
Psychometric Validation of the Arabic Fear of Illness and Virus Evaluation

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Measures
2.1.1. Fear of Illness and Virus Evaluation (FIVE; Ehrenreich-May, Unpublished)
2.1.2. Fear of COVID-19 Scale (FCV-19S)
2.2. Translation
2.3. Statistical Analysis
3. Results
3.1. Sample Characteristics
3.2. Mean Sum Scores of FIVE Subscales
3.3. Reliability
3.4. Concurrent Validity
3.5. Face Validity
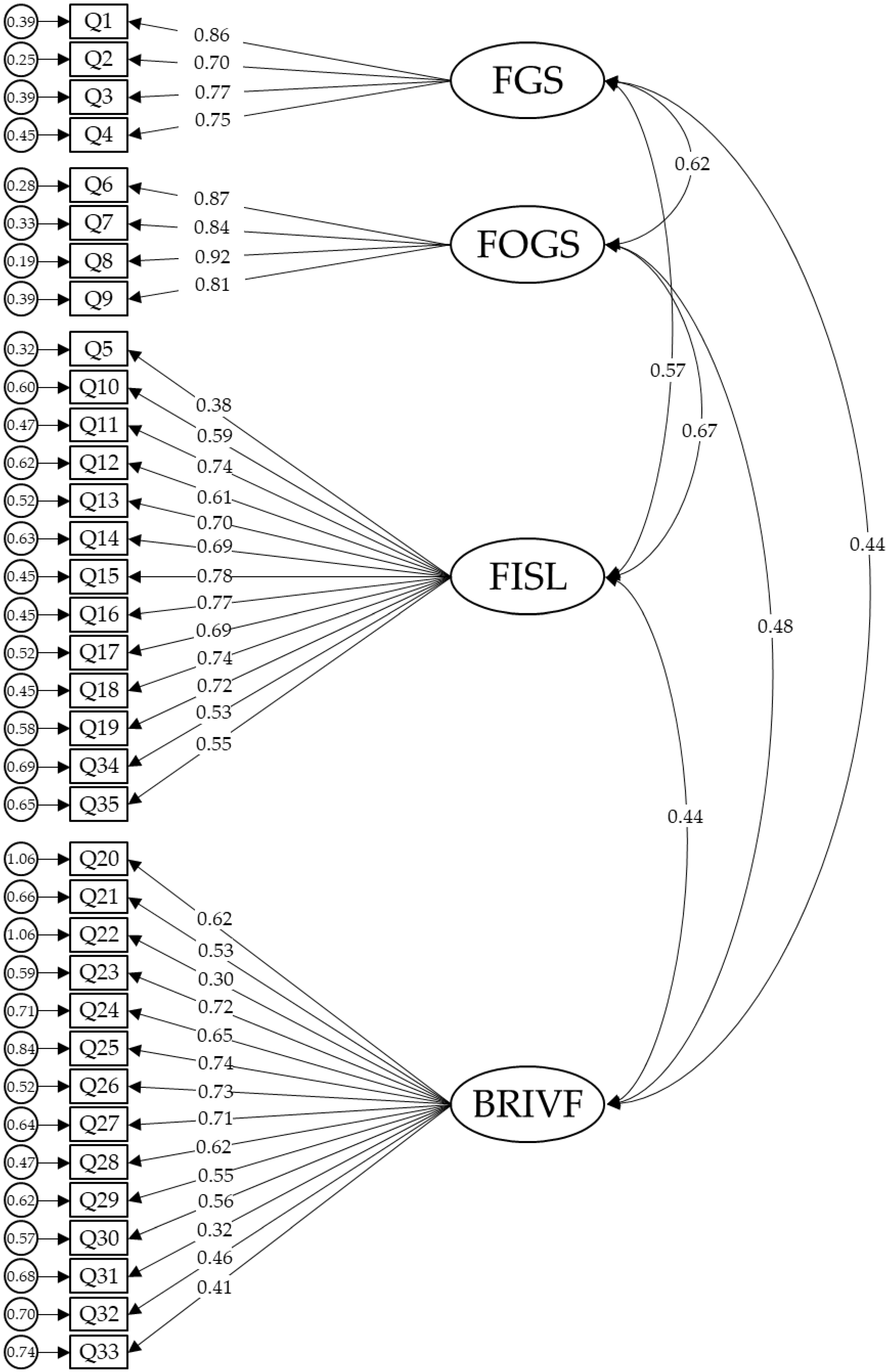
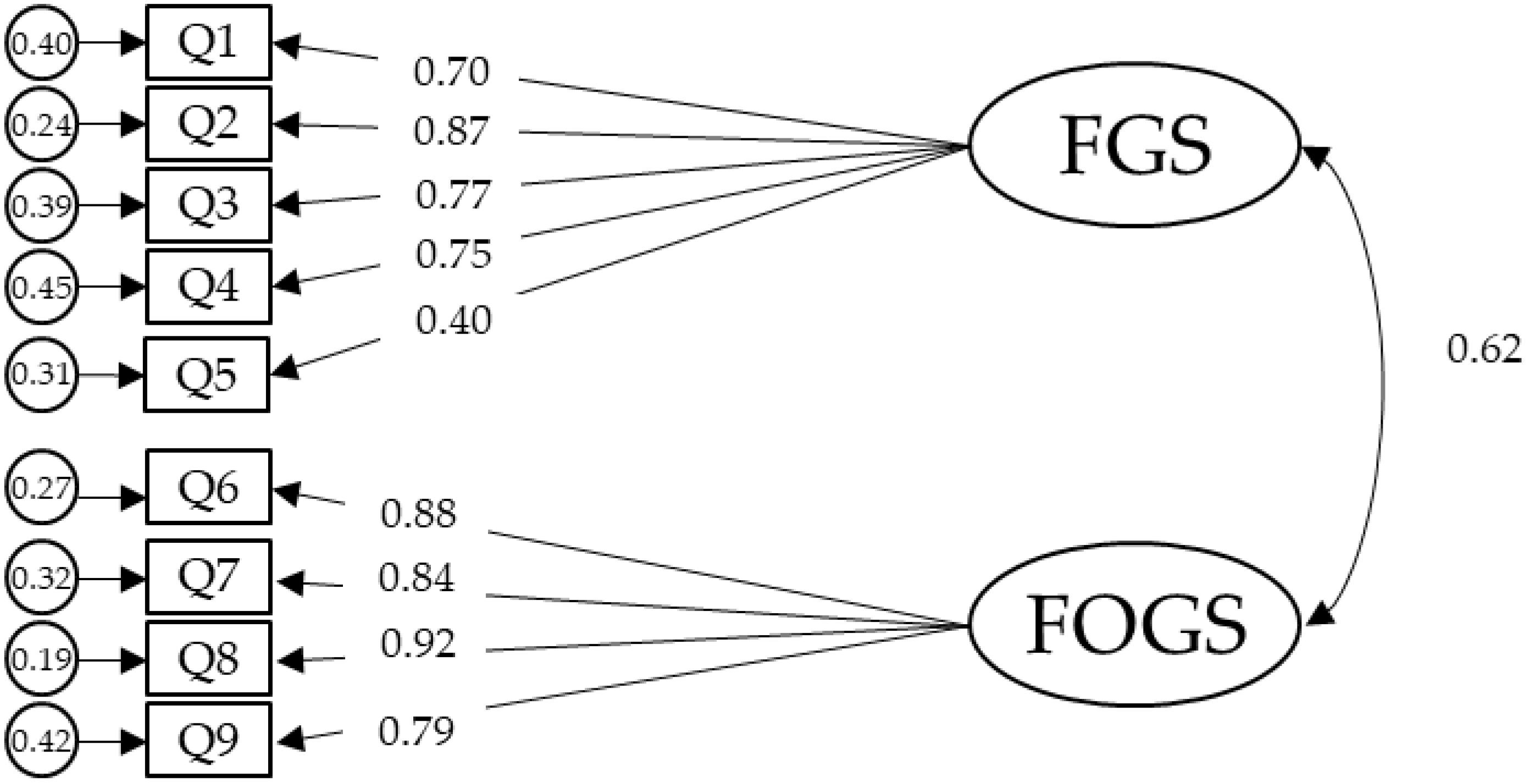
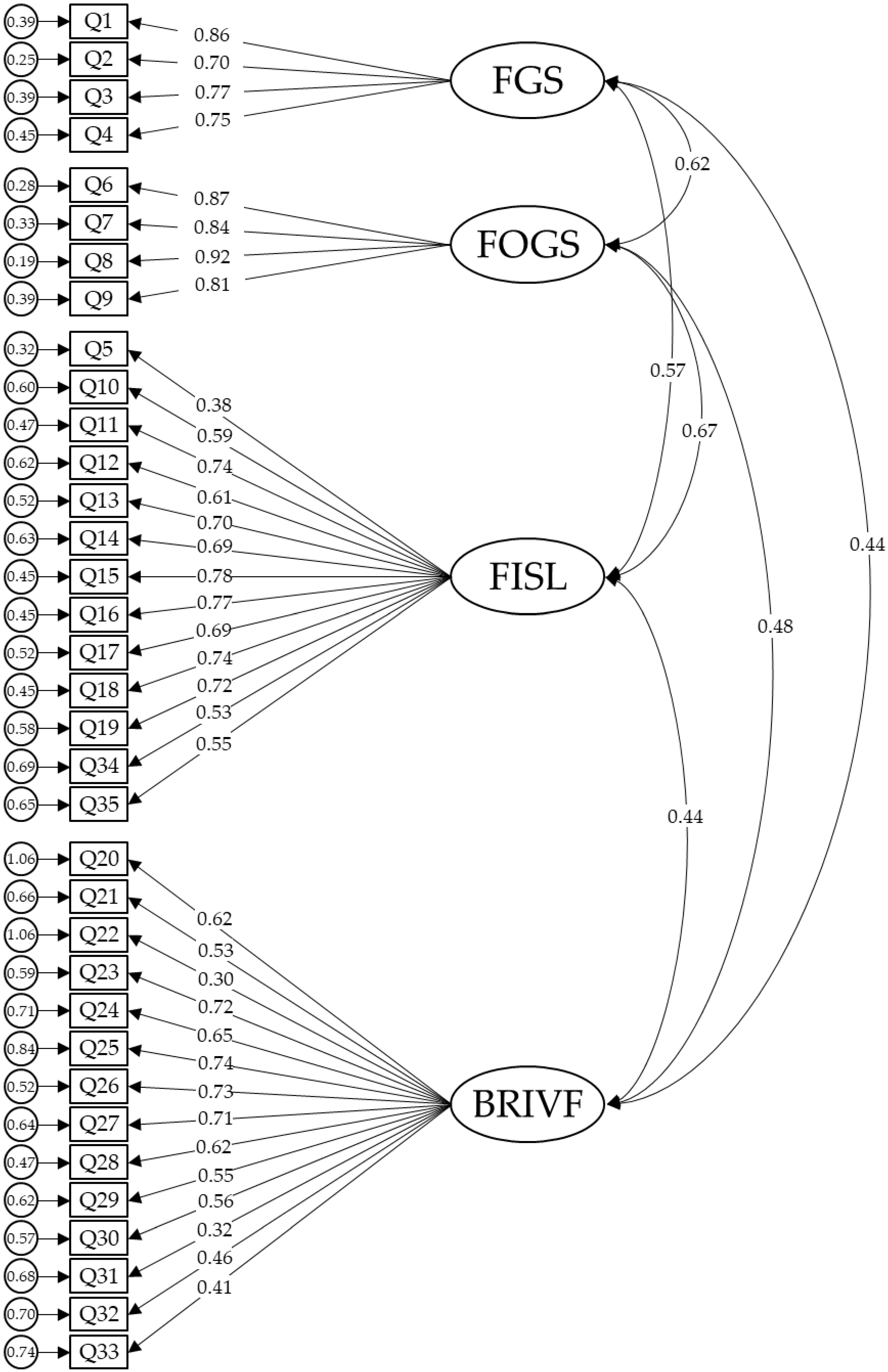
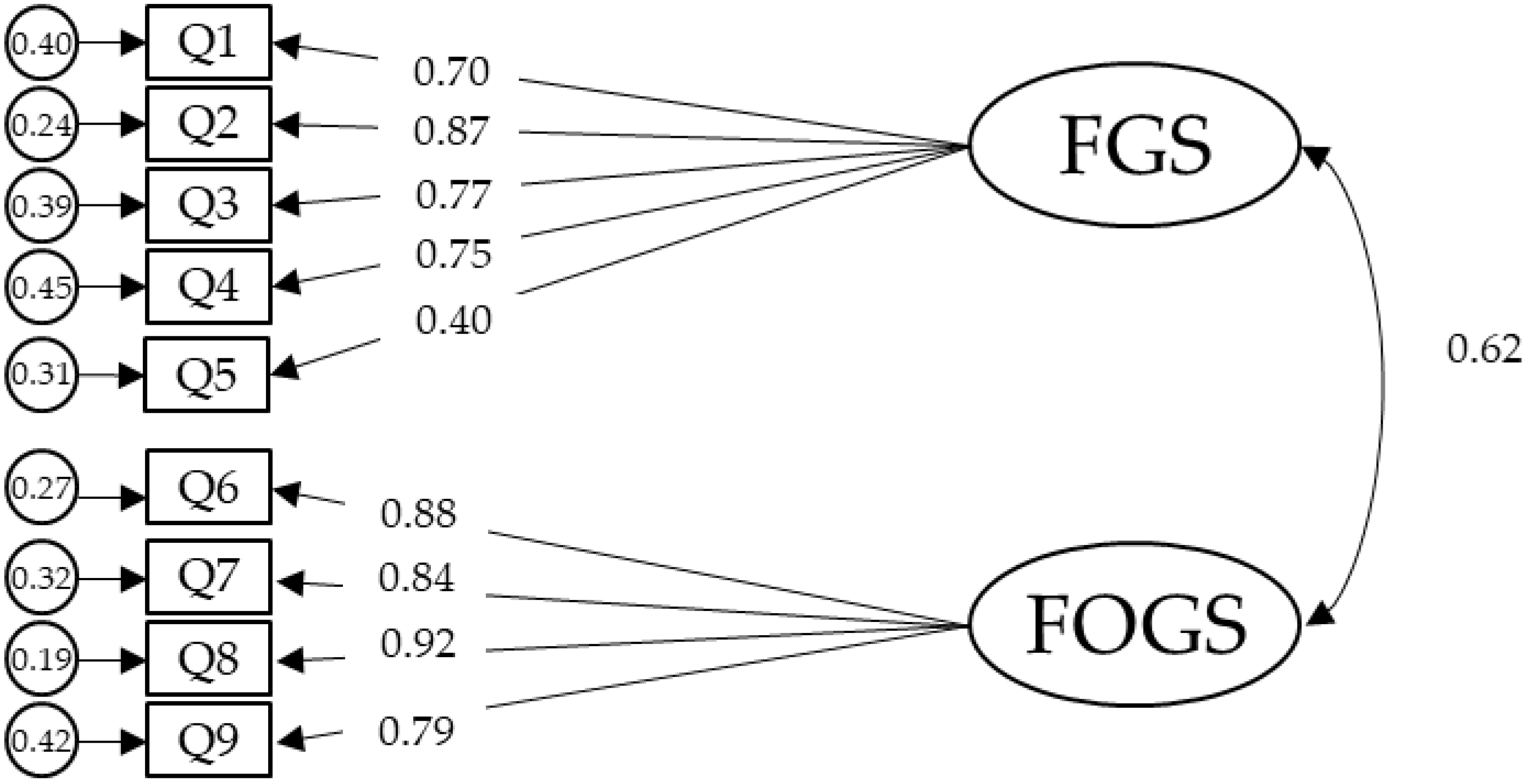
3.6. Factor Analysis
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Taylor, S. The Psychology of Pandemics: Preparing for the Next Global Outbreak of Infectious Disease. Newcastle upon Tyne; Cambridge Scholars Publishing: Cambridge, UK, 2019. [Google Scholar]
- Ackerl, K.; Atzmueller, M.; Grammer, K. The scent of fear. Neuroendocrinol. Lett. 2002, 23, 79–84. [Google Scholar] [PubMed]
- Shin, L.M.; Liberzon, I. The neurocircuitry of fear, stress, and anxiety disorders. Neuropsychopharmacology 2010, 35, 169–191. [Google Scholar] [CrossRef]
- Garcia, R. Neurobiology of fear and specific phobias. Learn. Mem. 2017, 24, 462–471. [Google Scholar] [CrossRef]
- Nelson, B.W.; Pettitt, A.; Flannery, J.E.; Allen, N.B. Rapid assessment of psychological and epidemiological correlates of COVID-19 concern, financial strain, and health-related behavior change in a large online sample. PLoS ONE 2020, 15, e0241990. [Google Scholar] [CrossRef]
- Qiu, J.; Shen, B.; Zhao, M.; Wang, Z.; Xie, B.; Xu, Y. A nationwide survey of psychological distress among Chinese people in the COVID-19 epidemic: Implications and policy recommendations. Gen. Psychiatry 2020, 33, e100213corr1. [Google Scholar] [CrossRef] [Green Version]
- Mohamed-Azzam Zakout, Y.; Saud Alreshidi, F.; Mustafa Elsaid, R.; Gadelkarim Ahmed, H. The magnitude of COVID-19 related stress, anxiety and depression associated with intense mass media coverage in Saudi Arabi. AIMS Public Health 2020, 7, 664. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Coronavirus Disease (COVID-19) Weekly Epidemiological Update and Weekly Operational Update; WHO: Geneva, Switzerland, 2021. [Google Scholar]
- Lai, C.C.; Shih, T.P.; Ko, W.C.; Tang, H.J.; Hsueh, P.R. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): The epidemic and the challenges. Int. J. Antimicrob. Agents 2020, 55, 105924. [Google Scholar] [CrossRef] [PubMed]
- Song, F.; Shi, N.; Shan, F.; Zhang, Z.; Shen, J.; Lu, H.; Ling, Y.; Jiang, Y.; Shi, Y. Emerging 2019 novel coronavirus (2019-NCoV) pneumonia. Radiology 2020, 295, 210–217. [Google Scholar] [CrossRef] [Green Version]
- World Health Organization. Transmission of SARS-CoV-2: Implications for Infection Prevention Precautions: Scientific Brief, 9 July 2020; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- Cox, R.C.; Jessup, S.C.; Luber, M.J.; Olatunji, B.O. Pre-pandemic disgust proneness predicts increased coronavirus anxiety and safety behaviors: Evidence for a diathesis-stress model. J. Anxiety Disord. 2020, 76, 102315. [Google Scholar] [CrossRef]
- Lupton, D.; Willis, K. The COVID-19 Crisis: Social Perspectives—Google Books; Routledge: London, UK, 2021. [Google Scholar]
- Ammar, A.; Brach, M.; Trabelsi, K.; Chtourou, H.; Boukhris, O.; Masmoudi, L.; Bouaziz, B.; Bentlage, E.; How, D.; Ahmed, M.; et al. Effects of COVID-19 Home Confinement on Eating Behaviour and Physical Activity: Results of the ECLB-COVID19 International Online Survey. Nutrients 2020, 12, 1583. [Google Scholar] [CrossRef]
- Drouin, M.; McDaniel, B.T.; Pater, J.; Toscos, T. How Parents and Their Children Used Social Media and Technology at the Beginning of the COVID-19 Pandemic and Associations with Anxiety. Cyberpsychol. Behav. Soc. Netw. 2020, 23, 727–736. [Google Scholar] [CrossRef]
- Goldmann, E.; Galea, S. Mental health consequences of disasters. Annu. Rev. Public Health 2014, 35, 169–183. [Google Scholar] [CrossRef]
- Kim, J.; Kim, Y.; Ha, J. Changes in Daily Life during the COVID-19 Pandemic among South Korean Older Adults with Chronic Diseases: A Qualitative Study. Int. J. Environ. Res. Public Health 2021, 18, 6781. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.-Y. Social reaction toward the 2019 novel coronavirus (COVID-19). Soc. Health Behav. 2020, 3, 1. [Google Scholar] [CrossRef]
- Fitzpatrick, K.M.; Harris, C.; Drawve, G. Fear of COVID-19 and the Mental Health Consequences in America. Psychol. Trauma Theory Res. Pract. Policy 2020, 12, S17–S21. [Google Scholar] [CrossRef] [PubMed]
- Ahorsu, D.K.; Lin, C.Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The Fear of COVID-19 Scale: Development and Initial Validation. Int. J. Ment. Health Addict. 2020, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Lee, Y.; Kim, B.-W.; Kim, S.-W.; Son, H.; Park, B.; Lee, H.; You, M.; Ki, M. Precautionary Behavior Practices and Psychological Characteristics of COVID-19 Patients and Quarantined Persons. Int. J. Environ. Res. Public Health 2021, 18, 6070. [Google Scholar] [CrossRef] [PubMed]
- Taylor, S.; Landry, C.A.; Paluszek, M.M.; Fergus, T.A.; McKay, D.; Asmundson, G.J.G. Development and initial validation of the COVID Stress Scales. J. Anxiety Disord. 2020, 72, 102232. [Google Scholar] [CrossRef]
- Mertens, G.; Gerritsen, L.; Duijndam, S.; Salemink, E.; Engelhard, I.M. Fear of the coronavirus (COVID-19): Predictors in an online study conducted in March 2020. J. Anxiety Disord. 2020, 74, 102258. [Google Scholar] [CrossRef] [PubMed]
- Cottin, M.; Hernández, C.; Núñez, C.; Labbé, N.; Quevedo, Y.; Davanzo, A.; Behn, A. “What If We Get Sick?”: Spanish Adaptation and Validation of the Fear of Illness and Virus Evaluation Scale in a Non-clinical Sample Exposed to the COVID-19 Pandemic. Front. Psychol. 2021, 12, 332. [Google Scholar] [CrossRef]
- Sousa, V.D.; Rojjanasrirat, W. Translation, adaptation and validation of instruments or scales for use in cross-cultural health care research: A clear and user-friendly guideline. J. Eval. Clin. Pract. 2011, 17, 268–274. [Google Scholar] [CrossRef] [PubMed]
- Conway, J.M.; Huffcutt, A.I. A Review and Evaluation of Exploratory Factor Analysis Practices in Organizational Research. Organ. Res. Methods 2003, 6, 147–168. [Google Scholar] [CrossRef]
- Terkawi, A.; Tsang, S.; Alkahtani, G.; Al-Mousa, S.; Al Musaed, S.; Alzoraigi, U.; Alasfar, E.; Doais, K.; Abdulrahman, A.; Altirkawi, K. Development and validation of Arabic version of the Hospital Anxiety and Depression Scale. Saudi J. Anaesth. 2017, 11, S11–S18. [Google Scholar] [CrossRef]
- Alyami, M.; Henning, M.; Krägeloh, C.U.; Alyami, H. Psychometric Evaluation of the Arabic Version of the Fear of COVID-19 Scale. Int. J. Ment. Health Addict. 2020, 1–14. [Google Scholar] [CrossRef]
- Hu, L.; Bentler, P.M. Cutoff criteria for fit indexes in covariance structure analysis: Conventional criteria versus new alternatives. PLoS ONE 2009, 6, e82131. [Google Scholar] [CrossRef]
- Kline, R. Principles and Practice of Structural Equation Modeling, 4th ed.; Kline, R., Ed.; The Guilford Press: New York, NY, USA, 2015. [Google Scholar]
- Steiger, J. Structural model evaluation and modification: An interval estimation approach. Mutlivariate Behav. Res. 1990, 52, 173–180. [Google Scholar] [CrossRef] [Green Version]
- Bentler, P.M.; Bonett, D.G. Significance Tests and Goodness-of-Fit in Analysis of Covariance Structures. Psychol. Bull. 1980, 88, 588–606. [Google Scholar] [CrossRef]
- Byrne, B.M. Structural Equation Modeling with AMOS: Basic Concepts, Applications, and Programming; Taylor & Francis Group: New York, NY, USA, 2010. [Google Scholar]
- Tucker, L.R.; Lewis, C. A reliability coefficient for maximum likelihood factor analysis. Psychometrika 1973, 38, 1–10. [Google Scholar] [CrossRef]
- Duncan, L.A.; Schaller, M.; Park, J.H. Perceived vulnerability to disease: Development and validation of a 15-item self-report instrument. Personal. Individ. Differ. 2009, 47, 541–546. [Google Scholar] [CrossRef]
- Pappas, G.; Kiriaze, I.J.; Giannakis, P.; Falagas, M.E. Psychosocial consequences of infectious diseases. Clin. Microbiol. Infect. 2009, 15, 743–747. [Google Scholar] [CrossRef] [Green Version]
- Schimmenti, A.; Starcevic, V.; Giardina, A.; Khazaal, Y.; Billieux, J. Multidimensional Assessment of COVID-19-Related Fears (MAC-RF): A Theory-Based Instrument for the Assessment of Clinically Relevant Fears During Pandemics. Front. Psychiatry 2020, 11, 748. [Google Scholar] [CrossRef]
- Çölkesen, F.; Kilincel, O.; Sozen, M.; Yıldız, E.; Beyaz, S.; Colkesen, F.; Aytekin, G.; Kocak, M.Z.; Alsancak, Y.; Araz, M.; et al. The impact of SARS-CoV-2 transmission fear and COVID-19 pandemic on the mental health of patients with primary immunodeficiency disorders, severe asthma, and other high-risk groups. medRxiv 2020. [Google Scholar] [CrossRef]
- DeVellis, R.F. Scale Development Theory and Applications, 4th ed.; SAGE Publications: Thousand Oaks, CA, USA, 2016; Volume 4. [Google Scholar]
- Krumpal, I. Determinants of social desirability bias in sensitive surveys: A literature review. Qual. Quant. 2013, 47, 2025–2047. [Google Scholar] [CrossRef]
- Ferketich, S. Focus on psychometrics. Aspects of item analysis. Res. Nurs. Health 1991, 14, 165–168. [Google Scholar] [CrossRef] [PubMed]
- Goyal, K.; Chauhan, P.; Chhikara, K.; Gupta, P.; Singh, M.P. Fear of COVID 2019: First suicidal case in India! Asian J. Psychiatr. 2020, 49. [Google Scholar] [CrossRef]
- Mamun, M.A.; Griffiths, M.D. First COVID-19 suicide case in Bangladesh due to fear of COVID-19 and xenophobia: Possible suicide prevention strategies. Asian J. Psychiatr. 2020, 51, 102073. [Google Scholar] [CrossRef]
- Asmundson, G.J.G.; Taylor, S. How health anxiety influences responses to viral outbreaks like COVID-19: What all decision-makers, health authorities, and health care professionals need to know. J. Anxiety Disord. 2020, 71, 102211. [Google Scholar] [CrossRef]
- Banerjee, D. The COVID-19 outbreak: Crucial role the psychiatrists can play. Asian J. Psychiatr. 2020, 50, 102014. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Age (Years) | Minimum | 18 |
| Maximum | 70 | |
| Mean ± SD | 33.88 ± 10.52 | |
| Under 25 | 128 (25.15) | |
| Between 25 and 50 | 334 (65.62) | |
| Above 50 | 47 (9.23) | |
| Gender n (%) | Male | 201 (39.49) |
| Female | 308 (60.51) | |
| Nationality n (%) | Saudi | 476 (93.52) |
| Non-Saudi | 33 (6.48) | |
| Educational Level n (%) | High school or less | 74 (14.54) |
| Diploma | 54 (10.61) | |
| Bachelor | 262 (51.47) | |
| Postgraduate | 119 (23.38) | |
| Living Status n (%) | Spouse | 31 (6.09) |
| Spouse and kids | 255 (50.10) | |
| Parents | 118 (23.18) | |
| Alone with/without kids | 25 (4.91) | |
| Other family members | 60 (11.79) | |
| Other | 20 (3.93) | |
| Marital Status n (%) | Single | 180 (35.36) |
| Married | 317 (62.28) | |
| Divorced or widow | 12 (2.36) | |
| Employment Status n (%) | Student | 135 (26.52) |
| Unemployed | 46 (9.04) | |
| Private sector | 88 (17.29) | |
| Governmental sector | 199 (39.10) | |
| Retired | 41 (8.05) | |
| Works in the Medical Field n (%) | Yes | 206 (40.47) |
| No | 303 (59.53) |
| Fears about Contamination and Illness | Fears about Social Distancing | Behaviors Related to Illness and Virus Fears | Impact of Illness and Virus Fears | ||
|---|---|---|---|---|---|
| Distribution | Skewness | 0.28 | 0.87 | 0.25 | 1.04 |
| Kurtosis | −0.60 | 0.02 | −0.16 | 0.06 | |
| Internal Reliability | Cronbach’s alpha | 0.89 | 0.91 | 0.87 | 0.84 |
| McDonald’s Omega | 0.90 | 0.91 | 0.87 | - | |
| Correlations | Fears about Contamination and Illness | 1 | |||
| Fears about Social Distancing | 0.64 ** | 1 | |||
| Behaviors Related to Illness and Virus Fears | 0.48 ** | 0.42 ** | 1 | ||
| Impact of Illness and Virus Fears | 0.44 ** | 0.51 ** | 0.33 ** | 1 | |
| FCV-19S | 0.54 ** | 0.44 ** | 0.47 ** | 0.51 ** | |
| Strongly Disagree n (%) | Disagree n (%) | Neutral n (%) | Agree n (%) | Strongly Agree n (%) | Mean ± SD | |
|---|---|---|---|---|---|---|
| 1. Questions were clear and easy | 17 (3.34) | 30 (5.89) | 51 (10.02) | 291 (57.17) | 120 (23.58) | 3.92 ± 0.93 |
| 2. Questions covered all my problem areas with fear of illness and virus | 14 (2.75) | 44 (8.64) | 95 (18.66) | 269 (52.85) | 87 (17.10) | 3.73 ± 0.94 |
| 3. I would like the use of this questionnaire for future assessments | 23 (4.52) | 61 (11.98) | 135 (26.52) | 224 (44.01) | 66 (12.97) | 3.49 ± 1.01 |
| 4. The questionnaire lacks important questions regarding my fear of illness and virus | 125 (24.55) | 156 (30.65) | 113 (22.20) | 87 (17.10) | 28 (5.50) | 2.48 ± 1.19 |
| 5. Some of the questions violate my privacy | 272 (53.44) | 128 (25.15) | 42 (8.25) | 47 (9.23) | 20 (3.93) | 1.85 ± 1.15 |
| X2/DF | TLI | CFI | RMSEA (90% CI) | SRMR | |
|---|---|---|---|---|---|
| Original structure | |||||
| Four factors (items 1–35) | 5.26 | 0.74 | 0.76 | 0.09 (0.09, 0.10) | 0.08 |
| Two factors (items 1–19) | 10.38 | 0.74 | 0.77 | 0.14 (0.13, 0.14) | 0.08 |
| Proposed new structures | |||||
| Four factors (items 1–35) | 4.78 | 0.77 | 0.79 | 0.08 (0.08, 0.09) | 0.07 |
| Three factors (items 1–19) | 6.96 | 0.83 | 0.85 | 0.11 (0.10, 0.12) | 0.07 |
| Two factors (items 1–9) | 4.68 | 0.95 | 0.97 | 0.09 (0.07, 0.11) | 0.03 |
| Component | ||||
|---|---|---|---|---|
| Item Number | Fears of Getting Sick | Fears That Others Get Sick | Fears of the Impact on Social Life | Behaviors Related to Illness and Virus Fears |
| 1 | 0.68 | |||
| 2 | 0.67 | |||
| 3 | 0.64 | |||
| 4 | 0.61 | |||
| 5 | 0.40 | |||
| 6 | 0.51 | |||
| 7 | 0.55 | |||
| 8 | 0.57 | |||
| 9 | 0.43 | |||
| 10 | 0.63 | |||
| 11 | 0.74 | |||
| 12 | 0.63 | |||
| 13 | 0.70 | |||
| 14 | 0.71 | |||
| 15 | 0.79 | |||
| 16 | 0.77 | |||
| 17 | 0.72 | |||
| 18 | 0.74 | |||
| 19 | 0.75 | |||
| 20 | 0.64 | |||
| 21 | 0.48 | |||
| 22 | 0.32 | |||
| 23 | 0.73 | |||
| 24 | 0.67 | |||
| 25 | 0.75 | |||
| 26 | 0.71 | |||
| 27 | 0.71 | |||
| 28 | 0.67 | |||
| 29 | 0.54 | |||
| 30 | 0.59 | |||
| 31 | 0.37 | |||
| 32 | 0.44 | |||
| 33 | 0.45 | |||
| 34 | 0.53 | |||
| 35 | 0.57 | |||
| Item Number | Component | ||
|---|---|---|---|
| Fears of the Impact on Social Life | Fears of Getting Sick | Fears That Others Get Sick | |
| 1 | 0.75 (0.71) | ||
| 2 | 0.81 (0.82) | ||
| 3 | 0.79 (0.80) | ||
| 4 | 0.76 (0.80) | ||
| 5 | 0.41 (0.50) | ||
| 6 | 0.80 (0.84) | ||
| 7 | 0.81 (0.86) | ||
| 8 | 0.84 (0.90) | ||
| 9 | 0.73 (0.83) | ||
| 10 | 0.66 | ||
| 11 | 0.71 | ||
| 12 | 0.59 | ||
| 13 | 0.73 | ||
| 14 | 0.63 | ||
| 15 | 0.73 | ||
| 16 | 0.71 | ||
| 17 | 0.75 | ||
| 18 | 0.71 | ||
| 19 | 0.65 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tounsi, A.; Alammar, S.; Almaflehi, N.; Bamashmous, M.; Al Madani, A.; Ibrahim, M.S. Psychometric Validation of the Arabic Fear of Illness and Virus Evaluation. Int. J. Environ. Res. Public Health 2021, 18, 8529. https://doi.org/10.3390/ijerph18168529
Tounsi A, Alammar S, Almaflehi N, Bamashmous M, Al Madani A, Ibrahim MS. Psychometric Validation of the Arabic Fear of Illness and Virus Evaluation. International Journal of Environmental Research and Public Health. 2021; 18(16):8529. https://doi.org/10.3390/ijerph18168529
Chicago/Turabian StyleTounsi, Abrar, Shahad Alammar, Nassr Almaflehi, Mohamed Bamashmous, Abdullah Al Madani, and Maria Salem Ibrahim. 2021. "Psychometric Validation of the Arabic Fear of Illness and Virus Evaluation" International Journal of Environmental Research and Public Health 18, no. 16: 8529. https://doi.org/10.3390/ijerph18168529
APA StyleTounsi, A., Alammar, S., Almaflehi, N., Bamashmous, M., Al Madani, A., & Ibrahim, M. S. (2021). Psychometric Validation of the Arabic Fear of Illness and Virus Evaluation. International Journal of Environmental Research and Public Health, 18(16), 8529. https://doi.org/10.3390/ijerph18168529