
A Virtual Reality-Based Self-Help Intervention for Dealing with the Psychological Distress Associated with the COVID-19 Lockdown: An Effectiveness Study with a Two-Week Follow-Up

 ,
, 
 ,
,  , and
, and
Abstract
:1. Introduction
2. Materials and Methods
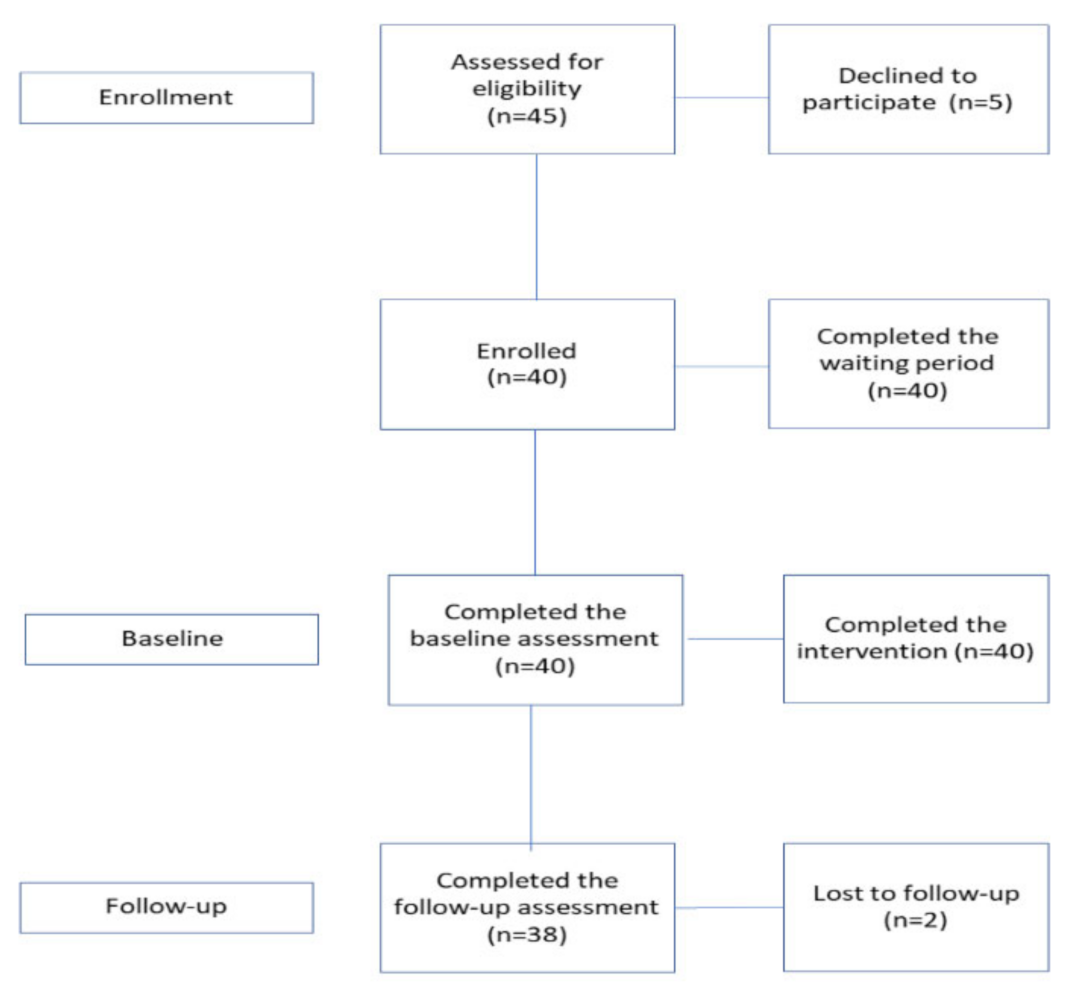
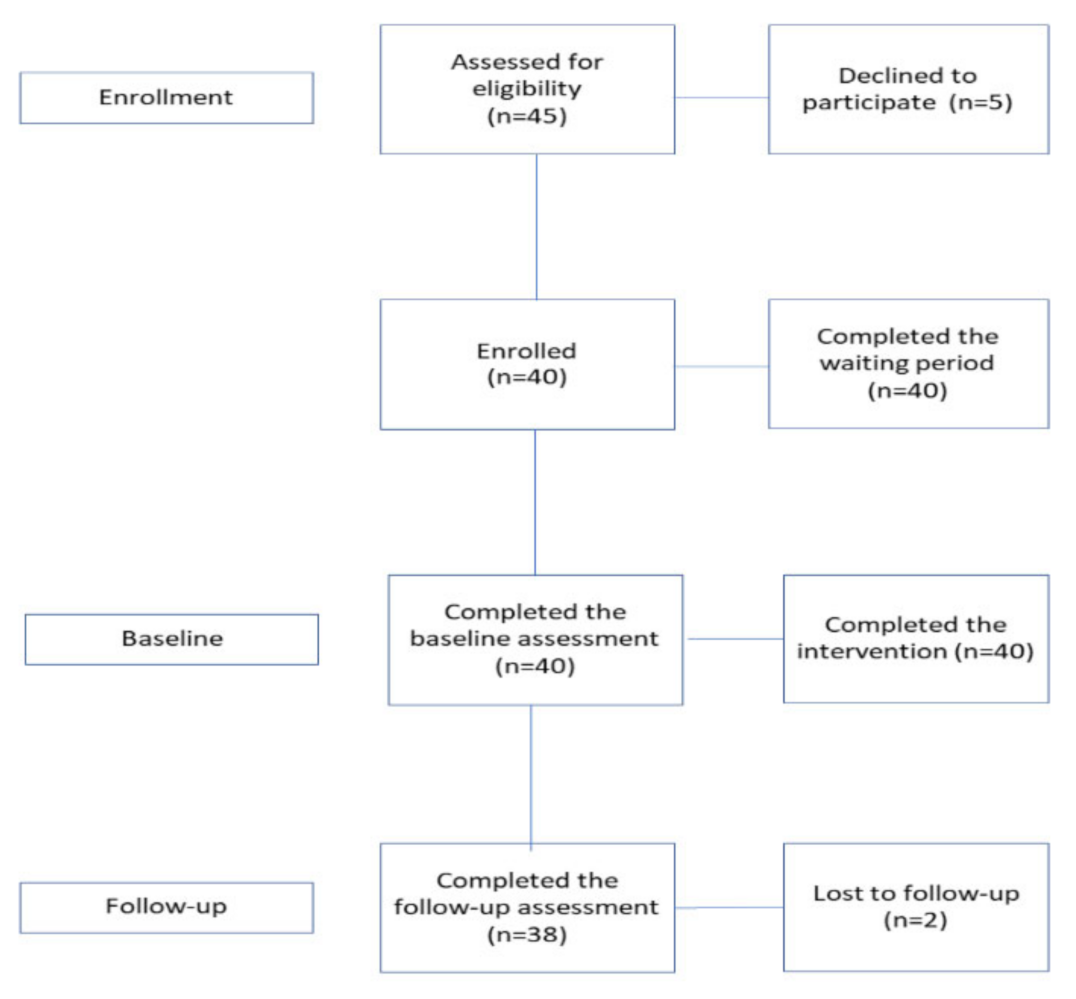
2.1. Recruitment and Experimental Design
2.2. Treatment Protocol
- Day 1: Support to cope with stress, negative intrusive thoughts, worries related to the COVID-19 pandemic;
- Day 2: Increase in self-esteem;
- Day 3: Promotion in the use of autobiographical memories to create a stable representation of themselves over time, as well as increase intimacy and connectedness by sharing personal memories;
- Day 4: Enhanced sense of community;
- Day 5: Promotion in conscious self-regulation and self-organisation of life goals;
- Day 6: Increase in empathy;
- Day 7: Support a long-term positive psychological change.
2.3. Outcome Measures
2.3.1. Primary Outcome Measure
- Depression Anxiety Stress Scale (DASS-21) [60,61]: The DASS-21 is the short version of the original self-report questionnaire developed and validated by Lovibond et al. [60] to evaluate depression, anxiety, and stress symptoms. It is composed of 21 items, with 7 items per subscale, namely, (1) DASS-21 Depression, a specific subscale for assessing depressed mood and absence of positive emotions (e.g., ‘I could not seem to experience any positive feeling at all’); (2) DASS-21 Anxiety, a specific subscale for evaluating anxiety feelings and somatic tension and (e.g., ‘I was aware of the dryness of my mouth’); (3) DASS-21 Stress, a specific subscale for evaluating somatic stress, with a focus on difficulty relaxing and irritability; (e.g., ‘I found it hard to wind down’). Participants are asked to score every item on a scale from 0 (‘did not apply to me at all’) to 3 (‘applied to me very much’). Sum scores are computed by adding up the scores on the items for each subscale the three subscales (DASS-21_Depression, DASS-21_Anxiety, DASS-21_Stress), and multiplying them by 2, but it is also possible to compute a composite score of ‘General Distress’ resulting from the sum of all items. Accordingly, total scale scores may range between 0 and 63 and subscales may range between 0 and 42.
- Perceived Stress Scale (PSS) [62,63]: The PSS is a self-report questionnaire for evaluating individuals’ perceived stress. The scale is composed of 10 items on a 5-point Likert, and it measures to what extent our daily experiences are subjectively perceived as stressful in the last month (e.g., ‘How often you have been upset because of something that happened unexpectedly?’) For the current study, it was adapted to evaluate the perceived level of stress in the last week. It yields a composite score of perceived stress resulting from the sum of the responses of single items, from 0 to 40.
- Beck Hopelessness Scale (BHS) [64,65]: The BHS is a self-report questionnaire for measuring pessimistic thoughts or negative attitudes toward the future in three different life spheres: feelings about the future, loss of motivation, and general expectations. It is composed of 20 true–false items. The total sum score can range from 1 to 20, with higher scores underscoring higher levels of hopelessness.
2.3.2. Secondary Outcome Measures
- Social Connectedness Scale (SCS) [66,67]: The SCS is a self-report instrument that measures the extent to which the individual feels connected to other persons or the social context. The scale is composed of 8 items on a 6-point Likert scale. Sum scores can range from 0 to 48, with higher scores indicating a higher sense of social connectedness.
- Fear of Coronavirus (FCOR) [68,69]: FCOR is a scale aimed at measuring the level of fear experienced during the COVID-19 pandemic (‘I am most afraid of coronavirus-19’). FCOR is composed of 8 items on a 5-point scale. Sum scores can range from 0 to 40, with higher scores indicating higher fear of COVID-19.
2.3.3. State Outcome Measures
- State–Trait Anxiety Inventory (STAI) [70,71]: The STAI is a 40-item self-report questionnaire on a 4-point Likert scale where participants are asked to evaluate both state and trait levels of anxiety. This questionnaire is divided into 20 items that refer to state anxiety (STAI-S), and 20 items that refer to trait anxiety (STAI-T). In this study, we used only the STAI-S. Total scores range from 20 to 80, where higher scores indicate higher anxiety feelings.
- Smith Relaxation State Inventory 3 (SRSI3) [72]: The SRSI3 is the revised version of the Smith Relaxation State inventory and measures 19 relaxation states. Individuals are asked to evaluate how they feel right now in response to 38 items on a 6-point Likert scale. The scale is divided into four subscales that can be selected independently. For this protocol, the following subscales have been selected, for a total of 20 items: rest/refresh, energised, physical relaxation, at ease/peace, joy, mental quiet, awareness, somatic stress, emotional stress, and cognitive stress.
- Subjective Units of Distress Scale (SUDS) [73]: The SUDS is a numeric rating scale from 0 to 100 that evaluates the subjectively perceived level of distress.
2.4. Data Analysis
3. Results
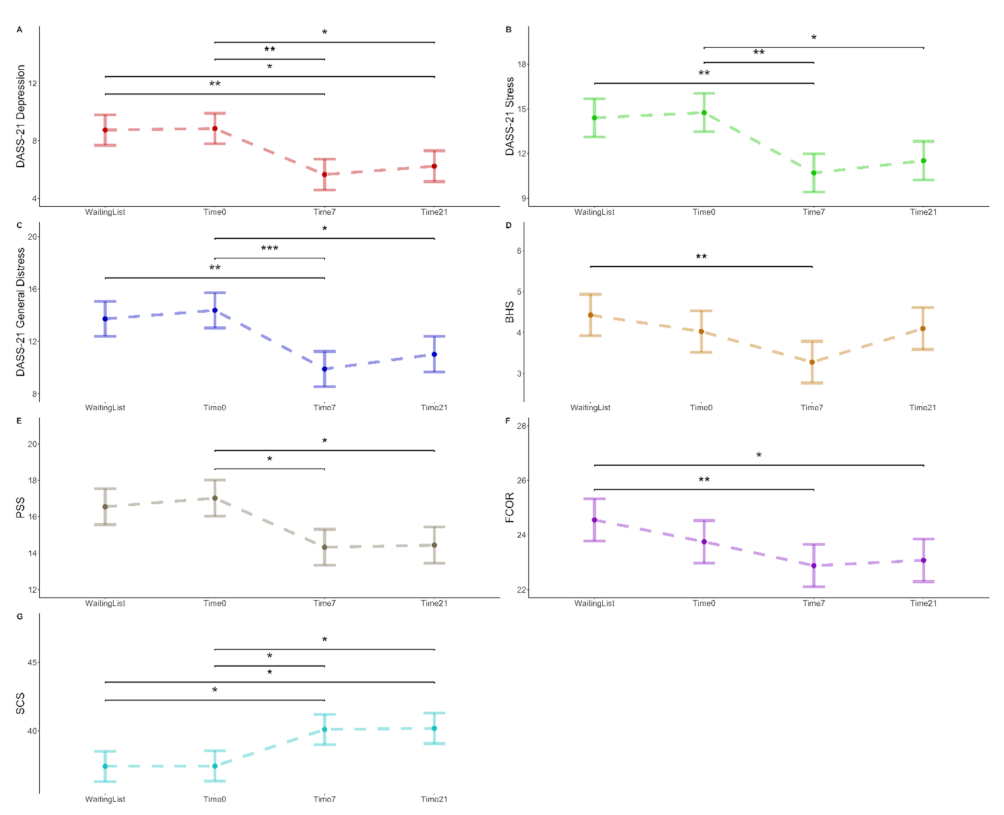
3.1. Primary and Secondary Outcome Measures
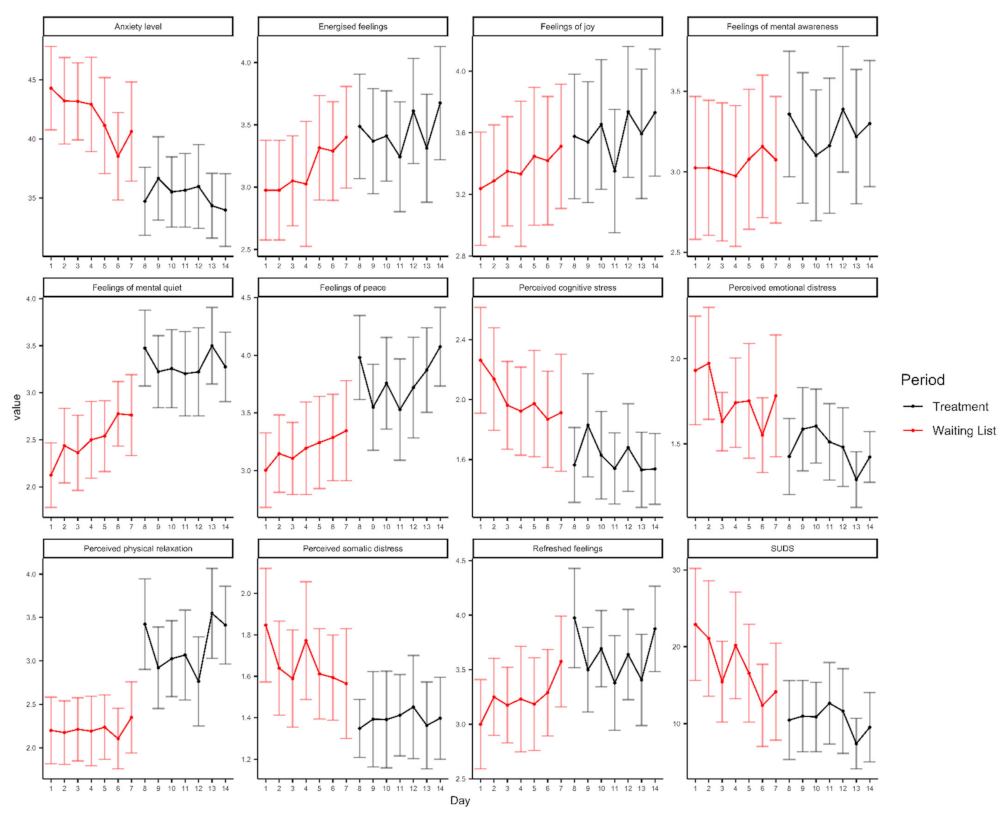
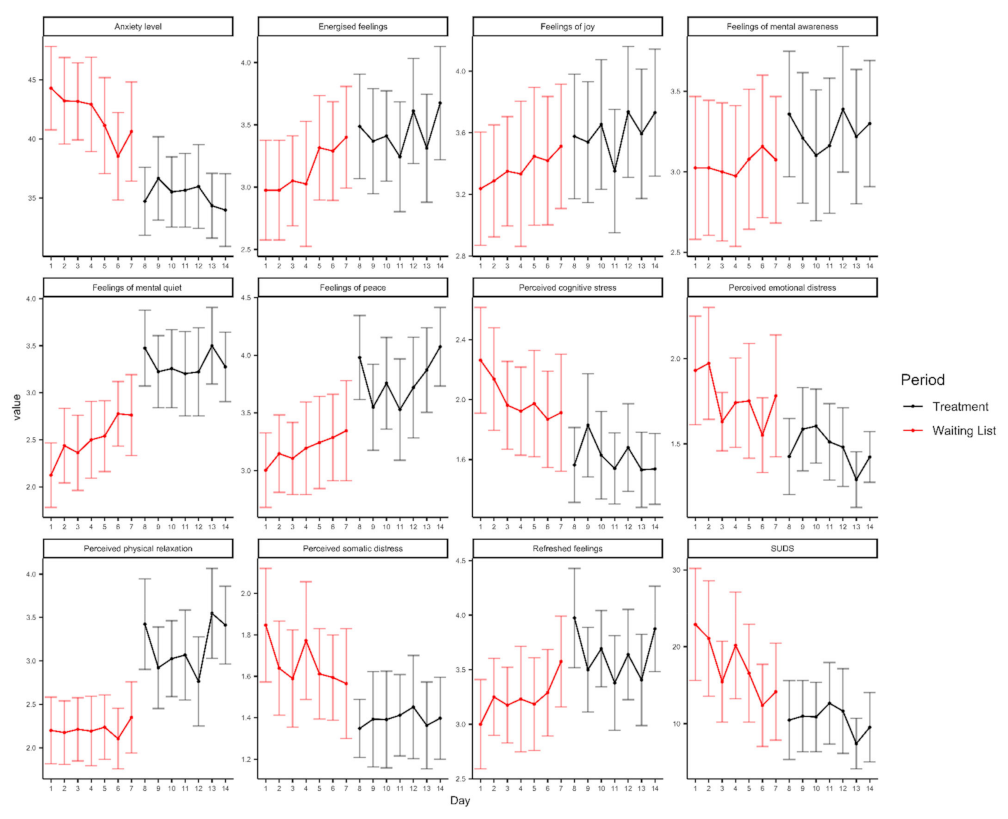
3.2. State Outcome Measures
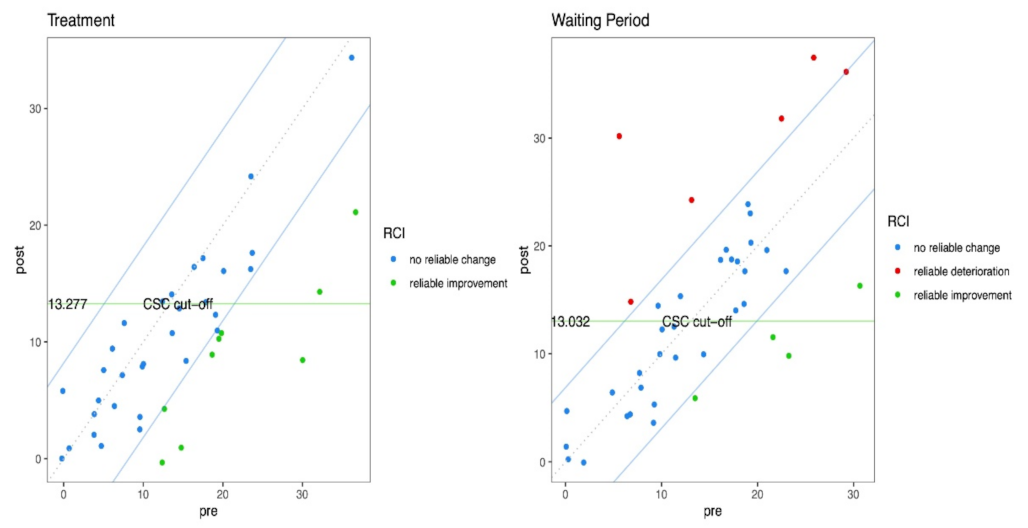
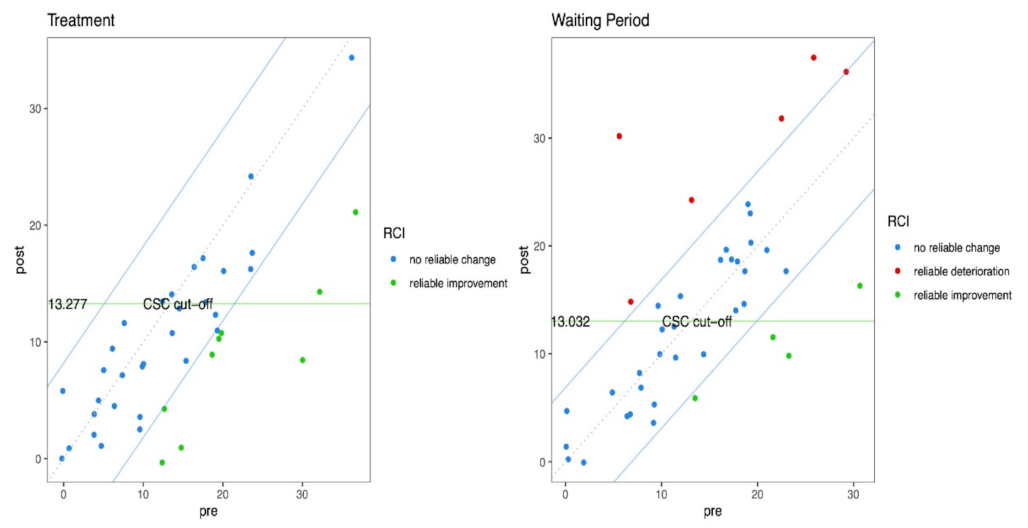
3.3. Clinical Change Analyses of Primary Outcomes
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Paules, C.I.; Marston, H.D.; Fauci, A.S. Coronavirus Infections-More Than Just the Common Cold. JAMA J. Am. Med. Assoc. 2020, 323, 707–708. [Google Scholar] [CrossRef] [Green Version]
- Reiss, C.S. Coronavirus Pandemic. DNA Cell Biol. 2020, 39, 919. [Google Scholar] [CrossRef]
- Jee, Y. WHO International Health Regulations Emergency Committee for the COVID-19 outbreak. Epidemiol. Health 2020, 42, e2020013. [Google Scholar] [CrossRef] [Green Version]
- Remuzzi, A.; Remuzzi, G. COVID-19 and Italy: What next? Lancet 2020, 395, 1225–1228. [Google Scholar] [CrossRef]
- Katz, R.; Vaught, A.; Simmens, S.J. Local Decision Making for Implementing Social Distancing in Response to Outbreaks. Public Health Rep. 2019, 134, 150–154. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Brooks, S.K.; Webster, R.K.; Smith, L.E.; Woodland, L.; Wessely, S.; Greenberg, N.; Rubin, G.J. The psychological impact of quarantine and how to reduce it: Rapid review of the evidence. Lancet 2020, 395, 912–920. [Google Scholar] [CrossRef] [Green Version]
- Holmes, E.A.; O’Connor, R.C.; Perry, V.H.; Tracey, I.; Wessely, S.; Arseneault, L.; Ballard, C.; Christensen, H.; Cohen Silver, R.; Everall, I.; et al. Multidisciplinary research priorities for the COVID-19 pandemic: A call for action for mental health science. Lancet Psychiatry 2020, 7, 547–560. [Google Scholar] [CrossRef]
- Vindegaard, N.; Benros, M.E. COVID-19 pandemic and mental health consequences: Systematic review of the current evidence. Brain. Behav. Immun. 2020, 89, 531–542. [Google Scholar] [CrossRef] [PubMed]
- Marazziti, D.; Pozza, A.; Di Giuseppe, M.; Conversano, C. The psychosocial impact of COVID-19 pandemic in Italy: A lesson for mental health prevention in the first severely hit European country. Psychol. Trauma Theory Res. Pract. Policy 2020, 12, 531–533. [Google Scholar] [CrossRef]
- Pfefferbaum, B.; North, C.S. Mental health and the Covid-19 pandemic. N. Engl. J. Med. 2020, 383, 510–512. [Google Scholar] [CrossRef]
- Pagnini, F.; Bonanomi, A.; Tagliabue, S.; Balconi, M.; Bertolotti, M.; Confalonieri, E.; Di Dio, C.; Gilli, G.; Graffigna, G.; Regalia, C.; et al. Knowledge, Concerns, and Behaviors of Individuals during the First Week of the Coronavirus Disease 2019 Pandemic in Italy. JAMA Netw. Open 2020, 3, e2015821. [Google Scholar] [CrossRef] [PubMed]
- De Giorgio, A. Global Psychological Implications of Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) and Coronavirus Disease-2019 (COVID-19). What Can Be Learned From Italy. Reflections, Perspectives, Opportunities. Front. Psychol. 2020, 11. [Google Scholar] [CrossRef] [PubMed]
- Xiong, J.; Lipsitz, O.; Nasri, F.; Lui, L.M.W.; Gill, H.; Phan, L.; Chen-Li, D.; Iacobucci, M.; Ho, R.; Majeed, A. Impact of COVID-19 pandemic on mental health in the general population: A systematic review. J. Affect. Disord. 2020, 277, 55–64. [Google Scholar] [CrossRef]
- Franceschini, C.; Musetti, A.; Zenesini, C.; Palagini, L.; Scarpelli, S.; Quattropani, M.C.; Lenzo, V.; Freda, M.F.; Lemmo, D.; Vegni, E.; et al. Poor sleep quality and its consequences on mental health during the COVID-19 lockdown in Italy. Front. Psychol. 2020, 11, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Rubin, G.J.; Wessely, S. The psychological effects of quarantining a city. BMJ 2020, 368. [Google Scholar] [CrossRef] [Green Version]
- Rossi, R.; Socci, V.; Talevi, D.; Mensi, S.; Niolu, C.; Pacitti, F.; Di Marco, A.; Rossi, A.; Siracusano, A.; Di Lorenzo, G. COVID-19 Pandemic and Lockdown Measures Impact on Mental Health Among the General Population in Italy. Front. Psychiatry 2020, 11, 790. [Google Scholar] [CrossRef]
- Park, S.C.; Park, Y.C. Secondary emotional reactions to the Covid-19 outbreak should be identified and treated in Korea. J. Korean Med. Sci. 2020, 35, e161. [Google Scholar] [CrossRef] [Green Version]
- Fernández, R.S.; Crivelli, L.; Guimet, N.M.; Allegri, R.F.; Pedreira, M.E. Psychological distress associated with COVID-19 quarantine: Latent profile analysis, outcome prediction and mediation analysis. J. Affect. Disord. 2020, 277, 75–84. [Google Scholar] [CrossRef] [PubMed]
- Gruber, J.; Prinstein, M.J.; Clark, L.A.; Rottenberg, J.; Abramowitz, J.S.; Albano, A.M.; Aldao, A.; Borelli, J.L.; Chung, T.; Davila, J.; et al. Mental Health and Clinical Psychological Science in the Time of COVID-19: Challenges, Opportunities, and a Call to Action. Am. Psychol. 2020, 76, 409–426. [Google Scholar] [CrossRef]
- Ruffolo, M.; Price, D.; Schoultz, M.; Leung, J.; Bonsaksen, T.; Thygesen, H.; Geirdal, A.Ø. Employment Uncertainty and Mental Health During the COVID-19 Pandemic Initial Social Distancing Implementation: A Cross-national Study. Glob. Soc. Welf. 2021, 8, 141–150. [Google Scholar] [CrossRef]
- Rettie, H.; Daniels, J. Coping and Tolerance of Uncertainty: Predictors and Mediators of Mental Health During the COVID-19 Pandemic. Am. Psychol. 2020, 76, 427–437. [Google Scholar] [CrossRef]
- Satici, B.; Saricali, M.; Satici, S.A.; Griffiths, M.D. Intolerance of Uncertainty and Mental Wellbeing: Serial Mediation by Rumination and Fear of COVID-19. Int. J. Ment. Health Addict. 2020, 1–12. [Google Scholar] [CrossRef]
- Thorell, L.B.; Skoglund, C.; de la Peña, A.G.; Baeyens, D.; Fuermaier, A.B.M.; Groom, M.J.; Mammarella, I.C.; van der Oord, S.; van den Hoofdakker, B.J.; Luman, M.; et al. Parental experiences of homeschooling during the COVID-19 pandemic: Differences between seven European countries and between children with and without mental health conditions. Eur. Child Adolesc. Psychiatry 2021, 1–13. [Google Scholar] [CrossRef]
- Sinclair, R.R.; Probst, T.M.; Watson, G.P.; Bazzoli, A. Caught between Scylla and Charybdis: How economic stressors and occupational risk factors influence workers’ occupational health reactions to COVID-19. Appl. Psychol. 2021, 70, 85–119. [Google Scholar] [CrossRef]
- Townsend, A.K.; Hawley, D.M.; Stephenson, J.F.; Williams, K.E.G. Emerging infectious disease and the challenges of social distancing in human and non-human animals. Proc. R. Soc. B Biol. Sci. 2020, 287, 20201039. [Google Scholar] [CrossRef] [PubMed]
- Riva, G.; Wiederhold, B.K.; Mantovani, F. Surviving COVID-19: The Neuroscience of Smart Working and Distance Learning. Cyberpsychol. Behav. Soc. Netw. 2021, 24, 79–85. [Google Scholar] [CrossRef]
- Sutin, A.R.; Luchetti, M.; Terracciano, A. Has loneliness increased during COVID-19? Comment on “Loneliness: A signature mental health concern in the era of COVID-19”. Psychiatry Res. 2020, 291, 113–117. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez, L.M.; Litt, D.M.; Stewart, S.H. Drinking to cope with the pandemic: The unique associations of COVID-19-related perceived threat and psychological distress to drinking behaviors in American men and women. Addict. Behav. 2020, 110, 106532. [Google Scholar] [CrossRef]
- Magson, N.R.; Freeman, J.Y.A.; Rapee, R.M.; Richardson, C.E.; Oar, E.L.; Fardouly, J. Risk and Protective Factors for Prospective Changes in Adolescent Mental Health during the COVID-19 Pandemic. J. Youth Adolesc. 2021, 50, 44–57. [Google Scholar] [CrossRef] [PubMed]
- Ye, Z.; Yang, X.; Zeng, C.; Wang, Y.; Shen, Z.; Li, X.; Lin, D. Resilience, Social Support, and Coping as Mediators between COVID-19-related Stressful Experiences and Acute Stress Disorder among College Students in China. Appl. Psychol. Heal. Well-Being 2020, 12, 1074–1094. [Google Scholar] [CrossRef]
- Zhou, X.; Snoswell, C.L.; Harding, L.E.; Bambling, M.; Edirippulige, S.; Bai, X.; Smith, A.C. The Role of Telehealth in Reducing the Mental Health Burden from COVID-19. Telemed. J. E Health 2020, 26, 377–379. [Google Scholar] [CrossRef] [Green Version]
- Luxton, D.D.; Pruitt, L.D.; Osenbach, J.E. Best practices for remote psychological assessment via telehealth technologies. Prof. Psychol. Res. Pract. 2014, 45, 27–35. [Google Scholar] [CrossRef] [Green Version]
- Riva, G. From telehealth to E-health: Internet and distributed virtual reality in health care. Cyberpsychology Behav. 2000, 3, 989–998. [Google Scholar] [CrossRef]
- Langarizadeh, M.; Tabatabaei, M.S.; Tavakol, K.; Naghipour, M.; Rostami, A.; Moghbeli, F. Telemental health care, an effective alternative to conventional mental care: A systematic review. Acta Inform. Medica 2017, 25, 240–246. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Connolly, S.L.; Stolzmann, K.L.; Heyworth, L.; Weaver, K.R.; Bauer, M.S.; Miller, C.J. Rapid Increase in Telemental Health within the Department of Veterans Affairs during the COVID-19 Pandemic. Telemed. e-Health 2021, 27, 454–458. [Google Scholar] [CrossRef] [PubMed]
- Madigan, S.; Racine, N.; Cooke, J.E.; Korczak, D.J. COVID-19 and telemental health: Benefits, challenges, and future directions. Can. Psychol. Can. 2021, 62, 5–11. [Google Scholar] [CrossRef]
- Wright, J.H.; Caudill, R. Remote treatment delivery in response to the COVID-19 Pandemic. Psychother. Psychosom. 2020, 89, 130–132. [Google Scholar] [CrossRef]
- Mishkind, M.C.; Shore, J.H.; Bishop, K.; D’Amato, K.; Brame, A.; Thomas, M.; Schneck, C.D. Rapid Conversion to Telemental Health Services in Response to COVID-19: Experiences of Two Outpatient Mental Health Clinics. Telemed. e-Health 2020. [Google Scholar] [CrossRef]
- Luxton, D.D.; McCann, R.A.; Bush, N.E.; Mishkind, M.C.; Reger, G.M. MHealth for mental health: Integrating smartphone technology in behavioral healthcare. Prof. Psychol. Res. Pract. 2011, 42, 505–512. [Google Scholar] [CrossRef] [Green Version]
- Riva, G.; Wiederhold, B.K.; Mantovani, F. Neuroscience of Virtual Reality: From Virtual Exposure to Embodied Medicine. Cyberpsychol. Behav. Soc. Netw. 2019, 22, 82–96. [Google Scholar] [CrossRef] [PubMed]
- Valmaggia, L.R.; Latif, L.; Kempton, M.J.; Rus-Calafell, M. Virtual reality in the psychological treatment for mental health problems: An systematic review of recent evidence. Psychiatry Res. 2016, 236, 189–195. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Villani, D.; Grassi, A.; Cognetta, C.; Toniolo, D.; Cipresso, P.; Riva, G. Self-help stress management training through mobile phones: An experience with oncology nurses. Psychol. Serv. 2013, 10, 315–322. [Google Scholar] [CrossRef] [PubMed]
- Beatty, L.; Lambert, S. A systematic review of internet-based self-help therapeutic interventions to improve distress and disease-control among adults with chronic health conditions. Clin. Psychol. Rev. 2013, 33, 609–622. [Google Scholar] [CrossRef]
- Karyotaki, E.; van Ballegooijen, W. Digital self-help interventions for suicidal ideation and behaviour. Lancet Digit. Heal. 2020, 2, e4–e5. [Google Scholar] [CrossRef] [Green Version]
- Yim, S.H.; Schmidt, U. Experiences of computer-based and conventional self-help interventions for eating disorders: A systematic review and meta-synthesis of qualitative research. Int. J. Eat. Disord. 2019, 52, 1108–1124. [Google Scholar] [CrossRef] [PubMed]
- Riva, G.; Wiederhold, B.K. How Cyberpsychology and Virtual Reality Can Help Us to Overcome the Psychological Burden of Coronavirus. Cyberpsychol. Behav. Soc. Netw. 2020, 23, 277–279. [Google Scholar] [CrossRef] [Green Version]
- Riva, G.; Mantovani, F.; Wiederhold, B.K. Positive technology and COVID-19. Cyberpsychol. Behav. Soc. Netw. 2020, 23, 581–587. [Google Scholar] [CrossRef]
- Pincus, L.E. Telemental Health During a Global Pandemic: Clinical Lessons from Guided Self-Help, Telephone Therapy Case Studies. Pragmatic Case Stud. Psychother. 2020, 16, 118–123. [Google Scholar] [CrossRef]
- Riva, G.; Riva, E. COVID Feel Good: A Free VR Self-Help Solution for Providing Stress Management and Social Support During the COVID-19 Pandemic. Cyberpsychol. Behav. Soc. Netw. 2020, 23, 652–653. [Google Scholar] [CrossRef]
- Fischer, R.; Bortolini, T.; Karl, J.A.; Zilberberg, M.; Robinson, K.; Rabelo, A.; Gemal, L.; Wegerhoff, D.; Nguyễn, T.B.T.; Irving, B.; et al. Rapid Review and Meta-Meta-Analysis of Self-Guided Interventions to Address Anxiety, Depression, and Stress During COVID-19 Social Distancing. Front. Psychol. 2020, 11, 563876. [Google Scholar] [CrossRef]
- Bohil, C.J.; Alicea, B.; Biocca, F.A. Virtual reality in neuroscience research and therapy. Nat. Rev. Neurosci. 2011, 12, 752–762. [Google Scholar] [CrossRef] [PubMed]
- Salisbury, J.P.; Aronson, T.M.; Simon, T.J. At-home self-administration of an immersive virtual reality therapeutic game for post-stroke upper limb rehabilitation. In Proceedings of the CHI PLAY 2020—Extended Abstracts of the 2020 Annual Symposium on Computer-Human Interaction in Play; Association for Computing Machinery, Inc.: New York, NY, USA, 2020; pp. 114–121. [Google Scholar]
- Donker, T.; van Klaveren, C.; Cornelisz, I.; Kok, R.N.; van Gelder, J.-L. Analysis of Usage Data from a Self-Guided App-Based Virtual Reality Cognitive Behavior Therapy for Acrophobia: A Randomized Controlled Trial. J. Clin. Med. 2020, 9, 1614. [Google Scholar] [CrossRef]
- Riva, G.; Bernardelli, L.; Browning, M.H.E.M.; Castelnuovo, G.; Cavedoni, S.; Chirico, A.; Cipresso, P.; de Paula, D.M.B.; Di Lernia, D.; Fernández-Álvarez, J.; et al. COVID Feel Good—An Easy Self-Help Virtual Reality Protocol to Overcome the Psychological Burden of Coronavirus. Front. Psychiatry 2020, 11, 996. [Google Scholar] [CrossRef] [PubMed]
- Italian Ministry of Health Covid-19. Available online: www.salute.gov.it/portale/news/p3_2_1_1_1.jsp?lingua=italiano&menu=notizie&p=dalministero&id=4186 (accessed on 1 June 2021).
- Chirico, A.; Clewis, R.R.; Yaden, D.B.; Gaggioli, A. Nature versus art as elicitors of the sublime: A virtual reality study. PLoS ONE 2021, 16, e0233628. [Google Scholar] [CrossRef]
- Gilbert, P. Developing a compassion-focused approach in cognitive behavioural therapy. In Cognitive Behaviour Therapy: A Guide for the Practising Clinician; Routledge/Taylor & Francis Group: New York, NY, USA, 2009; Volume 2, pp. 205–220, ISBN 978-0-415-44964-9 (Paperback), 978-0-415-44963-2 (Hardcover). [Google Scholar]
- Gilbert, P. An introduction to Compassion Focused Therapy in Cognitive Behavior Therapy. Int. J. Cogn. Ther. 2010, 3, 97–112. [Google Scholar] [CrossRef]
- Winch, G. Emotional First Aid: Practical Strategies for Treating Failure, Rejection, Guilt, and Other Everyday Psychological Injuries; Hudson Street Press: New York, NY, USA, 2013; ISBN 9781921966354. [Google Scholar]
- Lovibond, P.F.; Lovibond, S.H. The structure of negative emotional states: Comparison of the Depression Anxiety Stress Scales (DASS) with the Beck Depression and Anxiety Inventories. Behav. Res. Ther. 1995, 33, 335–343. [Google Scholar] [CrossRef]
- Bottesi, G.; Ghisi, M.; Altoè, G.; Conforti, E.; Melli, G.; Sica, C. The Italian version of the Depression Anxiety Stress Scales-21: Factor structure and psychometric properties on community and clinical samples. Compr. Psychiatry 2015, 60, 170–181. [Google Scholar] [CrossRef]
- Cohen, S.; Kamarck, T.; Mermelstein, R. Perceived Stress Scale; Mind Garden, Inc.: Menlo Park, CA, USA, 1983; Volume 10. [Google Scholar]
- Mondo, M.; Sechi, C.; Cabras, C. Psychometric evaluation of three versions of the Italian Perceived Stress Scale. Curr. Psychol. 2021, 40, 1884–1892. [Google Scholar] [CrossRef]
- Beck, A.T.; Weissman, A.; Lester, D.; Trexler, L. The measurement of pessimism: The Hopelessness Scale. J. Consult. Clin. Psychol. 1974, 42, 861–865. [Google Scholar] [CrossRef]
- Innamorati, M.; Lester, D.; Balsamo, M.; Erbuto, D.; Ricci, F.; Amore, M.; Girardi, P.; Pompili, M. Factor validity of the beck hopelessness scale in Italian medical patients. J. Psychopathol. Behav. Assess. 2014, 36, 300–307. [Google Scholar] [CrossRef]
- Capanna, C.; Stratta, P.; Collazzoni, A.; D’Ubaldo, V.; Pacifico, R.; Di Emidio, G.; Ragusa, M.; Rossi, A. Social connectedness as resource of resilience: Italian validation of the social connectedness scale—Revised. J. Psychopathol. 2013, 19, 320–326. [Google Scholar]
- Lee, R.M.; Robbins, S.B. Measuring Belongingness: The Social Connectedness and the Social Assurance Scales. J. Couns. Psychol. 1995, 42, 232–241. [Google Scholar] [CrossRef]
- Cosentino, T.; Pellegrini, V.; Giacomantonio, M.; Saliani, A.M.; Basile, B.; Saettoni, M.; Gragnani, A.; Buonanno, C.; Mancini, F. Validation and psychometric properties of the Italian version of the Fear of Guilt Scale. Rass. Psicol. 2020, 37, 59–70. [Google Scholar] [CrossRef]
- Ahorsu, D.K.; Lin, C.Y.; Imani, V.; Saffari, M.; Griffiths, M.D.; Pakpour, A.H. The Fear of COVID-19 Scale: Development and Initial Validation. Int. J. Ment. Health Addict. 2020, 1–9. [Google Scholar] [CrossRef] [Green Version]
- Pedrabissi, L.; Santinello, M. Verifica della validità dello S.T.A.I. forma Y di Spielberger. Boll. Psicol. Appl. 1989, 191, 11–14. [Google Scholar]
- Set, S. State-Trait Anxiety Inventory for Adults. Garden 2010, 1–75. [Google Scholar] [CrossRef]
- Smith, J. Relaxation Inventory; Lulupress: Raleigh, NC, USA, 2000; Volume 3, pp. 1201–1208. [Google Scholar]
- Ruden, R.A. Subjective Units of Distress Scale. Available online: http://haveningblog.tumblr.com/post/100433877079/suds-subjective-units-of-distress-scale (accessed on 1 June 2020).
- Cohen, J. Statistical Power Analysis for the Behavioral Sciences; Academic Press: New York, NY, USA, 2013; ISBN 1483276481. [Google Scholar]
- Heber, E.; Ebert, D.D.; Lehr, D.; Cuijpers, P.; Berking, M.; Nobis, S.; Riper, H. The benefit of web-and computer-based interventions for stress: A systematic review and meta-analysis. J. Med. Internet Res. 2017, 19, e32. [Google Scholar] [CrossRef] [Green Version]
- Luke, S.G. Evaluating significance in linear mixed-effects models in R. Behav. Res. Methods 2017, 49, 1494–1502. [Google Scholar] [CrossRef]
- Bates, D.; Mächler, M.; Bolker, B.M.; Walker, S.C. Fitting linear mixed-effects models using lme4. J. Stat. Softw. 2015, 67, 1–48. [Google Scholar] [CrossRef]
- Bolker, B.M. Ecological Models and Data in R; Princeton University Press: New Jersey, NY, USA, 2008; ISBN 9781400840908. [Google Scholar]
- Kuznetsova, A.; Brockhoff, P.B.; Christensen, R.H.B. lmerTest Package: Tests in Linear Mixed Effects Models. J. Stat. Softw. 2017, 82, 1–26. [Google Scholar] [CrossRef] [Green Version]
- Lenth, R.; Lenth, M.R. Package ‘lsmeans'. Am. Stat. 2018, 34, 216–221. [Google Scholar]
- Evans, C.; Margison, F.; Barkham, M. The contribution of reliable and clinically significant change methods to evidence-based mental health. Evid. Based. Ment. Health 1998, 1, 70–72. [Google Scholar] [CrossRef] [Green Version]
- Morris, S.B. Estimating effect sizes from pretest-posttest-control group designs. Organ. Res. methods 2008, 11, 364–386. [Google Scholar] [CrossRef]
- Page, P. Beyond statistical significance: Clinical interpretation of rehabilitation research literature. Int. J. Sports Phys. Ther. 2014, 9, 726. [Google Scholar] [PubMed]
- Necho, M.; Tsehay, M.; Birkie, M.; Biset, G.; Tadesse, E. Prevalence of anxiety, depression, and psychological distress among the general population during the COVID-19 pandemic: A systematic review and meta-analysis. Int. J. Soc. Psychiatry 2021, 00207640211003121. [Google Scholar] [CrossRef]
- Cipolletta, S.; Ortu, M.C. COVID-19: Common constructions of the pandemic and their implications. J. Constr. Psychol. 2020, 11, 1–17. [Google Scholar] [CrossRef]
- Wahlund, T.; Mataix-Cols, D.; Lauri, K.O.; de Schipper, E.; Ljótsson, B.; Aspvall, K.; Andersson, E. Brief online cognitive behavioural intervention for dysfunctional worry related to the COVID-19 pandemic: A randomised controlled trial. Psychother. Psychosom. 2021, 90, 191–199. [Google Scholar] [CrossRef] [PubMed]
- Piltch-Loeb, R.; Merdjanoff, A.; Meltzer, G. Anticipated mental health consequences of COVID-19 in a nationally-representative sample: Context, coverage, and economic consequences. Prev. Med. 2021, 145, 106441. [Google Scholar] [CrossRef]
- Livingston, N.A.; Shingleton, R.; Heilman, M.E.; Brief, D. Self-help smartphone applications for alcohol use, PTSD, anxiety, and depression: Addressing the new research-practice gap. J. Technol. Behav. Sci. 2019, 4, 139–151. [Google Scholar] [CrossRef]
- Poletti, B.; Tagini, S.; Brugnera, A.; Parolin, L.; Pievani, L.; Ferrucci, R.; Compare, A.; Silani, V. Telepsychotherapy: A leaflet for psychotherapists in the age of COVID-19. A review of the evidence. Couns. Psychol. Q. 2020, 1–16. [Google Scholar] [CrossRef]
- COVID Feel Good. Available online: https://www.covidfeelgood.com/ (accessed on 1 June 2021).


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | Total Sample (N = 40) |
|---|---|
| Age (years), mean (SD) | 30.28 (11.69) |
| Gender, N (%) | |
| Male | 15 (37.5) |
| Female | 25 (62.5) |
| Relationship Status, N (%) | |
| Single | 30 (72.5) |
| Married | 10 (25) |
| Employment Status, N (%) | |
| Student | 22 (55) |
| Employed | 18 (45) |
| Housing arrangements, N (%) | |
| Living alone | <5 (<5) |
| Living with partner | 6 (15) |
| Living with partner and children | 5 (12.5) |
| Living with parents | 23 (57.5) |
| Living with friends | <5 (<5) |
| Other | <5 (<5) |
| Experience of COVID Feel Good, N (%) | |
| Immersive modality Non-Immersive modality | 18 (45) 22 (55) |
| Waiting Period Mean (SD) | T0 Mean (SD) | T1 Mean (SD) | T2 Mean (SD) | ||
|---|---|---|---|---|---|
| Primary outcome measures | |||||
| DASS-21 | Depression symptoms | 8.75 (6.80) | 8.85 (8.18) | 5.65 (5.51) | 6.37 (6.59) |
| Anxiety symptoms | 4.30 (3.88) | 5.15 (4.77) | 3.45 (4.51) | 4.21 (4.50) | |
| Stress symptoms | 14.40 (8.25) | 14.75 (8.14) | 10.70 (7.01) | 11.74 (9.10) | |
| General distress | 13.73 (7.85) | 14.44 (9.34 | 9.90 (7.08) | 11.23 (9.56) | |
| PSS | Perceived stress level | 16.55 (5.82) | 17.03 (6.18) | 14.33 (5.98) | 14.50 (6.97) |
| BHS | Perceived hopelessness | 4.42 (3.22) | 4.03 (3.08) | 3.27 (2.79) | 4.13 (3.71) |
| Secondary outcome measures | |||||
| SCS | Perceived social connectedness | 37.40 (7.81) | 37.43 (6.63) | 40.10 (6.64) | 40.08 (6.96) |
| FCOR | Fear of coronavirus | 24.55 (4.62) | 23.75 (4.74) | 22.88 (5.00) | 23.03 (5.36) |
| State Outcome Measures | Waiting Period | Intervention Week | |
|---|---|---|---|
| Mean (SD) | Mean (SD) | ||
| STAI-S | Anxiety level | 42.00 (9.48) | 35.29 (7.52) |
| SRSI3 | Refreshed feelings | 3.24 (0.69) | 3.67 (0.88) |
| Energised feelings | 3.09 (0.60) | 3.46 (1.00) | |
| Perceived physical relaxation | 2.22 (0.87) | 3.15 (1.25) | |
| Feelings of peace | 3.20 (0.79) | 4.76 (0.41) | |
| Feelings of joy | 3.38 (0.91) | 3.61 (1.02) | |
| Feelings of mental quiet | 2.50 (0.81) | 3.31 (0.96) | |
| Feelings of mental awareness | 3.06 (1.01) | 3.25 (0.96) | |
| Perceived somatic distress | 1.66 (0.55) | 1.40 (0.50) | |
| Perceived emotional distress | 1.76 (0.66) | 1.48 (0.46) | |
| Perceived cognitive stress | 2.01 (0.83) | 1.62 (0.67) | |
| SUDS | Subjectively perceived levels of discomfort | 17.62 (15.6) | 10.71 (13.1) |
| Variables | Improvement RCI | Deterioration RCI | Improvement CSC | RR | CER | EER | RRR | ARR | NNT | Effect Size d |
|---|---|---|---|---|---|---|---|---|---|---|
| Depression Symptoms | Treatment: 4 Waiting period: 2 | Treatment: 0 Waiting period: 4 | Treatment: 1 Waiting period: 0 | 0 | 67 | 0 | 100 | 67 | 1 | 0.45 small-beneficial |
| Anxiety Symptoms | Treatment: 4 Waiting period: 0 | Treatment: 2 Waiting period: 4 | Treatment: 3 Waiting period: 0 | 0.33 | 100 | 33 | 67 | 67 | 1 | 0.56 medium-beneficial |
| Stress symptoms | Treatment: 8 Waiting period: 3 | Treatment: 1 Waiting period: 2 | Treatment: 4 Waiting period: 0 | 0.28 | 40 | 11 | 72 | 29 | 3 | 0.55 medium-beneficial |
| General Distress | Treatment: 9 Waiting period: 4 | Treatment: 0 Waiting period: 6 | Treatment: 5 Waiting period: 2 | 0 | 60 | 0 | 100 | 60 | 2 | 0.6 medium-beneficial |
| Perceived Stress Level | Treatment: 2 Waiting period: 1 | Treatment: 1 Waiting period: 3 | Treatment: 2 Waiting period: 1 | 0.44 | 75 | 33 | 56 | 42 | 2 | 0.66 medium-beneficial |
| Perceived Stress Level | Treatment: 2 Waiting period: 0 | Treatment: 0 Waiting period: 1 | Treatment: 1 Waiting period: 0 | 0 | 100 | 0 | 100 | 100 | 1 | 0.22 small-beneficial |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Riva, G.; Bernardelli, L.; Castelnuovo, G.; Di Lernia, D.; Tuena, C.; Clementi, A.; Pedroli, E.; Malighetti, C.; Sforza, F.; Wiederhold, B.K.; et al. A Virtual Reality-Based Self-Help Intervention for Dealing with the Psychological Distress Associated with the COVID-19 Lockdown: An Effectiveness Study with a Two-Week Follow-Up. Int. J. Environ. Res. Public Health 2021, 18, 8188. https://doi.org/10.3390/ijerph18158188
Riva G, Bernardelli L, Castelnuovo G, Di Lernia D, Tuena C, Clementi A, Pedroli E, Malighetti C, Sforza F, Wiederhold BK, et al. A Virtual Reality-Based Self-Help Intervention for Dealing with the Psychological Distress Associated with the COVID-19 Lockdown: An Effectiveness Study with a Two-Week Follow-Up. International Journal of Environmental Research and Public Health. 2021; 18(15):8188. https://doi.org/10.3390/ijerph18158188
Chicago/Turabian StyleRiva, Giuseppe, Luca Bernardelli, Gianluca Castelnuovo, Daniele Di Lernia, Cosimo Tuena, Alex Clementi, Elisa Pedroli, Clelia Malighetti, Francesca Sforza, Brenda K. Wiederhold, and et al. 2021. "A Virtual Reality-Based Self-Help Intervention for Dealing with the Psychological Distress Associated with the COVID-19 Lockdown: An Effectiveness Study with a Two-Week Follow-Up" International Journal of Environmental Research and Public Health 18, no. 15: 8188. https://doi.org/10.3390/ijerph18158188
APA StyleRiva, G., Bernardelli, L., Castelnuovo, G., Di Lernia, D., Tuena, C., Clementi, A., Pedroli, E., Malighetti, C., Sforza, F., Wiederhold, B. K., & Serino, S. (2021). A Virtual Reality-Based Self-Help Intervention for Dealing with the Psychological Distress Associated with the COVID-19 Lockdown: An Effectiveness Study with a Two-Week Follow-Up. International Journal of Environmental Research and Public Health, 18(15), 8188. https://doi.org/10.3390/ijerph18158188