
Clinical Decision Support Systems for Diagnosis in Primary Care: A Scoping Review


Abstract
1. Introduction
2. Materials and Methods
2.1. Search Strategy
2.2. Eligibility Criteria
3. Results
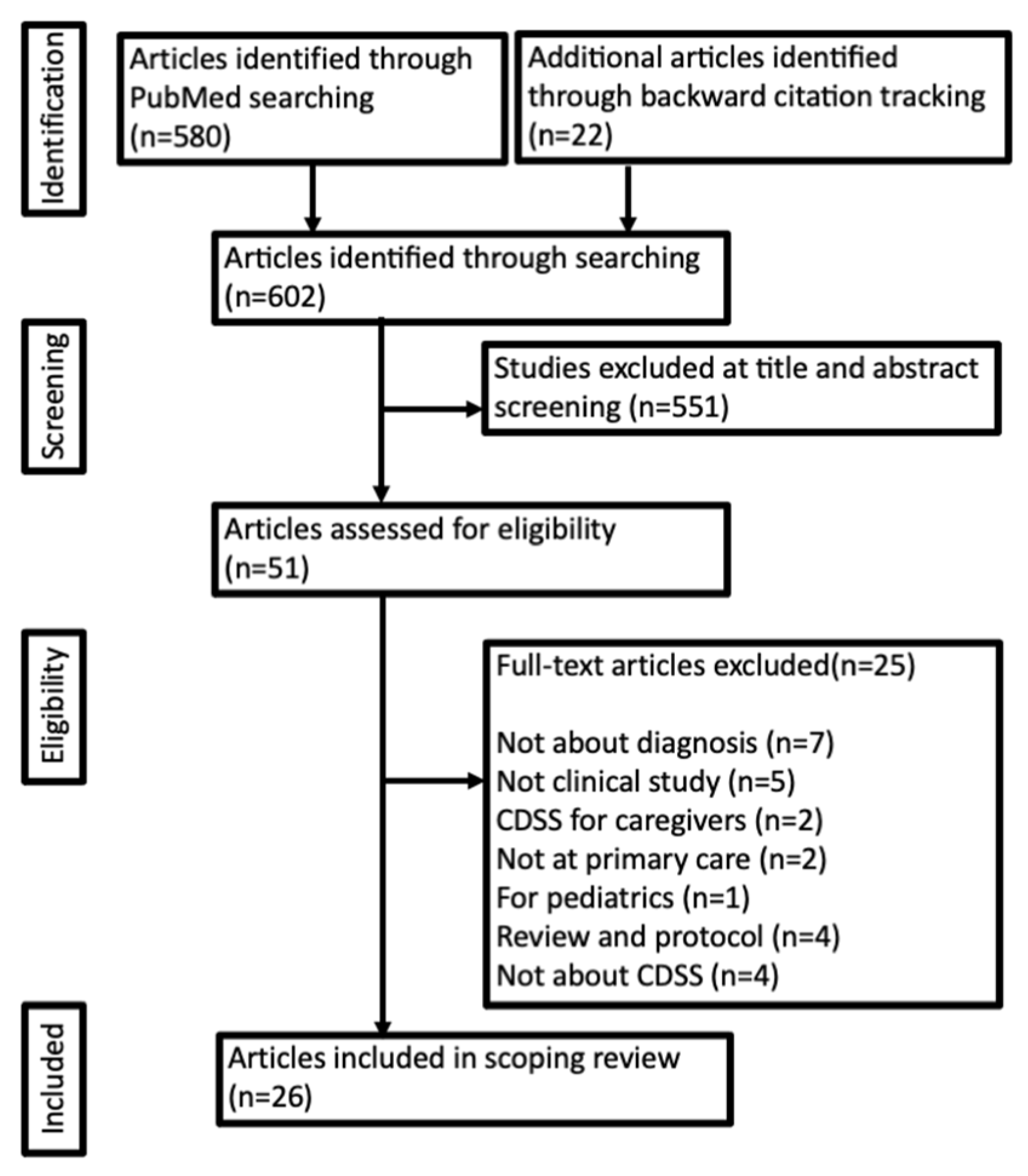
3.1. General Overview
3.2. Effect of CDSS on the Screening and Diagnosis of Composite Outcomes
3.3. Effect of CDSS on the Screening and Diagnosis of Cancer
3.4. Effect of CDSS on the Screening and Diagnosis of Cardiovascular Risk Factors
3.5. Effect of CDSS on the Screening and Diagnosis of Musculoskeletal Conditions
3.6. Effect of CDSS on the Screening and Diagnosis of Infectious Diseases
3.7. Effect of CDSS on the Screening and Diagnosis of Other Diseases
4. Discussion
Strengths and Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Nurek, M.; Kostopoulou, O.; Delaney, B.C.; Esmail, A. Reducing Diagnostic Errors in Primary Care. A Systematic Meta-Review of Computerized Diagnostic Decision Support Systems by the LINNEAUS Collaboration on Patient Safety in Primary Care. Eur. J. Gen. Pract. 2015, 21, 8–13. [Google Scholar] [CrossRef]
- Singh, H.; Meyer, A.N.D.; Thomas, E.J. The Frequency of Diagnostic Errors in Outpatient Care: Estimations from Three Large Observational Studies Involving US Adult Populations. BMJ Qual. Saf. 2014, 23, 727–731. [Google Scholar] [CrossRef]
- Singh, H.; Giardina, T.D.; Meyer, A.N.D.; Forjuoh, S.N.; Reis, M.D.; Thomas, E.J. Types and origins of diagnostic errors in primary care settings. JAMA Int. Med. 2013, 173, 418–425. [Google Scholar] [CrossRef] [PubMed]
- Cresswell, K.M.; Panesar, S.S.; Salvilla, S.A.; Carson-Stevens, A.; Larizgoitia, I.; Donaldson, L.J.; Bates, D.; Sheikh, A.; World Health Organization’s (WHO) Safer Primary Care Expert Working Group. Global Research Priorities to Better Understand the Burden of Iatrogenic Harm in Primary Care: An International Delphi Exercise. PLoS Med. 2013, 10, e1001554. [Google Scholar] [CrossRef]
- Panesar, S.S.; deSilva, D.; Carson-Stevens, A.; Cresswell, K.M.; Salvilla, S.A.; Slight, S.P.; Javad, S.; Netuveli, G.; Larizgoitia, I.; Donaldson, L.J.; et al. How Safe Is Primary Care? A Systematic Review. BMJ Qual. Saf. 2016, 25, 544–553. [Google Scholar] [CrossRef]
- Kostopoulou, O.; Delaney, B.C.; Munro, C.W. Diagnostic Difficulty and Error in Primary Care--A Systematic Review. Fam. Pract. 2008, 25, 400–413. [Google Scholar] [CrossRef] [PubMed]
- Singh, H.; Schiff, G.D.; Graber, M.L.; Onakpoya, I.; Thompson, M.J. The Global Burden of Diagnostic Errors in Primary Care. BMJ Qual. Saf. 2017, 26, 484–494. [Google Scholar] [CrossRef] [PubMed]
- Delaney, B.C.; Kostopoulou, O. Decision Support for Diagnosis Should Become Routine in 21st Century Primary Care. Br. J. Gen. Pract. 2017, 67, 494–495. [Google Scholar] [CrossRef] [PubMed]
- Farmer, N. An Update and Further Testing of a Knowledge-Based Diagnostic Clinical Decision Support System for Musculoskeletal Disorders of the Shoulder for Use in a Primary Care Setting. J. Eval. Clin. Pract. 2014, 20, 589–595. [Google Scholar] [CrossRef]
- Delaney, B.C.; Fitzmaurice, D.A.; Riaz, A.; Hobbs, F.D. Can Computerised Decision Support Systems Deliver Improved Quality in Primary Care? Interview by Abi Berger. BMJ 1999, 319, 1281. [Google Scholar] [CrossRef][Green Version]
- Roshanov, P.S.; Fernandes, N.; Wilczynski, J.M.; Hemens, B.J.; You, J.J.; Handler, S.M.; Nieuwlaat, R.; Souza, N.M.; Beyene, J.; Van Spall, H.G.; et al. Features of Effective Computerised Clinical Decision Support Systems: Meta-Regression of 162 Randomised Trials. BMJ 2013, 346, f657. [Google Scholar] [CrossRef]
- Osheroff, J.A.; Teich, J.M.; Middleton, B.; STeen, E.B.; Wright, A.; Detmer, D.E. A Roadmap for National Action on Clinical Decision Support. J. Am. Med. Inform. Assoc. 2007, 14, 141. [Google Scholar] [CrossRef] [PubMed]
- Sutton, R.T.; Pincock, T.; Baumgar, D.C.; Sadowski, D.C.; Fedorak, R.N.; Kroeker, K.I. An Overview of Clinical Decision Support Systems: Benefits, Risks, and Strategies for Success. NPJ Digit. Med. 2020, 3, 17. [Google Scholar] [CrossRef]
- Henderson, E.J.; Rubin, G.P. The Utility of an Online Diagnostic Decision Support System (Isabel) in General Practice: A Process Evaluation. JRSM Short Rep. 2013, 4, 31. [Google Scholar]
- Fraser, H.; Coiera, E.; Wong, D. Safety of Patient-facing Digital Symptom Checkers. Lancet 2018, 392, 2263. [Google Scholar] [CrossRef]
- Research and Markets. Healthcare. Hospital Management. E-Healthcare. Available online: https://www.researchandmarkets.com/reports/5317115/global-clinical-decision-support-system-market (accessed on 25 July 2021).
- Inokuchi, R.; Sato, H.; Nakajima, S.; Shinohara, K.; Nakamura, K.; Gunshin, M.; Hiruma, T.; Ishii, T.; Matsubara, T.; Kitsuta, Y.; et al. Development of Information Systems and Clinical Decision Support Systems for Emergency Departments: A Long Road Ahead for Japan. Emerg. Med. J. 2013, 30, 914. [Google Scholar] [CrossRef] [PubMed]
- Biruk, S.; Yilma, T.; Andualem, M.; Tilahun, B. Health Professionals’ Readiness to Implement Electronic Medical Record System at Three Hospitals in Ethiopia: A Cross Sectional Study. BMC Med. Inform. Decis. Mak. 2014, 14, 115. [Google Scholar]
- Ei-Kareh, R.; Hasan, O.; Schiff, G.D. Use of Health Information Technology to Reduce Diagnostic Errors. BMJ Qual. Saf. 2013, 22, ii40–ii51. [Google Scholar] [CrossRef]
- Chima, S.; Reece, C.J.; Milley, K.; Milton, S.; Mclntosh, J.G.; Emery, J.D. Decision Support Tools to Improve Cancer Diagnostic Decision Making in Primary Care: A Systematic Review. Br. J. Gen. Pract. 2019, 69, e809. [Google Scholar] [CrossRef] [PubMed]
- Jing, X.; Himawan, L.; Law, T. Availability and Usage of Clinical Decision Support Systems (CDSSs) in Office-based Primary Care Settings in the USA. BMJ Health Care Inform. 2019, 26, e100015. [Google Scholar]
- Harry, M.L.; Truitt, A.; Saman, D.M.; Henzler-Buckingham, H.A.; Allen, C.T.; Walton, K.M.; Ekstrom, H.L.; O’Connor, P.L.; Sperl-Hillen, J.M.; Bianco, J.A.; et al. Barriers and Facilitators to Implementing Cancer Prevention Clinical Decision Support in Primary Care: A Qualitative Study. BMC Health Serv. Res. 2019, 19, 534. [Google Scholar]
- Horsky, J.; Schiff, G.D.; Johnston, D.; Mercincavage, L.; Bell, D.; Middleton, B. Interface Design Principles for Usable Decision Support: A Targeted Review of Best Practices for Clinical Prescribing Interventions. J. Biomed. Inform. 2012, 45, 1202. [Google Scholar] [CrossRef]
- Brunner, J.; Chuang, E.; Goldzweig, C.; Cain, C.L.; Sugar, C.; Yano, E.M. User-centered Design to Improve Clinical Decision Support in Primary Care. Int. J. Med. Inform. 2017, 104, 56. [Google Scholar] [CrossRef]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA Extension for Scoping Reviews (PRISMA-ScR): Checklist and Explanation. Ann. Intern. Med. 2018, 169, 467–473. [Google Scholar] [CrossRef] [PubMed]
- Rosser, W.W.; McDowell, I.; Newell, C. Use of Reminders for Preventive Procedures in Family Medicine. Can. Med Assoc. J. 1991, 145, 807–814. [Google Scholar]
- Ornstein, S.M.; Garr, D.R.; Jenkins, R.G.; Rust, P.F.; Arnon, A. Computer-Generated Physician and Patient Reminders. Tools to Improve Population Adherence to Selected Preventive Services. J. Fam. Pract. 1991, 32, 82–90. [Google Scholar]
- McPhee, S.J.; Bird, J.A.; Fordham, D.; Rodnick, J.E.; Osborn, E.H. Promoting Cancer Prevention Activities by Primary Care Physicians. Results of a Randomized, Controlled Trial. JAMA 1991, 266, 538–544. [Google Scholar] [CrossRef]
- McPhee, S.J.; Bird, J.A.; Jenkins, C.N.; Fordham, D. Promoting Cancer Screening. A Randomized, Controlled Trial of Three Interventions. Arch. Intern. Med. 1989, 149, 1866–1872. [Google Scholar] [CrossRef] [PubMed]
- McDonald, C.J.; Hui, S.L.; Smith, D.M.; Tierney, W.M.; Cohen, S.J.; Weinberger, M.; McCabe, G.P. Reminders to Physicians from an Introspective Computer Medical Record. A Two-Year Randomized Trial. Ann. Intern. Med. 1984, 100, 130–138. [Google Scholar] [CrossRef] [PubMed]
- Hamilton, W.; Green, T.; Martins, T.; Elliott, K.; Rubin, G.; Macleod, U. Evaluation of Risk Assessment Tools for Suspected Cancer in General Practice: A Cohort Study. Br. J. Gen. Pract. 2013, 63, e30–e36. [Google Scholar] [CrossRef] [PubMed]
- Murphy, D.R.; Wu, L.; Thomas, E.J.; Forjuoh, S.N.; Meyer, A.N.; Singh, H. Electronic Trigger-Based Intervention to Reduce Delays in Diagnostic Evaluation for Cancer: A Cluster Randomized Controlled Trial. J. Clin. Oncol. 2015, 33, 3560–3567. [Google Scholar] [CrossRef]
- Price, S.; Spencer, A.; Medina-Lara, A.; Hamilton, W. Availability and Use of Cancer Decision-Support Tools: A Cross-Sectional Survey of UK Primary Care. Br. J. Gen. Pract. 2019, 69, e437–e443. [Google Scholar] [CrossRef] [PubMed]
- Vetter, M.J. The Influence of Clinical Decision Support on Diagnostic Accuracy in Nurse Practitioners. Worldviews Evid. Based Nurs. 2015, 12, 355–363. [Google Scholar] [CrossRef]
- Shimizu, T.; Nemoto, T.; Tokuda, Y. Effectiveness of a Clinical Knowledge Support System for Reducing Diagnostic Errors in Outpatient Care in Japan: A Retrospective Study. Int. J. Med. Inform. 2018, 109, 1–4. [Google Scholar] [CrossRef]
- Burack, R.C.; Gimotty, P.A. Promoting Screening Mammography in Inner-City Settings. The Sustained Effectiveness of Com-puterized Reminders in a Randomized Controlled Trial. Med. Care 1997, 35, 921–931. [Google Scholar] [CrossRef] [PubMed]
- Burack, R.C.; Gimotty, P.A.; George, J.; McBride, S.; Moncrease, A.; Simon, M.S.; Dews, P.; Coombs, J. How Reminders Given to Patients and Physicians Affected Pap Smear Use in a Health Maintenance Organization: Results of a Randomized Controlled Trial. Cancer 1998, 82, 2391–2400. [Google Scholar] [CrossRef]
- Sequist, T.D.; Zaslavsky, A.M.; Marshall, R.; Fletcher, R.H.; Ayanian, J.Z. Patient and Physician Reminders to Promote Colo-rectal Cancer Screening: A Randomized Controlled Trial. Arch. Intern. Med. 2009, 169, 364–371. [Google Scholar] [CrossRef] [PubMed]
- Litvin, C.B.; Hyer, J.M.; Ornstein, S.M. Use of Clinical Decision Support to Improve Primary Care Identification and Man-agement of Chronic Kidney Disease (CKD). J. Am. Board Fam. Med. 2016, 29, 604–612. [Google Scholar] [CrossRef]
- Lee, N.J.; Chen, E.S.; Currie, L.M.; Donovan, M.; Hall, E.K.; Jia, H.; John, R.M.; Bakken, S. The Effect of a Mobile Clinical Deci-sion Support System on the Diagnosis of Obesity and Overweight in Acute and Primary Care Encounters. Adv. Nurs. Sci. 2009, 32, 211–221. [Google Scholar] [CrossRef] [PubMed]
- Chaudhry, R.; Tulledge-Scheitel, S.M.; Parks, D.A.; Angstman, K.B.; Decker, L.K.; Stroebel, R.J. Use of a Web-Based Clinical Decision Support System to Improve Abdominal Aortic Aneurysm Screening in a Primary Care Practice. J. Eval. Clin. Pract. 2012, 18, 666–670. [Google Scholar] [CrossRef]
- Kenealy, T.; Arroll, B.; Petrie, K.J. Patients and Computers as Reminders to Screen for Diabetes in Family Practice. Random-ized-Controlled Trial. J. Gen. Intern. Med. 2005, 20, 916–921. [Google Scholar] [CrossRef] [PubMed][Green Version]
- van Wyk, J.T.; van Wijk, M.A.; Sturkenboom, M.C.; Mosseveld, M.; Moorman, P.W.; van der Lei, J. Electronic Alerts Versus On-Demand Decision Support to Improve Dyslipidemia Treatment: A Cluster Randomized Controlled Trial. Circulation 2008, 117, 371–378. [Google Scholar] [CrossRef] [PubMed]
- Rubenstein, L.V.; McCoy, J.M.; Cope, D.W.; Barrett, P.A.; Hirsch, S.H.; Messer, K.S.; Young, R.T. Improving Patient Quality of Life with Feedback to Physicians About Functional Status. J. Gen. Intern. Med. 1995, 10, 607–614. [Google Scholar] [CrossRef]
- DeJesus, R.S.; Angstman, K.B.; Kesman, R.; Stroebel, R.J.; Bernard, M.E.; Scheitel, S.M.; Hunt, V.L.; Rahman, A.S.; Chaudhry, R. Use of a Clinical Decision Support System to Increase Osteoporosis Screening. J. Eval. Clin. Pract. 2012, 18, 89–92. [Google Scholar] [CrossRef]
- DeSilva, M.B.; Kodet, A.; Walker, P.F. A Best Practice Alert for Identifying Hepatitis B-Infected Patients. Am. J. Trop. Med. Hyg. 2020, 103, 884–886. [Google Scholar] [CrossRef]
- Chak, E.; Taefi, A.; Li, C.S.; Chen, M.S.; Harris, A.M.; MacDonald, S.; Bowlus, C. Electronic Medical Alerts Increase Screening for Chronic Hepatitis B: A Randomized, Double-Blind, Controlled Trial. Cancer Epidemiol. Biomark. Prev. 2018, 27, 1352–1357. [Google Scholar] [CrossRef]
- Sundaram, V.; Lazzeroni, L.C.; Douglass, L.R.; Sanders, G.D.; Tempio, P.; Owens, D.K. A Randomized Trial of Computer-Based Reminders and Audit and Feedback to Improve HIV Screening in a Primary Care Setting. Int. J. STD AIDS 2009, 20, 527–533. [Google Scholar] [CrossRef] [PubMed]
- Miller, M.J.; Burns, C.F.; Kapusnik-Uner, J.; Carreno, R.; Matuszewski, K.A. Depression Screening for Prescribed Medications with Mental Health Risk: Considerations for Clinical Decision Support, Workflow Redesign, and Health Information Exchange Arrangements. Res. Soc. Adm. Pharm. 2017, 13, 485–493. [Google Scholar] [CrossRef] [PubMed]
- Downs, M.; Turner, S.; Bryans, M.; Wilcock, J.; Keady, J.; Levin, E.; O’Carroll, R.; Howie, K.; Iliffe, S. Effectiveness of Educational Interventions in Improving Detection and Management of Dementia in Primary Care: Cluster Randomised Controlled Study. BMJ 2006, 332, 692–696. [Google Scholar] [CrossRef]
- Ahmad, F.; Hogg-Johnson, S.; Stewart, D.E.; Skinner, H.A.; Glazier, R.H.; Levinson, W. Computer-Assisted Screening for In-timate Partner Violence and Control: A Randomized Trial. Ann. Intern. Med. 2009, 151, 93–102. [Google Scholar] [CrossRef]
- Cooper, J.G.; West, R.M.; Clamp, S.E.; Hassan, T.B. Does Computer-Aided Clinical Decision Support Improve the Management of Acute Abdominal Pain? A Systematic Review. Emerg. Med. J. 2011, 28, 553–557. [Google Scholar] [CrossRef] [PubMed]
- López, M.M.; López, M.M.; de la Torre Díez, I.T.; Jimeno, J.C.P.; López-Coronado, M. MHealth App for iOS to Help in Diagnostic Decision in Ophthalmology to Primary Care Physicians. J. Med. Syst. 2017, 41, 81. [Google Scholar] [CrossRef]
- Gerbert, B.; Bronstone, A.; Maurer, T.; Hofmann, R.; Berger, T. Decision Support Software to Help Primary Care Physicians Triage Skin Cancer: A Pilot Study. Arch. Dermatol. 2000, 136, 187–192. [Google Scholar] [CrossRef]
- Pearce, F.; Lanyon, P.C.; Watts, R.A. Can Prediction Models in Primary Care Enable Earlier Diagnosis of Rare Rheumatic Diseases? Rheumatology 2018, 57, 2065–2066. [Google Scholar] [CrossRef] [PubMed]
- Ramnarayan, P.; Roberts, C.G.; Coren, M.; Nanduri, V.; Tomlinson, A.; Taylor, M.P.; Wyatt, J.C.; Britto, J.F. Assessment of the potential impact of a reminder system on the reduction of diagnostic errors: A quasi-experimental study. BMC Med. Inform. Decis. Mak. 2006, 6, 22. [Google Scholar] [CrossRef] [PubMed]
- Feldman, M.D.; Petersen, A.J.; Karliner, L.S.; Tice, J.A. Who is responsible for evaluating the safety and effectiveness of medical devices? The role of independent technology assessment. J. Gen. Intern. Med. 2007, 23 (Suppl. S1), 57–63. [Google Scholar] [CrossRef]
- Ronicke, S.; Hirsch, M.C.; Türk, E.; Larionov, K.; Tientcheu, D.; Wagner, A.D. Can a Decision Support System Accelerate Rare Disease Diagnosis? Evaluating the Potential Impact of Ada DX in a Retrospective Study. Orphanet J. Rare Dis. 2019, 14, 69. [Google Scholar] [CrossRef]
- Rees, F.; Doherty, M.; Lanyon, P.; Davenport, G.; Riley, R.D.; Zhang, W.; Grainge, J.W. Early Clinical Features in Systemic Lupus Erythematosus: Can They Be Used to Achieve Earlier Diagnosis? A Risk Prediction Model. Arthritis Care Res. 2016, 69, 8334. [Google Scholar] [CrossRef]
- Pearce, F.A.; Habbard, R.B.; Grainge, M.J.; Watts, R.A.; Abhishek, A.; Lanyon, P.C. Can granulomatosis with polyangiitis be diagnosed earlier in primary care? A case-control study. QJM Int. J. Med. 2018, 111, 39–45. [Google Scholar] [CrossRef]
- Hamilton, W.; Walter, F.M.; Rubin, G.; Neal, R.D. Improving Early Diagnosis of Symptomatic Cancer. Nat. Rev. Clin. Oncol. 2016, 13, 740–749. [Google Scholar] [CrossRef]
- Graber, M.L. Progress Understanding Diagnosis and Diagnostic Errors: Thoughts at Year 10. Diagnosis 2020, 7, 151–159. [Google Scholar] [CrossRef]
- Abdellatif, A.; Bouaud, J.; Nghiem, D.; Lafuente-Lafuente, C.; Belmin, J.; Seroussi, B. Clinical Decision Support Systems in Nursing Homes: A Scoping Review. Stud. Health Technol. Inform. 2020, 270, 542–546. [Google Scholar] [PubMed]
- Boers, S.N.; Jongsma, K.R.; Lucivero, F.; Aardoom, J.; Büchner, F.L.; de Vries, M.; Honkoop, P.; Houwink, E.J.F.; Kasteleyn, M.J.; Meijer, E.; et al. SERIES: EHealth in Primary Care. Part 2: Exploring the Ethical Implications of Its Application in Primary Care Practice. Eur. J. Gen. Pract. 2020, 26, 26–32. [Google Scholar] [CrossRef] [PubMed]
- Harada, T.; Shimizu, T.; Kaji, Y.; Suyama, Y.; Matsumoto, T.; Kosaka, C.; Shimizu, H.; Nei, T.; Watanuki, S. A Perspective from a Case Conference on Comparing the Diagnostic Process: Human Diagnostic Thinking vs. Artificial Intelligence (AI) Decision Support Tools. Int. J. Environ. Res. Public Health 2020, 17, 6110. [Google Scholar] [CrossRef] [PubMed]
- van der Kleij, R.M.J.J.; Kasteleyn, M.J.; Meijer, E.; Bonten, T.N.; Houwink, E.J.F.; Teichert, M.; van Luenen, S.; Vedanthan, R.; Evers, A.; Car, J.; et al. SERIES: EHealth in Primary Care. Part 1: Concepts, Conditions and Challenges. Eur. J. Gen. Pract. 2019, 25, 179–189. [Google Scholar] [CrossRef]
- Shimizu, T. The 6C model for accurately capturing the patient’s medical history. Diagnosis 2021. [Google Scholar] [CrossRef]
- Harada, Y.; Katsukura, S.; Kawamura, R.; Shimizu, T. Efficacy of Artificial-Intelligence-Driven Differential-Diagnosis List on the Diagnostic Accuracy of Physicians: An Open-Label Randomized Controlled Study. Int. J. Environ. Res. Public Health 2021, 18, 2086. [Google Scholar] [CrossRef]


{kind=link}
| Reference | Participants | Age | Study Design | Target Disease | Process Outcome | Main Outcome | Main Observation | Significant Difference | Evaluator | Support Method |
|---|---|---|---|---|---|---|---|---|---|---|
| Rosser et al. 1991, Canada [26] | 8502 patients | Over 15 years old | Randomized controlled trials | combined outcomes | Screening rate | Rates of completion of the preventive procedures | Five screening procedures (Flu vaccine, measure blood pressure, Assess smoking status, Papanicolaou smear, Tetanus vaccine) | ○ | Physician | Reminder |
| Ornstein et al. 1991, USA [27] | 7397 patients | 40.0 ± 17.3 | Randomized controlled trials | combined outcomes | Screening rate | Adherence to preventive serivices | Five recommended preventive services (cholesterol measurements, fecal occult blood testing, mammography, Papanicolaou smears, and tetanus vaccine) | ○ | Physician | Reminder |
| McPhee et al. 1991, USA [28] | 2331 encount | No details available | Randomized controlled trials | combined outcomes | Screening rate | Rates of completion of the preventive procedures | Nine cancer prevention services and screenings (stool occult-blood test, rectal examination, pelvic examination, Papanicolaou’s smear, breast examination, smoking assessment, smoking counseling, dietary assessment, dietary counseling, sigmoidoscopy, mammography) | ○ | Physician | Reminder |
| McPhee et al. 1989, USA [29] | 1936 records | Varies by criteria | Randomized controlled trials | combined outcomes | Screening rate | Rates of completion of the cancer screening procedures | Seven cancer prevention screenings (stool occult blood test, rectal examination, sigmoidoscopy, pap smear, pelvic examination, breast examination, mammogram) | ○ | Physician | Reminder |
| McDonald et al. 1984, USA [30] | 12467 patients | No details available | Randomized controlled trials | combined outcomes | Screening rate | Response rate for reminder | Twelve actions including 5 preventive procedures (occult blood testing, mammographic screening, weight reduction diets, influenza, and pneumococcal vaccines) | ○ | Physician | Reminder |
| Hamilton et al. 2013, UK [31] | 2593 records | No details available | Nested case-control study | Lung and colorectal cancer | Screening rate and diagnosis | Diagnosis of cancer and diagnostic test | 2-week referrals for lung and colorectal cancer, requested CXR, coloscopies | ○ | Physician | Decision support system |
| Murphy et al. 2015, USA [32] | 733 records | 60.4 ± 7.4 (intervention group) | Randomized controlled trials | Lung, colorectal and prostate cancers | Time to diagnostic evaluation | Proportion and time to diagnostic evaluation of cancer | Electronic health record-based trigger (red flag criteria of colorectal, lung and prostate cancer), Proportion and time to diagnostic evaluation of cancer | ○ | Physician | E-trigger |
| Price et al. 2019, UK [33] | No details available | No details available | Cross-sectional study | Lung and colorectal cancer | Referral rate for suspected malignancy | 2-week wait referral rate | Availability and use cancer decision-support tools | × | Physician | Decision support system |
| Vetter, 2015, USA [34] | 39 records | No details available | Non-randomized controlled trials | General diagnosis | Accuracy of diagnosis | Diagnostic accuracy and clinical documentation | Chart audit tool | ○ | Nurse practitioner | Decision support system |
| Shimizu et al. 2018, Japan [35] | 100 patients | 70 ± 20.9 | Retrospective observational study | General diagnosis | Accuracy of diagnosis | Diagnostic error rate | Exposure to computor clinical decision support system | ○ | Physician | Decision support system |
| Burack et al. 1997, USA [36] | 1225 patients | Women over 40 years old | Randomized controlled trials | Breast cancer | Screening rate | Mammography rates | Mammography rates | ○ | Physician | Reminder |
| Burack et al. 1998, USA [37] | 5801 patients | Women 18–40 years old | Randomized controlled trials | Cervical cancer | Screening rate | Visitation, Pap smear | Visitation, Pap smear | × | Physician | Reminder |
| Sequist et al. 2009, USA [38] | 21860 patients | 60.3 ± 8.3 (Intervention group) | Randomized controlled trials | Colorectal cancer | Screening rate | Fecal occult blood testing, flexible sigmoidoscopy and colonoscopy | Fecal occult blood testing, flexible sigmoidoscopy, colonoscopy and detection of colorectal adenomas | ○ | Physician | Reminder |
| Litvin et al. 2016, USA [39] | No details available | Over 18 years old | Non-randomized controlled trials | Chronic kidney disease | Screening rate | CKD identification and management | Performance on chronic kidney disease clinical quality measures | ○ | Physician | Decision support system |
| Lee et al. 2007, USA [40] | 1874 encounters | 47.8 ± 17.88 (Intervention group) | Randomized controlled trials | Obesity | Diagnostic rate | Diagnostic accuracy of obesity-related diagnoses | Screening rate and diagnsis of obesity-related diagnoses | ○ | Nurse practitioner | Decision support system |
| Chaudhry et al. 2012, USA [41] | 1763 patients | Men aged 65-75 | Retrospective observational study | Abdominal aortic aneurysm | Screening rate | Screening rate of abdominal aortic aneurysm | Screening rate of abdominal aortic aneurysm | ○ | Physician | Decision support system |
| Kanealy et al. 2005, New Zealand [42] | 5628 patients | Over 50 years old | Randomized controlled trials | Diabetes | Screening rate | Screening rate of diabetes | Screening rate of diabetes | ○ | Physician | Reminder |
| Wyk et al. 2008, Netherlands [43] | 87886 patients | 43.8 ± 14.8 (intervention group) | Randomized controlled trials | Dyslipidemia | Screening rate | Screening and treated rate of dyslipidemia | Screening and treated rate of dyslipidemia | ○ | Physician | E-alert |
| Rubenstein et al. 1995, USA [44] | 557 patients | 51.4 ± 18.2 (intervention group) | Randomized controlled trials | Physical function | Functional decline | Functional Status Questionnaire | Functional Status Questionnaire and completion rate of interventions | ○ | Physician | Feedback report |
| DeJesus et al. 2012, USA [45] | 14674 patients | Women over 65 years old | Retrospective observational study | Osteoporosis | Screening rate | Completion rate of osteoporosis screening | Completion rate of osteoporosis screening, pratice rate of osteoporosis screening | ○ | Physician | Decision support system |
| DeSilva et al. 2020, USA [46] | 13707 patients | Over 12 years old | Randomized controlled trials | Hepatitis B virus infection | Screening rate | Diagnosis of chronic HBV infection | Rate of alerts opened, test order, obtain of result, positive HBV screening test | ○ | Physician | E-alert |
| Chak et al. 2018, USA [47] | 2987 patients | 38.5 ± 14.7 (intervention group) | Randomized controlled trials | Hepatitis B virus infection | Screening rate | Completion rate of hepatitis B infection screening | Completion rate of hepatitis B virus infection screening, positive rate of test | ○ | Physician | E-alert |
| Sundaram et al. 2009, USA [48] | 26042 patients | No details available | Randomized controlled trials | Human immunodeficiency virus infection | Screening rate | HIV screening rates | HIV screening rates, degree to guideline concordant, adherence to reminders, and provider attitude and knowledge. | × | Physician | Reminder |
| Miller et al. 2017, USA [49] | 19869 patients | No details available | Cross-sectional study | Depression | Screening rate | Depression screening rates | Depression screening rates, contraindications to medication, level of alert, mental health risk | ○ | Physician | Decision support system |
| Downs et al. 2006, UK [50] | 450 records | 84.9 ± 6.6 (Intervention group) | Non-randomized controlled trials | Dementia | Rates of detection of dementia | Detection rates of dementia | Detection rates of dementia, concordance with guidelines | ○ | Physician | Decision support system |
| Ahmad et al. 2009, Canada [51] | 293 patients | 43.5 ± 14.8 | Randomized controlled trials | Intimate partner violence and control | Screening rate | Initiation of discussion about risk for Intimate partner violence and control and detection of women at risk | Initiation of discussion about risk for Intimate partner violence and control and detection of women at risk | ○ | Physician | Decision support system |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Harada, T.; Miyagami, T.; Kunitomo, K.; Shimizu, T. Clinical Decision Support Systems for Diagnosis in Primary Care: A Scoping Review. Int. J. Environ. Res. Public Health 2021, 18, 8435. https://doi.org/10.3390/ijerph18168435
Harada T, Miyagami T, Kunitomo K, Shimizu T. Clinical Decision Support Systems for Diagnosis in Primary Care: A Scoping Review. International Journal of Environmental Research and Public Health. 2021; 18(16):8435. https://doi.org/10.3390/ijerph18168435
Chicago/Turabian StyleHarada, Taku, Taiju Miyagami, Kotaro Kunitomo, and Taro Shimizu. 2021. "Clinical Decision Support Systems for Diagnosis in Primary Care: A Scoping Review" International Journal of Environmental Research and Public Health 18, no. 16: 8435. https://doi.org/10.3390/ijerph18168435
APA StyleHarada, T., Miyagami, T., Kunitomo, K., & Shimizu, T. (2021). Clinical Decision Support Systems for Diagnosis in Primary Care: A Scoping Review. International Journal of Environmental Research and Public Health, 18(16), 8435. https://doi.org/10.3390/ijerph18168435