
Endometriosis—A Multifaceted Problem of a Modern Woman

 , , , , and
, , , , and
Abstract
:1. Introduction
2. Materials and Methods
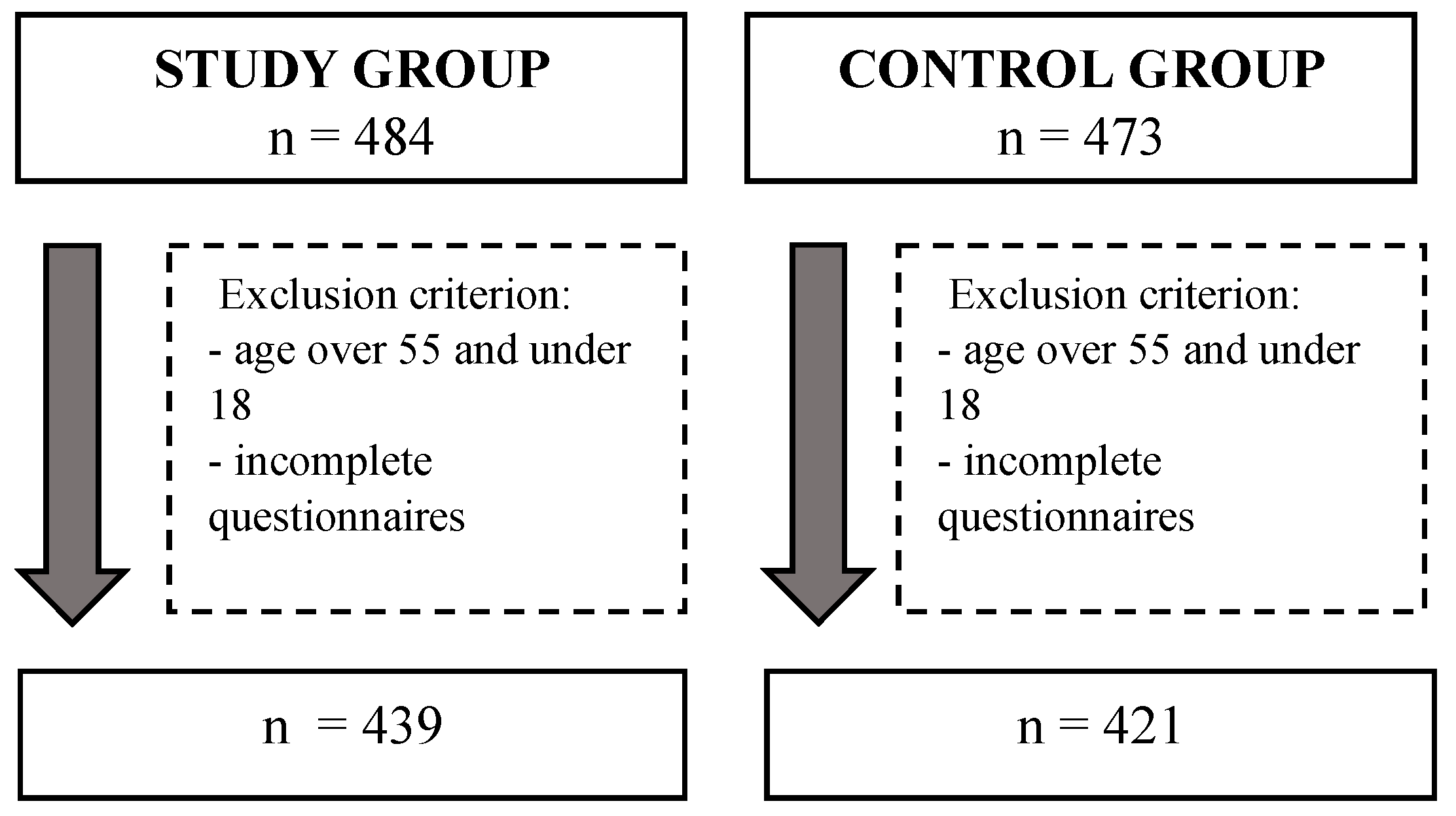
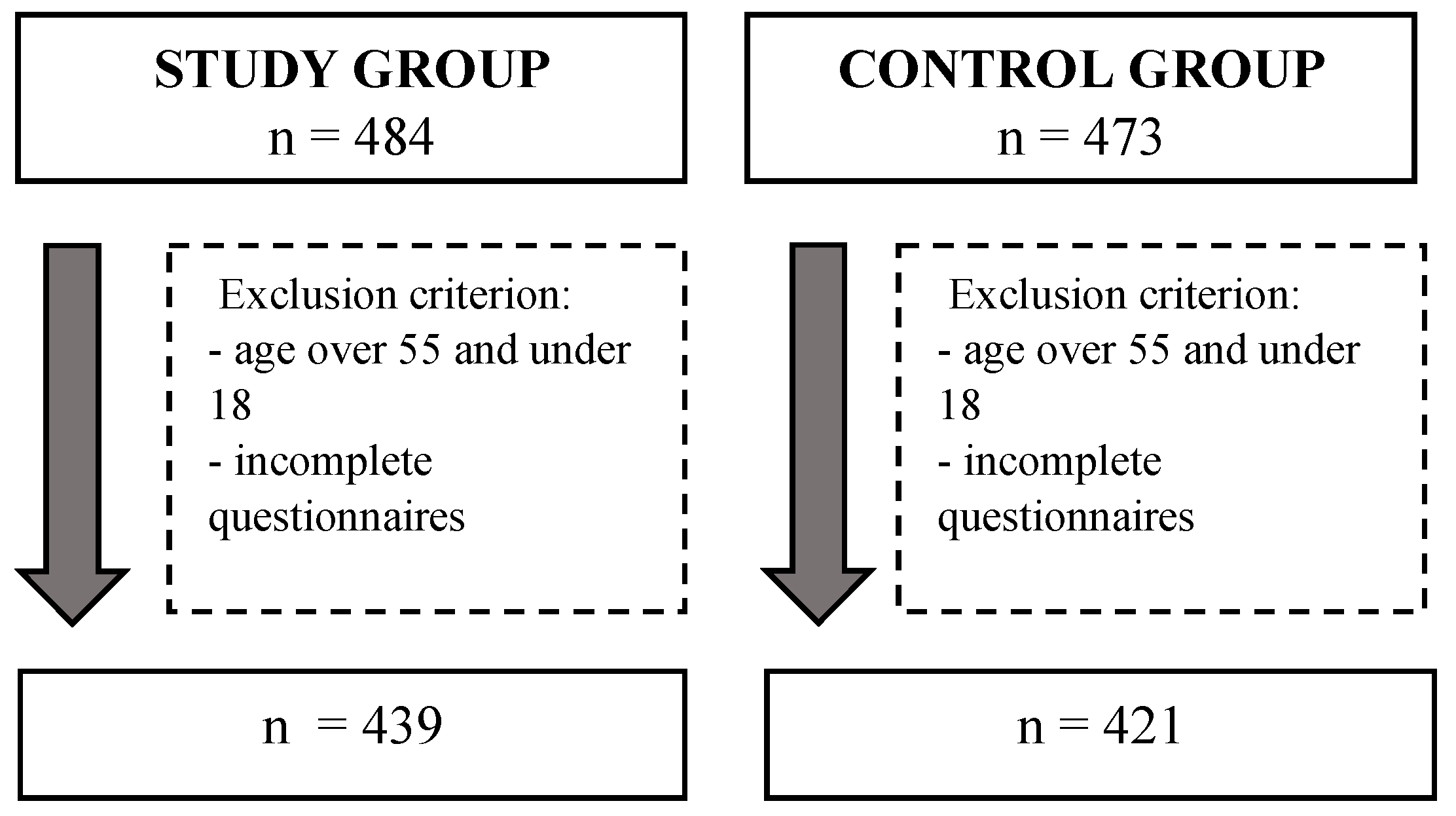
2.1. Survey Sample
2.2. Questionnaires
2.3. Statistical Analysis
3. Results
3.1. Group Characteristics
3.2. Quality of Life Assessment
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bulun, S.E.; Yilmaz, B.D.; Sison, C.; Miyazaki, K.; Bernardi, L.; Liu, S.; Kohlmeier, A.; Yin, P.; Milad, M.; Wei, J. Endometriosis. Endocr. Rev. 2019, 1, 1048–1079. [Google Scholar] [CrossRef]
- Scutiero, G.; Iannone, P.; Bernardi, G.; Bonaccorsi, G.; Spadaro, S.; Volta, C.A.; Greco, P.; Nappi, L. Oxidative Stress and Endometriosis: A Systematic Review of the Literature. Oxid. Med. Cell. Longev. 2017, 7265238. [Google Scholar] [CrossRef] [PubMed]
- Soliman, A.M.; Yang, H.; Du, E.X.; Kelley, C.; Winkel, C. The direct and indirect costs associated with endometriosis: A systematic literature review. Hum. Reprod. 2016, 31, 712–722. [Google Scholar] [CrossRef] [PubMed]
- Culley, L.; Law, C.; Hudson, N.; Denny, E.; Mitchell, H.; Baumgarten, M.; Raine-Fenning, N. The social and psychological impact of endometriosis on women’s lives: A critical narrative review. Hum. Reprod. Update 2013, 19, 625–639. [Google Scholar] [CrossRef] [Green Version]
- Wyderka, M.I.; Zalewska, D.; Szeląg, E. Endometriosis and the quality of life. Piel. Pol. 2011, 4, 199–206. [Google Scholar]
- Macer, M.L.; Taylor, H.S. Endometriosis and infertility: A review of the pathogenesis and treatment of endometriosis-associated infertility. Obstet. Gynecol. Clin. N. Am. 2012, 39, 535–549. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bonocher, C.M.; Montenegro, M.L.; Rosa, E.; Silva, J.C.; Ferriani, R.A.; Meola, J. Endometriosis and physical exercises: A systematic review. Reprod. Biol. Endocrinol. 2014, 6, 4. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burney, R.O.; Giudice, L.C. Pathogenesis and pathophysiology of endometriosis. Fertil. Steril. 2012, 98, 511–519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Della Corte, L.; Di Filippo, C.; Gabrielli, O.; Reppuccia, S.; La Rosa, V.L.; Ragusa, R.; Fichera, M.; Commodari, E.; Bifulco, G.; Giampaolino, P. The Burden of Endometriosis on Women`s Lifespan: A Narrative Overview on Quality of Life and Psychosocial Wellbeing. Int. J. Environ. Res. Public Health. 2020, 29, 4683. [Google Scholar] [CrossRef]
- Hemmert, R.; Schliep, K.C.; Willis, S.; Peterson, C.M.; Louis, G.B.; Allen-Brady, K.; Simonsen, S.E.; Stanford, J.B.; Byun, J.; Smith, K.R. Modifiable life style factors and risk for incident endometriosis. Paediatr. Perinat. Epidemiol. 2019, 33, 19–25. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Missmer, S.A.; Hankinson, S.E.; Spiegelman, D.; Barbieri, R.L.; Marshall, L.M.; Hunter, D.J. Incidence of laparoscopically confirmed endometriosis by demographic, anthropomet-ric, and lifestyle factors. Am. J. Epidemiol. 2004, 15, 784–796. [Google Scholar] [CrossRef] [PubMed]
- Sroślak, K.; Ziętalewicz, U.; Pyrcz, P. The impact of endometriosis and its treatment methods on the quality of life and sexual functioning of women—A review of the latest research. Przegl. Seks. 2017, 1, 17–24. [Google Scholar]
- Gordts, S.; Koninckx, P.; Brosens, I. Pathogenesis of deep endometriosis. Fertil. Steril. 2017, 108, 872–885.e1. [Google Scholar] [CrossRef] [Green Version]
- Audebert, A. Endométriose stade III et IV: Implications physiopathologiques, cliniques et thérapeutiques [Physiopathology, diagnosis and therapeutic management of stage III and IV endometriosis]. J. Gynecol. Obstet. Biol. Reprod. 2003, 32, 15–19. [Google Scholar]
- Smorgick, N.; As-Sanie, S.; Marsh, C.A.; Smith, Y.R.; Quint, E.H. Advanced stage endome-triosis in adolescents and young women. J. Pediatr. Adolesc. Gynecol. 2014, 27, 320–323. [Google Scholar] [CrossRef]
- Nisolle, M.; Nervo, P. Endométriose stade I et II: Implications physiopathologiques, cliniques et thérapeutiques [Physiopathology and therapeutic management of stage I and II endometriosis]. J. Gynecol. Obstet. Biol. Reprod. 2003, 32, 11–14. [Google Scholar]
- Cope, A.G.; VanBuren, W.M.; Sheedy, S.P. Endometriosis in the postmenopausal female: Clinical presentation, imaging features, and management. Abdom. Radiol. 2020, 45, 1790–1799. [Google Scholar] [CrossRef] [PubMed]
- Mundo-López, A.; Ocón-Hernández, O.; San-Sebastián, A.P.; Galiano-Castillo, N.; Rodríguez-Pérez, O.; Arroyo-Luque, M.S.; Arroyo-Morales, M.; Cantarero-Villanueva, I.; Fernández-Lao, C.; Artacho-Cordón, F. Contribution of Chronic Fatigue to Psychosocial Status and Quality of Life in Spanish Women Diagnosed with Endometriosis. Int. J. Environ. Res. Public Health 2020, 28, 3831. [Google Scholar] [CrossRef] [PubMed]
- Chapron, C.; Marcellin, L.; Borghese, B.; Santulli, P. Rethinking mechanisms, diagnosis and management of endometriosis. Nat. Rev. Endocrinol. 2019, 15, 666–682. [Google Scholar] [CrossRef] [PubMed]
- Pessoa de Farias Rodrigues, M.; Lima Vilarino, F.; de Souza Barbeiro Munhoz, A.; da Silva Paiva, L.; de Alcantara Sousa, L.V.; Zaia, V.; Parente Barbosa, C. Clinical aspects and the quality of life among women with endometriosis and infertility: A cross-sectional study. BMC Womens Health 2020, 12, 124. [Google Scholar] [CrossRef]
- La Rosa, V.L.; De Franciscis, P.; Barra, F.; Schiattarella, A.; Török, P.; Shah, M.; Karaman, E.; Marques Cerentini, T.; Di Guardo, F.; Gullo, G.; et al. Quality of life in women with endometriosis: A narrative overview. Minerva Med. 2020, 111, 68–78. [Google Scholar] [CrossRef]
- Rush, G.; Misajon, R. Examining subjective wellbeing and health-related quality of life in women with endometriosis. Health Care Women Int. 2018, 39, 303–321. [Google Scholar] [CrossRef]
- Huntington, A.; Gilmour, J.A. A life shaped by pain: Women and endometriosis. J. Clin. Nurs. 2005, 14, 1124–1132. [Google Scholar] [CrossRef]
- Sachedina, A.; Todd, N. Dysmenorrhea, Endometriosis and Chronic Pelvic Pain in Adolescents. J. Clin. Res. Pediatr. Endocrinol. 2020, 6, 7–17. [Google Scholar] [CrossRef] [PubMed]
- Joseph, S.; Mahale, S.D. Endometriosis Knowledgebase: A gene-based resource on endometriosis. Database 2019, baz062. [Google Scholar] [CrossRef] [Green Version]
- As-Sanie, S.; Black, R.; Giudice, L.C.; Gray Valbrun, T.; Gupta, J.; Jones, B.; Laufer, M.R.; Mil-spaw, A.T.; Missmer, S.A.; Norman, A.; et al. Assessing research gaps and unmet needs in endometriosis. Am. J. Obstet. Gynecol. 2019, 221, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Findeklee, S.; Radosa, J.C.; Hamza, A.; Haj Hamoud, B.; Iordache, I.; Sklavounos, P.; Takacs, Z.F.; Solomayer, E.F.; Radosa, M. Treatment algorithm for women with endometriosis in a certified Endometriosis Unit. Minerva Ginecol. 2020, 72, 43–49. [Google Scholar] [CrossRef]
- Facchin, F.; Barbara, G.; Saita, E.; Mosconi, P.; Roberto, A.; Fedele, L.; Vercellini, P. Impact of endometriosis on quality of life and mental health: Pelvic pain makes the difference. J. Psychosom. Obstet. Gynaecol. 2015, 36, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Friedl, F.; Riedl, D.; Fessler, S.; Wildt, L.; Walter, M.; Richter, R.; Schüßler, G.; Böttcher, B. Impact of endometriosis on quality of life, anxiety, and depression: An Austrian perspective. Arch. Gynecol. Obstet. 2015, 292, 1393–1399. [Google Scholar] [CrossRef]
- Chen, L.C.; Hsu, J.W.; Huang, K.L.; Bai, Y.M.; Su, T.P.; Li, C.T.; Yang, A.C.; Chang, W.H.; Chen, T.J.; Tsai, S.J.; et al. Risk of developing major depression and anxiety disorders among women with endometriosis: A longitudinal follow-up study. J. Affect. Disord. 2016, 190, 282–285. [Google Scholar] [CrossRef]
- Laganà, A.S.; Condemi, I.; Retto, G.; Muscatello, M.R.; Bruno, A.; Zoccali, R.A.; Triolo, O.; Cedro, C. Analysis of psychopathological comorbidity behind the common symptoms and signs of endometriosis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2015, 194, 30–33. [Google Scholar] [CrossRef] [PubMed]
- Biernat, E.; Stupnicki, R.; Gajewski, A.K. International Physical Activity Questionnaire (IPAQ)—Polish version. Wych. Fiz. Sport 2007, 51, 47–54. [Google Scholar]
- Biernat, E. International Physical Activity Questionnaire—Polish Long Version. Med. Sport. 2013, 1, 1–15. [Google Scholar]
- Craig, C.L.; Marshall, A.L.; Sjöström, M.; Bauman, A.E.; Booth, M.L.; Ainsworth, B.E.; Pratt, M.; Ekelund, U.; Yngve, A.; Sallis, J.F.; et al. International physical activity question-naire: 12-country reliability and validity. Med. Sci. Sports Exerc. 2003, 35, 1381–1395. [Google Scholar] [CrossRef] [Green Version]
- Meriwether, R.A.; McMahon, P.M.; Islam, N.; Steinmann, W.C. Physical activity as-sessment: Validation of a clinical assessment tool. Am. J. Prev. Med. 2006, 31, 484–491. [Google Scholar] [CrossRef]
- Neijenhuijs, K.I.; Hooghiemstra, N.; Holtmaat, K.; Aaronson, N.K.; Groenvold, M.; Holzner, B.; Terwee, C.B.; Cuijpers, P.; Verdonck-de Leeuw, I.M. The Female Sexual Function Index (FSFI)-A Systematic Review of Measurement Properties. J. Sex. Med. 2019, 16, 640–660. [Google Scholar] [CrossRef] [PubMed]
- Wiegel, M.; Meston, C.; Rosen, R. The female sexual function index (FSFI): Cross-validation and development of clinical cutoff scores. J. Sex. Marital. Ther. 2005, 31, 1–20. [Google Scholar] [CrossRef]
- Crisp, C.C.; Fellner, A.N.; Pauls, R.N. Validation of the Female Sexual Function Index (FSFI) for web-based administration. Int. Urogynecol. J. 2015, 26, 219–222. [Google Scholar] [CrossRef]
- Olssøn, I.; Mykletun, A.; Dahl, A.A. The Hospital Anxiety and Depression Rating Scale: Across-sectional study of psychometrics and case finding abilities in general practice. BMC Psychiatry 2005, 14, 46. [Google Scholar] [CrossRef] [Green Version]
- Krzemińska, S.A.; Magolan, J.; Borodzicz, A.; Arendarczyk, M. Selected emotional problems of caregivers of patients fed by gastrostomy in domestic environment. Piel. Zdr. Pub. 2017, 7, 117–123. [Google Scholar] [CrossRef]
- Mocny-Pachońska, K.; Trzcionka, A.; Doniec, R.J.; Sieciński, S.; Tanasiewicz, M. The Influence of Gender and Year of Study on Stress Levels and Coping Strategies among Polish Dental. Medicina 2020, 12, 531. [Google Scholar] [CrossRef]
- Białek, K.; Sadowski, M. Level of stress and strategies used to cope with stress by physicians working in intensive care units. Anaesthesiol. Intensive Ther. 2019, 51, 361–369. [Google Scholar] [CrossRef] [PubMed]
- Vitale, S.G.; La Rosa, V.L.; Rapisarda, A.M.; Laganà, A.S. Impact of endometriosis on quality of life and psychological well-being. J. Psychosom. Obstet. Gynaecol. 2016, 18, 1–3. [Google Scholar] [CrossRef]
- Pope, C.J.; Sharma, V.; Sharma, S.; Mazmanian, D. A systematic review of the association between psychiatric disturbances and endometriosis. J. Obstet. Gynaecol. Can. 2015, 37, 1006–1015. [Google Scholar] [CrossRef] [Green Version]
- Laganà, A.S.; La Rosa, V.; Petrosino, B.; Vitale, S.G. Comment on “Risk of developing major depression and anxiety disorders among women with endometriosis: A longitudinal follow-up study”. J. Affect. Disord. 2017, 208, 672–673. [Google Scholar] [CrossRef]
- Sepulcri Rde, P.; do Amaral, V.F. Depressive symptoms, anxiety, and quality of life in women with pelvic endometriosis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2009, 142, 53–56. [Google Scholar] [CrossRef]
- Hassa, H.; Tanir, H.M.; Uray, M. Symptom distribution among infertile and fertile endometriosis cases with different stages and localisations. Eur. J. Obstet. Gynecol. Reprod. Biol. 2005, 119, 82–86. [Google Scholar] [CrossRef]
- Warzecha, D.; Szymusik, I.; Wielgos, M.; Pietrzak, B. The Impact of Endometriosis on the Quality of Life and the Incidence of Depression-A Cohort Study. Int. J. Environ. Res. Public Health 2020, 17, 3641. [Google Scholar] [CrossRef] [PubMed]
- Eriksen, H.L.; Gunnersen, K.F.; Sørensen, J.A.; Munk, T.; Nielsen, T.; Knudsen, U.B. Psychological aspects of endometriosis: Differences between patients with or without pain on four psychological variables. Eur. J. Obstet. Gynecol. Reprod. Biol. 2008, 139, 100–105. [Google Scholar] [CrossRef]
- Tripoli, T.M.; Sato, H.; Sartori, M.G.; de Araujo, F.F.; Girão, M.J.; Schor, E. Evaluation of quality of life and sexual satisfaction in women suffering from chronic pelvic pain with or without endometriosis. J. Sex. Med. 2011, 8, 497–503. [Google Scholar] [CrossRef]
- Souza, C.A.; Oliveira, L.M.; Scheffel, C.; Genro, V.K.; Rosa, V.; Chaves, M.F.; Cunha Filho, J.S. Quality of life associated to chronic pelvic pain is independent of endometriosis diagnosis—A cross-sectional survey. Health Qual. Life Outcomes 2011, 9, 41. [Google Scholar] [CrossRef] [Green Version]
- Kumar, A.; Gupta, V.; Maurya, A. Mental health and quality of life of chronic pelvic pain and endometriosis patients. J. Proj. Psychol. Ment. Health. 2010, 17, 153–157. [Google Scholar]
- Lorençatto, C.; Petta, C.A.; Navarro, M.J.; Bahamondes, L.; Matos, A. Depression in women with endometriosis with and without chronic pelvic pain. Acta Obstet. Gynecol. Scand. 2006, 85, 88–92. [Google Scholar] [CrossRef]
- Roth, R.S.; Punch, M.; Bachman, J.E. Psychological factors in chronic pelvic pain due to endometriosis: A comparative study. Gynecol. Obstet. Investig. 2011, 72, 15–19. [Google Scholar] [CrossRef]
- Missmer, S.A.; Tu, F.F.; Agarwal, S.K.; Chapron, C.; Soliman, A.M.; Chiuve, S.; Eichner, S.; Flores-Caldera, I.; Horne, A.W.; Kimball, A.B.; et al. Impact of Endometriosis on Life-Course Potential: A Narrative Review. Int. J. Gen. Med. 2021, 14, 9–25. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Xu, X.; Lin, L.; Xu, K.; Xu, M.; Ye, J.; Shen, X. Sexual function in patients with endometriosis: A prospective case-control study in China. J. Int. Med. Res. 2021, 49, 3000605211004388. [Google Scholar] [CrossRef]
- Grangier, L.; Aerts, L.; Pluchino, N. Les dyspareunies chez les patientes atteintes d’endométriose [Clinical investigation of Sexual pain in patients with endometriosis]. Rev. Med. Suisse 2019, 15, 1941–1944. [Google Scholar]
- Youseflu, S.; Jahanian Sadatmahalleh, S.; Bahri Khomami, M.; Nasiri, M. Influential factors on sexual function in infertile women with endometriosis: A path analysis. BMC Womens Health 2020, 20, 92. [Google Scholar] [CrossRef]
- Vercellini, P.; Viganò, P.; Somigliana, E.; Fedele, L. Endometriosis: Pathogenesis and treatment. Nat. Rev. Endocrinol. 2014, 10, 261–275.44. [Google Scholar] [CrossRef] [PubMed]
- Fairbanks, F.; Abdo, C.H.; Baracat, E.C.; Podgaec, S. Endometriosis doubles the risk of sexual dysfunction: A cross-sectional study in a large amount of patients. Gynecol. Endocrinol. 2017, 33, 544–547. [Google Scholar] [CrossRef]
- Ferrero, S.; Abbamonte, L.H.; Parisi, M.; Ragni, N.; Remorgida, V. Dyspareunia and quality of sex life after laparoscopic excision of endometriosis and postoperative administration of triptorelin. Fertil. Steril. 2007, 87, 227–229. [Google Scholar] [CrossRef]
- Denny, E.; Mann, C.H. Endometriosis-associated dyspareunia: The impact on women’s lives. J. Fam. Plann. Reprod. Health Care 2007, 33, 189–193. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Aerts, L.; Grangier, L.; Streuli, I.; Dällenbach, P.; Marci, R.; Wenger, J.M.; Pluchino, N. Psychosocial impact of endometriosis: From co-morbidity to intervention. Best Pract. Res. Clin. Obstet. Gynaecol. 2018, 50, 2–10. [Google Scholar] [CrossRef]
- Pluchino, N.; Wenger, J.M.; Petignat, P.; Tal, R.; Bolmont, M.; Taylor, H.S.; Bianchi-Demicheli, F. Sexual function in endometriosis patients and their partners: Effect of the disease and consequences of treatment. Hum. Reprod. Update 2016, 22, 762–774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hämmerli, S.; Kohl-Schwartz, A.; Imesch, P.; Rauchfuss, M.; Wölfler, M.M.; Häberlin, F.; von Orelli, S.; Leeners, B. Sexual Satisfaction and Frequency of Orgasm in Women with Chronic Pelvic Pain due to Endometriosis. J. Sex. Med. 2020, 17, 2417–2426.50. [Google Scholar] [CrossRef]
- Fritzer, N.; Haas, D.; Oppelt, P.; Renner, S.; Hornung, D.; Wölfler, M.; Ulrich, U.; Fischerlehner, G.; Sillem, M.; Hudelist, G. More than just bad sex: Sexual dysfunction and distress in patients with endometriosis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2013, 169, 392–396. [Google Scholar] [CrossRef] [PubMed]
- Youseflu, S.; Jahanian Sadatmahalleh, S.; Roshanzadeh, G.; Mottaghi, A.; Kazemnejad, A.; Moini, A. Effects of endometriosis on sleep quality of women: Does life style factor make a difference? BMC Womens Health 2020, 10, 168. [Google Scholar] [CrossRef]
- De Graaff, A.A.; Van Lankveld, J.; Smits, L.J.; Van Beek, J.J.; Dunselman, G.A. Dyspareunia and depressive symptoms are associated with impaired sexual functioning in women with endometriosis, whereas sexual functioning in their male partners is not affected. Hum. Reprod. 2016, 31, 2577–2586. [Google Scholar] [CrossRef] [Green Version]
- Donatti, L.; Ramos, D.G.; Andres, M.P.; Passman, L.J.; Podgaec, S. Patients with endometriosis using positive coping strategies have less depression, stress and pelvic pain. Einstein 2017, 15, 65–70. [Google Scholar] [CrossRef] [Green Version]
- Awad, E.; Ahmed, H.A.H.; Yousef, A.; Abbas, R. Efficacy of exercise on pelvic pain and posture associated with endometriosis: Within subject design. J. Phys. Ther. Sci. 2017, 29, 2112–2115. [Google Scholar] [CrossRef] [Green Version]
- Leonardi, M.; Horne, A.W.; Vincent, K.; Sinclair, J.; Sherman, K.A.; Ciccia, D.; Condous, G.; Johnson, N.P.; Armour, M. Self-management strategies to consider to combat endometriosis symptoms during the COVID-19 pandemic. Hum. Reprod. Open. 2020, 1, hoaa028. [Google Scholar] [CrossRef] [PubMed]
- Bergström, I.; Freyschuss, B.; Jacobsson, H.; Landgren, B.M. The effect of physical training on bone mineral density in women with endometriosis treated with GnRH analogs: A pilot study. Acta Obstet. Gynecol. Scand. 2005, 84, 380–383. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Wu, H.; Zhou, X.; Wang, Q.; Zhu, W.; Chen, J. Effects of progressive muscular relaxation training on anxiety, depression and quality of life of endometriosis patients under gonadotrophin-releasing hormone agonist therapy. Eur. J. Obstet. Gynecol. Reprod. Biol. 2012, 162, 211–215. [Google Scholar] [CrossRef]
- Stanton, A.M.; Handy, A.B.; Meston, C.M. The Effects of Exercise on Sexual Function in Women. Sex. Med. Rev. 2018, 6, 548–557. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Variable | Group B | Group C | p-Value | |||
|---|---|---|---|---|---|---|
| M | Min–Max | M | Min–Max | |||
| Age | 33.1 | 19.0–55.0 | 32.6 | 18.0–50.0 | 0.235 | |
| N | % | N | % | p-Value | ||
| Education | Primary | 5 | 1.13% | 3 | 0.71% | <0.001 * |
| junior high school | 2 | 0.45% | 5 | 1.18% | ||
| vocational | 4 | 0.91% | 16 | 3.80% | ||
| secondary | 106 | 24.14% | 163 | 38.71% | ||
| Higher | 322 | 73.34% | 234 | 55.58% | ||
| Menstrual cycle | stopped by medication | 123 | 14.30% | 28 | 3.26% | <0.001 * |
| Regular | 138 | 16.05% | 172 | 20.00% | ||
| quite regular | 119 | 13.84% | 173 | 20.12% | ||
| irregular | 53 | 6.16% | 47 | 5.47% | ||
| I am bleeding all the time | 6 | 0.70% | 1 | 0.12% | ||
| Occurrence of miscarriage | Yes | 70 | 13.49% | 65 | 12.52% | 0.249 |
| No | 177 | 34.10% | 207 | 39.88% | ||
| Multiple pregnancies | one child | 172 | 43.11% | 203 | 50.88% | 0.746 |
| Twins | 9 | 2.26% | 14 | 3.51% | ||
| triplets or more | 0 | 0.00% | 1 | 0.25% | ||
| Smoking cigarettes | Yes | 62 | 14.12% | 106 | 25.17% | <0.001 * |
| No | 377 | 85.87% | 315 | 74.82% | ||
| Drinking alcohol | does not drink | 92 | 10.71% | 71 | 8.27% | 0.017 * |
| occasionally | 233 | 27.12% | 210 | 24.45% | ||
| once a week | 76 | 8.85% | 75 | 8.73% | ||
| once a month | 35 | 4.07% | 58 | 6.75% | ||
| every day | 2 | 0.23% | 7 | 0.81% | ||
| Variable (Age) | Stage I | Stage II | Stage III | Stage IV | p-Value |
|---|---|---|---|---|---|
| 18–25 years old | 20 | 10 | 6 | 10 | 0.046 * |
| 25–35 years old | 71 | 42 | 50 | 73 | |
| 35–45 years old | 40 | 23 | 25 | 62 | |
| Above 45 years old | 3 | 2 | 1 | 1 | |
| Overall | 134 (30.5%) | 77 (17.5%) | 82 (18.7%) | 146 (33.3%) |
| Variable | Group B | Group C | p-Value | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| M | Min | Max | SD | M | Min | Max | SD | |||
| HADS | Depression | 8.78 | 2.00 | 18.00 | 2.50 | 5.08 | 0.00 | 18.00 | 3.15 | <0.001 * |
| Anxiety | 11.48 | 5.00 | 18.00 | 3.00 | 8.66 | 0.00 | 20.00 | 3.90 | <0.001 * | |
| FSFI | Overall | 21.30 | 0.00 | 46.50 | 7.04 | 23.89 | 1.20 | 34.40 | 6.97 | <0.001 * |
| Desire | 1.88 | 0.00 | 4.80 | 1.30 | 2.78 | 0.00 | 4.80 | 1.28 | <0.001 * | |
| Excitement | 3.71 | 0.00 | 6.00 | 1.57 | 4.36 | 0.00 | 6.00 | 1.57 | <0.001 * | |
| Lubrication | 4.08 | 0.00 | 6.00 | 1.69 | 4.83 | 0.00 | 6.00 | 1.66 | <0.001 * | |
| Orgasm | 3.90 | 0.00 | 6.00 | 1.68 | 4.37 | 0.00 | 6.00 | 1.74 | <0.001 * | |
| Satisfaction | 3.43 | 0.00 | 5.60 | 1.40 | 3.80 | 0.00 | 5.20 | 1.27 | <0.001 * | |
| Pain | 3.51 | 0.00 | 6.00 | 1.56 | 2.21 | 0.00 | 6.00 | 1.30 | <0.001 * | |
| IPAQ | 793.79 | 0.00 | 10,956.00 | 1123.05 | 834.02 | 0.00 | 14,680.00 | 1137.22 | 0.135 | |
| Mini-COPE | Active coping | 1.89 | 0.00 | 3.00 | 0.83 | 2.05 | 0.00 | 3.00 | 0.74 | 0.012 * |
| Planning | 1.84 | 0.00 | 3.00 | 0.86 | 1.89 | 0.00 | 3.00 | 0.77 | 0.606 | |
| Positive reframing and development | 1.33 | 0.00 | 3.00 | 0.87 | 1.58 | 0.00 | 3.00 | 0.78 | <0.001 * | |
| Acceptance | 1.59 | 0.00 | 3.00 | 0.82 | 1.70 | 0.00 | 3.00 | 0.75 | 0.069 | |
| Turning to religion | 0.71 | 0.00 | 3.00 | 0.86 | 0.67 | 0.00 | 3.00 | 0.91 | 0.246 | |
| Sense of humour | 0.67 | 0.00 | 3.00 | 0.62 | 0.81 | 0.00 | 3.00 | 0.66 | 0.002 * | |
| Seeking emotional support | 1.62 | 0.00 | 3.00 | 0.90 | 1.67 | 0.00 | 3.00 | 0.93 | 0.424 | |
| Self-distraction | 1.56 | 0.00 | 3.00 | 0.84 | 1.62 | 0.00 | 3.00 | 0.80 | 0.382 | |
| Seeking instrumental support | 1.55 | 0.00 | 3.00 | 0.88 | 1.43 | 0.00 | 3.00 | 1.03 | 0.049 * | |
| Denial | 0.75 | 0.00 | 3.00 | 0.76 | 0.75 | 0.00 | 3.00 | 0.76 | 0.970 | |
| Venting | 1.42 | 0.00 | 3.00 | 0.71 | 1.49 | 0.00 | 3.00 | 0.73 | 0.216 | |
| Use of alcohol and psychoactive substances | 0.36 | 0.00 | 3.00 | 0.66 | 0.45 | 0.00 | 3.00 | 0.76 | 0.293 | |
| Discontinuation of actions | 0.79 | 0.00 | 3.00 | 0.71 | 0.67 | 0.00 | 3.00 | 0.70 | 0.005 * | |
| Self-blame | 1.33 | 0.00 | 3.00 | 0.87 | 1.38 | 0.00 | 3.00 | 0.93 | 0.541 | |
| Variable | Group B | Group C | ||||
|---|---|---|---|---|---|---|
| R | p-Value | R | p-Value | |||
| HADS | Depression | FSFI-overall | −0.10971 | 0.021 * | −0.31206 | <0.001 * |
| FSFI-desire | −0.1109 | 0.020 * | −0.3004 | <0.001 * | ||
| FSFI–excitement | −0.1203 | 0.012 * | −0.2310 | <0.001 * | ||
| FSFI–lubrication | −0.0381 | 0.427 | −0.2448 | <0.001 * | ||
| FSFI–orgasm | −0.0812 | 0.090 | −0.2529 | <0.001 * | ||
| FSFI–satisfaction | −0.1051 | 0.028 * | −0.2860 | <0.001 * | ||
| FSFI-pain | 0.0552 | 0.250 | 0.0839 | 0.086 | ||
| IPAQ | −0.01737 | 0.717 | −0.14881 | 0.002 * | ||
| Anxiety | FSFI-overall | −0.18758 | <0.001 * | −0.33007 | <0.001 * | |
| FSFI-desire | −0.1346 | 0.005 * | −0.2522 | <0.001 * | ||
| FSFI–excitement | −0.1203 | 0.012 * | −0.2806 | <0.001 * | ||
| FSFI–lubrication | −0.1586 | 0.001 * | −0.2408 | <0.001 * | ||
| FSFI–orgasm | −0.1451 | 0.002 * | −0.2915 | <0.001 * | ||
| FSFI–satisfaction | −0.2215 | <0.001 * | −0.3041 | <0.001 * | ||
| FSFI-pain | 0.2046 | <0.001 * | 0.2542 | <0.001 * | ||
| IPAQ | 0.07447 | 0.119 | −0.00489 | 0.920 | ||
| IPAQ | FSFI-overall | −0.00926 | 0.847 | 0.02139 | 0.662 | |
| FSFI-desire | 0.0572 | 0.233 | −0.0471 | 0.335 | ||
| FSFI–excitement | −0.0497 | 0.300 | −0.0117 | 0.811 | ||
| FSFI–lubrication | −0.0085 | 0.860 | −0.0061 | 0.901 | ||
| FSFI–orgasm | −0.0585 | 0.222 | −0.0589 | 0.228 | ||
| FSFI–satisfaction | −0.0034 | 0.944 | −0.0262 | 0.593 | ||
| FSFI-pain | 0.0908 | 0.058 | −0.0065 | 0.894 | ||
| HADS depression | −0.01737 | 0.717 | −0.14881 | 0.002 * | ||
| HADS anxiety | 0.07447 | 0.119 | −0.00489 | 0.920 | ||
| Variable | Stage I | Stage II | Stage III | Stage IV | ||||||
|---|---|---|---|---|---|---|---|---|---|---|
| R | p | R | p | R | p | R | p | |||
| IPAQ | HADS | Depression | 0.00902 | 0.918 | −0.02735 | 0.813 | 0.04737 | 0.672 | −0.07507 | 0.368 |
| Anxiety | 0.00211 | 0.981 | 0.27574 | 0.015 * | 0.08742 | 0.435 | 0.03464 | 0.678 | ||
| FSFI | 0.01889 | 0.828 | 0.07788 | 0.501 | −0.06894 | 0.538 | −0.04495 | 0.590 | ||
| Mini-COPE | Active coping | 0.14862 | 0.087 | 0.03549 | 0.759 | 0.23342 | 0.035 * | 0.09011 | 0.279 | |
| Planning | 0.06983 | 0.423 | 0.07719 | 0.505 | 0.32578 | 0.003 * | 0.16344 | 0.049 * | ||
| Positive reframing and development | 0.00002 | 0.999 | 0.01418 | 0.903 | 0.19491 | 0.079 | 0.10674 | 0.199 | ||
| Acceptance | 0.15535 | 0.073 | 0.06890 | 0.552 | 0.23033 | 0.037 * | 0.01722 | 0.837 | ||
| Turning to religion | −0.00363 | 0.967 | 0.18934 | 0.099 | −0.00890 | 0.937 | 0.12492 | 0.133 | ||
| Sense of humour | 0.05783 | 0.507 | 0.10948 | 0.343 | −0.05839 | 0.602 | −0.00235 | 0.978 | ||
| Seeking emotional support | −0.04981 | 0.568 | 0.12528 | 0.278 | 0.08316 | 0.458 | −0.01202 | 0.885 | ||
| Self-distraction | 0.07032 | 0.419 | 0.30425 | 0.007 * | 0.24565 | 0.026* | 0.21765 | 0.008 * | ||
| Seeking instrumental support | −0.01219 | 0.889 | 0.15562 | 0.179 | 0.14545 | 0.195 | −0.05164 | 0.536 | ||
| Denial | −0.12039 | 0.166 | 0.02912 | 0.801 | 0.02451 | 0.827 | 0.25349 | 0.002 * | ||
| Venting | −0.01942 | 0.824 | −0.15412 | 0.181 | −0.10949 | 0.327 | 0.05590 | 0.503 | ||
| Use of alcohol and psychoactive substances | −0.11449 | 0.188 | 0.24961 | 0.029 * | 0.01804 | 0.872 | −0.02620 | 0.754 | ||
| Discontinuation of actions | 0.02184 | 0.802 | 0.09309 | 0.421 | 0.01248 | 0.911 | 0.12836 | 0.123 | ||
| Self-blame | −0.09049 | 0.298 | 0.08668 | 0.454 | 0.10695 | 0.339 | 0.07351 | 0.378 | ||
| Variable | Age | Education Level | Cigarette Smoking | |||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | p-Value | 95% CI | β | p-Value | 95% CI | β | p-Value | 95% CI | ||||
| HADS-depression | 0.047954 | 0.358 | −0.05451 | 0.150421 | −0.08742 | 0.094 | −0.18985 | 0.015016 | 0.040992 | 0.439 | −0.06304 | 0.145019 |
| HADS-anxiety | −0.12881 | 0.014 * | −0.23178 | −0.02583 | −0.08084 | 0.123 | −0.18378 | 0.022105 | −0.05813 | 0.275 | −0.16267 | 0.046417 |
| FSFI | −0.14992 | 0.001 * | −0.24384 | −0.05599 | −0.09718 | 0.043 * | −0.19108 | −0.00329 | −0.02813 | 0.562 | −0.12348 | 0.067228 |
| IPAQ | 0.074198 | 0.117 | −0.01853 | 0.166922 | −0.1074 | 0.023 * | −0.20009 | −0.01471 | 0.063958 | 0.182 | −0.03018 | 0.158093 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mińko, A.; Turoń-Skrzypińska, A.; Rył, A.; Bargiel, P.; Hilicka, Z.; Michalczyk, K.; Łukowska, P.; Rotter, I.; Cymbaluk-Płoska, A. Endometriosis—A Multifaceted Problem of a Modern Woman. Int. J. Environ. Res. Public Health 2021, 18, 8177. https://doi.org/10.3390/ijerph18158177
Mińko A, Turoń-Skrzypińska A, Rył A, Bargiel P, Hilicka Z, Michalczyk K, Łukowska P, Rotter I, Cymbaluk-Płoska A. Endometriosis—A Multifaceted Problem of a Modern Woman. International Journal of Environmental Research and Public Health. 2021; 18(15):8177. https://doi.org/10.3390/ijerph18158177
Chicago/Turabian StyleMińko, Alicja, Agnieszka Turoń-Skrzypińska, Aleksandra Rył, Patrycja Bargiel, Zuzanna Hilicka, Kaja Michalczyk, Paulina Łukowska, Iwona Rotter, and Aneta Cymbaluk-Płoska. 2021. "Endometriosis—A Multifaceted Problem of a Modern Woman" International Journal of Environmental Research and Public Health 18, no. 15: 8177. https://doi.org/10.3390/ijerph18158177
APA StyleMińko, A., Turoń-Skrzypińska, A., Rył, A., Bargiel, P., Hilicka, Z., Michalczyk, K., Łukowska, P., Rotter, I., & Cymbaluk-Płoska, A. (2021). Endometriosis—A Multifaceted Problem of a Modern Woman. International Journal of Environmental Research and Public Health, 18(15), 8177. https://doi.org/10.3390/ijerph18158177