
Minimum Detectable Change of Visual Acuity Measurements Using ETDRS Charts (Early Treatment Diabetic Retinopathy Study)

 ,
,  , , and
, , and 
{kind=link}
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design
2.2. Subjects
2.3. Study Procedure
2.4. Statistical Analysis
3. Results
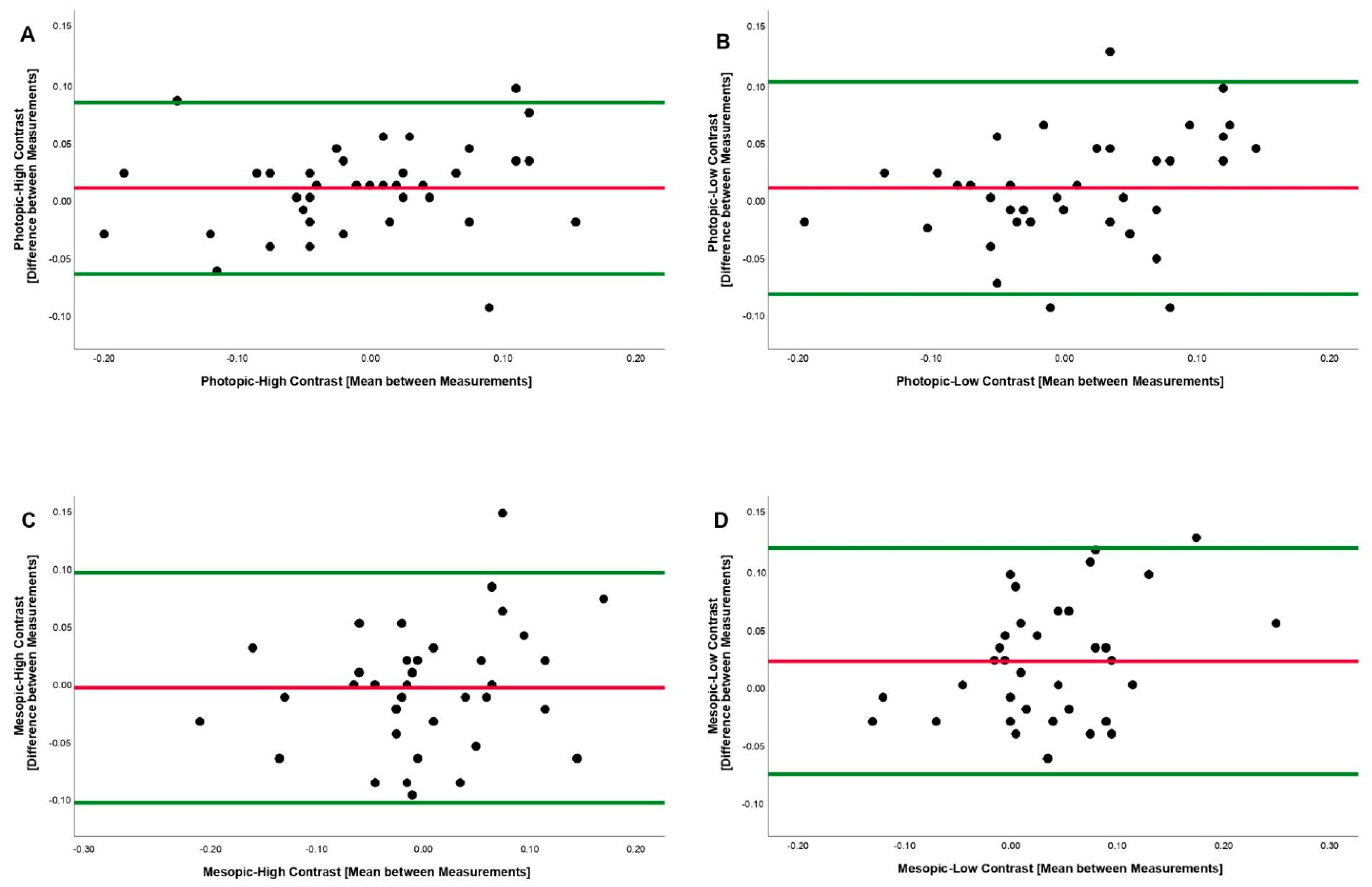
3.1. Photopic and High Contrast
3.2. Photopic and Low Contrast
3.3. Mesopic and High Contrast
3.4. Mesopic and Low Contrast
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Manny, R.E.; Hussein, M.; Gwiazda, J.; Marsh-Tootle, W. Repeatability of ETDRS Visual Acuity in Children. Investig. Opthalmol. Vis. Sci. 2003, 44, 3294–3300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bailey, I.L.; Lovie, J.E. New design principles for visual acuity letter charts. Am. J. Optom. Physiol. Opt. 1976, 53, 740–745. [Google Scholar] [CrossRef] [PubMed]
- Ferris, F.L., 3rd; Kassoff, A.; Bresnick, G.H.; Bailey, I. New visual acuity charts for clinical research. Am. J. Ophthalmol. 1982, 94, 91–96. [Google Scholar] [CrossRef]
- Koenig, S.; Tonagel, F.; Schiefer, U.; Bach, M.; Heinrich, S.P. Assessing visual acuity across five disease types: ETDRS charts are faster with clinical outcome comparable to Landolt Cs. Graefes Arch. Clin. Exp. Ophthalmol. 2014, 252, 1093–1099. [Google Scholar] [CrossRef] [PubMed]
- Solomon, S.D.; Goldberg, M.F. ETDRS Grading of Diabetic Retinopathy: Still the Gold Standard? Ophthalmic Res. 2019, 62, 190–195. [Google Scholar] [CrossRef] [PubMed]
- Shah, N.; Laidlaw, D.A.H.; Shah, S.P.; Sivasubramaniam, S.; Bunce, C.; Cousens, S. Computerized Repeating and Averaging Improve the Test-Retest Variability of ETDRS Visual Acuity Measurements: Implications for Sensitivity and Specificity. Investig. Opthalmol. Vis. Sci. 2011, 52, 9397–9402. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rosser, D.A.; Murdoch, I.E.; Fitzke, F.W.; Laidlaw, D.A.H. Improving on ETDRS acuities: Design and results for a computerised thresholding device. Eye 2003, 17, 701–706. [Google Scholar] [CrossRef] [Green Version]
- Barrio, A.; Antona, B.; Puell, M.C. Repeatability of mesopic visual acuity measurements using high- and low-contrast ETDRS letter charts. Graefe’s Arch. Clin. Exp. Ophthalmol. 2015, 253, 791–795. [Google Scholar] [CrossRef]
- Chaikitmongkol, V.; Nanegrungsunk, O.; Patikulsila, D.; Ruamviboonsuk, P.; Bressler, N.M. Repeatability and Agreement of Visual Acuity Using the ETDRS Number Chart, Landolt C Chart, or ETDRS Alphabet Chart in Eyes With or Without Sight-Threatening Diseases. JAMA Ophthalmol. 2018, 136, 286–290. [Google Scholar] [CrossRef]
- Patel, P.J.; Chen, F.K.; Rubin, G.S.; Tufail, A. Intersession repeatability of visual acuity scores in age-related macular degeneration. Investig. Ophthalmol. Vis. Sci. 2008, 49, 4347–4352. [Google Scholar] [CrossRef] [Green Version]
- Lin, Z.; Wu, C.; Chen, X.; He, M. [Repeatability of ETDRS visual acuity measurement in children]. Yan Ke Xue Bao = Eye Sci. 2008, 24, 48–52. [Google Scholar]
- Ruamviboonsuk, P.; Tiensuwan, M.; Kunawut, C.; Masayaanon, P. Repeatability of an automated Landolt C test, compared with the early treatment of diabetic retinopathy study (ETDRS) chart testing. Am. J. Ophthalmol. 2003, 136, 662–669. [Google Scholar] [CrossRef]
- Kuo, H.-K.; Kuo, M.-T.; Tiong, I.-S.; Wu, P.-C.; Chen, Y.-J.; Chen, C.-H. Visual acuity as measured with Landolt C chart and Early Treatment of Diabetic Retinopathy Study (ETDRS) chart. Graefes Arch. Clin. Exp. Ophthalmol. 2011, 249, 601–605. [Google Scholar] [CrossRef] [PubMed]
- Falkenstein, I.A.; Cochran, D.E.; Azen, S.P.; Dustin, L.; Tammewar, A.M.; Kozak, I.; Freeman, W.R. Comparison of Visual Acuity in Macular Degeneration Patients Measured with Snellen and Early Treatment Diabetic Retinopathy Study Charts. Ophthalmology 2008, 115, 319–323. [Google Scholar] [CrossRef] [Green Version]
- Kaiser, P.K. Prospective evaluation of visual acuity assessment: A comparison of snellen versus ETDRS charts in clinical practice (An AOS Thesis). Trans. Am. Ophthalmol. Soc. 2009, 107, 311–324. [Google Scholar]
- Jolly, J.K.; Juenemann, K.; Boagey, H.; Nadsady, M.; Bridge, H.; Maclaren, R.E. Validation of electronic visual acuity (EVA) measurement against standardised ETDRS charts in patients with visual field loss from inherited retinal degenerations. Br. J. Ophthalmol. 2020, 104, 924–931. [Google Scholar] [CrossRef] [PubMed]
- Beck, R.W.; Moke, P.S.; Turpin, A.H.; Ferris, F.L.; SanGiovanni, J.P.; Johnson, C.A.; Birch, E.E.; Chandler, D.L.; Cox, T.A.; Blair, R.C.; et al. A computerized method of visual acuity testing: Adaptation of the early treatment of diabetic retinopathy study testing protocol. Am. J. Ophthalmol. 2003, 135, 194–205. [Google Scholar] [CrossRef]
- Cotter, S.A.; Chu, R.H.; Chandler, D.L.; Beck, R.W.; Holmes, J.M.; Rice, M.L.; Hertle, R.W.; Birch, E.E.; Moke, P.S. Reliability of the electronic early treatment diabetic retinopathy study testing protocol in children 7 to. Am. J. Ophthalmol. 2003, 136, 655–661. [Google Scholar] [CrossRef]
- Laidlaw, D.A.H.; Tailor, V.; Shah, N.; Atamian, S.; Harcourt, C. Validation of a computerised logMAR visual acuity measurement system (COMPlog): Comparison with ETDRS and the electronic ETDRS testing algorithm in adults and amblyopic children. Br. J. Ophthalmol. 2008, 92, 241–244. [Google Scholar] [CrossRef]
- Turner, D.; Schünemann, H.J.; Griffith, L.E.; Beaton, D.E.; Griffiths, A.M.; Critch, J.N.; Guyatt, G.H. The minimal detectable change cannot reliably replace the minimal important difference. J. Clin. Epidemiol. 2010, 63, 28–36. [Google Scholar] [CrossRef] [PubMed]
- Lam, A.K.; Tong, C.; Tse, J.; Yu, M. Repeatability of near visual acuity measurement at high and low contrast. Clin. Exp. Optom. 2008, 91, 447–452. [Google Scholar] [CrossRef]
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J. Chiropr. Med. 2016, 15, 155–163. [Google Scholar] [CrossRef] [Green Version]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef] [Green Version]
- Weir, J.P. Quantifying test-retest reliability using the intraclass correlation coefficient and the SEM. J. Strength Cond. Res. 2005, 19, 231–240. [Google Scholar] [CrossRef] [PubMed]
- Bland, J.M.; Altman, D.G. Statistical methods for assessing agreement between two methods of clinical measurement. Lancet 1986, 1, 307–310. [Google Scholar] [CrossRef]
- Camparini, M.; Cassinari, P.; Ferrigno, L.; Macaluso, C. ETDRS-fast: Implementing psychophysical adaptive methods to standardized visual acuity measurement with ETDRS charts. Investig. Ophthalmol. Vis. Sci. 2001, 42, 1226–1231. [Google Scholar]
- Lee, H.S.; Park, S.W.; Chung, H.K. The Korean version of relative and absolute reliability of gait and balance assessment tools for patients with dementia in day care center and nursing home. J. Phys. Ther. Sci. 2017, 29, 1934–1939. [Google Scholar] [CrossRef] [Green Version]
- Pang, Y.; Sparschu, L.; Nylin, E. Validation of an automated-ETDRS near and intermediate visual acuity measurement. Clin. Exp. Optom. 2020, 103, 663–667. [Google Scholar] [CrossRef]
- Yu, H.J.; Kaiser, P.K.; Zamora, D.; Bocanegra, M.; Cone, C.; Brown, D.M.; Sadda, S.R.; Wykoff, C.C. Visual Acuity Variability: Comparing Discrepancies between Snellen and ETDRS Measurements among Subjects Entering Prospective Trials. Ophthalmol. Retin. 2021, 5, 224–233. [Google Scholar] [CrossRef] [PubMed]

Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sánchez-González, M.C.; García-Oliver, R.; Sánchez-González, J.-M.; Bautista-Llamas, M.-J.; Jiménez-Rejano, J.-J.; De-Hita-Cantalejo, C. Minimum Detectable Change of Visual Acuity Measurements Using ETDRS Charts (Early Treatment Diabetic Retinopathy Study). Int. J. Environ. Res. Public Health 2021, 18, 7876. https://doi.org/10.3390/ijerph18157876
Sánchez-González MC, García-Oliver R, Sánchez-González J-M, Bautista-Llamas M-J, Jiménez-Rejano J-J, De-Hita-Cantalejo C. Minimum Detectable Change of Visual Acuity Measurements Using ETDRS Charts (Early Treatment Diabetic Retinopathy Study). International Journal of Environmental Research and Public Health. 2021; 18(15):7876. https://doi.org/10.3390/ijerph18157876
Chicago/Turabian StyleSánchez-González, María Carmen, Raquel García-Oliver, José-María Sánchez-González, María-José Bautista-Llamas, José-Jesús Jiménez-Rejano, and Concepción De-Hita-Cantalejo. 2021. "Minimum Detectable Change of Visual Acuity Measurements Using ETDRS Charts (Early Treatment Diabetic Retinopathy Study)" International Journal of Environmental Research and Public Health 18, no. 15: 7876. https://doi.org/10.3390/ijerph18157876
APA StyleSánchez-González, M. C., García-Oliver, R., Sánchez-González, J.-M., Bautista-Llamas, M.-J., Jiménez-Rejano, J.-J., & De-Hita-Cantalejo, C. (2021). Minimum Detectable Change of Visual Acuity Measurements Using ETDRS Charts (Early Treatment Diabetic Retinopathy Study). International Journal of Environmental Research and Public Health, 18(15), 7876. https://doi.org/10.3390/ijerph18157876