
An Analysis of COVID-19 Global Guidelines Published in the Early Phase of the Pandemic for People with Disabilities




Abstract
:1. Introduction
2. Methods
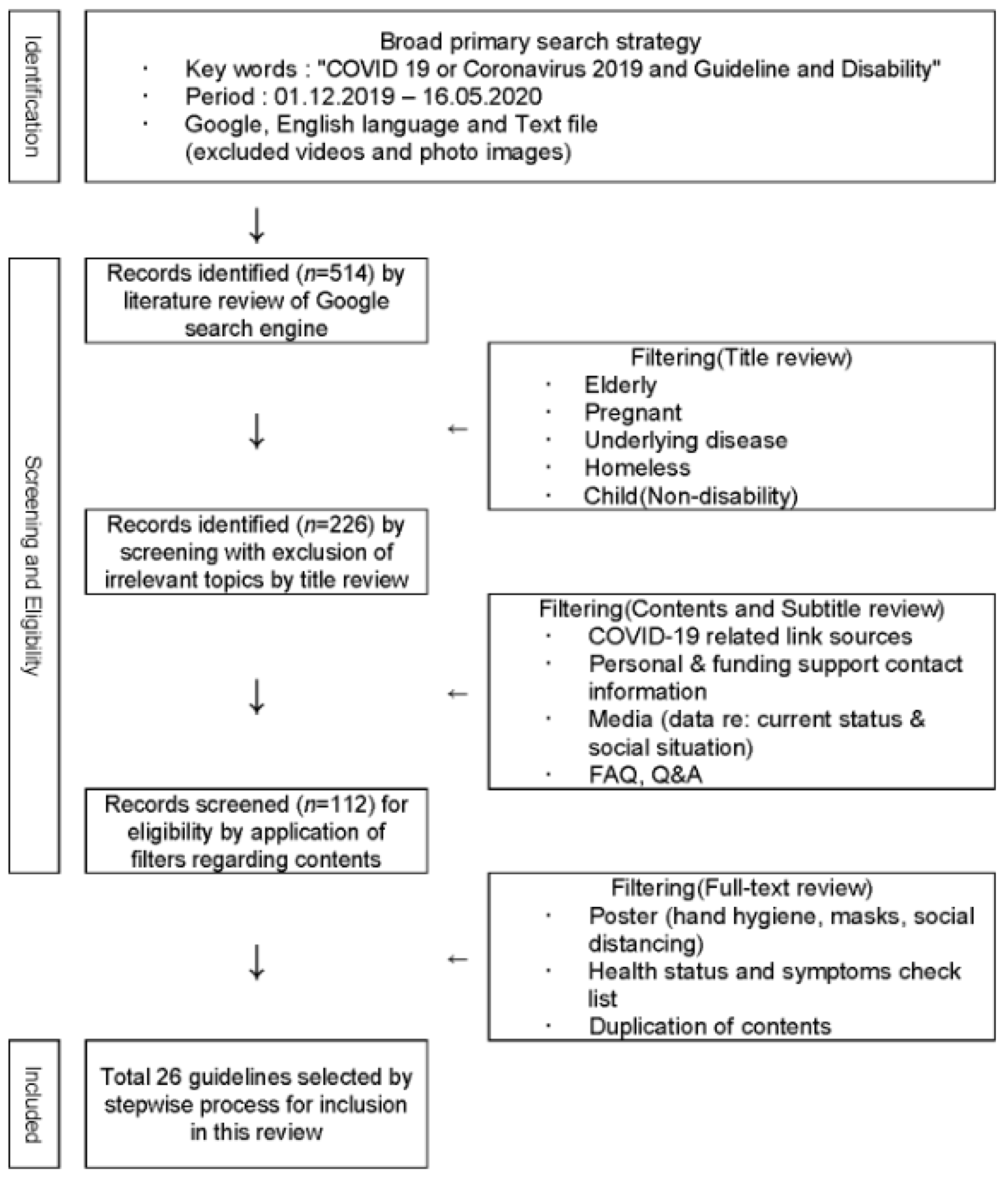
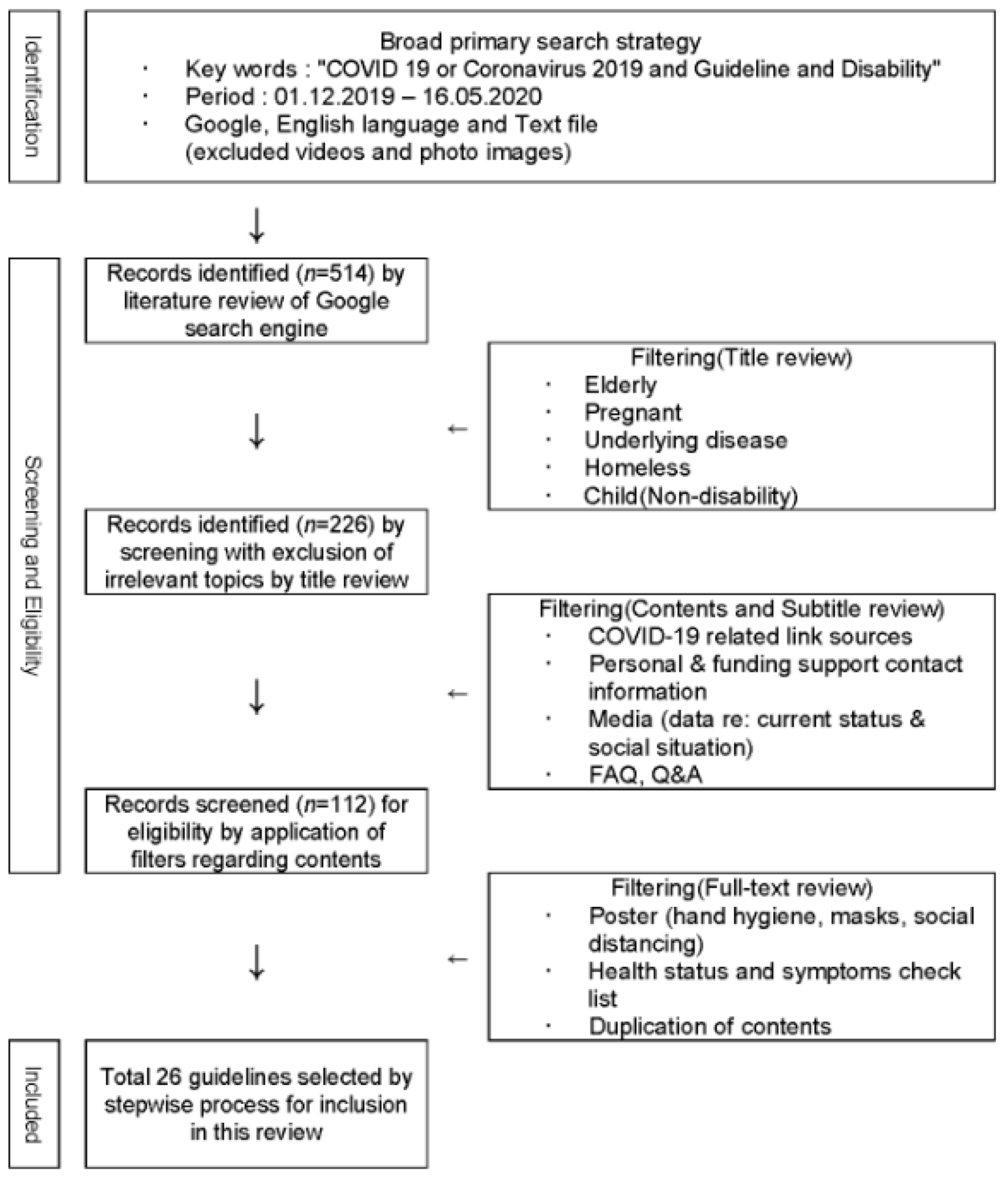
2.1. Search Strategy and Selection Criteria
2.2. Procedure
2.3. Data Extraction
3. Results
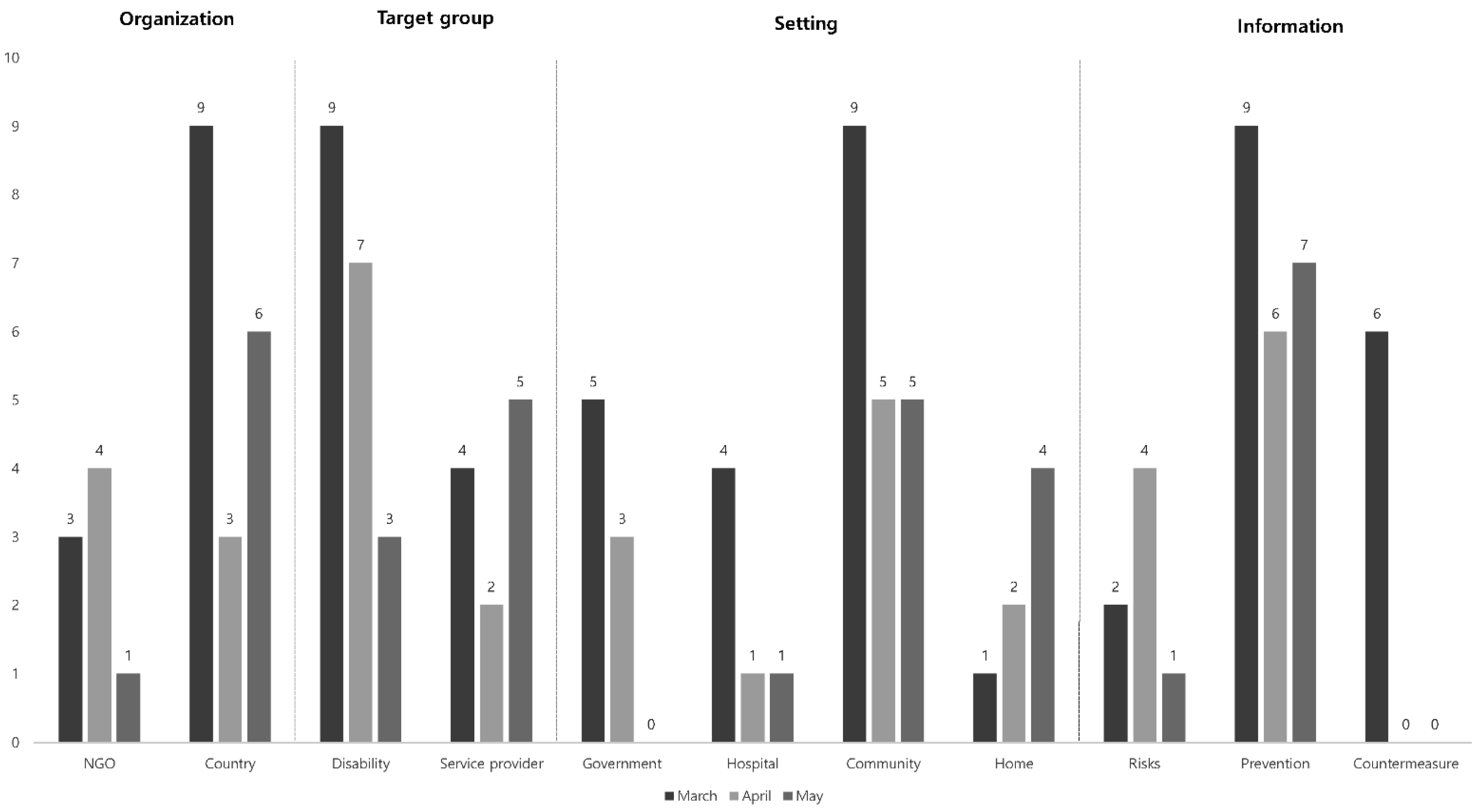
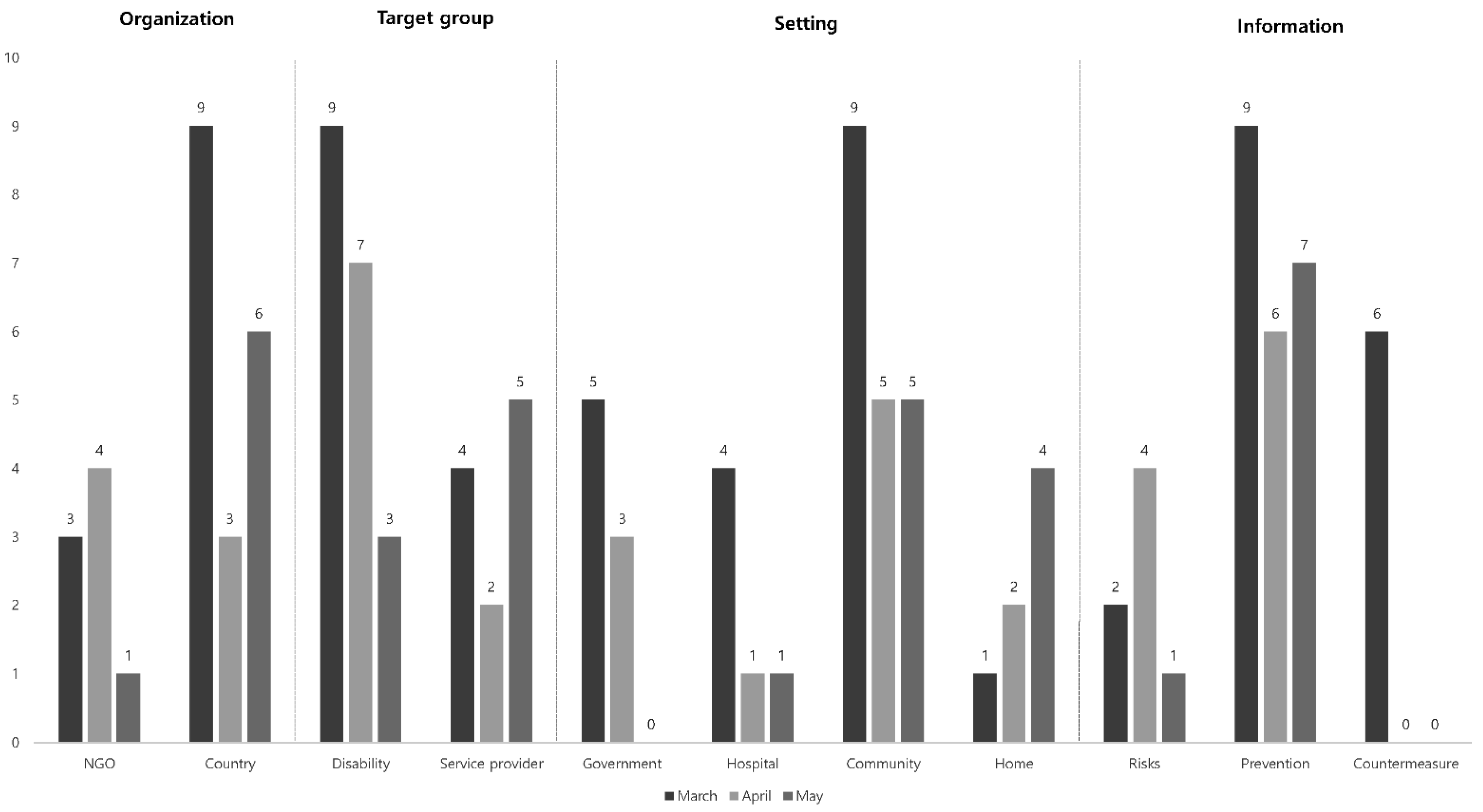
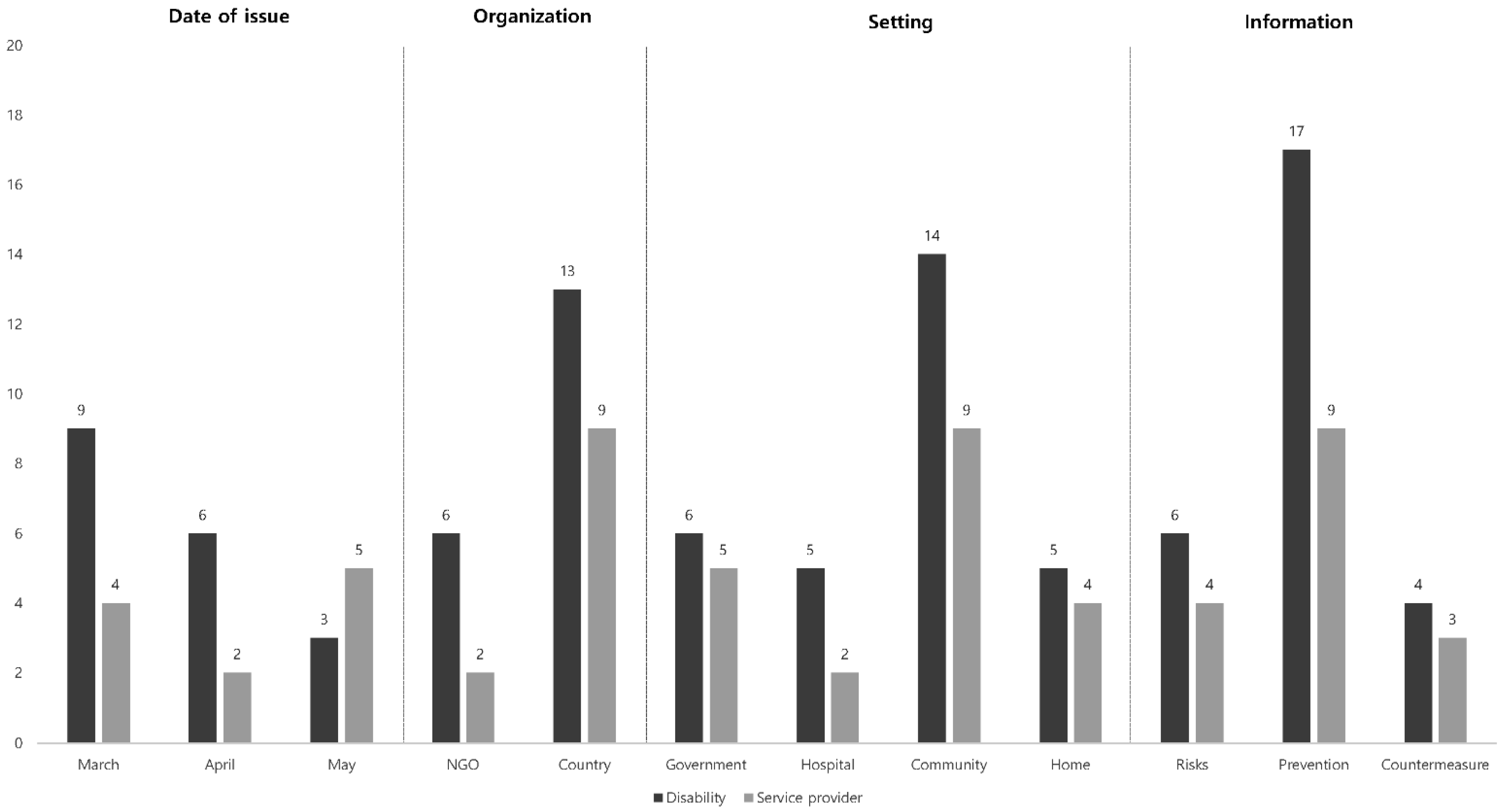
3.1. Classification of Guidelines
3.2. Data Comparison of NGO and Country
3.3. Data Comparison of Target Groups
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- World Health Organization. Geneva; 11 March 2020. Available online: https://www.who.int/emergencies/diseases/novel-coronavirus-2019 (accessed on 1 July 2020).
- CDC COVID-19 Response Team. Preliminary Estimates of the Prevalence of Selected Underlying Health Conditions Among Patients with Coronavirus Disease 2019—United States, February 12–March 28, 2020. Weekly 2020, 69, 382–386. [Google Scholar]
- Lee, D.; Lee, J. Testing on the Move South Korea’s rapid response to the COVID-19 pandemic. Transp. Res. Interdiscip. Perspect. 2020. [Google Scholar] [CrossRef]
- Lee, S.B.; Kim, J.A. Country report: Impact of COVID-19 and inequity of health on South Korea’s disabled community during a pandemic. Disabil. Soc. 2020, 35, 1514–1519. [Google Scholar] [CrossRef]
- Aimone, F. The 1918 influenza epidemic in New York City: A review of the public health response. Public Health Rep. 2010, 125 (Suppl. 3), 71–79. [Google Scholar] [CrossRef] [Green Version]
- Li, L.Q.; Huang, T.; Wang, Y.Q. COVID-19 patients’ clinical characteristics, discharge rate, and fatality rate of meta-analysis. J. Med. Virol. 2020, 92, 577–583. [Google Scholar] [CrossRef]
- Dowd, J.B.; Andriano, L.; Brazel, D. Demographic science aids in understanding the spread and fatality rates of COVID-19. Proc. Natl. Acad. Sci. USA 2020, 117, 9696–9698. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Danny, H. It’s hit our front door: Homes for the disabled see a surge of COVID-19. New York Times. 8 April 2020. Health. Available online: https://www.nytimes.com/2020/04/08/nyregion/coronavirus-disabilities-group-homes.html (accessed on 20 July 2020).
- Kwon, S.H. A people with severe disability in 50s who was discharged from Uijeongbu St. Mary’s Hospital died in a day. Yonhap News Agency. 4 April 2020. Society. Available online: https://www.yna.co.kr/view/AKR20200404061051060 (accessed on 18 July 2020).
- ANMJ Staff. Coronavirus pandemic creating fear for Australian children and young people with a disability. Australian Nursing & Midwifery Journal. 18 March 2020. Wellbeing. Available online: https://anmj.org.au/coronavirus-pandemic-creating-fear-for-australian-children-and-young-people-with-a-dsability/ (accessed on 17 July 2020).
- Turk, M.A.; Landes, S.D.; Formica, M.K.; Goss, K.D. Intellectual and developmental disability and COVID-19 case-fatality trends: TriNetX analysis. Disabil. Health J. 2020, 13, 100942. [Google Scholar] [CrossRef]
- Jordan, R.E.; Adap, P.; Cheng, K.K. Covid-19: Risk factors for severe disease and death. Br. Med. J. 2020. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Turk, M.A.; McDermott, S. The Covid-19 pandemic and people with disability. Disabil. Health J. 2020. [Google Scholar] [CrossRef] [PubMed]
- Thelwall, M.; Levitt, J.M. Retweeting Covid-19 disability issues: Risks, support and outrage. El Prof. Inf. 2020, 29, e290216. [Google Scholar] [CrossRef] [Green Version]
- Lancet, T. Redefining vulnerability in the era of COVID-19. Lancet 2020, 395, 1089. [Google Scholar] [CrossRef]
- Guideline on Hospitalization of COVID-19 Confirmed PWD; Daegu Solidarity Against Disability Discrimination: Daegu, Korea, 2020.
- Guidelines on Providing Access to Public Health Information in National Sign Languages during the Coronavirus Pandemic; World Federation of The Deaf/World Association of Sign Language Interpreters: Helsinki, Finland, 2020.
- Information on Coronavirus (COVID-19) for People with Spinal Cord Injury Living in SA and NT; Government of South Australia: Brisbane, Australia, 2020.
- Toward a Disability-Inclusive COVID19 Response: 10 Recommendations from the International Disability Alliance; International Disability Alliance: Geneva, Switzerland, 2020.
- COVID-19 Hospital Discharge Service Requirements; Department of Health and Social Care: London, UK, 2020.
- COVID-19 Response Plan; Veterans Health Administration Office of Emergency Management: Washington, DC, USA, 2020.
- Questions and Answers: Provision of Services to Students with Disabilities During School Facility Closures for COVID-19; Washington Office of Superintendent of Public Instruction: Washington, DC, USA, 2020.
- Comprehensive Disability Inclusive Guidelines for Protection and Safety of Persons with Disabilities (Divyangjan) during COVID 19; Ministry of Home Affairs: New Delhi, India, 2020.
- Disability Considerations during the COVID-19 Outbreak; World Health Organization: Geneva, Switzerland, 2020.
- Faculty of Psychiatry of Intellectual Disability Covid-19 and People with Intellectual Disability; Faculty of Psychiatry of Intellectual Disability: London, UK, 2020.
- Planning for Disruption to Supports and Services Because of COVID-19 Advice for People with Spinal Cord Injury; Queensland Spinal Cord Injuries Service: Queensland, Australia, 2020.
- COVID-19 in Disability Accommodation; Disability Services Consulting: Melbourne, Australia, 2020.
- Basic Guidance of Management of Spinal Cord Injury Patients during Coronavirus (COVID-19) Pandemic; The British Association of Spinal Cord Injury Specialists: Shropshire, UK, 2020.
- COVID-19 Response: Considerations for Children and Adults with Disabilities; UNICEF: New York, NY, USA, 2020.
- A Disability-Inclusive COVID-19 Response; Global Protection Cluster, Syria Protection Cluster: Ankara, Turkey, 2020.
- Management and Operational Plan for People with Disability: Australian Health Sector Emergency Response Plan for Novel Coronavirus; Australian Government Department of Health: Canberra, Australia, 2020.
- COVID-19 and Intellectual Disability Supporting People with Intellectual Disabilities and Their Families; Inclusion Ireland National Association for People with an Intellectual Disability: Dublin, Ireland, 2020.
- Tip Sheet for Disability Inclusion during COVID-19 Child Protection, Education, Health Nutrition, WASH; Save the Children: London, UK, 2020.
- COVID-19 and the Rights of Persons with Disabilities; Guidance; United Nations: New York, NY, USA, 2020.
- Life in the Times of Covid 19: A Guide for Parents of Children with Disabilities; UNESCO New Delhi Cluster Office: Delhi, India, 2020.
- COVID-19 Guidance for Individuals and Families of Individuals with Intellectual and Developmental Disabilities; NJ Department of Human Services Division of Developmental Disabilities: Trenton, NJ, USA, 2020.
- Mental Health Resources for Disability Support Service Providers; Ministry of Health: Wellington, New Zealand, 2020.
- Alert Level 2 Guidance for Disability Support Service Providers; Ministry of Health: Wellington, New Zealand, 2020.
- Clinical Guidance for Responding to Patients with an Intellectual (Learning) Disability during COVID-19 in Aotearoa New Zealand; Ministry of Health: Wellington, New Zealand, 2020.
- Attention: Wheelchair and Assistive Technology Users Precautions for COVID-19; Beneficial Designs Inc.: Minden, NV, USA, 2020.
- Guidelines for Personal Protective Equipment (PPE) Disability Support Care Workers Who Work in Clients Homes; Ministry of Health: Wellington, New Zealand, 2020.
- Korupolu, R.; Stampas, A.; Gibbons, C. COVID-19: Screening and triage challenges in people with disability due to Spinal Cord Injury. Spinal Cord Ser. Case 2020, 6, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Courtenay, K. Covid-19: Challenges for people with intellectual disability. Br. Med. J. 2020, 369. [Google Scholar] [CrossRef] [PubMed]
- Pineda, V.S.; Corburn, J. Disability, Urban Health Equity, and the Coronavirus Pandemic: Promoting Cities for All. J. Urban Health 2020, 97, 336–341. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Courtenay, K.; Perera, B. COVID-19 and people with intellectual disability: Impacts of a Pandemic. Ir. J. Psychol. Med. 2020, 37, 231–236. [Google Scholar] [CrossRef]
- Wolf, M.S.; Serper, M.; Opsasnick, L. Awareness, attitudes, and actions related to COVID-19 among adults with chronic conditions at the onset of the US outbreak: A cross-sectional survey. Ann. Intern. Med. 2020, 173, 100–109. [Google Scholar] [CrossRef] [Green Version]
- Kuper, H.; Banks, L.; Bright, T. Disability-inclusive COVID-19 response: What it is, why it is important and what we can learn from the United Kingdom’s response. Welcome Open Res. 2020, 5. [Google Scholar] [CrossRef]
- UN Economic and Social Commission for Asia and the Pacific (ESCAP). Ensuring Disability Rights and Inclusion in the Response to COVID-19; UNESCAP: Bankok, Thailand, 2020. [Google Scholar]
- Sendai Statement to Promote Disability-Inclusive Disaster Risk Reduction for Resilient, Inclusive and Equitable Societies in ASIA and the Pacific; Nippon Foundation (JPN), Rehabilitation International, the United Nations Economic and Social Commission for Asia and the Pacific: Sendai, Japan, 2014.
- Liasidou, A.; Mavrou, K. Disability rights in Higher Education Programs: The case of medical schools and other health-related disciplines. Soc. Sci. Med. 2017, 191, 143–150. [Google Scholar] [CrossRef] [PubMed]
- NHS. Responding to COVID-19: Mental Health, Learning Disabilities and Autism; National Health Service: London, UK, 2020. [Google Scholar]
- Pulrang, A. Five things to know about coronavirus and people with disabilities. Forbes. 8 March 2020. Lifestyle. Available online: https://www.forbes.com/sites/andrewpulrang/2020/03/08/5-things-to-know-about-coronavirus-and-people-withdisabilities/#44657db31d21 (accessed on 2 July 2020).
- Lakhani, A. Which Melbourne metropolitan areas are vulnerable to COVID-19 based on age, disability and access to health services? Using spatial analysis to identify service gaps and inform delivery. J. Pain Sympt. Manag. 2020, 60, e41–e44. [Google Scholar] [CrossRef] [PubMed]
- Downar, J.; Seccareccia, D. Palliating a Pandemic: “All patients must be cared for”. J. Pain Sympt. Manag. 2010, 39, 291–295. [Google Scholar] [CrossRef]
- Kaiser, C.; Brossard, L. Recommendations for Health Protection of People with Disabilities during Outbreaks: Lessons Learned from the 2019 Novel Coronavirus, 2020. ONG Inclusiva. Available online: https://onginclusiva.org/wp-content/uploads/2021/03/RECOMMENDATIONS-FOR-HEALTH-PROTECTION-OF-PEOPLE-WITH-DISABILITIES-DURING-OUTBREAKS.pdf (accessed on 3 July 2020).
- Bareham, L. Royal Association for Deaf People. Available online: http://royaldeaf.org.uk/covid-19-coronavirus-update-from-rad-ceos/ (accessed on 3 July 2020).
- Alzhehimer’s association, Chicago (IL). Available online: http://www.alz.org/help-support/caregiving/coronavirus-(covid-19)-tips-for-dementia-care (accessed on 30 June 2020).
- Devandas, C. UN Human Rights. Geneva, Switzerland, 17 March 2020. Available online: https://www.ohchr.org/EN/NewsEvents/Pages/DisplayNews.aspx?NewsID=25725&LangID=E.%20Accessed%2023%20March%202020 (accessed on 30 June 2020).
- Rajgor, D.D.; Lee, M.H.; Archuleta, S. The many estimates of the COVID-19 case fatality rate. Lancet Infect. Dis. 2020, 20, 776–777. [Google Scholar] [CrossRef] [Green Version]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Date of Issue | Organization | Title | Target Group | Setting (Environment) | Information Type Provided | |||||
|---|---|---|---|---|---|---|---|---|---|---|
| Government | Hospital | Community | Home (Family) | Risks | Prevention | Countermeasure | ||||
| 13 March 2020 | Daegu Solidarity Against Disability Discrimination (Republic of Korea) [16] | Guideline on hospitalization of COVID-19 confirmed PWD | All people with disabilities | √ | √ | |||||
| 18 March 2020 | World Federation of The Deaf/World Association of Sign Language Interpreters (NGO) [17] | Guidelines on Providing Access to Public Health Information in National Sign Languages during the Coronavirus Pandemic | Sign language interpreters or translators | √ | √ | |||||
| 18 March 2020 | Government of South Australia (Australia) [18] | Information on coronavirus (COVID-19) for people with spinal cord injury in SA and NT | People with spinal cord injury | √ | √ | √ | ||||
| 19 March 2020 | International Disability Alliance (NGO) [19] | Toward a Disability-Inclusive COVID-19 Response: 10 recommendations from the International Disability Alliance | All people with disabilities | √ | √ | √ | ||||
| 19 March 2020 | Department of Health and Social Care (UK) [20] | COVID-19 Hospital Discharge Service Requirements | Community health services and social staff | √ | √ | √ | √ | |||
| 23 March 2020 | Veterans Health Administration—Office of Emergency Management (USA) [21] | COVID-19 Response Plan | Veterans and staff personnel | √ | √ | √ | √ | √ | √ | |
| 24 March 2020 | Washington Office of Superintendent of Public Instruction (USA) [22] | Questions and Answers: Provision of Services to Students with Disabilities During School Facility Closures for COVID-19 | Students with disabilities | √ | √ | |||||
| 25 March 2020 | Ministry of Home Affairs (India) [23] | Comprehensive disability inclusive guidelines for protection and safety of persons with disabilities (Divyangjan) during COVID 19 | All people with disabilities | √ | √ | √ | ||||
| 26 March 2020 | World Health Organization (NGO) [24] | Disability considerations during the COVID-19 outbreak | All people with disabilities | √ | √ | √ | √ | |||
| 27 March 2020 | Faculty of Psychiatry of Intellectual Disability (UK) [25] | Faculty of Psychiatry of Intellectual Disability COVID-19 and People with Intellectual Disability | People with intellectual disabilities | √ | √ | √ | ||||
| 30 March 2020 | Queensland Spinal Cord Injuries Service (Australia) [26] | Planning for disruption to supports and services because of COVID-19 advice for people with spinal cord injury | People with spinal cord injury | √ | √ | |||||
| 31 March 2020 | Disability Services Consulting (Australia) [27] | COVID-19 in Disability Accommodation | Supported independent living providers | √ | √ | |||||
| 03 April 2020 | The British Association of Spinal Cord Injury Specialists (UK) [28] | Basics guidance of management of spinal cord injury patients during coronavirus (COVID-19) pandemic | People with spinal cord injury | √ | √ | |||||
| 08 April 2020 | UNICEF (NGO) [29] | COVID-19 response: Considerations for Children and Adults with Disabilities | Children and adults with disabilities | √ | √ | |||||
| 09 April 2020 | Global Protection Cluster: Syria Protection Cluster (Turkey) (NGO) [30] | A disability-inclusive COVID-19 response | All people with disabilities | √ | √ | √ | ||||
| 09 April 2020 | Australian Government: Department of Health (Australia) [31] | Management and operational plan for people with disability: Australian Health Sector Emergency Response Plan for Novel Coronavirus | All people with disabilities, families, caregivers, support workers, disability and healthcare sectors | √ | √ | √ | √ | √ | ||
| 15 April 2020 | Inclusion Ireland National Association for People with an Intellectual Disability (Ireland) [32] | COVID-19 and Intellectual Disability: Supporting people with intellectual disabilities and their families | People with intellectual disabilities and their families | √ | √ | √ | √ | |||
| 28 April 2020 | Save the Children (NGO) [33] | Tip Sheet for Disability Inclusion during COVID-19 child protection, education, health, nutrition, WASH | Children with disabilities | √ | √ | √ | ||||
| 29 April 2020 | United Nations (NGO) [34] | COVID-19 and the rights of persons with disabilities: Guidance | All people with disabilities | √ | √ | |||||
| 05 May 2020 | UNESCO New Delhi Cluster Office (NGO) [35] | Life in the Times of COVID-19: A guide for parents of children with disabilities | Parents of children with disabilities | √ | √ | |||||
| 05 May 2020 | NJ Department of HumanServices Division of Developmental Disabilities (USA) [36] | COVID-19 Guidance for Individuals and Families of Individuals with Intellectual and Developmental Disabilities | People with intellectual disabilities and their families | √ | √ | √ | ||||
| 11 May 2020 | Ministry of Health (New Zealand) [37] | Mental health resources for disability support service providers | Disability support service providers | √ | √ | |||||
| 12 May 2020 | Ministry of Health (New Zealand) [38] | Alert Level 2 guidance for disability support service providers | Disability support service provider | √ | √ | √ | ||||
| 12 May 2020 | Ministry of Health (New Zealand) [39] | Clinical guidance for responding to patients with an intellectual (learning) disability during COVID-19 in Aotearoa, New Zealand | People with intellectual disabilities | √ | √ | |||||
| 12 May 2020 | Beneficial Designs Inc. Minden, NV (USA) [40] | Attention: Wheelchair and Assistive Technology Users Precautions for COVID-19 | Wheelchair and assistive technology users | √ | √ | √ | ||||
| 15 May 2020 | Ministry of Health (New Zealand) [41] | Guidelines for personal protective equipment (PPE) disability support care workers who work in clients’ homes | Support and care workers providing support in clients’ homes | √ | √ | √ | ||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, J.-h.; Lee, S.; Lee, Y.-h.; Kim, J. An Analysis of COVID-19 Global Guidelines Published in the Early Phase of the Pandemic for People with Disabilities. Int. J. Environ. Res. Public Health 2021, 18, 7710. https://doi.org/10.3390/ijerph18147710
Kim J-h, Lee S, Lee Y-h, Kim J. An Analysis of COVID-19 Global Guidelines Published in the Early Phase of the Pandemic for People with Disabilities. International Journal of Environmental Research and Public Health. 2021; 18(14):7710. https://doi.org/10.3390/ijerph18147710
Chicago/Turabian StyleKim, Jeong-hyun, Seungbok Lee, Yun-hwan Lee, and Jongbae Kim. 2021. "An Analysis of COVID-19 Global Guidelines Published in the Early Phase of the Pandemic for People with Disabilities" International Journal of Environmental Research and Public Health 18, no. 14: 7710. https://doi.org/10.3390/ijerph18147710
APA StyleKim, J.-h., Lee, S., Lee, Y.-h., & Kim, J. (2021). An Analysis of COVID-19 Global Guidelines Published in the Early Phase of the Pandemic for People with Disabilities. International Journal of Environmental Research and Public Health, 18(14), 7710. https://doi.org/10.3390/ijerph18147710