
Effects of Shift Work in a Sample of Italian Nurses: Analysis of Rest-Activity Circadian Rhythm

 ,
,  ,
,  ,
,  ,
, 

Abstract
:1. Introduction
2. Materials and Methods
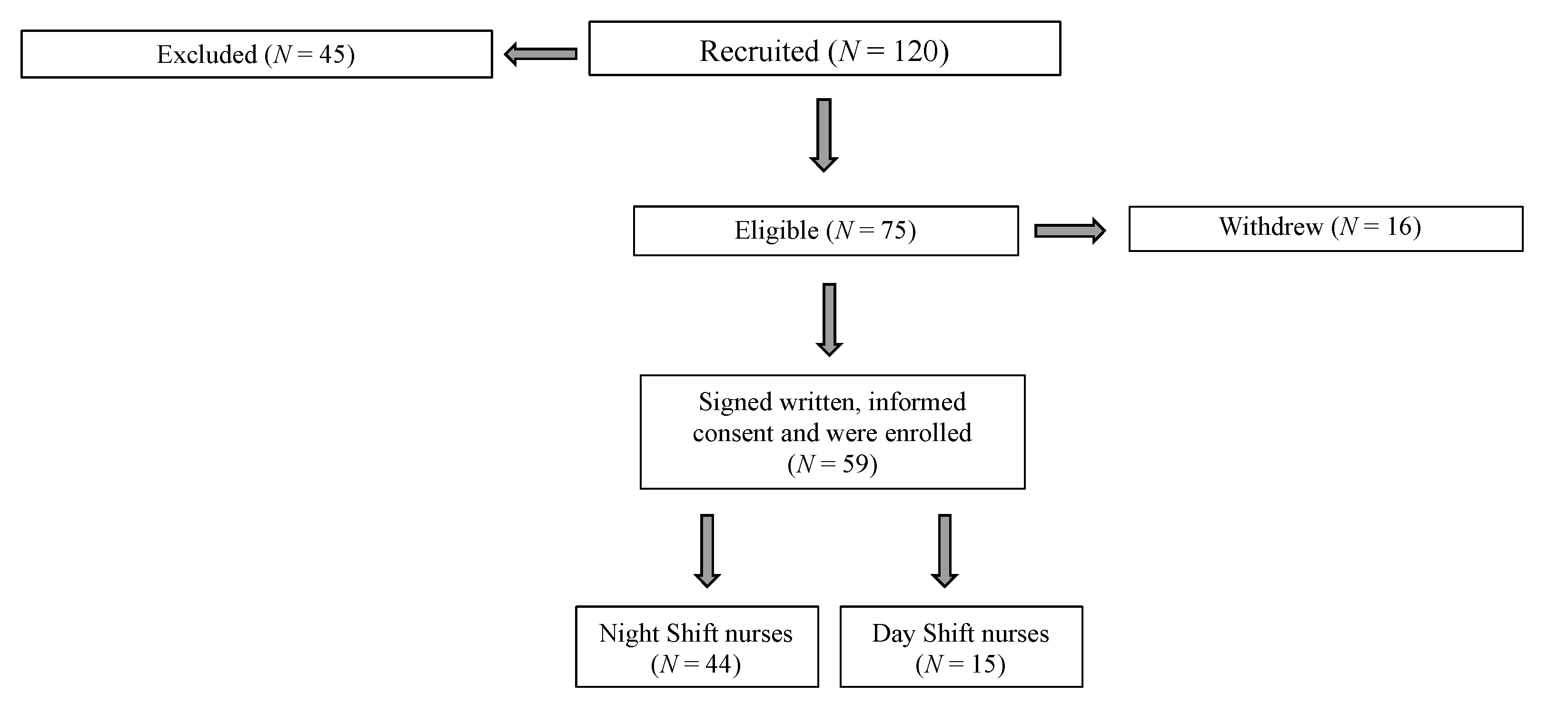
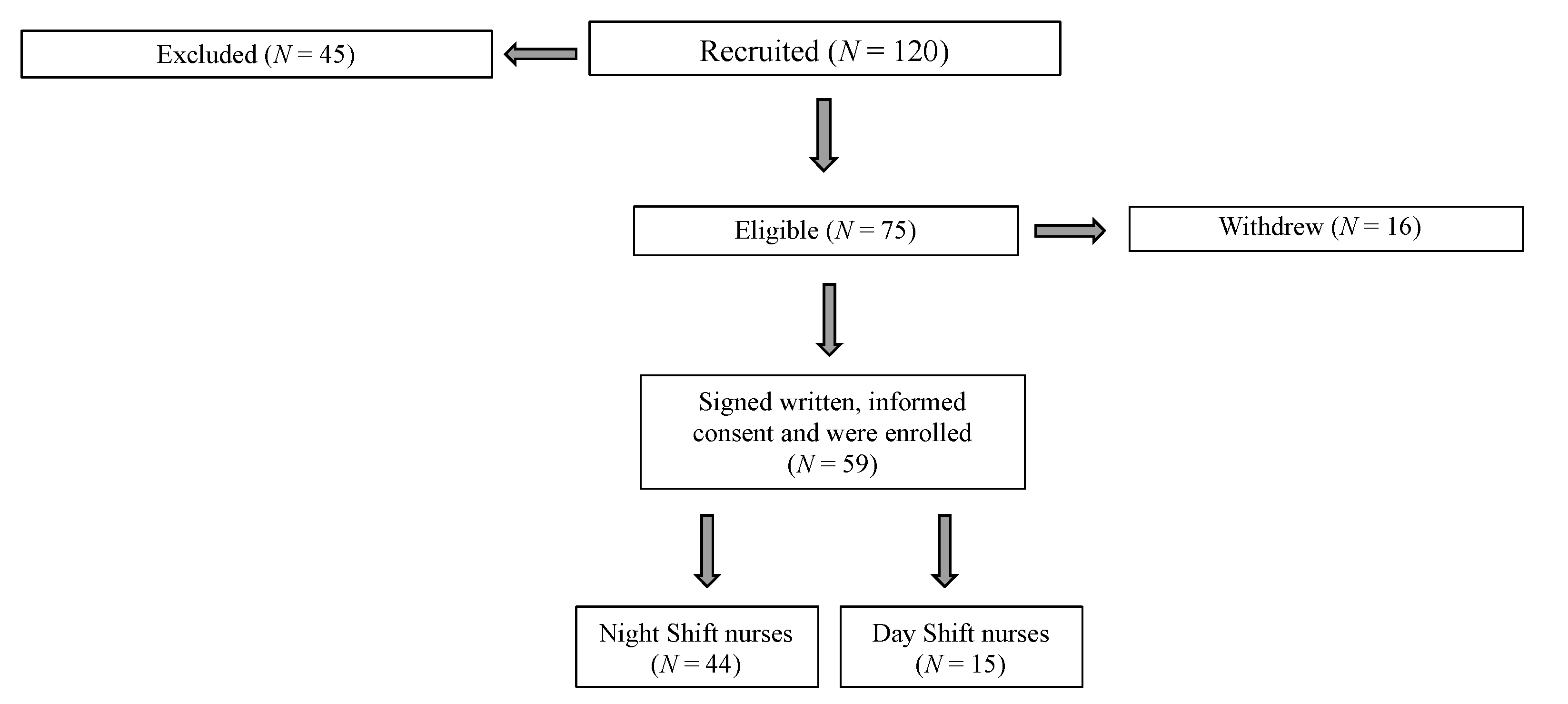
2.1. Participants
- -
- At least one year experience of shift work (day/afternoon or night) to guarantee an adaptation and synchronization to the shift by the nurses;
- -
- Willingness to perform actigraphic monitoring for 5 consecutive days and to maintain a daily diary during the period.
- -
- Cardiovascular, endocrine or neuromuscular diseases (self-reported);
- -
- Pharmacological therapy affecting sleep quality (self-reported);
- -
- Pregnancy (self-reported).
2.2. Study Design
- -
- Demographic data, health status, ongoing pharmacological therapy;
- -
- Height and body mass to calculate body mass index (BMI, kg/m2) [35];
- -
- Actigraphic monitoring to record RAR. The actigraph (MotionWatch 8®, CamNtech, Cambridge, UK) was worn on the non-dominant wrist: the participants were instructed to remove it only when bathing, showering, washing dishes or when engaging in contact or combat sports. A daily diary was provided for entering the clock time when not wearing the actigraph and napping. Based on the data recorded in the diaries, the participants removed the actigraph once a day for about 30 min on average. The time during which the device was not worn (e.g., during personal hygiene) was deleted from the data analysis.
2.3. Experimental Procedures
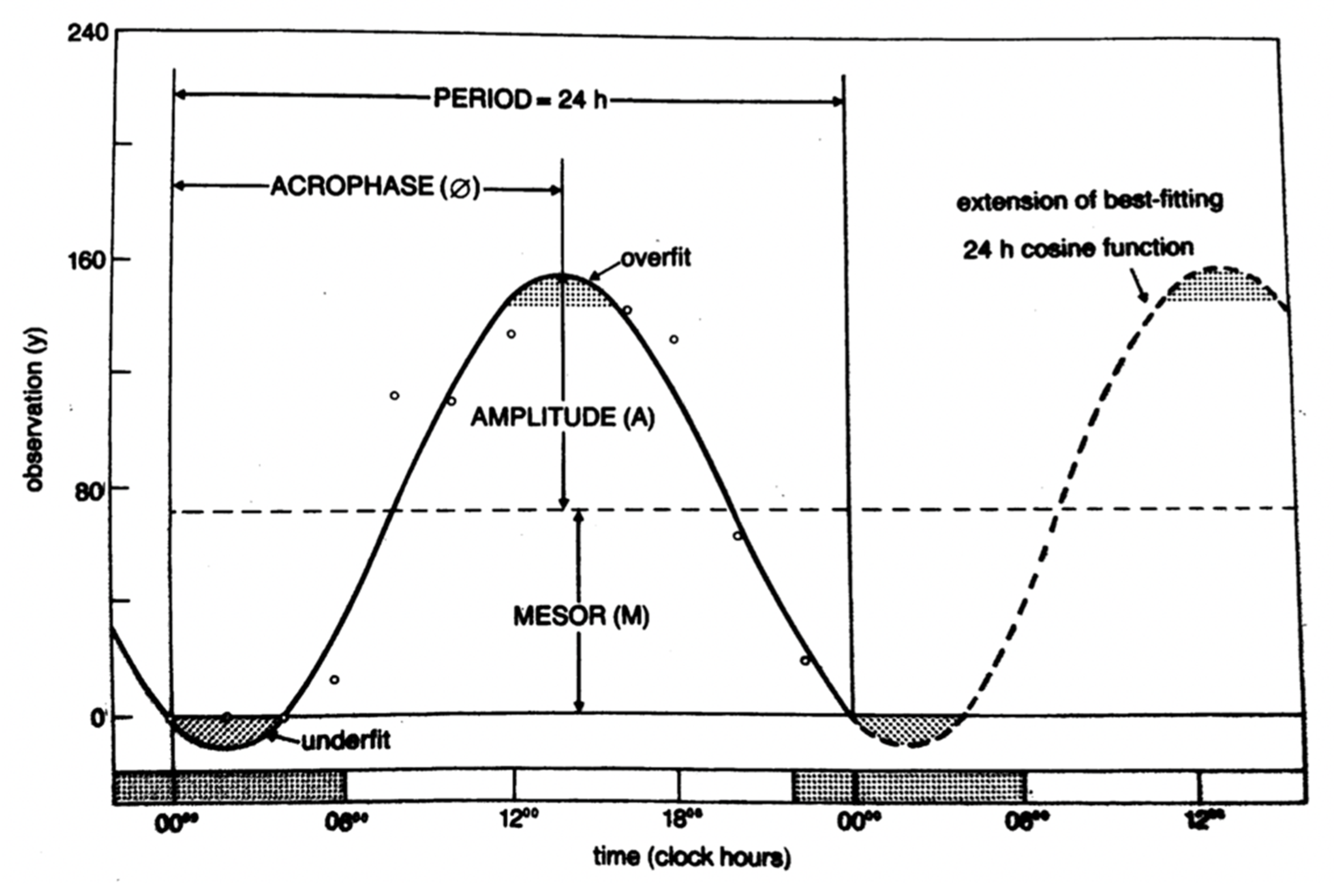
2.3.1. RAR Assessment
2.3.2. Data Processing
- -
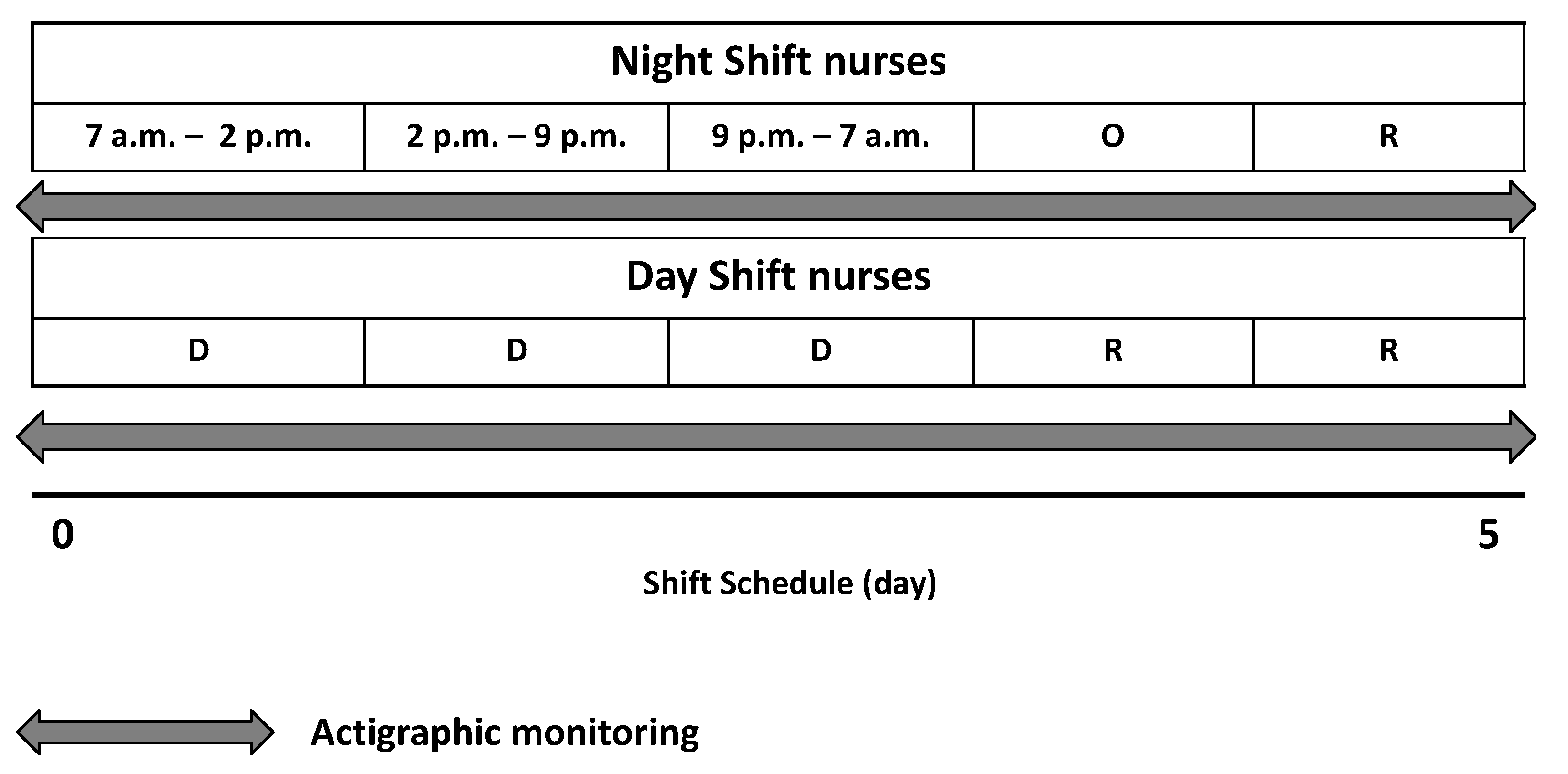
- Entire working cycle: all 5 days of working time;
- -
- Working period: day 1 (morning shift 07:00 a.m.–02:00 p.m.), day 2 (afternoon shift 02:00 p.m.–09:00 p.m.), day 3 (night shift 09:00 p.m.–07:00 a.m.) for the NS group, and the 3 consecutive workdays (morning shift 07:00 a.m.–02:00 p.m. or afternoon shift 02:00 p.m.–09:00 p.m.) for the DS group;
- -
- Rest period: day 4 (night-off) and day 5 (rest) for the NS group and the 2 consecutive rest days for the DS group.
2.4. Statistical Analysis
3. Results
3.1. Rhythmometric Analysis in Night Shift and Day Shift Nurses during the Entire Working Cycle
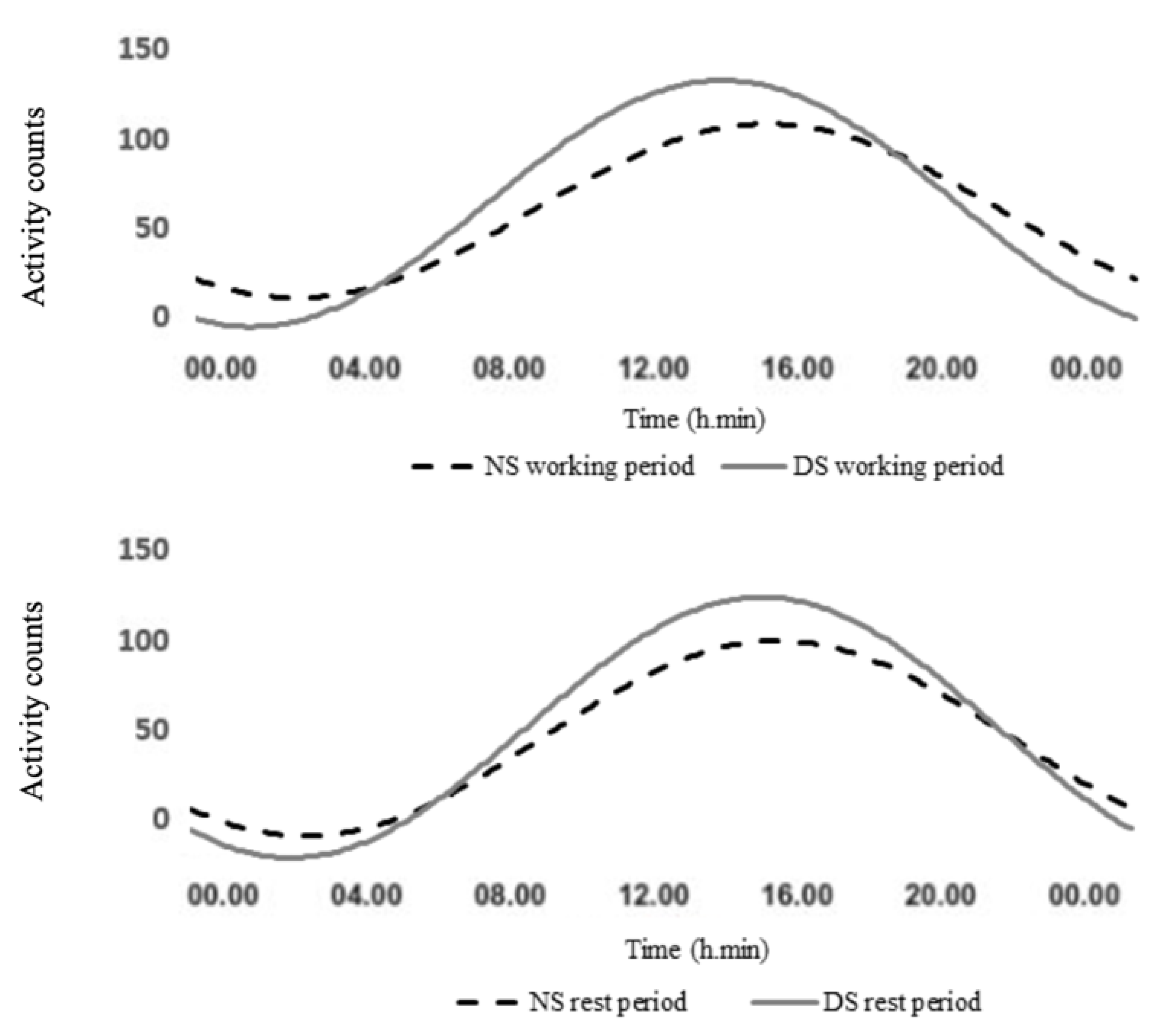
3.2. Rhythmometric Analysis in Night Shift and Day Shift Nurses during the Working Period
3.3. Rhythmometric Analysis in Night Shift and Day Shift Nurses during the Rest Period
3.4. Rhythmometric Analysis between the Working Period and the Rest Period in Night Shift and Day Shift Nurses
3.5. Rhythmometric Analysis in Normal Weight and Overweight Nurses in Relation to Work Shift during the Entire Working Cycle
3.6. Rhythmometric Analysis in Normal Weight and Overweight Nurses in Relation to Work Shift during the Working Period
3.7. Rhythmometric Analysis in Normal Weight and Overweight Nurses in Relation to Work Shift during the Rest Period
3.8. Rhythmometric Analysis between the Working Period and the Rest Period in Normal Weight and Overweight Nurses in Relation to Work Shift
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Boivin, D.B. Disturbances of hormonal circadian rhythms in shift workers. In Neuroendocrine Correlates of Sleep/Wakefulness; Cardinali, D.P., Pandi-Perumal, S.R., Eds.; Springer: Boston, MA, USA, 2006; pp. 325–354. [Google Scholar]
- Boudreau, P.; Yeh, W.H.; Dumont, G.A.; Boivin, D.B. Circadian variation of heart rate variability across sleep stages. Sleep 2013, 36, 1919–1928. [Google Scholar] [CrossRef] [Green Version]
- Sack, R.L.; Auckley, D.; Auger, R.R.; Carskadon, M.A.; Wright, K.P., Jr.; Vitiello, M.V.; Zhdanova, I.V.; American Academy of Sleep Medicine. Circadian rhythm sleep disorders: Part I, basic principles, shift work and jet lag disorders. Sleep 2007, 30, 1460–1483. [Google Scholar] [CrossRef] [Green Version]
- Sack, R.L.; Auckley, D.; Auger, R.R.; Carskadon, M.A.; Wright, K.P., Jr.; Vitiello, M.V.; Zhdanova, I.V.; American Academy of Sleep Medicine. Circadian rhythm sleep disorders: Part II, advanced sleep phase disorder, delayed sleep phase disorder, free-running disorder, and irregular sleep-wake rhythm. Sleep 2007, 30, 1484–1501. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, X.S.; Armstrong, M.E.G.; Cairns, B.J.; Key, T.J.; Travis, R.C. Shift work and chronic disease: The epidemiological evidence. Occup. Med. 2011, 61, 78–89. [Google Scholar] [CrossRef] [Green Version]
- Boivin, D.B.; Boudreau, P. Impacts of shift work on sleep and circadian rhythms. Pathol. Biol. 2014, 62, 292–301. [Google Scholar] [CrossRef]
- Saksvik, I.B.; Bjorvatn, B.; Hetland, H.; Sandal, G.M.; Pallesen, S. Individual differences in tolerance to shift work—A systematic review. Sleep Med. Rev. 2011, 15, 221–235. [Google Scholar] [CrossRef] [PubMed]
- Selvi, Y.; Özdemir, P.G.; Özdemir, O.; Aydin, A.; Beşiroğlu, L. Influence of night shift work on psychologic state and quality of life in health workers. J. Psychiatry Neurol. Sci. 2010, 23, 238–243. [Google Scholar] [CrossRef]
- Roveda, E.; Castelli, L.; Galasso, L.; Mulè, A.; Cè, E.; Condemi, V.; Banfi, G.; Montaruli, A.; Esposito, F. Differences in daytime activity levels and daytime sleep between night and day duty: An observational study in italian orthopedic nurses. Front. Physiol. 2021, 12, 628231. [Google Scholar] [CrossRef]
- Cè, E.; Doria, C.; Roveda, E.; Montaruli, A.; Galasso, L.; Castelli, L.; Mulè, A.; Longo, S.; Coratella, G.; D’Aloia, P.; et al. Reduced neuromuscular performance in night shift orthopedic nurses: New insights from a combined electromyographic and force signals approach. Front. Physiol. 2020, 11, 693. [Google Scholar] [CrossRef] [PubMed]
- Chellappa, S.L. Circadian misalignment: A biological basis for mood vulnerability in shift work. Eur. J. Neurosci. 2020, 52, 3846–3850. [Google Scholar] [CrossRef] [PubMed]
- Knutsson, A.; Bøggild, H. Gastrointestinal disorders among shift workers. Scand. J. Work Environ. Health 2010, 36, 85–95. [Google Scholar] [CrossRef] [Green Version]
- Wong, I.S.; McLeod, C.B.; Demers, P.A. Shift work trends and risk of work injury among canadian workers. Scand. J. Work Environ. Health 2011, 37, 54–61. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Khaleque, A. Sleep deficiency and quality of life of shift workers. Soc. Indic. Res. 1999, 46, 181–189. [Google Scholar] [CrossRef]
- Rajaratnam, S.M.; Arendt, J. Health in a 24-h society. Lancet 2001, 358, 999–1005. [Google Scholar] [CrossRef]
- Schernhammer, E.S.; Laden, F.; Speizer, F.E.; Willett, W.C.; Hunter, D.J.; Kawachi, I.; Colditz, G.A. Rotating night shifts and risk of breast cancer in women participating in the nurses’ health study. J. Natl. Cancer Inst. 2001, 93, 1563–1568. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cornelissen, G.; Otsuka, K. Chronobiology of aging: A mini-review. Gerontology 2017, 63, 118–128. [Google Scholar] [CrossRef]
- Abbott, S.M.; Malkani, R.G.; Zee, P.C. Circadian disruption and human health: A bidirectional relationship. Eur. J. Neurosci. 2020, 51, 567–583. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gehrman, P.; Marler, M.; Martin, J.L.; Shochat, T.; Corey-Bloom, J.; Ancoli-Israel, S. The timing of activity rhythms in patients with dementia is related to survival. J. Gerontol. A Biol. Sci. Med. Sci. 2004, 59, 1050–1055. [Google Scholar] [CrossRef] [Green Version]
- Mormont, M.C.; Waterhouse, J.; Bleuzen, P.; Giacchetti, S.; Jami, A.; Bogdan, A.; Lellouch, J.; Misset, J.L.; Touitou, Y.; Lévi, F. Marked 24-h rest/activity rhythms are associated with better quality of life, better response, and longer survival in patients with metastatic colorectal cancer and good performance status. Clin. Cancer Res. 2000, 6, 3038–3045. [Google Scholar]
- Tranah, G.J.; Waterhouse, J.; Bleuzen, P.; Giacchetti, S.; Jami, A.; Bogdan, A.; Lellouch, J.; Misset, J.L.; Touitou, Y.; Lévi, F. Circadian activity rhythms and risk of incident dementia and mild cognitive impairment in older women. Ann. Neurol. 2011, 70, 722–732. [Google Scholar] [CrossRef] [Green Version]
- Paudel, M.L.; Taylor, B.C.; Ancoli-Israel, S.; Blackwell, T.; Stone, K.L.; Tranah, G.; Redline, S.; Cummings, S.R.; Ensrud, K.E.; Osteoporotic Fractures in Men (MrOS) Study. Rest/activity rhythms and mortality rates in older men: MrOS sleep study. Chronobiol. Int. 2010, 27, 363–377. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tranah, G.J.; Blackwell, T.; Ancoli-Israel, S.; Paudel, M.L.; Ensrud, K.E.; Cauley, J.A.; Redline, S.; Hillier, T.A.; Cummings, S.R.; Stone, K.L.; et al. Circadian activity rhythms and mortality: The study of osteoporotic fractures. J. Am. Geriatr. Soc. 2010, 58, 282–291. [Google Scholar] [CrossRef]
- Hosseinabadi, M.B.; Ebrahimi, M.H.; Khanjani, N.; Biganeh, J.; Mohammadi, S.; Abdolahfard, M. The effects of amplitude and stability of circadian rhythm and occupational stress on burnout syndrome and job dissatisfaction among irregular shift working nurses. J. Clin. Nurs. 2019, 28, 1868–1878. [Google Scholar] [CrossRef]
- Rosa, D.; Terzoni, S.; Dellafiore, F.; Destrebecq, A. Systematic review of shift work and nurses’ health. Occup. Med. 2019, 69, 237–243. [Google Scholar] [CrossRef] [PubMed]
- Chang, W.P.; Li, H.B. Differences in workday sleep fragmentation, rest-activity cycle, sleep quality, and activity level among nurses working different shifts. Chronobiol. Int. 2019, 36, 1761–1771. [Google Scholar] [CrossRef]
- Nabe-Nielsen, K.; Quist, H.G.; Garde, A.H.; Aust, B. Shift work and changes in health behaviors. J. Occup. Environ. Med. 2011, 53, 1413–1417. [Google Scholar] [CrossRef] [PubMed]
- Barbadoro, P.; Santarelli, L.; Croce, N.; Bracci, M.; Vincitorio, D.; Prospero, E.; Minelli, A. Rotating shift-work as an independent risk factor for overweight italian workers: A cross-sectional study. PLoS ONE 2013, 8, e63289. [Google Scholar]
- KivimÄki, M.; Kuisma, P.; Virtanen, M.; Elovainio, M. Does shift work lead to poorer health habits? A comparison between women who had always done shift work with those who had never done shift work. Work Stress 2001, 15, 3–13. [Google Scholar] [CrossRef]
- Neil-Sztramko, S.E.; Gotay, C.C.; Demers, P.A.; Campbell, K.L. Physical activity, physical fitness, and body composition of canadian shift workers: Data from the canadian health measures survey cycles 1 and 2. J. Occup. Environ. Med. 2016, 58, 94–100. [Google Scholar] [CrossRef] [PubMed]
- Peplonska, B.; Bukowska, A.; Sobala, W. Rotating night shift work and physical activity of nurses and midwives in the cross-sectional study in Łódź, Poland. Chronobiol. Int. 2014, 31, 1152–1159. [Google Scholar] [CrossRef] [PubMed]
- Alves, M.S.; Andrade, R.Z.; Silva, G.C.; Mota, M.C.; Resende, S.G.; Teixeira, K.R.; Gonçalves, B.F.; Crispim, C.A. Social jetlag among night workers is negatively associated with the frequency of moderate or vigorous physical activity and with energy expenditure related to physical activity. J. Biol. Rhythm. 2017, 32, 83–93. [Google Scholar] [CrossRef] [PubMed]
- Loef, B.; van der Beek, A.J.; Holtermann, A.; Hulsegge, G.; van Baarle, D.; Proper, K.I. Objectively measured physical activity of hospital shift workers. Scand. J. Work Environ. Health 2018, 44, 265–273. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Costa, G. The problem: Shiftwork. Chronobiol. Int. 1997, 14, 89–98. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Obesity: Preventing and Managing the Global Epidemic; Report of a WHO Consultation; WHO Technical Report Series 894; WHO: Geneva, Switzerland, 2000. [Google Scholar]
- Halberg, F.; Carandente, F.; Cornelissen, G.; Katinas, G.S. Glossary of chronobiology. Chronobiologia 1977, 4, 1–189. [Google Scholar] [PubMed]
- Nelson, W.; Tong, L.Y.; Lee, J.K.; Halberg, F. Methods of cosinor rhythmometry. Chronobiologia 1979, 6, 305–323. [Google Scholar] [PubMed]
- Bartter, F.C.; Delea, C.S.; Baker, W.; Halberg, F.; Lee, J.K. Chronobiology in the diagnosis and treatment of mesor-hypertension. Chronobiologia 1976, 3, 199–213. [Google Scholar] [PubMed]
- Koukkari, W.L.; Halberg, F.; Gordon, S.A. Quantifying Rhythmic Movements of Albizzia julibrissin Pinnules. Plant Physiol. 1973, 51, 1084–1088. [Google Scholar] [CrossRef] [Green Version]
- Koukkari, W.L.; Duke, S.H.; Halberg, F.; Lee, J.K. Circadian rhythmic leaflet movements: Student exercise in chronobiology. Chronobiologia 1974, 1, 281–302. [Google Scholar] [PubMed]
- Halberg, F.; Reinberg, A. Circadian rhythm and low frequency rhythms in human physiology. J. Physiol. 1967, 59, 117–200. [Google Scholar]
- De Prins, J.; Cornelissen, G.; Halberg, F. Harmonic interpolation on equispaced series covering integral period of anticipated circadian rhythm in adriamycin tolerance. Chronobiologia 1977, 4, 173. [Google Scholar]
- Blume, C.; Santhi, N.; Schabus, M. “nparACT” package for R: A free software tool for the non-parametric analysis of actigraphy data. MethodsX 2016, 3, 430–435. [Google Scholar] [CrossRef] [PubMed]
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences, 2nd ed.; Academic Press: New York, NY, USA, 1977. [Google Scholar]
- Atkinson, G.; Davenne, D. Relationships between sleep, physical activity and human health. Physiol. Behav. 2007, 90, 229–235. [Google Scholar] [CrossRef] [Green Version]
- Kaliterna, L.L.; Prizmic, L.Z.; Zganec, N. Quality of life, life satisfaction and happiness in shift- and non-shiftworkers. Rev. Saude Publica 2004, 38, 3–10. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, G.; Fullick, S.; Grindey, C.; Maclaren, D.; Waterhouse, J. Exercise, energy balance and the shift worker. Sports Med. 2008, 38, 671–685. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, G.; Edwards, B.; Reilly, T.; Waterhouse, J. Exercise as a synchronizer of human circadian rhythms: An update and discussion of the methodological problems. Eur. J. Appl. Physiol. 2007, 99, 331–341. [Google Scholar] [CrossRef]
- Tevy, M.F.; Giebultowicz, J.; Pincus, Z.; Mazzoccoli, G.; Vinciguerra, M. Aging signaling pathways and circadian clock-dependent metabolic derangements. Trends Endocrinol. Metab. 2013, 24, 229–237. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Mormont, M.C.; Waterhouse, J. Contribution of the rest-activity circadian rhythm to quality of life in cancer patients. Chronobiol. Int. 2002, 19, 313–323. [Google Scholar] [CrossRef]
- Antunes, L.C.; Levandovski, R.; Dantas, G.; Caumo, W.; Hidalgo, M.P. Obesity and shift work: Chronobiological aspects. Nutr. Res. Rev. 2010, 23, 155–168. [Google Scholar] [CrossRef] [Green Version]
- Depner, C.M.; Stothard, E.R.; Wright, K.P., Jr. Metabolic consequences of sleep and circadian disorders. Curr. Diabetes Rep. 2014, 14, 507. [Google Scholar] [CrossRef] [PubMed]
- Ekmekcioglu, C.; Touitou, Y. Chronobiological aspects of food intake and metabolism and their relevance on energy balance and weight regulation. Obes. Rev. 2011, 12, 14–25. [Google Scholar] [CrossRef]
- Garaulet, M.; Gomez-Abellan, P. Timing of food intake and obesity: A novel association. Physiol. Behav. 2014, 134, 44–50. [Google Scholar] [CrossRef] [PubMed]
- McHill, A.W.; Wright, K.P., Jr. Role of sleep and circadian disruption on energy expenditure and in metabolic predisposition to human obesity and metabolic disease. Obes. Rev. 2017, 18, 15–24. [Google Scholar] [CrossRef]
- Scheer, F.A.; Hilton, M.F.; Mantzoros, C.S.; Shea, S.A. Adverse metabolic and cardiovascular consequences of circadian misalignment. Proc. Natl. Acad. Sci. USA 2009, 106, 4453–4458. [Google Scholar] [CrossRef] [Green Version]
- Garaulet, M.; Ordovas, J.M.; Madrid, J.A. The chronobiology, etiology and pathophysiology of obesity. Int. J. Obes. 2010, 34, 1667–1683. [Google Scholar] [CrossRef] [Green Version]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Group | PR (%) | p-Value | MESOR (a.c.) | Amplitude (a.c.) | Acrophase (h:min) |
|---|---|---|---|---|---|
| NS (n = 44) | |||||
| Entire working cycle | 28 | <0.001 | 113.1 ± 7.57 | 59.9 ± 6.2 a | 15:34 ± 00:48 |
| Working period | 10 | <0.001 | 122.7 ± 8.5 d | 67.5 ± 6.9 b,e | 14:32 ± 00:31 c |
| Rest period | 11 | <0.001 | 87.9 ± 8.8 d | 51.5 ± 10.5 e | 14:52 ± 01:11 |
| DS (n = 15) | |||||
| Entire working cycle | 47 | <0.001 | 120.9 ± 14.53 | 90.6 ± 14.26 a | 15:09 ± 01:25 |
| Working period | 21 | <0.001 | 128.5 ± 15.5 f | 96 ± 14.5 b,g | 13:29 ± 02:31 c |
| Rest period | 14 | <0.001 | 90.3 ± 17.1 f | 69.8 ± 20.8 g | 14:40 ± 01:22 |
| Group | PR (%) | p-Value | MESOR (a.c.) | Amplitude (a.c.) | Acrophase (h:min) |
|---|---|---|---|---|---|
| BMI < 25 kg/m2 | |||||
| Entire working cycle | |||||
| NS (n = 19) | 29 | <0.001 | 117.3 ± 12.6 | 62 ± 11 a | 15:47 ± 01:21 |
| DS (n = 9) | 51 | <0.001 | 119.8 ± 14.68 | 92 ± 16.89 a | 15:31 ± 02:07 |
| Working period | |||||
| NS (n = 19) | 11 | <0.001 | 128.3 ± 13 f | 71 ± 10.7 c | 14:39 ± 01:04 |
| DS (n = 9) | 21 | <0.001 | 126.3 ± 21.4 i | 99 ± 24.7 c | 13:35 ± 02:32 |
| Rest period | |||||
| NS (n = 19) | 11 | <0.001 | 88.1 ± 13.3 f | 52.9 ± 19.6 | 15:08 ± 01:03 |
| DS (n = 9) | 17 | <0.001 | 101.7 ± 18.3 i | 81 ± 26.8 | 14:49 ± 02:01 |
| BMI ≥ 25 kg/m2 | |||||
| Entire working cycle | |||||
| NS (n = 25) | 27 | <0.001 | 109.8 ± 9.89 | 58.4 ± 7.66 b | 15:47 ± 01:02 |
| DS (n = 6) | 41 | <0.001 | 122.5 ± 38.39 | 90 ± 33.83 b | 15:39 ± 02:14 |
| Working period | |||||
| NS (n = 25) | 10 | <0.001 | 118 ± 11.7 g | 64.7 ± 9.7 d,h | 14:25 ± 01:38 e |
| DS (n = 6) | 18 | <0.001 | 131.4 ± 37.1 l | 97.7 ± 24.7 d | 12:26 ± 02:07 e,m |
| Rest period | |||||
| NS (n = 25) | 10 | <0.001 | 87.8 ± 12.6 g | 49.8 ± 12.1 h | 14:38 ± 01:59 |
| DS (n = 6) | 11 | <0.001 | 75.2 ± 35.2 l | 55 ± 41.3 | 14:21 ± 04:59 m |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Galasso, L.; Mulè, A.; Castelli, L.; Cè, E.; Condemi, V.; Banfi, G.; Roveda, E.; Montaruli, A.; Esposito, F. Effects of Shift Work in a Sample of Italian Nurses: Analysis of Rest-Activity Circadian Rhythm. Int. J. Environ. Res. Public Health 2021, 18, 8378. https://doi.org/10.3390/ijerph18168378
Galasso L, Mulè A, Castelli L, Cè E, Condemi V, Banfi G, Roveda E, Montaruli A, Esposito F. Effects of Shift Work in a Sample of Italian Nurses: Analysis of Rest-Activity Circadian Rhythm. International Journal of Environmental Research and Public Health. 2021; 18(16):8378. https://doi.org/10.3390/ijerph18168378
Chicago/Turabian StyleGalasso, Letizia, Antonino Mulè, Lucia Castelli, Emiliano Cè, Vincenzo Condemi, Giuseppe Banfi, Eliana Roveda, Angela Montaruli, and Fabio Esposito. 2021. "Effects of Shift Work in a Sample of Italian Nurses: Analysis of Rest-Activity Circadian Rhythm" International Journal of Environmental Research and Public Health 18, no. 16: 8378. https://doi.org/10.3390/ijerph18168378
APA StyleGalasso, L., Mulè, A., Castelli, L., Cè, E., Condemi, V., Banfi, G., Roveda, E., Montaruli, A., & Esposito, F. (2021). Effects of Shift Work in a Sample of Italian Nurses: Analysis of Rest-Activity Circadian Rhythm. International Journal of Environmental Research and Public Health, 18(16), 8378. https://doi.org/10.3390/ijerph18168378