Turabian StyleRuedl, Gerhard, Martin Niedermeier, Lukas Wimmer, Vivien Ploner, Elena Pocecco, Armando Cocca, and Klaus Greier. 2021. "Impact of Parental Education and Physical Activity on the Long-Term Development of the Physical Fitness of Primary School Children: An Observational Study" International Journal of Environmental Research and Public Health 18, no. 16: 8736. https://doi.org/10.3390/ijerph18168736
APA StyleRuedl, G., Niedermeier, M., Wimmer, L., Ploner, V., Pocecco, E., Cocca, A., & Greier, K. (2021). Impact of Parental Education and Physical Activity on the Long-Term Development of the Physical Fitness of Primary School Children: An Observational Study. International Journal of Environmental Research and Public Health, 18(16), 8736. https://doi.org/10.3390/ijerph18168736