
Development and Validation of Nurses’ Well-Being and Caring Nurse–Patient Interaction Model: A Psychometric Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Design and Participants
2.2. Measures and Variables
2.3. Data Analysis
3. Results
3.1. Participant Characteristics and Scale Score
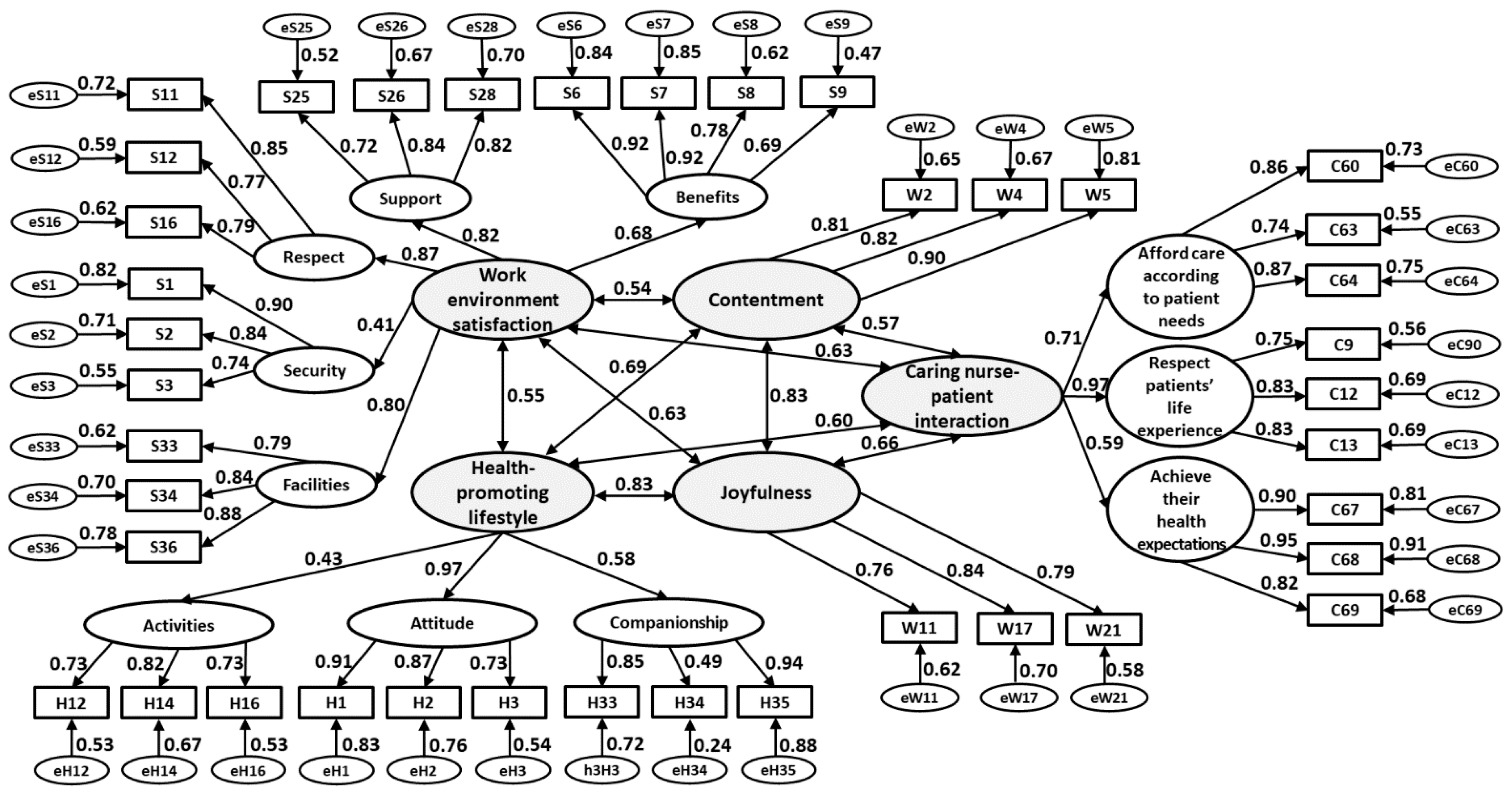
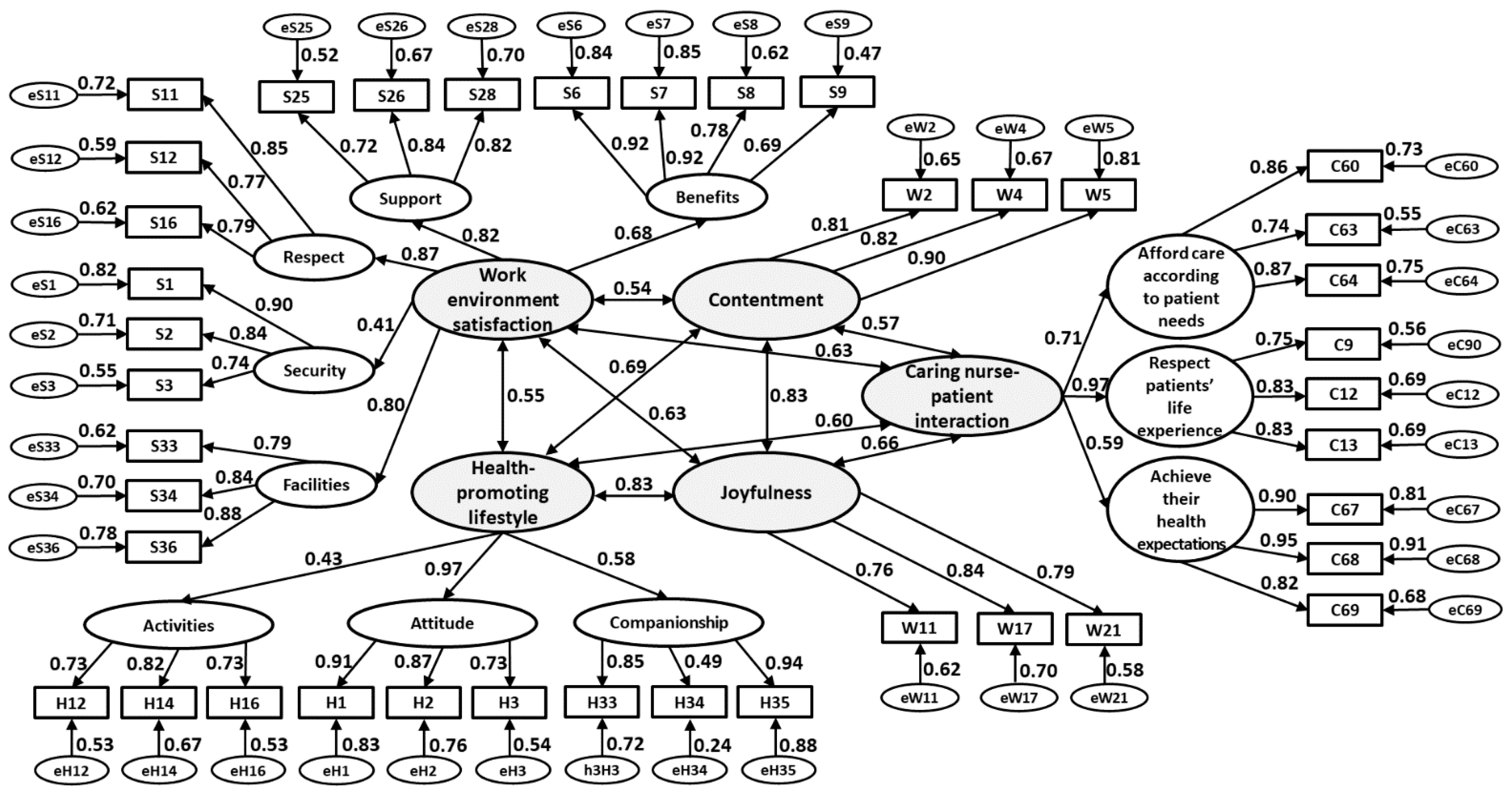
3.2. Findings of SEM Analysis
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Shattell, M. Nurse–patient interaction: A review of the literature. J. Clin. Nurs. 2004, 13, 714–722. [Google Scholar] [CrossRef] [Green Version]
- Finfgeld-Connett, D. Meta-synthesis of caring in nursing. J. Clin. Nurs. 2008, 17, 196–204. [Google Scholar] [CrossRef]
- Watson, J. Caring science and the next decade of holistic healing: Transforming self and system from the inside out. Beginnings 2010, 30, 14–16. [Google Scholar]
- Chung, H.C.; Hsieh, T.C.; Chen, Y.C.; Chang, S.C.; Hsu, W.L. Cross-cultural adaptation and validation of the Chinese Comfort, Afford, Respect, and Expect scale of caring nurse–patient interaction competence. J. Clin. Nurs. 2018, 27, 3287–3297. [Google Scholar] [CrossRef]
- Cossette, S.; Cara, C.; Ricard, N.; Pepin, J. Assessing nurse-patient interactions from a caring perspective: Report of the development and preliminary psychometric testing of the Caring Nurse—Patient Interactions Scale. Int. J. Nurs. Stud. 2005, 42, 673–686. [Google Scholar] [CrossRef]
- Cossette, S.; Cote, J.K.; Pepin, J.; Ricard, N.; D’Aoust, L.X. A dimensional structure of nurse-patient interactions from a caring perspective: Refinement of the Caring Nurse-Patient Interaction Scale (CNPI-Short Scale). J. Adv. Nurs. 2006, 55, 198–214. [Google Scholar] [CrossRef] [PubMed]
- Cossette, S.; Pepin, J.; Cote, J.K.; de Courval, F.P. The multidimensionality of caring: A confirmatory factor analysis of the Caring Nurse-Patient Interaction Short Scale. J. Adv. Nurs. 2008, 61, 699–710. [Google Scholar] [CrossRef]
- Dodge, R.; Daly, A.P.; Huyton, J.; Sanders, L.D. The challenge of defining wellbeing. Int. J. Wellbeing 2012, 2, 222–235. [Google Scholar] [CrossRef] [Green Version]
- Arrogante, O.; Perez-Garcia, A.M. Is subjective well-being perceived by non-health care workers different from that perceived by nurses? Relation with personality and resilience. Enferm. Intensiva 2013, 24, 145–154. [Google Scholar] [CrossRef]
- Lu, L. The relationship between subjective well-being and psychosocial variables in Taiwan. J. Soc. Psychol. 1995, 135, 351–357. [Google Scholar] [CrossRef]
- Luo, L.; Gilmour, R.; Kao, S.F. Cultural values and happiness: An East-West dialogue. J. Soc. Psychol. 2001, 141, 477–493. [Google Scholar] [CrossRef]
- Chung, H.C.; Chen, Y.C.; Chang, S.C.; Hsu, W.L.; Hsieh, T.C. Nurses’ Well-Being, Health-Promoting Lifestyle and Work Environment Satisfaction Correlation: A Psychometric Study for Development of Nursing Health and Job Satisfaction Model and Scale. Int. J. Environ. Res. Public Health 2020, 17, 3582. [Google Scholar] [CrossRef]
- Bentler, P.M.; Chou, C.-P. Practical Issues in Structural Modeling. Sociol. Methods Res. 1987, 16, 78–117. [Google Scholar] [CrossRef]
- Thompson, B. Exploratory and Confirmatory Factor Analysis: Understanding Concepts and Applications, 1st ed.; American Psychological Association: Washington, DC, USA, 2004; pp. 273–275. [Google Scholar]
- Hooper, D.; Coughlan, J.; Mullen, M. Structural equation modelling: Guidelines for determining model fit. Electron. J. Bus. Res. Methods 2008, 6, 53–60. [Google Scholar]
- Hall, L.H.; Johnson, J.; Watt, I.; Tsipa, A.; O’Connor, D.B. Healthcare Staff Wellbeing, Burnout, and Patient Safety: A Systematic Review. PLoS ONE 2016, 11, e0159015. [Google Scholar] [CrossRef]
- Barrué, P.; Sánchez-Gómez, M. The emotional experience of nurses in the Home Hospitalization Unit in palliative care: A qualitative exploratory study. Enferm. Clin. Engl. Ed. 2021, 31, 211–221. [Google Scholar] [CrossRef]
- Walker, S.N.; Sechrist, K.R.; Pender, N.J. The health-promoting lifestyle profile: Development and psychometric characteristics. Nurs. Res. 1987, 36, 76–81. [Google Scholar] [CrossRef]
- Pérez-Francisco, D.H.; Duarte-Clíments, G.; Del Rosario-Melián, J.M.; Gómez-Salgado, J.; Romero-Martín, M.; Sánchez-Gómez, M.B. Influence of Workload on Primary Care Nurses’ Health and Burnout, Patients’ Safety, and Quality of Care: Integrative Review. Healthcare 2020, 8, 12. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Putra, K.R.; Andayani, T.; Ningrum, E.H. Job satisfaction and caring behavior among nurses in a military hospital: A cross-sectional study. J. Public Health Res. 2021, 10, 2212. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Liu, J.; Liu, K.; Baggs, J.G.; Wang, J.; Zheng, J.; Wu, Y.; Li, M.; You, L. Association of changes in nursing work environment, non-professional tasks, and nursing care left undone with nurse job outcomes and quality of care: A panel study. Int. J. Nurs. Stud. 2021, 115, 103860. [Google Scholar] [CrossRef] [PubMed]
- Moisoglou, I.; Yfantis, A.; Galanis, P.; Pispirigou, A.; Chatzimargaritis, E.; Theoxari, A.; Prezerakos, P. Nurses work environment and patients’ quality of care. Int. J. Caring Sci. 2020, 13, 108–116. [Google Scholar]

{kind=link}
{kind=link}
| Variables | Mean ± SD. | N (%) |
|---|---|---|
| Age (years) | 29.0 ± 7.2 | |
| <30 years | 132 (62.3) | |
| >=30 years | 80 (37.7) | |
| Marital status | ||
| Married | 61 (28.8) | |
| Others | 151 (71.2) | |
| Education | ||
| College | 111 (38.2) | |
| Bachelor or above | 185 (61.8) | |
| Tenure (years) | 7.5 ± 7.1 | |
| <=2 years | 58 (28.4) | |
| >2 years | 154 (72.6) | |
| Affiliated unit | ||
| Emergency and critical unit | 71 (33.4) | |
| Others | 141 (66.6) | |
| Clinical ladder | ||
| N | 39 (18.4) | |
| N1 | 42 (19.8) | |
| N2 | 84 (39.6) | |
| N3 | 35 (16.5) | |
| N4 | 12 (5.7) |
| Scale | Cronbach’s α | Mean ± SD. | Med. (Q1, Q3) | Min., Max. |
|---|---|---|---|---|
| CARE scale | 0.91 | 45.0 ± 5.8 | 45.0 (41.0, 48.0) | 28.0, 60.0 |
| NHJS scale | ||||
| Well-being subscale: Contentment | 0.87 | 10.0 ± 2.4 | 10.0 (9.0, 12.0) | 3.0, 15.0 |
| Well-being subscale: Joyfulness | 0.84 | 10.6 ± 2.1 | 11.0 (9.0, 12.0) | 3.0, 15.0 |
| Work environment satisfaction subscale | 0.91 | 53.8 ± 9.2 | 54.0 (48.0, 61.8) | 25.0, 79.0 |
| Health-promoting lifestyle subscale | 0.84 | 27.6 ± 5.9 | 27.0 (24.0, 32.0) | 14.0, 43.0 |
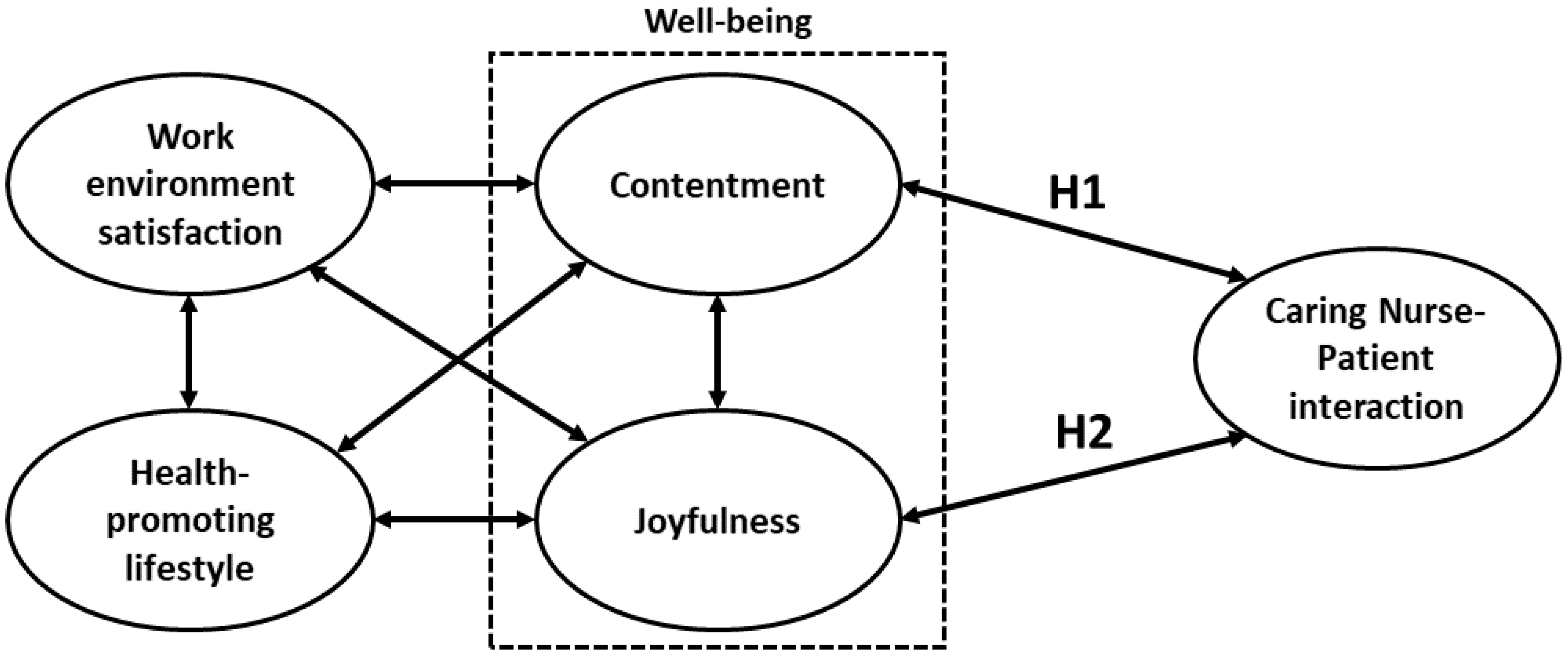
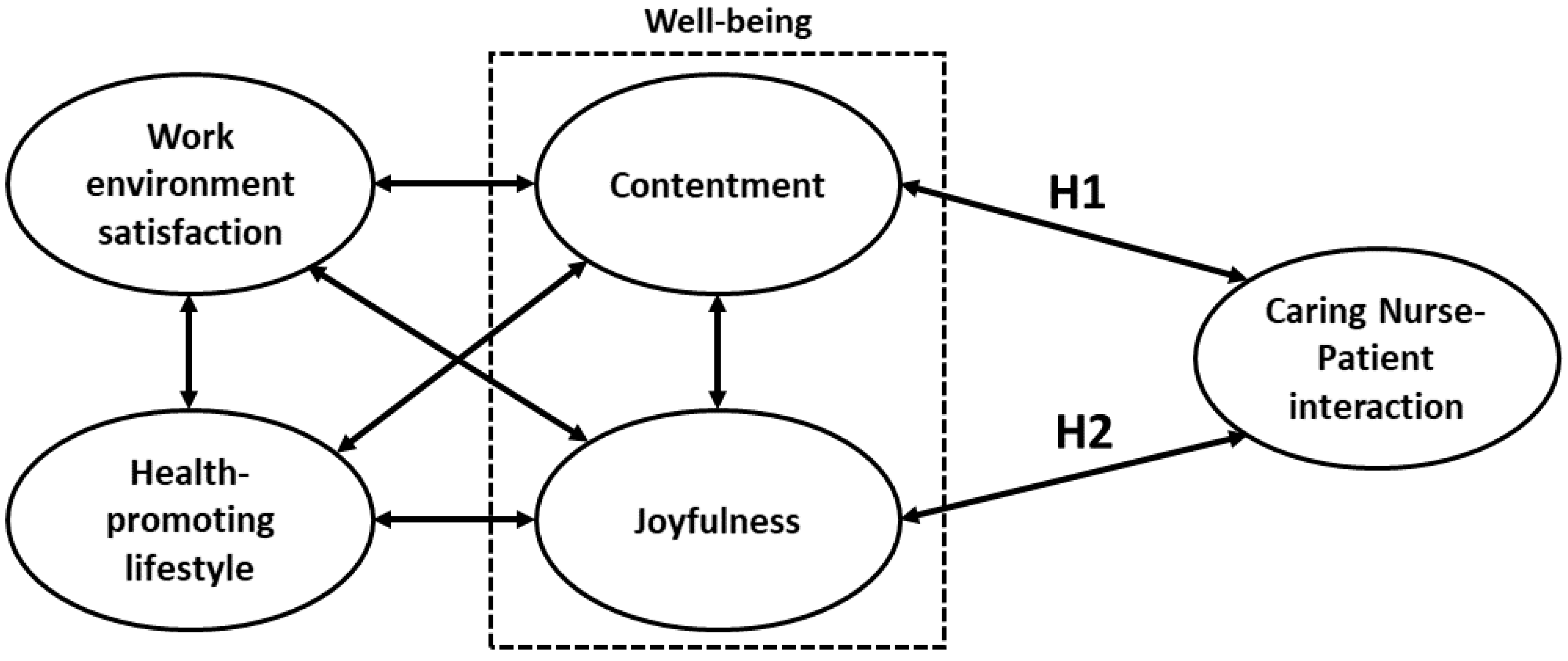
| Hypothesis | PC 1 | Z | p-Value | |
|---|---|---|---|---|
| H1 | Contentment was positively correlated with CNPI competence | 0.57 | 5.30 | p < 0.001 |
| H2 | Joyfulness was positively correlated with CNPI competence | 0.66 | 5.31 | p < 0.001 |
| Subscale of NJHS Scale | Construct | CNPI Competence | |||||
|---|---|---|---|---|---|---|---|
| Afford Care According to Patient Needs | Respect Patients’ Life Experience | Help Patients Achieve Their Health Expectations | |||||
| r | p-Value | r | p-Value | r | p-Value | ||
| Well-being | Contentment | 0.377 | <0.001 | 0.477 | <0.001 | 0.403 | <0.001 |
| Joyfulness | 0.424 | <0.001 | 0.558 | <0.001 | 0.332 | <0.001 | |
| Work environment satisfaction | Benefits | 0.192 | 0.005 | 0.350 | <0.001 | 0.285 | <0.001 |
| Support | 0.342 | <0.001 | 0.472 | <0.001 | 0.290 | <0.001 | |
| Respect | 0.375 | <0.001 | 0.474 | <0.001 | 0.325 | <0.001 | |
| Security | 0.075 | 0.276 | 0.207 | 0.002 | 0.184 | 0.007 | |
| Facilities | 0.324 | <0.001 | 0.396 | <0.001 | 0.265 | <0.001 | |
| Health-promoting lifestyle | Activities | 0.177 | 0.010 | 0.182 | 0.008 | 0.171 | 0.012 |
| Attitude | 0.407 | <0.001 | 0.516 | <0.001 | 0.383 | <0.001 | |
| Companionship | 0.209 | <0.001 | 0.251 | <0.001 | 0.191 | <0.005 | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chung, H.-C.; Chen, Y.-C.; Chang, S.-C.; Hsu, W.-L.; Hsieh, T.-C. Development and Validation of Nurses’ Well-Being and Caring Nurse–Patient Interaction Model: A Psychometric Study. Int. J. Environ. Res. Public Health 2021, 18, 7750. https://doi.org/10.3390/ijerph18157750
Chung H-C, Chen Y-C, Chang S-C, Hsu W-L, Hsieh T-C. Development and Validation of Nurses’ Well-Being and Caring Nurse–Patient Interaction Model: A Psychometric Study. International Journal of Environmental Research and Public Health. 2021; 18(15):7750. https://doi.org/10.3390/ijerph18157750
Chicago/Turabian StyleChung, Hui-Chun, Yueh-Chih Chen, Shu-Chuan Chang, Wen-Lin Hsu, and Tsung-Cheng Hsieh. 2021. "Development and Validation of Nurses’ Well-Being and Caring Nurse–Patient Interaction Model: A Psychometric Study" International Journal of Environmental Research and Public Health 18, no. 15: 7750. https://doi.org/10.3390/ijerph18157750
APA StyleChung, H.-C., Chen, Y.-C., Chang, S.-C., Hsu, W.-L., & Hsieh, T.-C. (2021). Development and Validation of Nurses’ Well-Being and Caring Nurse–Patient Interaction Model: A Psychometric Study. International Journal of Environmental Research and Public Health, 18(15), 7750. https://doi.org/10.3390/ijerph18157750