1. Introduction
The COVID-19 pandemic severely disrupted higher education, displacing millions of students and personnel from the thousands of institutions of higher learning globally. In the fall of 2020, of 905 international universities outside the United States, only 7% offered classes primarily in-person, which is defined as classes conducted in person with some exceptions for online delivery. Of 1442 institutions of higher education in the United States during this same timeframe, only 3% offered fully in-person instruction. For the 97% of institutions that did not resume normal operations, 28% offered classes primarily in person, while another 22% offered instruction in a hybrid model, which is classified as some weeks/days online and some weeks/days in person. Another 31% taught primarily or fully online [
1].
For institutions that remained open to students, campus activities such as athletics presented significant challenges. Athletes make up a significant portion of the campus population of the 1098 institutions that have membership with one of the three divisions of the NCAA. More specifically, 1 in 23 students (4%) are athletes for NCAA Division 1 affiliates, 1 in 10 (10%) for Division 2, and 1 in 6 (17%) for Division 3 [
2]. In total, this accounts for hundreds of thousands of student-athletes across the United States. Given these numbers, the threat of COVID-19 outbreaks within this population is a possibility. In support of this, one such report demonstrated that repeat social gatherings with limited preventative measures (mask use and social distancing), led to 17 confirmed cases of COVID-19 within a university soccer team [
3].
Additional outbreaks of COVID-19 within a university environment have been characterized. In August of 2020, a university in North Carolina recorded 670 new cases of COVID-19 within 22 days of reopening [
4], resulting in the university transitioning all classes to online format. Similarly, an outbreak on a university campus in Indiana resulted in 371 new cases between 16–22 August 2020 [
5]. This prompted the university to transition classes online on 19 August 2020 before returning to in-person instruction on 2 September 2020. Additionally, Duke University identified 84 new cases from 2 August 2020–11 October 2020, which did not require a transition to online classes [
6]. While these studies present responses to individual outbreaks, a comprehensive analysis of COVID-19 management strategies spanning an entire academic year has not been reported. Such evidence-based guidance is needed as easing public restrictions and increased vaccine availability are leading universities to consider resuming fully in-person operations. This is especially true since SARS-CoV-2 variants among other emerging pathogens could leave institutions vulnerable to outbreaks.
In response to the pandemic, Gannon University implemented significant operational changes during the 2020–2021 academic year to maintain a level of on campus presence for students and staff. Gannon is a small, private university with 4755 students and personnel on its campus in Erie, Pennsylvania. There are 3208 students enrolled in undergraduate programs, including 705 student-athletes and associated staff. Gannon offers an array of athletic programs, including those that are classified by NCAA guidelines as high, intermediate, and low risk for the transmission of COVID-19 [
7].
One of the safety measures Gannon required on campus included gathering limitations to reflect local COVID-19 guidelines, along with mask requirements at all times, unless eating. To allow for social distancing in the classroom, technology upgrades for in-person classes were installed to allow for simultaneous remote and in-person lecture delivery when necessary. Temperature check stations were utilized before entering high traffic buildings, and room sanitation was conducted before the start of each class. Gannon also made use of a mobile app that required students and personnel to complete a daily symptom survey. If an individual reported COVID-19 symptoms, they would be flagged and contacted by university health staff to schedule a COVID-19 test.
A unique feature of Gannon’s COVID-19 response included an in-house real-time RT-PCR based surveillance program, which allowed for regular daily testing and delivered results within 8–12 h from the time samples were taken. The results obtained from the 23,227 samples analyzed throughout the academic year made it possible for rapid contact tracing, isolation, and quarantine responses, also facilitated by Gannon employees. These practices made it possible for Gannon to offer 903 of its 1221 classes (75%) fully in-person in the 2020 fall semester. Of the remaining 25% of classes, 249 (20%) utilized a hybrid model, and only 69 classes (5%) were taught remotely. In addition, Gannon was able to facilitate activity and competition for all athletic teams in accordance with NCAA guidance for the entire academic year.
Despite stringent mitigation strategies, Gannon University was not without outbreaks of COVID-19 on its campus environment, many of which were attributed to the student-athlete population. However, with rapid response and continued surveillance, Gannon was able to maintain classroom instruction as designed, without interruption for both the 2020 fall and 2021 spring semesters. Additionally, all sports were able to complete a modified season for the duration of the academic year. The results of our year-long COVID-19 surveillance program provide insights that may prove useful to the thousands of institutions seeking to resume a more traditional presence, while limiting the spread of COVID-19 and other infectious diseases on their campus environment.
4. Discussion
To meet the need of high-throughput COVID-19 testing at Gannon’s campus, we developed a modified, but novel in-house surveillance strategy which allowed for rapid and regular COVID-19 screening of students and personnel for the entire academic year. By comparing the results of our findings with an independent CLIA certified reference lab (
Table 1), we show that our approach is effective in identifying cases of COVID-19 in our campus environment. More specifically, samples that were designated as positive were in alignment with the reference laboratory 98.7% of the time. Samples that did not have a signal by real-time RT-PCR and were designated as negative, were in alignment with the reference laboratory 100% of the time. It is noteworthy that in some cases a signal was detected by real-time RT-PCR but was below our reliable limit of detection, which we classified as negative. There were three instances of results of this nature that were designated as positive by follow-up testing in a reference laboratory, indicating a discrepancy between the two labs. This suggests that some positive specimens may not have viral loads which can be reliably distinguished by this limit of detection. Additionally, the timing of testing can influence the detectable signal produced by presence of SARS-CoV-2 in an individual, with a mean incubation period of 4–5 days post-exposure [
11]. This implies that tests administered to infected individuals before this period may not have sufficient viral load to produce detectable signal. Lowering the minimum threshold of detection is a strategy that can increase the likelihood of identifying samples with low SARS-CoV-2 viral load but risks an increased number of false positive results. Regardless, our results were remarkably consistent with those of a CLIA certified reference lab and allowed for a rapid and aggressive public health response to outbreaks of COVID-19 on campus. Hence, while we were unable to identify all COVID-19 cases within our campus environment, our strategy was effective in mitigating COVID-19 spread in a way that allowed Gannon to resume in-person instruction and activities for the entire academic year.
The low number of COVID-19 cases at Gannon suggests that the strategy of preventative measures (e.g., masks, social distancing, and frequent sanitation) in combination with regular testing [
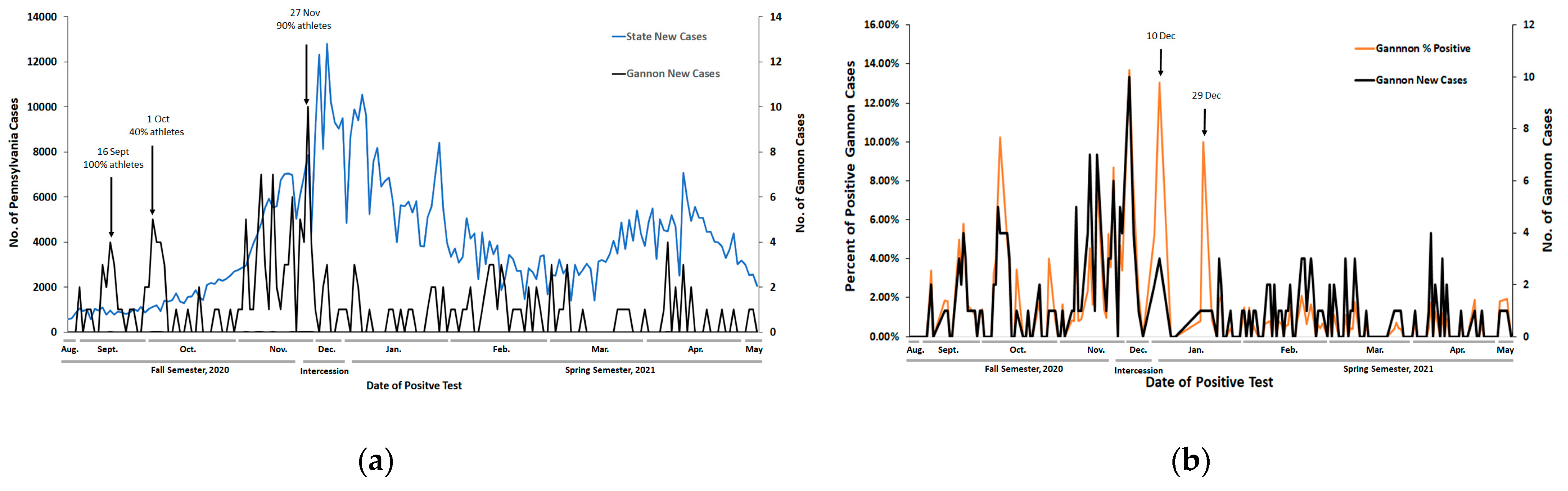
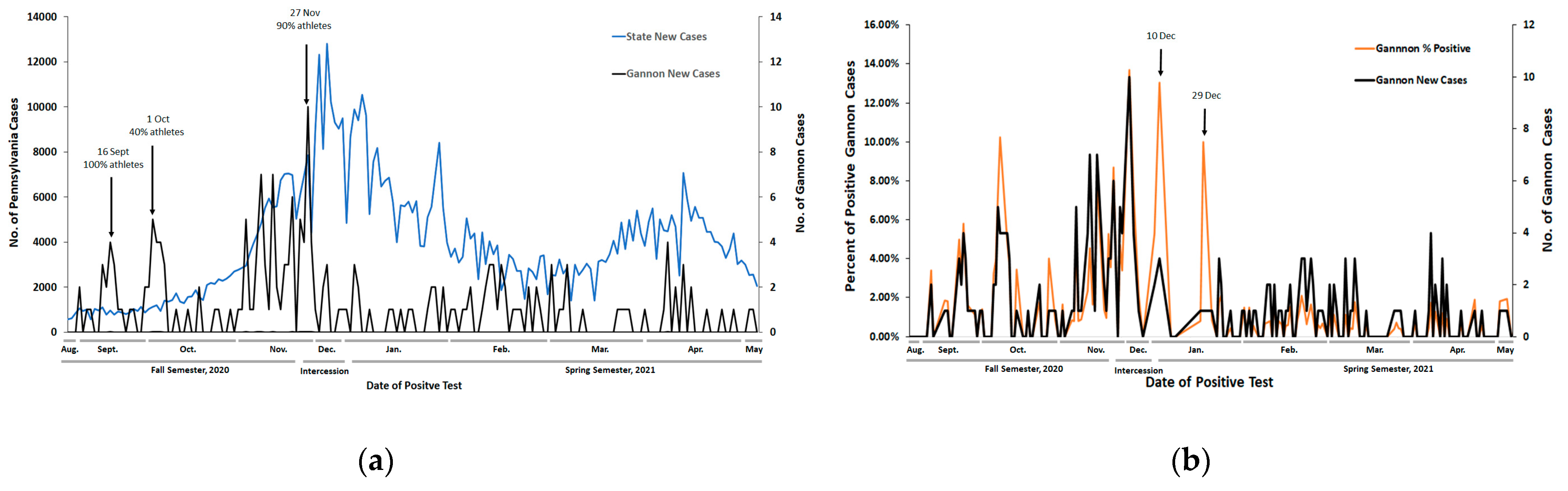
12] has contributed to Gannon’s ability to maintain in-person operations. It is noteworthy that there is a distinct temporal pattern of new COVID-19 cases on Gannon’s Erie campus compared with statewide data (
Figure 1a). For most days, the trend of percent of samples positive for COVID-19 closely reflected the new case count, indicating that spikes in cases were not driven by changes in the volume of testing (
Figure 1b). The few exceptions were on days where total volume of testing was low.
These results demonstrate low, but persistent presence of COVID-19 infection on Gannon’s campus that is distinctive of statewide trends, which has two important implications. First, despite adoption of national and state guidance for mitigating spread of COVID-19 on campus, along with enhancing measures that included rapid surveillance testing, Gannon was only able to limit but not eliminate the occurrence of outbreaks of COVID-19 on its campus. This suggests that state guidance and enhanced protocols are necessary but not sufficient in mitigating the spread of COVID-19 in a university campus environment. Second, our data provides evidence that the unique trends we observe at Gannon compared with statewide data are not largely due to difference in daily testing volume, but instead arise from unique features of the campus community which cannot be easily predicted from statewide trends.
One of the distinguishing populations responsible for outbreaks of COVID-19 on our campus are student-athletes (
Figure 1,
Table 1,
Figure 2). For days where athlete status was known, 45.9% of all COVID-19 cases on Gannon’s campus were student-athletes (
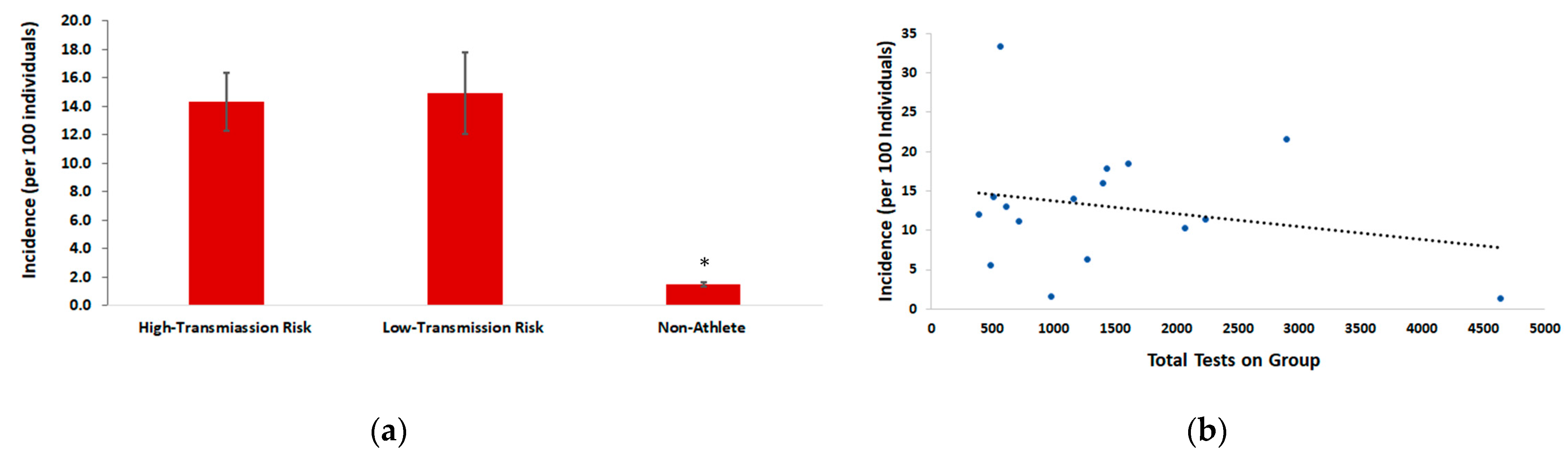
Table 2). An important note is that athletes across risk designations experienced a comparable percent of samples positive for COVID-19. Athletic teams designated as high-risk for transmission of COVID-19 had an average incidence of 14.3, which is remarkably similar to the average incidence of low/intermediate risk athletic teams of 14.9. This indicates that student-athletes as a population, regardless of the risk designation for individual sports are prone to contracting COVID-19, and should be surveilled in increased, and comparable volumes across all sports. This demonstrates that risk classifications for sports is not a relevant indicator for transmission risk of COVID-19. A plausible explanation for this finding is that strict preventative measures (masking, temperature checks, frequent sanitation, and symptom reporting, etc.) are in place during practices and competition for all sports at Gannon, which may decrease the risk of transmission irrespective of risk factors. Regardless, given the high incidence of COVID-19 found in athlete groups within our population, studies that further explore events and/or behaviors associated with the transmission of COVID-19 are warranted.
The percent of samples from student-athletes that tested positive for COVID-19 was relatively low, indicating that testing volume was efficient in identifying cases within this group. Despite this, we noted disproportionately high COVID-19 incidence within this population compared with non-athletes (
Figure 2). The risk ratio associated with these incidences demonstrates that student-athletes on Gannon’s campus were nearly 5 times more likely to contract COVID-19 compared with non-athletes. While the exact reason for higher incidence of COVID-19 in student-athletes is unknown, the information gathered from contact tracing suggests repeated group gatherings, that are non-compliant with safety protocols, rather than sport related activities are likely reasons. A possible explanation is that athletes in university environments typically coexist in larger social groups than other campus populations and frequently interact with other team members, and across athletic teams. Frequent and sustained social interactions present a large risk for the spread of contagion [
13], which is evidence to suggest that athletes as a university population are at high risk for contracting COVID-19. In support of this, an outbreak of COVID-19 on a university men’s and women’s soccer team demonstrated by whole-genome sequencing that 17 new cases across both teams, likely emanated from a single introduction of SARS-CoV-2 during multiple social gatherings between teams, where preventative measures were not taken [
3].
An alternative explanation for the higher incidence of COVID-19 infection in athletes is sampling bias, given that student-athletes were tested with greater frequency than non-athletes. However, three pieces of evidence suggest that this is not the case. First, we found no correlation between the number of tests performed on a group and the incidence of infection. Second, the frequency in which a particular athlete group was tested showed no statistical relationship between COVID-19 incidence rates. Lastly, of the non-athlete groups that were tested repeatedly (five times or greater) during the study period, there was not a single case of COVID-19 identified on days these groups were selected for surveillance testing.
Together, this information provides strong evidence that sampling frequency is not a major contributing factor to the high incidence of COVID-19 observed in athletes compared with the general student population. These data were an important factor in the decision to allocate our focus and resources on efforts that increase rapid surveillance testing of student-athletes, allowing us to make critical public health decisions with limited resources. However, we cannot entirely exclude the possibility that increasing the sampling frequency of other non-athlete populations could reveal a high COVID-19 incidence in our other campus environments, which has been documented at other institutions [
4,
5,
6]. Thus, if resources allow, more frequent surveillance of all campus populations would be the optimal approach for fully understanding COVID-19 transmission patterns in all campus environments.
COVID-19 outbreaks are characteristic of university populations, as reported at other institutions across the United States [
3,
4,
5,
6]. This article is unique in that it follows patterns of COVID-19 infection over an entire academic year. The importance of identifying effective mitigation strategies on university campuses to reduce transmission to individuals at greatest risk of severe complications has been demonstrated [
6,
14]. Successful COVID-19 responses to outbreaks in campus environments have utilized strategies which identified symptomatic individuals by routine symptom monitoring, in combination with random surveillance testing of the general population, and routine testing of select populations [
5,
6]. Our results provide insights into factors that may be responsible for the distinctive outbreak patterns characteristic of campus environments. Student-athletes have been demonstrated to be at increased risk for contracting COVID-19 in this setting.
A limitation of this study is that the trends observed at Gannon’s Erie campus may not be generalizable to other institutions. This might especially become true given that COVID-19 vaccinations are becoming more readily available. However, the emergence of new SARS-CoV-2 variants and other outbreaks of infectious disease on college campuses remains threatening. Given the millions of students attending college globally, many of which are intending to resume athletic participation, the recommendation to monitor the spread of COVID-19, particularly within the student-athlete population, should be strongly considered. Additional studies are needed to further establish the specific role student-athletes have in facilitating the spread of COVID-19 within a campus environment.





{kind=link}
{kind=link}