
Evaluating a Psychoeducation Program to Foster Chinese Primary School Students’ Covitality

Abstract
:1. Introduction
1.1. Positive Psychoeducation Approaches
1.2. Covitality Model
1.3. Effectiveness of Covitality Intervention Programs
1.4. Culturally Relevant Covitality Fostering Psychoeducation Program
- Consciousness raising: finding and learning new facts, ideas, and tips that support the healthy behavior change.
- Dramatic relief: experiencing the negative emotions (fear, anxiety, worry) that go along with unhealthy behavioral risks.
- Self-reevaluation: realizing that the behavior change is an important part of one’s identity as a person.
- Environmental reevaluation: realizing the negative impact of the unhealthy behavior or the positive impact of the healthy behavior on one’s proximal social and/or physical environment.
- Self-liberation: making a firm commitment to change.
- Helping relationships: seeking and using social support for the healthy behavior change.
- Counterconditioning: substitution of healthier alternative behaviors and cognitions for the unhealthy behavior.
- Contingency management: increasing the rewards for the positive behavior change and decreasing the rewards of the unhealthy behavior.
- Stimulus control: removing reminders or cues to engage in the unhealthy behavior and adding cues or reminders to engage in the healthy behavior.
- Social liberation: realizing that the social norms are changing in the direction of supporting the healthy behavior change.
2. Materials and Methods
2.1. Study Purpose
2.2. Ethical Concerns
2.3. GPI Rationale and Development
2.4. Participants
2.5. Measures
Quantitative Measures
2.6. Procedures
2.7. Statistical Analysis
3. Results
3.1. Pretest Differences
3.2. Covitality Comparisons
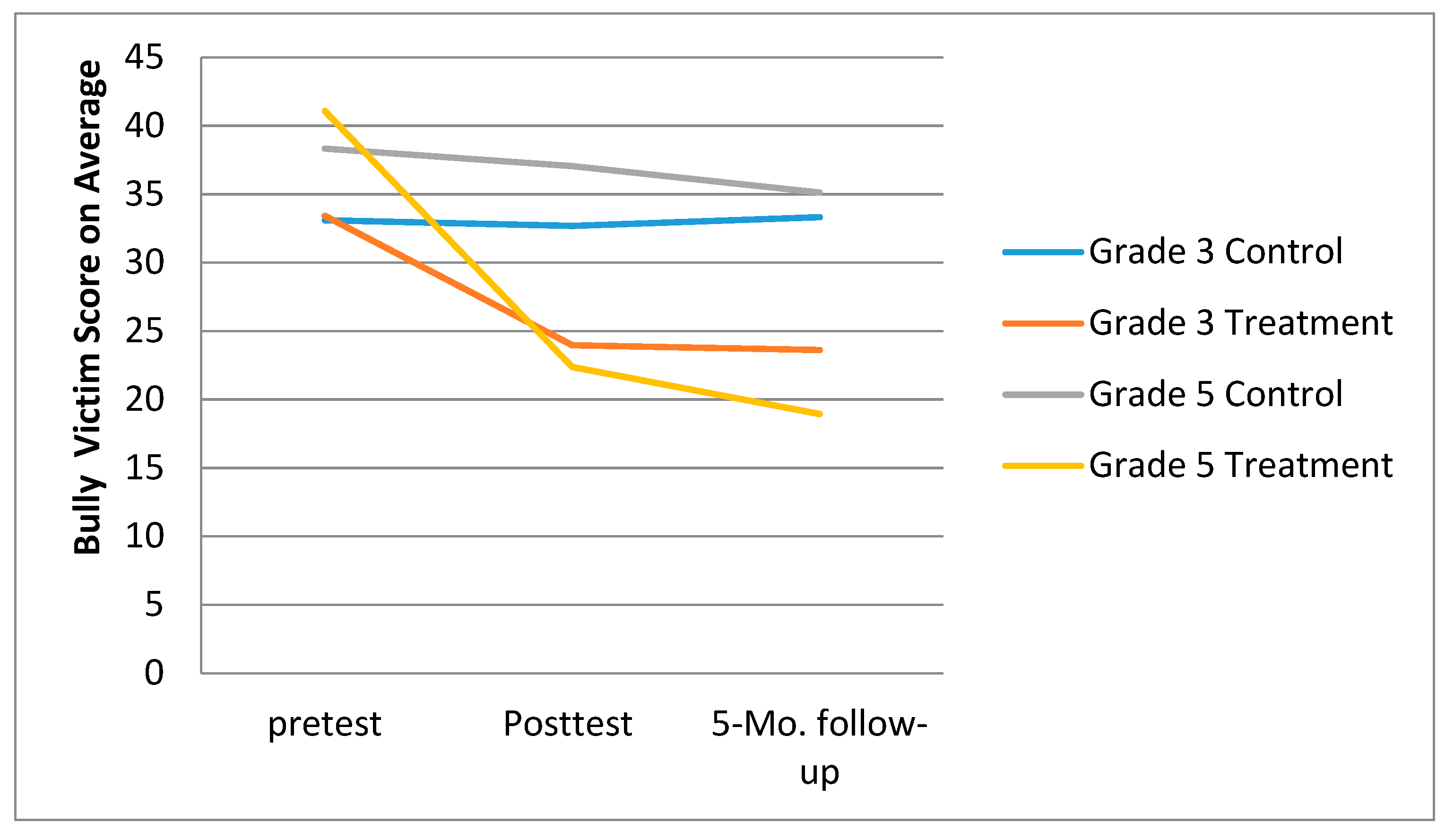
3.3. Bullying Victimization Comparisons
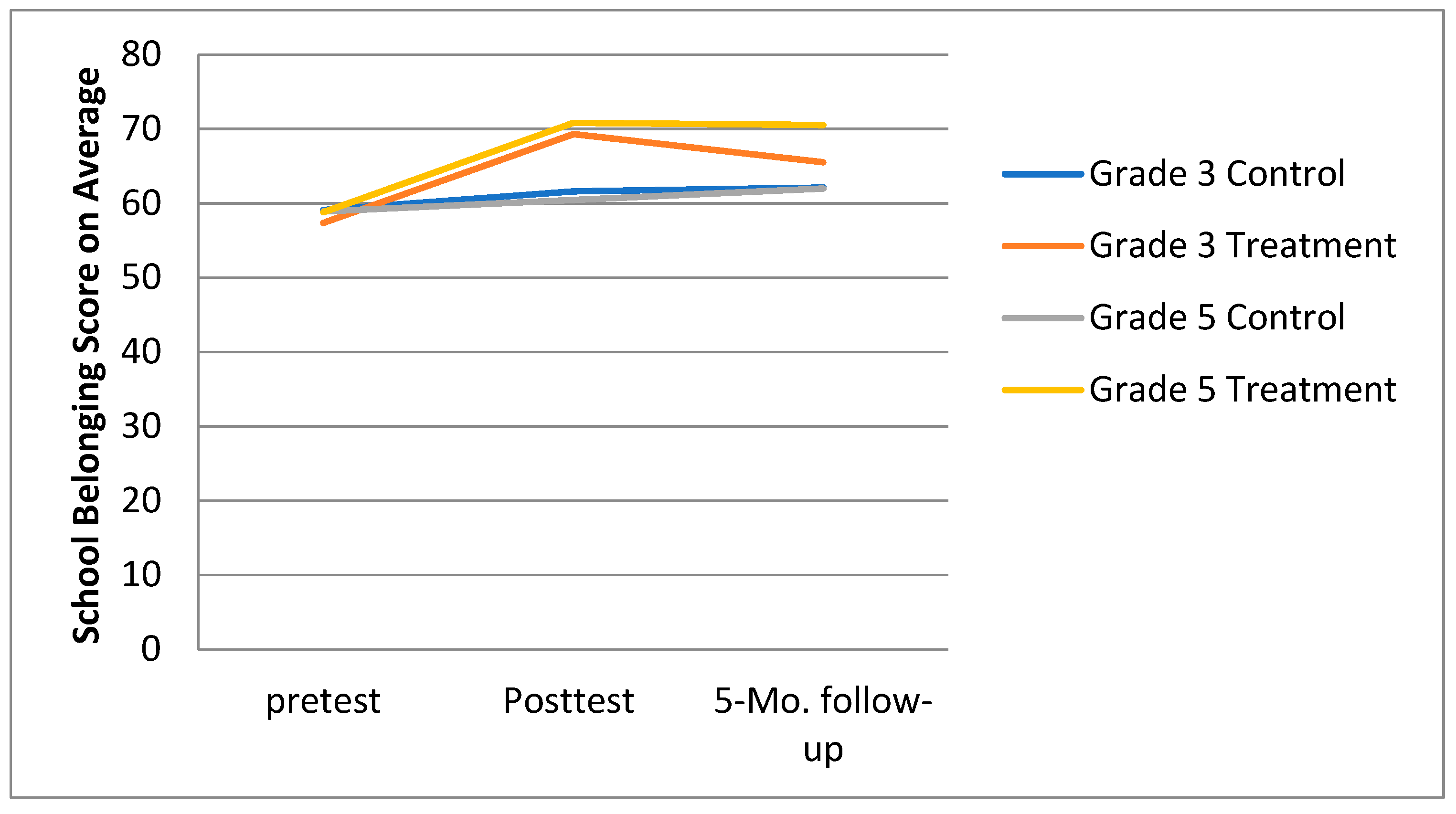
3.4. School Belonging Comparisons
4. Discussion
5. Practical Implications
6. Limitations
7. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Ge, M.-G.; Zhang, H.-L. Relationship Among the Parental Rearing Behaviors and Personality and Social Anxiety of Pupils. Chin. Prim. Health Care 2007, 21, 33–34. [Google Scholar]
- Wang, C.; Yang, C.; Jiang, X.; Furlong, M. Validation of the Chinese version of the Social Emotional Health Survey–Primary. Int. J. Sch. Educ. Psychol. 2016, 6, 62–74. [Google Scholar] [CrossRef]
- Ginsburg, G.S.; Drake, K.L.; Tein, J.-Y.; Teetsel, R.; Riddle, M.A. Preventing Onset of Anxiety Disorders in Offspring of Anxious Parents: A Randomized Controlled Trial of a Family-Based Intervention. Am. J. Psychiatry 2015, 172, 1207–1214. [Google Scholar] [CrossRef]
- Li, Y. The Co-occurring Patterns of Bullying/victimization Behaviors in Adolescents. Chin. J. Clin. Psychol. 2021, 3, 489–495. [Google Scholar] [CrossRef]
- Xie, J.; Yang, C.; Bear, G.G.; Lu, X. A Comparative Study of Bullying Victimization in Chinese and American Adolescents. Chin. J. Clin. Psychol. 2016, 24, 706–709. [Google Scholar] [CrossRef]
- Zheng, Y.; Zheng, X. Current state and recent developments of child psychiatry in China. Child Adolesc. Psychiatry Ment. Health 2015, 9, 10. [Google Scholar] [CrossRef] [Green Version]
- Bai, H.; Rong, Z. The Intervention Effect of Group Counseling on Coping Style of College Students being Lovelorn. China J. Health Psychol. 2014, 12, 763–773. [Google Scholar]
- Larkin, R.; Thyer, B.A. Evaluating cognitive-behavioral group counseling to improve elementary school students′ self-esteem, self-control, and classroom behavior. Behav. Interv. 1999, 14, 147–161. [Google Scholar] [CrossRef]
- Wang, Y.W. Harmonious Personality Development of Teenagers Based on Group Counseling. J. Chongqing Jiaotong Univ. 2012, 12, 3–5. [Google Scholar]
- Kim, Y.S. The Effect of a Group Counseling Program on Depression and Suicidal Prevention in High School Students. J. Korean Acad. Community Health Nurs. 2009, 20, 343–350. [Google Scholar]
- Froh, J.J.; Sefick, W.J.; Emmons, R.A. Counting blessings in early adolescents: An experimental study of gratitude and subjective well-being. J. Sch. Psychol. 2008, 46, 213–233. [Google Scholar] [CrossRef]
- Boman, P.; Furlong, M.J.; Shochet, I.; Lilles, E.; Jones, C. Optimism and the school context. Handb. Posit. Psychol. Sch. 2009, 69–82. [Google Scholar] [CrossRef]
- Brown Kirschman, K.J.; Johnson, R.J.; Bender, J.A.; Roberts, M.C. Positive Psychology for Children and Adolescents: Development, Prevention, and Promotion. In The Oxford Handbook of Positive Psychology, 2nd ed.; Oxford University Press: Oxford, UK, 2012; pp. 133–148. ISBN 9780199940615. [Google Scholar]
- Ostaszewski, K.; Zimmerman, M.A. The Effects of Cumulative Risks and Promotive Factors on Urban Adolescent Alcohol and Other Drug Use: A Longitudinal Study of Resiliency. Am. J. Community Psychol. 2006, 38, 251–262. [Google Scholar] [CrossRef] [Green Version]
- Huebner, E.S.; Gilman, R. Toward a focus on positive psychology in school psychology. Sch. Psychol. Q. 2003, 18, 99–102. [Google Scholar] [CrossRef]
- Suldo, S.M.; Shaffer, E.J. Looking Beyond Psychopathology: The Dual-Factor Model of Mental Health in Youth. Sch. Psychol. Rev. 2008, 37, 52–68. [Google Scholar] [CrossRef]
- Shernoff, D.J.; Csikszentmihalyi, M. Flow in schools: Cultivating engaged learners and optimal learning environments. In Handbook of Positive Psychology in Schools; Routledge: London, UK, 2009; pp. 131–145. ISBN 0203884086. [Google Scholar]
- Furlong, M.J.; You, S.; Renshaw, T.L.; O’Malley, M.D.; Rebelez, J. Preliminary Development of the Positive Experiences at School Scale for Elementary School Children. Child Indic. Res. 2013, 6, 753–775. [Google Scholar] [CrossRef]
- Nie, Q.; Yang, C.; Teng, Z.; Furlong, M.J.; Pan, Y.; Guo, C.; Zhang, D. Longitudinal association between school climate and depressive symptoms. Sch. Psychol. 2020, 35, 267–276. [Google Scholar] [CrossRef] [PubMed]
- Furlong, M.J.; Dowdy, E.; Nylund-Gibson, K.; Wagle, R.; Carter, D.; Hinton, T. Enhancement and Standardization of a Universal Social-Emotional Health Measure for Students’ Psychological Strengths. J. Well-Being Assess. 2021, 1–23. [Google Scholar] [CrossRef]
- Moore, S.A.; Dowdy, E.; Nylund-Gibson, K.; Furlong, M.J. A latent transition analysis of the longitudinal stability of dual-factor mental health in adolescence. J. Sch. Psychol. 2019, 73, 56–73. [Google Scholar] [CrossRef] [PubMed]
- Moore, S.A.; Dowdy, E.; Nylund-Gibson, K.; Furlong, M.J. An Empirical Approach to Complete Mental Health Classification in Adolescents. Sch. Ment. Health 2019, 11, 438–453. [Google Scholar] [CrossRef]
- Seligman, M.E.P.; Reivich, K.; Gillham, J. The Optimistic Child: A Proven Program to Safeguard Children Against Depression and Build Lifelong Resilience; Houghton Mifflin: Boston, MA, USA, 2007. [Google Scholar]
- Cloninger, C.R. Character Strengths and Virtues: A Handbook and Classification. Am. J. Psychiatry 2005, 162, 820–821. [Google Scholar] [CrossRef]
- Park, N.; Peterson, C. Moral competence and character strengths among adolescents: The development and validation of the Values in Action Inventory of Strengths for Youth. J. Adolesc. 2006, 29, 891–909. [Google Scholar] [CrossRef]
- Weber, M.; Ruch, W. The role of character strengths in adolescent romantic relationships: An initial study on partner selection and mates’ life satisfaction. J. Adolesc. 2012, 35, 1537–1546. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Duckworth, A. Grit: The Power of Passion & Perseverance; Scribner: New York, NY, USA, 2013. [Google Scholar]
- Duckworth, A.L.; Peterson, C.; Matthews, M.D.; Kelly, D.R. Grit: Perseverance and passion for long-term goals. J. Pers. Soc. Psychol. 2007, 92, 1087–1101. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.K.; Choe, D. Universal Social, Emotional, and Behavioral Strength and Risk Screening: Relative Predictive Validity for Students’ Subjective Well-Being in Schools. Sch. Psychol. Rev. 2021, 1–15. [Google Scholar] [CrossRef]
- Furlong, M.J.; You, S.; Renshaw, T.; Smith, D.C.; O’Malley, M.D. Preliminary Development and Validation of the Social and Emotional Health Survey for Secondary School Students. Soc. Indic. Res. 2013, 117, 1011–1032. [Google Scholar] [CrossRef]
- You, S. Validation of the social and emotional health survey for five sociocultural groups: Multigroup invariance and latent mean analyses. J. Adolesc. 2014, 74, 274–283. [Google Scholar] [CrossRef]
- Xie, J.; Liu, S.; Yang, C.; Furlong, M.J.; Wang, C. Validation of the Social and Emotional Health Survey-Primary for Chinese Students. Chin. J. Clin. Psychol. 2018, 26, 522–527. [Google Scholar] [CrossRef]
- Naples, L.; Tuckwiller, E. Taking Students on a Strengths Safari: A Multidimensional Pilot Study of School-Based Wellbeing for Young Neurodiverse Children. Int. J. Environ. Res. Public Health 2021, 18, 6947. [Google Scholar] [CrossRef]
- Naples, L.H. Neurodivergence in Early Childhood: Deriving a Dual-Factor Model of Educational Well-Being through a Design-Based Research Pilot Program. Ph.D. Thesis, The George Washington University, Washington, DC, USA, 2019. [Google Scholar]
- Martínez-Martínez, A.; Pineda, D.; Galán, M.; Marzo, J.; Piqueras, J. Effects of the Action for Neutralization of Bullying Program on Bullying in Spanish Schoolchildren. Int. J. Environ. Res. Public Health 2021, 18, 6898. [Google Scholar] [CrossRef]
- Prochaska, J.O.; Redding, C.A.; Evers, K.E. The transtheoretical model and stages of change. Med. Sci. Sport. Exerc. 1991, 23, 1404. [Google Scholar] [CrossRef]
- Yang, T. A strategy for clinical intervention: Introduction to the theory of staged behavioral change. Chin. J. Behav. Med. Sci. 2002, 11, 352–353. [Google Scholar]
- Sameroff, A. A Unified Theory of Development: A Dialectic Integration of Nature and Nurture. Child Dev. 2010, 81, 6–22. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bronfenbrenner, K. The ecology of human development. Work. Occup. 1995, 22, 234–235. [Google Scholar] [CrossRef]
- Li, J.; Pan, Y.; Wang, Z. Research on stages of change model in health behaviors. J. Health Soc. Behav. 2011, 38, 4914–4916. [Google Scholar]
- Froh, J.J.; Fan, J.; Emmons, R.A.; Bono, G.; Huebner, E.S.; Watkins, P. Measuring gratitude in youth: Assessing the psychometric properties of adult gratitude scales in children and adolescents. Psychol. Assess. 2011, 23, 311–324. [Google Scholar] [CrossRef] [Green Version]
- Gillham, J.; Reivich, K. Cultivating Optimism in Childhood and Adolescence. Ann. Am. Acad. Political Soc. Sci. 2004, 591, 146–163. [Google Scholar] [CrossRef]
- Park, N.; Peterson, C.; Seligman, M.E.P. Character strengths in fifty-four nations and the fifty US states. J. Posit. Psychol. 2006, 1, 118–129. [Google Scholar] [CrossRef]
- Iida, J.; Ito, A.; Aoyama, I.; Sugimoto, K.; Endo, H.; Chan, M.; Furlong, M.J. Validation of a social emotional wellness survey among Japanese elementary school students. Educ. Dev. Psychol. 2021, 38, 1–10. [Google Scholar] [CrossRef]
- Wagle, R.; Dowdy, E.; Yang, C.; Palikara, O.; Castro, S.; Nylund-Gibson, K.; Furlong, M.J. Preliminary investigation of the psychological sense of school membership scale with primary school students in a cross-cultural context. Sch. Psychol. Int. 2018, 39, 568–586. [Google Scholar] [CrossRef] [Green Version]
- Xie, J.; Yang, C.; Bear, G.G.; Marshall, S.J. Reliability and Validity of the Chinese Version of Delaware Bullying Victimization Scale-student Hunan. Chin. J. Clin. Psychol. 2015, 23, 594–596. [Google Scholar] [CrossRef]
- Xie, J.; Wei, Y.; Bear, G.G. Revision of Chinese Version of Delaware Bullying Victimization Scale-student in Adolescents. Chin. J. Clin. Psychol. 2018, 26, 259–263. [Google Scholar] [CrossRef]
- Pan, F.-D.; Wang, Q.; Song, L.-L.; Dai, J.-J. A Research on Reliability and Validity of Psychological Sense of School Membership Scale. Chin. J. Clin. Psychol. 2011, 19, 2010–2012. [Google Scholar] [CrossRef]
- Ito, A.; Smith, D.C.; You, S.; Shimoda, Y.; Furlong, M.J. Validation and Utility of the Social Emotional Health Survey—Secondary for Japanese Students. Contemp. Sch. Psychol. 2015, 19, 243–252. [Google Scholar] [CrossRef]
- Lee, S.-Y.; You, S.; Furlong, M.J. Validation of the Social Emotional Health Survey–Secondary for Korean Students. Child Indic. Res. 2015, 9, 73–92. [Google Scholar] [CrossRef]
- Wood, A.M.; Maltby, J.; Gillett, R.; Linley, P.A.; Joseph, S. The role of gratitude in the development of social support, stress, and depression: Two longitudinal studies. J. Res. Pers. 2008, 42, 854–871. [Google Scholar] [CrossRef]
- Frydenberg, E.; Martin, A.J.; Collie, R.J. Social and Emotional Learning in Australia and The Asia-Pacific: Perspectives, Pro-Grams and Approaches. Social and Emotional Learning in the Australasian Context; Springer: Melbourne, Australia, 2017; pp. 1–471. ISBN 9789811033940. [Google Scholar]
- Rose, C.; Espelage, D.L.; Monda-Amaya, L.E.; Shogren, K.A.; Aragon, S.R. Bullying and Middle School Students with and Without Specific Learning Disabilities: An Examination of Social-Ecological Predictors. J. Learn. Disabil. 2013, 48, 239–254. [Google Scholar] [CrossRef]
- Zhang, B. Work on The Whole People. Theor. Appl. Genet. 2010, 7, 1–7. [Google Scholar]
- Wang, Y. Promote the insituationalization and standardization of military training for students. China Educ. Dly. 2007, 4, 1–10. [Google Scholar]
- Gang, S.W. Discuss on Mathematics Classroom Teaching Strategy under the Background of Quality Education. W. Success 2021, 18, 106–107. [Google Scholar]
- Huang, Z.W. Talking about information technology in physical education teaching the promoting effect of cultivating students’ perseverance. China New Telecommun. 2021, 6, 184–185. [Google Scholar]
- Lu, Y.C. Comparison of mental health between public and private primary school students in Leshan. Time Educ. 2010, 6, 103–104. [Google Scholar]
- Patalay, P.; O’Neill, E.; Deighton, J.; Fink, E. School characteristics and children’s mental health: A linked survey-administrative data study. Prev. Med. 2020, 141, 106292. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Sessions Topic | Session Content and Title |
|---|---|
| Strong Winds Blow The Rules and Principles |
| Love at the Fingertips 1 Gratitude Heart |
| You are Good at Playing Basketball! Guess Who He or She Is Reveal Your True Feelings I Admire You |
| Thousand-hand Kwan Yin Be an Optimistic Person Make Every Day Full of Joy |
| I See Create an Emotional Calendar 2 |
| Giving is the Best Return Through the Virgin Forest Our Road to Friendship It’s Good to Have You Around |
| Forrest Gump Difficult Event Table |
| Thousand Knots Daily Sniper 3 My Junzi is the Most Standard 4 |
| Pretest | Posttest | |||||||
|---|---|---|---|---|---|---|---|---|
| M | SD | M | SD | t | p | d | ||
| Gratitude | Gr 3 control | 22.02 | 5.59 | 22.22 | 5.16 | 0.19 | 0.849 | 0.04 |
| Gr 3 experimental | 21.89 | 5.26 | 25.39 | 4.11 | 3.07 | 0.004 | 0.67 | |
| Gr 5 control | 22.29 | 3.95 | 21.74 | 4.49 | 0.74 | 0.465 | 0.23 | |
| Gr 5 experimental | 22.02 | 4.40 | 25.80 | 4.17 | 2.69 | 0.010 | 0.63 | |
| Optimism | Gr 3 control | 21.00 | 5.26 | 20.20 | 4.86 | −0.73 | 0.471 | 0.15 |
| Gr 3 experimental | 19.03 | 5.37 | 24.51 | 4.21 | 4.79 | 0.000 | 1.02 | |
| Gr 5 control | 22.63 | 4.47 | 21.79 | 5.20 | 0.99 | 0.327 | 0.16 | |
| Gr 5 experimental | 21.95 | 4.73 | 24.90 | 4.27 | 3.47 | 0.001 | 0.62 | |
| Zest | Gr 3 control | 23.62 | 6.79 | 23.38 | 6.86 | −0.17 | 0.867 | 0.04 |
| Gr 3 exp | 23.31 | 5.87 | 28.23 | 5.28 | 3.54 | 0.001 | 0.84 | |
| Gr 5 control | 22.94 | 5.71 | 22.85 | 6.25 | 0.07 | 0.942 | 0.01 | |
| Gr 5 experimental | 24.65 | 5.81 | 27.62 | 6.54 | 2.07 | 0.045 | 0.51 | |
| Persistence | Gr 3 control | 24.16 | 5.38 | 23.40 | 5.60 | −0.68 | 0.498 | 0.14 |
| Gr 3 experimental | 22.97 | 4.74 | 27.57 | 3.24 | 4.92 | 0.001 | 0.97 | |
| Gr 5 control | 25.18 | 4.37 | 25.10 | 4.61 | 0.24 | 0.811 | 0.02 | |
| Gr 5 experimental | 24.50 | 4.58 | 26.42 | 4.82 | 1.82 | 0.076 | 0.42 | |
| Covitality | Gr 3 control | 90.80 | 19.42 | 89.20 | 19.65 | −0.39 | 0.699 | 0.08 |
| Gr 3 experimental | 87.08 | 14.62 | 105.50 | 13.26 | 5.47 | 0.001 | 1.26 | |
| Gr 5 control | 92.56 | 14.19 | 91.25 | 16.07 | 0.57 | 0.575 | 0.08 | |
| Gr 5 experimental | 93.77 | 15.95 | 104.92 | 17.30 | 2.95 | 0.005 | 0.70 | |
| Posttest | 5-Mo. Follow Up Test | |||||||
|---|---|---|---|---|---|---|---|---|
| Variable | Experimental Group | M | SD | M | SD | t | p | d |
| Gratitude | Grade 3 | 25.41 | 4.06 | 24.40 | 4.32 | −0.84 | 0.405 | 0.23 |
| Grade 5 | 25.97 | 4.08 | 24.46 | 6.20 | −1.71 | 0.096 | 0.37 | |
| Optimism | Grade 3 | 24.51 | 4.21 | 23.57 | 3.95 | −1.31 | 0.198 | 0.22 |
| Grade 5 | 24.77 | 4.25 | 23.66 | 5.51 | −1.24 | 0.222 | 0.26 | |
| Zest | Grade 3 | 28.23 | 5.28 | 27.05 | 5.36 | −1.63 | 0.111 | 0.22 |
| Grade 5 | 27.71 | 6.60 | 26.15 | 7.14 | −1.23 | 0.230 | 0.24 | |
| Persistence | Grade 3 | 27.49 | 3.30 | 26.24 | 3.66 | −1.91 | 0.064 | 0.34 |
| Grade 5 | 26.50 | 4.80 | 25.60 | 5.65 | −1.04 | 0.305 | 0.19 | |
| Covitality | Grade 3 | 105.64 | 12.81 | 101.26 | 13.43 | −1.87 | 0.069 | 0.33 |
| Grade 5 | 105.44 | 17.26 | 100.75 | 22.73 | −1.07 | 0.294 | 0.27 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Fang, M.; Zhang, L.; Pan, D.; Xie, J. Evaluating a Psychoeducation Program to Foster Chinese Primary School Students’ Covitality. Int. J. Environ. Res. Public Health 2021, 18, 8703. https://doi.org/10.3390/ijerph18168703
Fang M, Zhang L, Pan D, Xie J. Evaluating a Psychoeducation Program to Foster Chinese Primary School Students’ Covitality. International Journal of Environmental Research and Public Health. 2021; 18(16):8703. https://doi.org/10.3390/ijerph18168703
Chicago/Turabian StyleFang, Min, Li Zhang, Dachen Pan, and Jiashu Xie. 2021. "Evaluating a Psychoeducation Program to Foster Chinese Primary School Students’ Covitality" International Journal of Environmental Research and Public Health 18, no. 16: 8703. https://doi.org/10.3390/ijerph18168703
APA StyleFang, M., Zhang, L., Pan, D., & Xie, J. (2021). Evaluating a Psychoeducation Program to Foster Chinese Primary School Students’ Covitality. International Journal of Environmental Research and Public Health, 18(16), 8703. https://doi.org/10.3390/ijerph18168703