
Analysis of a Vaping-Associated Lung Injury Outbreak through Participatory Surveillance and Archival Internet Data


Abstract
1. Introduction
2. Materials and Methods
2.1. Data Sources
2.1.1. Source 1: YouVape
2.1.2. Source 2: Google Trends
2.1.3. Source 3: Reddit
2.1.4. Source 4: Bing
2.2. Analysis Overview
3. Results
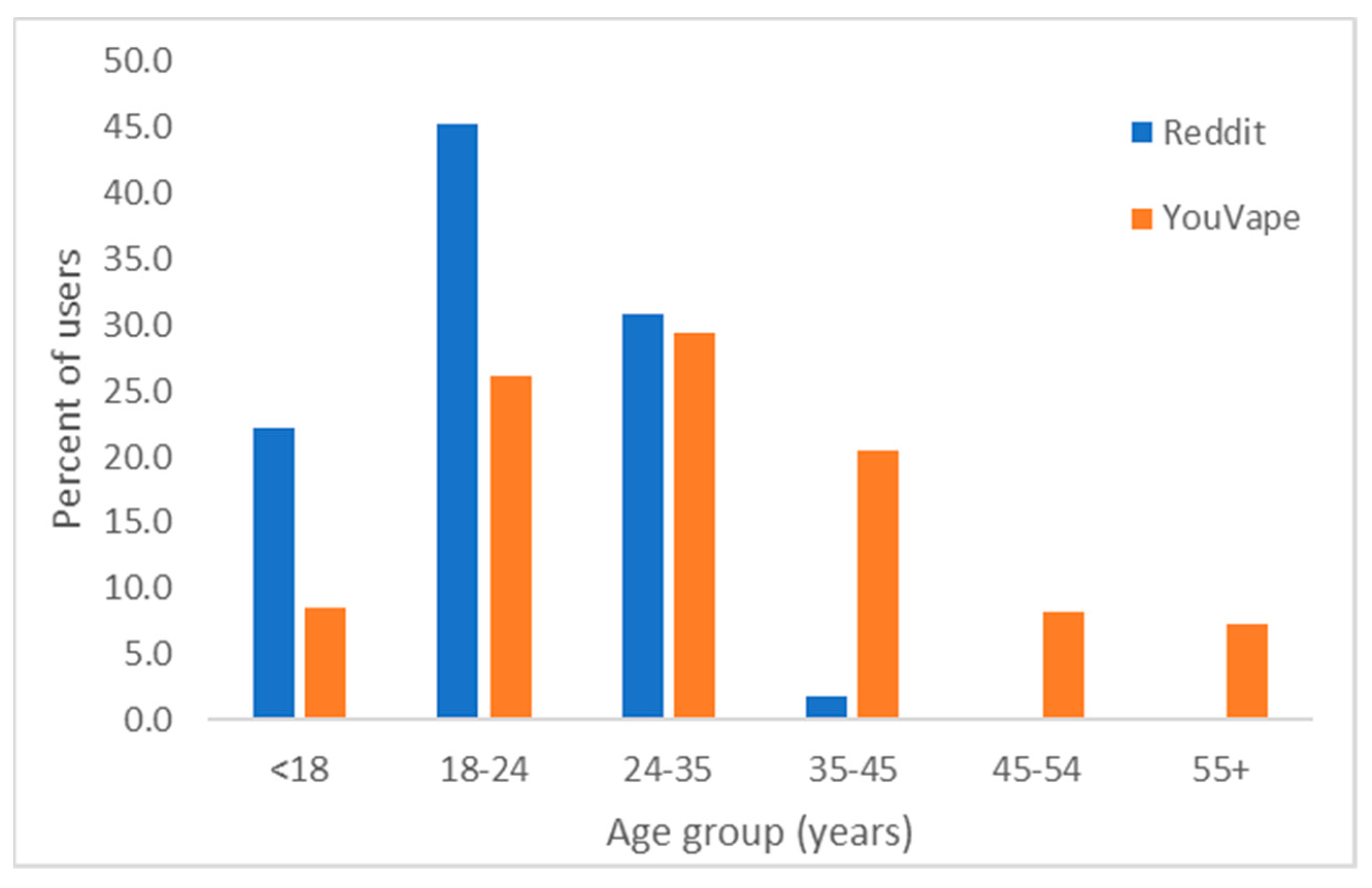
3.1. Population Statistics
3.2. Adverse Reactions to Vaping
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Appendix A. Logistic Regression Model Coefficients for Separate Ingredients and Product

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Product | Parameter | Chest Pain | Chills | Cough | Coughing Up Blood | Diarrhea | Difficulty Breathing | Feeling Tired | Fever | Nausea | Stomach Pain | Vomiting | Weight Loss |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| CBD | Age | −0.04 | −0.02 | −0.01 | −0.01 | −0.04 | −0.02 | −0.04 | −0.03 | −0.03 | −0.03 | −0.06 | −0.02 |
| Is female | −0.06 | −0.56 | −0.23 | −0.82 | 0.26 | −0.57 | −0.01 | −0.24 | −1.04 | 0.10 | 0.32 | 0.05 | |
| Duration | 0.64 | 0.50 | 0.41 | 0.36 | 0.11 | 0.79 | 0.71 | 0.27 | 0.46 | 0.55 | 0.13 | −0.07 | |
| Vape freq. | 0.61 | 0.41 | 0.21 | 0.31 | 0.19 | 0.43 | 0.59 | 0.25 | 0.57 | 0.37 | 0.06 | −0.01 | |
| R2 | 0.00 | 0.24 | 0.42 | 0.60 | 0.33 | 0.02 | 0.00 | 0.51 | 0.02 | 0.08 | 0.20 | 0.92 | |
| Flavored | Age | −0.06 * | −0.02 | −0.05 | 0.00 | −0.07 | −0.04 | −0.04 | −0.04 | −0.04 | −0.03 | −0.04 | 0.03 |
| Is female | −0.10 | −1.20 | −0.66 | −1.64 | −0.01 | −0.99 | −0.19 | −0.57 | −1.52 | −0.62 | −0.23 | −1.04 | |
| Duration | 0.48 | −0.16 | 0.10 | 0.00 | −0.44 | 0.41 | 0.22 | 0.13 | 0.02 | 0.49 | 0.14 | −0.28 | |
| Vape freq. | 0.16 | −0.30 | −0.06 | −0.50 | −0.05 | 0.07 | 0.14 | −0.21 | 0.05 | −0.03 | −0.32 | −0.36 | |
| R2 | 0.00 | 0.18 | 0.00 | 0.25 | 0.05 | 0.00 | 0.05 | 0.37 | 0.01 | 0.04 | 0.30 | 0.12 | |
| Homemade | Age | −0.01 | 0.11 | −0.02 | 0.11 | 0.01 | 0.02 | 0.00 | 0.11 | 0.02 | 0.01 | 0.05 | 0.10 |
| Is female | −2.69 | −2.33 | −2.54 | −2.33 | −1.90 | −3.10 | −2.69 | −2.33 | −1.64 | −1.69 | −1.94 | −1.54 | |
| Duration | 0.78 | −74.34 | 0.5 | −74.34 | −66.66 | 0.73 | 0.55 | −74.34 | −61.04 | −0.14 | −67.57 | −53.74 | |
| Vape freq. | −0.13 | −0.61 | 0.05 | −0.61 | 0.03 | −0.07 | 0.10 | −0.61 | 0.10 | 0.26 | −0.20 | −0.67 | |
| R2 | 0.08 | 0.1 | 0.27 | 0.10 | 0.5 | 0.08 | 0.24 | 0.10 | 0.47 | 0.73 | 0.35 | 0.05 | |
| Nicotine | Age | −0.05 * | −0.04 | −0.04 * | 0.02 | −0.04 | −0.03 | −0.03 | −0.03 | −0.04 | −0.04 | −0.06 | 0.00 |
| Is female | −0.30 | −0.65 | −0.65 | −1.39 | −0.70 | −0.57 | −0.50 | −0.59 | −1.07 * | −0.64 | −0.41 | −0.99 | |
| Duration | 0.53 * | 0.1 | 0.28 | 0.69 | 0.12 | 0.22 | 0.18 | 0.33 | 0.07 | 0.21 | 0.23 | −0.18 | |
| Vape freq. | 0.10 | −0.07 | 0.02 | −0.13 | −0.10 | −0.12 | 0.15 | 0.05 | 0.17 | 0.02 | −0.11 | −0.13 | |
| R2 | 0.00 | 0.10 | 0.00 | 0.01 | 0.02 | 0.00 | 0.00 | 0.26 | 0.00 | 0.02 | 0.08 | 0.10 | |
| Other products | Age | −0.01 | 8.89 | −0.02 | 8.89 | 0.08 | 0.12 | 25.4 | 8.89 | 0.04 | 0.09 | 0.04 | 16.83 |
| Is female | −1.16 | 105.2 | −1.02 | 105.2 | 1.94 | 2.08 | 468.66 | 105.2 | −0.29 | 1.98 | −0.29 | −45.57 | |
| Duration | 0.32 | 20.03 | 0.1 | 20.03 | −58.94 | 0.79 | 330.06 | 20.03 | −58.36 | −0.13 | −58.36 | 120.54 | |
| Vape freq. | −0.08 | −7.17 | 0.04 | −7.17 | 0.44 | 0.31 | 59.45 | −7.17 | −0.16 | 0.44 | −0.16 | −141.9 | |
| R2 | 0.95 | 0.06 | 0.99 | 0.06 | 0.44 | 0.61 | 0.00 | 0.06 | 0.52 | 0.73 | 0.52 | 0.01 | |
| THC | Age | −0.03 | −0.02 | −0.02 | 0.01 | −0.04 | −0.02 | −0.03 | −0.01 | −0.01 | −0.03 | −0.05 | 0.00 |
| Is female | 0.16 | −0.58 | −0.33 | −0.95 | 0.02 | −0.06 | −0.09 | 0.22 | −0.48 | −0.19 | 0.56 | −0.11 | |
| Duration | 0.26 | 0.3 | 0.12 | 0.32 | 0.13 | 0.52 | 0.36 | 0.18 | 0.11 | 0.05 | 0.21 | 0.30 | |
| Vape freq. | 0.22 | 0.05 | 0.11 | 0.12 | 0.18 | 0.04 | 0.27 | 0.01 | 0.22 | 0.17 | −0.23 | 0.08 | |
| R2 | 0.00 | 0.15 | 0.20 | 0.49 | 0.04 | 0.00 | 0.00 | 0.94 | 0.27 | 0.13 | 0.02 | 0.67 |
| Product | Parameter | Chest Pain | Chills | Cough | Coughing Up Blood | Diarrhea | Difficulty Breathing | Feeling Tired | Fever | Nausea | Stomach Pain | Vomiting | Weight Loss |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Blu | Age | 0.01 | 0.06 | −0.02 | 0.02 | 0.00 | 0.00 | 0.01 | 0.02 | 0.00 | −0.04 | 0.03 | −0.04 |
| Is female | 0.44 | −3.40 | 0.11 | −1.79 | −0.96 | −0.54 | −1.35 | −1.55 | −2.18 | −1.39 | −0.57 | −56.66 | |
| Duration | 0.62 | 1.17 | 0.09 | 0.45 | −0.21 | 0.74 | 0.67 | 0.50 | 0.36 | −0.15 | 0.11 | −108.33 | |
| Vape freq. | 0.20 | −0.45 | −0.50 | −0.32 | −0.09 | −0.49 | −0.23 | −0.09 | 0.10 | 0.07 | −0.17 | −54.95 | |
| R2 | 0.79 | 0.03 | 0.56 | 0.43 | 0.90 | 0.23 | 0.30 | 0.49 | 0.16 | 0.56 | 0.92 | 0.00 | |
| Brass | Age | 0.05 | 0.05 | 0.04 | 12.08 | 0.05 | 0.07 | 0.06 | 0.12 | 0.06 | 0.04 | 0.06 | 0.06 |
| knuckles | Is female | −1.61 | −1.03 | −0.26 | 120.68 | 1.21 | −0.16 | 0.64 | 0.99 | 0.60 | 0.63 | 0.97 | 0.89 |
| Duration | 0.63 | 0.11 | −0.32 | 80.05 | −0.01 | 0.54 | 0.84 | 0.68 | 0.26 | −0.03 | 0.23 | −0.39 | |
| Vape freq. | 0.10 | 0.07 | −0.19 | 0.14 | 0.15 | −0.02 | 0.22 | 0.11 | 0.40 | 0.18 | 0.25 | −0.36 | |
| R2 | 0.25 | 0.63 | 0.75 | 0.03 | 0.39 | 0.39 | 0.22 | 0.32 | 0.44 | 0.76 | 0.61 | 0.46 | |
| Cereal carts | Age | 15.67 | 24.72 | 0.34 | 24.72 | 24.72 | 0.33 | 0.37 | 24.72 | 24.72 | 5.15 | 24.72 | 3.61 |
| Is female | 454.87 | 308.89 | 10.14 | 308.89 | 308.89 | 8.37 | 9.61 | 308.89 | 308.89 | −118.46 | 308.89 | 104.09 | |
| Duration | −24.78 | 73.78 | −1.24 | 73.78 | 73.78 | −0.59 | −0.80 | 73.78 | 73.78 | 87.39 | 73.78 | −349.42 | |
| Vape freq. | 102.92 | 83.1 | 2.41 | 83.1 | 83.1 | 0.15 | 2.33 | 83.1 | 83.1 | −118.78 | 83.10 | −198.27 | |
| R2 | 0.02 | 0.01 | 0.17 | 0.01 | 0.01 | 0.12 | 0.18 | 0.01 | 0.01 | 0.00 | 0.01 | 0.03 | |
| Dank vapes | Age | 0.03 | 0.07 | 0.05 | 0.11 | 0.00 | 0.03 | 0.03 | 0.08 | 0.03 | 0.03 | 0.01 | 0.04 |
| Is female | 1.63 | 0.18 | 0.27 | 1.34 | 1.16 | 0.27 | −0.52 | 0.06 | 0.40 | 1.41 | 1.96 | 2.40 | |
| Duration | −0.26 | 0.33 | −0.50 | −69.38 | −0.17 | 0.11 | 0.61 | 0.60 | −0.21 | −0.07 | −1.1 | −0.18 | |
| Vape freq. | 0.76 | 0.34 | −0.02 | −0.35 | 0.02 | 0.29 | 0.49 | 0.10 | 0.03 | −0.13 | −0.54 | −0.02 | |
| R2 | 0.05 | 0.12 | 0.22 | 0.02 | 0.63 | 0.62 | 0.17 | 0.10 | 0.83 | 0.43 | 0.11 | 0.29 | |
| Exotics | Age | 0.03 | 0.10 | 0.03 | 8.70 | 0.05 | 0.05 | 0.13 | 0.08 | 0.08 | 0.01 | 0.00 | 0.07 |
| Is female | 2.73 | 0.09 | 1.23 | 64.73 | 0.75 | 1.99 | 3.28 | 0.63 | 0.72 | −1.53 | −2.03 | 1.06 | |
| Duration | −0.56 | −0.22 | −0.79 | −43.39 | −0.82 | −0.34 | −0.3 | −0.16 | −0.47 | −0.39 | −0.27 | −0.65 | |
| Vape freq. | 0.43 | −0.03 | 0.35 | 19.58 | 0.10 | 0.59 | 0.91 | 0.23 | 0.22 | −0.2 | −0.41 | 0.37 | |
| R2 | 0.23 | 0.41 | 0.39 | 0.01 | 0.49 | 0.51 | 0.26 | 0.70 | 0.59 | 0.65 | 0.50 | 0.56 | |
| Juul | Age | −0.04 | −0.02 | 0.00 | 0.05 | −0.01 | −0.05 | −0.03 | −0.01 | −0.06 | −0.04 | −0.01 | 0.03 |
| Is female | 0.14 | 0.01 | −0.29 | −1.25 | −0.82 | −0.07 | −0.76 | −0.17 | −0.6 | −0.47 | −0.27 | −1.07 | |
| Duration | 0.72 | 0.19 | 0.27 | 0.43 | 0.37 | 0.05 | 0.46 | 0.24 | 0.03 | 0.16 | −0.12 | −0.44 | |
| Vape freq. | 0.37 | −0.01 | 0.18 | −0.28 | 0.05 | −0.18 | 0.46 | 0.05 | 0.15 | 0.10 | −0.37 | −0.11 | |
| R2 | 0.01 | 0.90 | 0.56 | 0.14 | 0.23 | 0.03 | 0.01 | 0.96 | 0.06 | 0.32 | 0.51 | 0.12 | |
| Kingpen | Age | −0.01 | 0.08 | 0.03 | 0.3 | 0.03 | 0.04 | 0.04 | 0.17 | 0.04 | 0.02 | 0.05 | 0.04 |
| Is female | 0.51 | 0.71 | −0.49 | 6.28 | 1.14 | 0.43 | 1.32 | 2.56 | 0.19 | 0.04 | 1.13 | 0.06 | |
| Duration | 0.21 | 0.43 | −0.03 | 0.98 | 0.01 | 0.38 | 0.85 | 0.82 | 0.14 | 0.03 | 0.29 | 0.29 | |
| Vape freq. | 0.05 | −0.03 | 0.35 | 0.11 | −0.06 | 0.04 | 0.20 | 0.32 | 0.39 | −0.16 | −0.16 | 0.10 | |
| R2 | 0.84 | 0.18 | 0.53 | 0.01 | 0.67 | 0.57 | 0.06 | 0.01 | 0.58 | 0.97 | 0.64 | 0.70 | |
| Mario carts | Age | 0.07 | 0.12 | 0.12 | 0.22 | 0.17 | 0.21 | 0.1 | 0.12 | 0.12 | 0.22 | 0.12 | 0.09 |
| Is female | 2.70 | 2.34 | 7.09 | 4.27 | 4.52 | 6.78 | 3.47 | 2.34 | 2.34 | 4.21 | 2.34 | 1.80 | |
| Duration | 0.91 | 0.96 | −0.43 | 0.4 | 0.98 | −0.27 | 0.33 | 0.96 | 0.96 | 2.23 | 0.96 | −0.08 | |
| Vape freq. | 0.84 | 0.88 | 1.84 | 1.22 | 1.49 | 0.79 | 0.98 | 0.88 | 0.88 | 1.01 | 0.88 | −0.06 | |
| R2 | 0.63 | 0.40 | 0.15 | 0.20 | 0.23 | 0.16 | 0.49 | 0.40 | 0.40 | 0.09 | 0.40 | 0.74 | |
| Other | Age | −0.03 | −0.01 | −0.03 | 0.02 | −0.03 | −0.01 | −0.03 | −0.01 | −0.02 | −0.03 | −0.03 | 0.00 |
| Is female | −0.09 | −1.32 | −0.82 | −2.12 | −0.73 | −0.63 | −0.23 | −0.70 | −1.34 * | −0.83 | −0.20 | −0.41 | |
| Duration | 0.37 | 0.11 | 0.27 | 0.43 | −0.12 | 0.51 | 0.39 | 0.10 | 0.01 | −0.12 | 0.36 | 0.45 | |
| Vape freq. | 0.04 | −0.1 | −0.02 | −0.06 | 0.04 | 0.07 | 0.02 | −0.09 | 0.15 | 0.06 | −0.13 | 0.15 | |
| R2 | 0.01 | 0.02 | 0.00 | 0.00 | 0.10 | 0.00 | 0.00 | 0.54 | 0.00 | 0.08 | 0.14 | 0.21 | |
| Pax | Age | −0.01 | 0.02 | −0.02 | 0.04 | 0.01 | 0.01 | −0.03 | 0.02 | −0.03 | −0.02 | 0.02 | 0.03 |
| Is female | −0.87 | −0.59 | −2.00 | −1.01 | 0.06 | −1.84 | −1.64 | −0.59 | −1.77 | −0.89 | −0.41 | 1.69 | |
| Duration | 0.61 | 0.95 | 0.31 | 0.87 | 0.52 | 1.22 | 0.54 | 0.95 | 0.73 | 0.59 | 0.71 | 0.29 | |
| Vape freq. | 0.43 | 0.40 | 0.46 | 0.46 | 0.40 | 0.96 | 0.81 | 0.40 | 0.68 | 0.61 | 0.34 | −0.24 | |
| R2 | 0.59 | 0.41 | 0.06 | 0.48 | 0.73 | 0.06 | 0.05 | 0.41 | 0.08 | 0.29 | 0.67 | 0.39 | |
| Stiiizy | Age | 0.07 | 0.10 | 0.16 | 6.8 | 0.03 | 0.06 | 0.06 | 0.13 | 0.13 | 0.11 | 0.13 | 0.24 |
| Is female | 1.05 | −0.06 | −5.39 | −67.77 | 1.68 | −0.35 | −0.04 | 0.62 | 0.62 | −2.08 | 0.62 | −5.56 | |
| Duration | −0.05 | −0.26 | −62.64 | −2.12 | −1.27 | 0.45 | −0.22 | 0.17 | 0.17 | −63.68 | 0.17 | 1.23 | |
| Vape freq. | 0.31 | −1.07 | 0.58 | −39.8 | 0.15 | −0.51 | 0.94 | −0.81 | −0.81 | 0.33 | −0.81 | −0.38 | |
| R2 | 0.38 | 0.20 | 0.01 | 0.01 | 0.37 | 0.51 | 0.19 | 0.17 | 0.17 | 0.12 | 0.17 | 0.08 | |
| TKO | Age | −0.01 | 0.00 | 0.00 | 0.07 | 0.01 | 0.03 | 0.00 | 0.06 | 0.03 | −0.01 | 0.01 | 0.05 |
| Is female | 0.34 | −1.29 | 0.46 | −0.53 | −0.24 | 0.25 | 0.30 | −0.24 | −0.03 | −0.13 | −0.33 | −0.78 | |
| Duration | 0.37 | 0.40 | 0.34 | 0.12 | 0.15 | 0.52 | 0.80 | 0.40 | 0.65 | 0.03 | 0.26 | 0.02 | |
| Vape freq. | 0.7 | 0.01 | 0.10 | 0.03 | 0.14 | 0.63 | 0.77 | −0.13 | 0.34 | 0.00 | −0.27 | −0.02 | |
| R2 | 0.25 | 0.43 | 0.87 | 0.45 | 0.98 | 0.37 | 0.14 | 0.55 | 0.43 | 1.00 | 0.81 | 0.46 |
References
- Centers for Disease Control Outbreak of Lung Injury Associated with the Use of E-Cigarette, or Vaping, Products. Available online: https://www.cdc.gov/tobacco/basic_information/e-cigarettes/severe-lung-disease.html (accessed on 6 September 2019).
- Layden, J.E.; Ghinai, I.; Pray, I.; Kimball, A.; Layer, M.; Tenforde, M.W.; Navon, L.; Hoots, B.; Salvatore, P.P.; Elderbrook, M.; et al. Pulmonary Illness Related to E-Cigarette Use in Illinois and Wisconsin—Final Report. N. Engl. J. Med. 2020, 382, 903–916. [Google Scholar] [CrossRef]
- Cullen, K.A.; Gentzke, A.S.; Sawdey, M.D.; Chang, J.T.; Anic, G.M.; Wang, T.W.; Creamer, M.R.; Jamal, A.; Ambrose, B.K.; King, B.A. e-Cigarette Use Among Youth in the United States, 2019. JAMA 2019, 322, 2095. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, R.D.; Awopegba, A.; De León, E.; Cohen, J.E. Global approaches to regulating electronic cigarettes. Tob. Control 2017, 26, 440–445. [Google Scholar] [CrossRef] [PubMed]
- Yom-Tov, E.; Borsa, D.; Cox, I.J.; McKendry, R.A. Detecting Disease Outbreaks in Mass Gatherings Using Internet Data. J. Med. Internet Res. 2014, 16, e154. [Google Scholar] [CrossRef]
- Internet/Broadband Fact Sheet; Pew Research Center: Washington, DC, USA, 2019.
- Yom-Tov, E. Crowdsourced Health: How What You Do on the Internet Will Improve Medicine; The MIT Press: Cambridge, MA, USA, 2016; ISBN 978-0-262-03450-0. [Google Scholar]
- Giat, E.; Yom-Tov, E. Evidence From Web-Based Dietary Search Patterns to the Role of B12 Deficiency in Non-Specific Chronic Pain: A Large-Scale Observational Study. J. Med. Internet Res. 2018, 20, e4. [Google Scholar] [CrossRef]
- Yom-Tov, E.; Lev-Ran, S. Adverse Reactions Associated With Cannabis Consumption as Evident From Search Engine Queries. JMIR Public Health Surveill. 2017, 3, e77. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Kou, S.C.; Lu, F.; Brownstein, J.S.; Brooke, N.; Santillana, M. Advances in using Internet searches to track dengue. PLoS Comput. Biol. 2017, 13, e1005607. [Google Scholar] [CrossRef]
- Lazer, D.; Kennedy, R.; King, G.; Vespignani, A. Google Flu Trends Still Appears Sick: An Evaluation of the 2013–2014 Flu Season. SSRN Electron. J. 2014. [Google Scholar] [CrossRef]
- Lampos, V.; Miller, A.C.; Crossan, S.; Stefansen, C. Advances in nowcasting influenza-like illness rates using search query logs. Sci. Rep. 2015, 5, 12760. [Google Scholar] [CrossRef]
- Yom-Tov, E. Predicting Drug Recalls from Internet Search Engine Queries These findings suggest that aggregated Internet search engine data can be used to facilitate in early warning of faulty batches of medicines. IEEE J. Transl. Eng. Health Med. 2017, 5, 1–6. [Google Scholar] [CrossRef]
- Costello, K.L.; Martin, J.D.; Edwards Brinegar, A. Online disclosure of illicit information: Information behaviors in two drug forums. J. Assoc. Inf. Sci. Technol. 2017, 68, 2439–2448. [Google Scholar] [CrossRef]
- Bajardi, P.; Vespignani, A.; Funk, S.; Eames, K.T.; Edmunds, W.J.; Turbelin, C.; Debin, M.; Colizza, V.; Smallenburg, R.; Koppeschaar, C.E.; et al. Determinants of Follow-Up Participation in the Internet-Based European Influenza Surveillance Platform Influenzanet. J. Med. Internet Res. 2014, 16, e78. [Google Scholar] [CrossRef] [PubMed]
- Guerrisi, C.; Turbelin, C.; Blanchon, T.; Hanslik, T.; Bonmarin, I.; Levy-Bruhl, D.; Perrotta, D.; Paolotti, D.; Smallenburg, R.; Koppeschaar, C.; et al. Participatory Syndromic Surveillance of Influenza in Europe. J. Infect. Dis. 2016, 214, S386–S392. [Google Scholar] [CrossRef]
- Carlson, S.J.; Durrheim, D.N.; Dalton, C.B. Flutracking provides a measure of field influenza vaccine effectiveness, Australia, 2007–2009. Vaccine 2010, 28, 6809–6810. [Google Scholar] [CrossRef]
- Wójcik, O.P.; Brownstein, J.S.; Chunara, R.; Johansson, M.A. Public health for the people: Participatory infectious disease surveillance in the digital age. Emerg. Themes Epidemiol. 2014, 11, 7. [Google Scholar] [CrossRef]
- Smolinski, M.S.; Crawley, A.W.; Baltrusaitis, K.; Chunara, R.; Olsen, J.M.; Wójcik, O.; Santillana, M.; Nguyen, A.; Brownstein, J.S. Flu Near You: Crowdsourced Symptom Reporting Spanning 2 Influenza Seasons. Am. J. Public Health 2015, 105, 2124–2130. [Google Scholar] [CrossRef]
- Visweswaran, S.; Colditz, J.B.; O’Halloran, P.; Han, N.-R.; Taneja, S.B.; Welling, J.; Chu, K.-H.; Sidani, J.E.; Primack, B.A. Machine Learning Classifiers for Twitter Surveillance of Vaping: Comparative Machine Learning Study. J. Med. Internet Res. 2020, 22, e17478. [Google Scholar] [CrossRef]
- Allem, J.-P.; Ferrara, E.; Uppu, S.P.; Cruz, T.B.; Unger, J.B. E-Cigarette Surveillance With Social Media Data: Social Bots, Emerging Topics, and Trends. JMIR Public Health Surveill. 2017, 3, e98. [Google Scholar] [CrossRef]
- Li, Q.; Wang, C.; Liu, R.; Wang, L.; Zeng, D.D.; Leischow, S.J. Understanding Users’ Vaping Experiences from Social Media: Initial Study Using Sentiment Opinion Summarization Techniques. J. Med. Internet Res. 2018, 20, e252. [Google Scholar] [CrossRef] [PubMed]
- Huang, J.; Kornfield, R.; Emery, S.L. 100 Million Views of Electronic Cigarette YouTube Videos and Counting: Quantification, Content Evaluation, and Engagement Levels of Videos. J. Med. Internet Res. 2016, 18, e67. [Google Scholar] [CrossRef]
- Wang, L.; Zhan, Y.; Li, Q.; Zeng, D.; Leischow, S.; Okamoto, J. An Examination of Electronic Cigarette Content on Social Media: Analysis of E-Cigarette Flavor Content on Reddit. Int. J. Environ. Res. Public. Health 2015, 12, 14916–14935. [Google Scholar] [CrossRef]
- Meacham, M.C.; Vogel, E.A.; Thrul, J. Vaping-Related Mobile Apps Available in the Google Play Store After the Apple Ban: Content Review. J. Med. Internet Res. 2020, 22, e20009. [Google Scholar] [CrossRef] [PubMed]
- Chen, L.; Lu, X.; Yuan, J.; Luo, J.; Luo, J.; Xie, Z.; Li, D. A Social Media Study on the Associations of Flavored Electronic Cigarettes With Health Symptoms: Observational Study. J. Med. Internet Res. 2020, 22, e17496. [Google Scholar] [CrossRef]
- Perrine, C.G.; Pickens, C.M.; Boehmer, T.K.; King, B.A.; Jones, C.M.; DeSisto, C.L.; Duca, L.M.; Lekiachvili, A.; Kenemer, B.; Shamout, M.; et al. Characteristics of a Multistate Outbreak of Lung Injury Associated with E-cigarette Use, or Vaping—United States, 2019. MMWR Morb. Mortal. Wkly. Rep. 2019, 68, 860–864. [Google Scholar] [CrossRef]
- Alexander, L.E.C.; Bellinghausen, A.L.; Eakin, M.N. What are the mechanisms underlying vaping-induced lung injury? J. Clin. Invest. 2020, 130, 2754–2756. [Google Scholar] [CrossRef]
- Triantafyllou, G.A.; Tiberio, P.J.; Zou, R.H.; Lamberty, P.E.; Lynch, M.J.; Kreit, J.W.; Gladwin, M.T.; Morris, A.; Chiarchiaro, J. Vaping-associated Acute Lung Injury: A Case Series. Am. J. Respir. Crit. Care Med. 2019, 200, 1430–1431. [Google Scholar] [CrossRef] [PubMed]
- Butt, Y.M.; Smith, M.L.; Tazelaar, H.D.; Vaszar, L.T.; Swanson, K.L.; Cecchini, M.J.; Boland, J.M.; Bois, M.C.; Boyum, J.H.; Froemming, A.T.; et al. Pathology of Vaping-Associated Lung Injury. N. Engl. J. Med. 2019, 381, 1780–1781. [Google Scholar] [CrossRef] [PubMed]
- Hall, W.; Gartner, C.; Bonevski, B. Lessons from the public health responses to the US outbreak of vaping-related lung injury. Addiction 2021, 116, 985–993. [Google Scholar] [CrossRef]
- Yom-Tov, E.; Gabrilovich, E. Postmarket Drug Surveillance Without Trial Costs: Discovery of Adverse Drug Reactions Through Large-Scale Analysis of Web Search Queries. J. Med. Internet Res. 2013, 15, e124. [Google Scholar] [CrossRef] [PubMed]
- Oren, E.; Frere, J.; Yom-Tov, E.; Yom-Tov, E. Respiratory syncytial virus tracking using internet search engine data. BMC Public Health 2018, 18, 445. [Google Scholar] [CrossRef] [PubMed]
- Pray, I.W.; Atti, S.K.; Tomasallo, C.; Meiman, J.G. E-cigarette, or Vaping, Product Use–Associated Lung Injury Among Clusters of Patients Reporting Shared Product Use—Wisconsin, 2019. MMWR Morb. Mortal. Wkly. Rep. 2020, 69, 236–240. [Google Scholar] [CrossRef] [PubMed]
- Lozier, M.J.; Wallace, B.; Anderson, K.; Ellington, S.; Jones, C.M.; Rose, D.; Baldwin, G.; King, B.A.; Briss, P.; Mikosz, C.A.; et al. Update: Demographic, Product, and Substance-Use Characteristics of Hospitalized Patients in a Nationwide Outbreak of E-cigarette, or Vaping, Product Use–Associated Lung Injuries—United States, December 2019. MMWR Morb. Mortal. Wkly. Rep. 2019, 68, 1142–1148. [Google Scholar] [CrossRef] [PubMed]
- Navon, L.; Jones, C.M.; Ghinai, I.; King, B.A.; Briss, P.A.; Hacker, K.A.; Layden, J.E. Risk Factors for E-Cigarette, or Vaping, Product Use–Associated Lung Injury (EVALI) Among Adults Who Use E-Cigarette, or Vaping, Products—Illinois, July–October 2019. MMWR Morb. Mortal. Wkly. Rep. 2019, 68, 1034–1039. [Google Scholar] [CrossRef]
- Centers for Disease Control For Healthcare Providers. Available online: https://www.cdc.gov/tobacco/basic_information/e-cigarettes/severe-lung-disease/healthcare-providers/index.html (accessed on 25 February 2020).
- Siegel, D.A.; Jatlaoui, T.C.; Koumans, E.H.; Kiernan, E.A.; Layer, M.; Cates, J.E.; Kimball, A.; Weissman, D.N.; Petersen, E.E.; Reagan-Steiner, S.; et al. Update: Interim Guidance for Health Care Providers Evaluating and Caring for Patients with Suspected E-cigarette, or Vaping, Product Use Associated Lung Injury—United States, October 2019. MMWR Morb. Mortal. Wkly. Rep. 2019, 68, 919–927. [Google Scholar] [CrossRef] [PubMed]
- Pelleg, D.; Yom-Tov, E.; Maarek, Y. Can You Believe an Anonymous Contributor? On Truthfulness in Yahoo! Answers; IEEE: Piscataway, NJ, USA, 2012; pp. 411–420. [Google Scholar]
- Gentzkow, M.; Shapiro, J.M. Ideological Segregation Online and Offline. Q. J. Econ. 2011, 126, 1799–1839. [Google Scholar] [CrossRef]




| Source | Number of Users | Date Range | Source Type |
|---|---|---|---|
| YouVape | 720 | 29 October 2019—25 January 2020 | Participatory, online digital cohort |
| Google Trends | Unknown | 1 January 2018—31 December 2019 | Web search, aggregate |
| Bing | 1.03 M (vaping group), 3.2 M (control group) | 1 October 2018—30 June 2019 | Web search, anonymous individuals |
| 4331 | 1 January 2015—31 December 2019 | Social media, anonymous individuals |
| Chest Pain | Chills | Cough | Coughing Up Blood | Diarrhea | Difficulty Breathing | Feeling Tired | Fever | Nausea | Stomach Pain | Vomiting | Weight Loss | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Age | 0.96 * | 0.97 | 0.98 | 1.01 | 0.96 * | 0.98 | 0.97 * | 0.97 | 0.97 | 0.96 * | 0.94 * | 0.99 |
| Is female | 0.83 | 0.51 | 0.60 | 0.23 | 0.63 | 0.69 | 0.80 | 1.01 | 0.46 | 0.63 | 1.19 | 0.78 |
| Duration | 1.48 * | 1.14 | 1.21 | 1.97 | 1.11 | 1.48 * | 1.31 | 1.20 | 1.07 | 1.13 | 1.28 | 1.34 |
| Vape freq. | 1.21 | 1.07 | 1.01 | 1.04 | 1.12 | 1.05 | 1.28 * | 1.11 | 1.27 | 1.07 | 0.91 | 1.12 |
| CBD | 1.39 | 2.12 | 1.02 | 10.70 * | 1.35 | 1.11 | 1.38 | 3.82 * | 1.65 | 2.16 | 2.53 | 2.39 |
| Flavored | 0.79 | 0.71 | 0.72 | 0.31 | 0.87 | 0.80 | 0.98 | 0.96 | 0.93 | 1.21 | 1.12 | 0.78 |
| Homemade | 0.83 | 0.73 | 0.81 | 5.37 | 0.80 | 0.63 | 0.62 | 0.79 | 0.91 | 1.02 | 1.46 | 0.95 |
| Nicotine | 1.04 | 0.68 | 1.45 | 5.81 | 1.02 | 1.22 | 0.77 | 0.80 | 0.82 | 1.32 | 0.63 | 1.05 |
| Other | 2.12 | 1.99 | 1.97 | 1.54 | 4.39 | 1.48 | 1.62 | 2.25 | 2.27 | 3.16 | 3.86 | 3.86 |
| THC | 1.20 | 1.57 | 1.72 | 1.11 | 2.46 * | 1.62 | 1.42 | 1.00 | 1.88 | 2.10 | 2.61 | 1.82 |
| Model R2 | 0.06 | 0.03 | 0.04 | 0.12 | 0.03 | 0.04 | 0.05 | 0.02 | 0.04 | 0.05 | 0.05 | 0.03 |
| Model p-value | <10−4 | 0.0002 | <10−4 | 0.0001 | 0.0002 | <10−4 | <10−4 | 0.0536 | 0.0001 | <10−4 | <10−4 | 0.0027 |
| Age | 0.97 * | 0.98 | 0.99 | 1.01 | 0.98 | 0.98 | 0.98 | 0.98 | 0.98 | 0.97 | 0.95 | 1.00 |
| Is female | 0.81 | 0.40 * | 0.63 | 0.20 | 0.55 | 0.66 | 0.74 | 0.86 | 0.42 * | 0.61 | 0.87 | 0.62 |
| Duration | 1.43 * | 1.14 | 1.25 | 1.80 | 1.07 | 1.51 * | 1.36 | 1.30 | 1.13 | 1.13 | 1.34 | 1.31 |
| Vape freq. | 1.16 | 0.97 | 0.97 | 0.86 | 1.05 | 1.02 | 1.21 | 1.01 | 1.12 | 0.99 | 0.79 | 1.03 |
| blu | 1.54 | 1.42 | 1.48 | 10.07 | 1.65 | 1.32 | 1.62 | 2.05 | 1.90 | 1.95 | 2.64 | 1.82 |
| Brass knuckles | 2.69 | 2.34 | 3.00 | 1.46 | 2.77 | 2.48 | 1.02 | 0.98 | 2.23 | 1.73 | 1.04 | 2.51 |
| Cereal carts | 1.00 | 0.93 | 0.74 | 4.44 | 0.38 | 0.92 | 0.45 | 1.20 | 0.80 | 2.12 | 1.05 | 1.51 |
| Dank vape | 2.72 | 1.31 | 2.18 | 4.66 | 1.82 | 1.70 | 2.32 | 1.86 | 3.78 * | 2.69 | 2.29 | 0.95 |
| exotics | 2.41 | 0.23 | 0.32 | 0.00 | 0.68 | 0.68 | 0.35 | 0.53 | 0.23 | 0.46 | 0.73 | 0.72 |
| Juul | 1.45 | 0.90 | 2.39 | 4.06 | 1.08 | 1.65 | 1.04 | 2.48 | 1.86 | 2.39 | 1.42 | 1.14 |
| kingpen | 0.97 | 1.32 | 0.98 | 0.07 | 1.28 | 1.40 | 1.92 | 0.70 | 0.71 | 0.58 | 0.92 | 1.32 |
| Mario carts | 0.98 | 5.75 | 4.31 * | 107.77 | 3.06 | 3.03 | 2.20 | 6.62 | 3.13 | 2.29 | 3.94 | 5.87 |
| Other | 0.67 | 0.68 | 1.05 | 9.12 | 0.88 | 1.02 | 1.01 | 1.55 | 1.73 | 1.32 | 1.93 | 1.26 |
| Pax | 0.30 | 0.76 | 1.09 | 2.66 | 0.79 | 0.42 | 0.76 | 1.67 | 1.55 | 1.49 | 1.70 | 1.49 |
| Stiiizy | 0.55 | 1.27 | 0.61 | 0.86 | 1.93 | 1.46 | 1.46 | 1.17 | 0.44 | 0.68 | 0.99 | 1.22 |
| TKO | 1.63 | 2.80 | 0.93 | 8.58 | 3.06 | 0.90 | 1.73 | 1.99 | 2.51 | 4.44 * | 4.01 | 0.93 |
| Model R2 | 0.10 | 0.06 | 0.07 | 0.28 | 0.06 | 0.06 | 0.05 | 0.08 | 0.07 | 0.08 | 0.09 | 0.03 |
| Model p-value | <10−4 | 0.0004 | <10−4 | <10−4 | 0.0001 | <10−4 | <10−4 | 0.0417 | <10−4 | <10−4 | 0.0003 | 0.0389 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hswen, Y.; Yom-Tov, E. Analysis of a Vaping-Associated Lung Injury Outbreak through Participatory Surveillance and Archival Internet Data. Int. J. Environ. Res. Public Health 2021, 18, 8203. https://doi.org/10.3390/ijerph18158203
Hswen Y, Yom-Tov E. Analysis of a Vaping-Associated Lung Injury Outbreak through Participatory Surveillance and Archival Internet Data. International Journal of Environmental Research and Public Health. 2021; 18(15):8203. https://doi.org/10.3390/ijerph18158203
Chicago/Turabian StyleHswen, Yulin, and Elad Yom-Tov. 2021. "Analysis of a Vaping-Associated Lung Injury Outbreak through Participatory Surveillance and Archival Internet Data" International Journal of Environmental Research and Public Health 18, no. 15: 8203. https://doi.org/10.3390/ijerph18158203
APA StyleHswen, Y., & Yom-Tov, E. (2021). Analysis of a Vaping-Associated Lung Injury Outbreak through Participatory Surveillance and Archival Internet Data. International Journal of Environmental Research and Public Health, 18(15), 8203. https://doi.org/10.3390/ijerph18158203