
The Impact of Nordic Walking on Bone Properties in Postmenopausal Women with Pre-Diabetes and Non-Alcohol Fatty Liver Disease

 and
and
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Exercise Intervention
2.3. Background Information
2.4. Anthropometric and Bone Measurements
2.5. Clinical and Laboratory Measurements
2.6. Data Analysis
3. Results
3.1. Baseline Participant Characteristics
3.2. Change in BMC and BMD after the Intervention
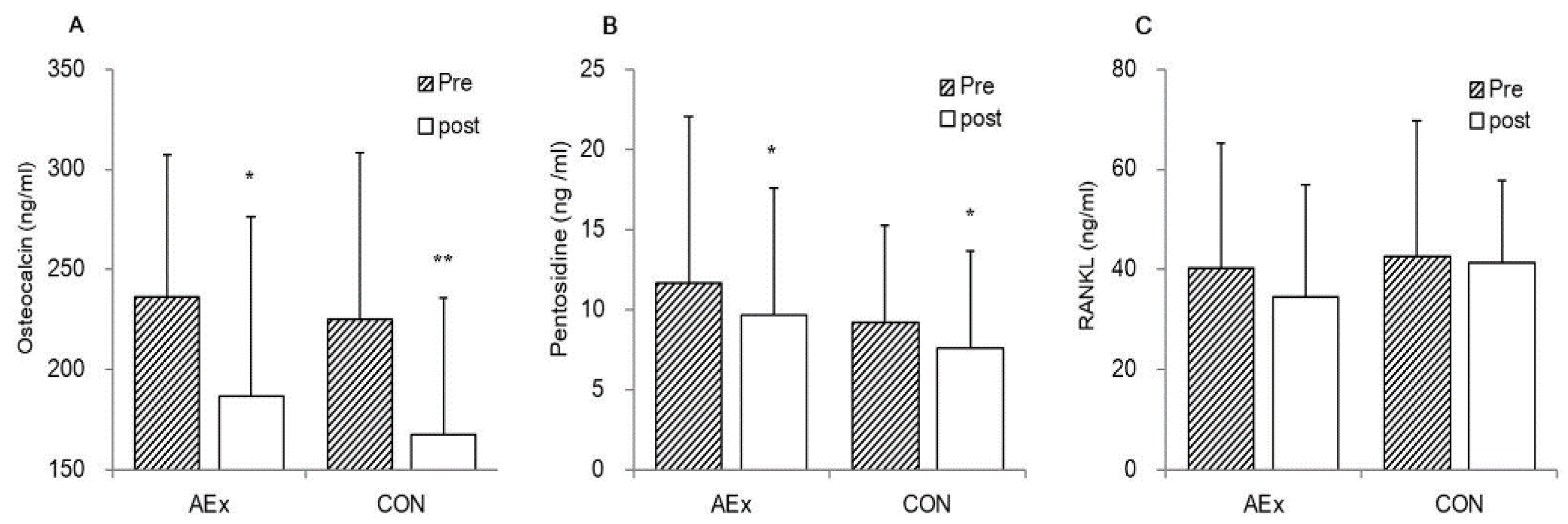
3.3. Change in Bone Turnover Markers after the Intervention
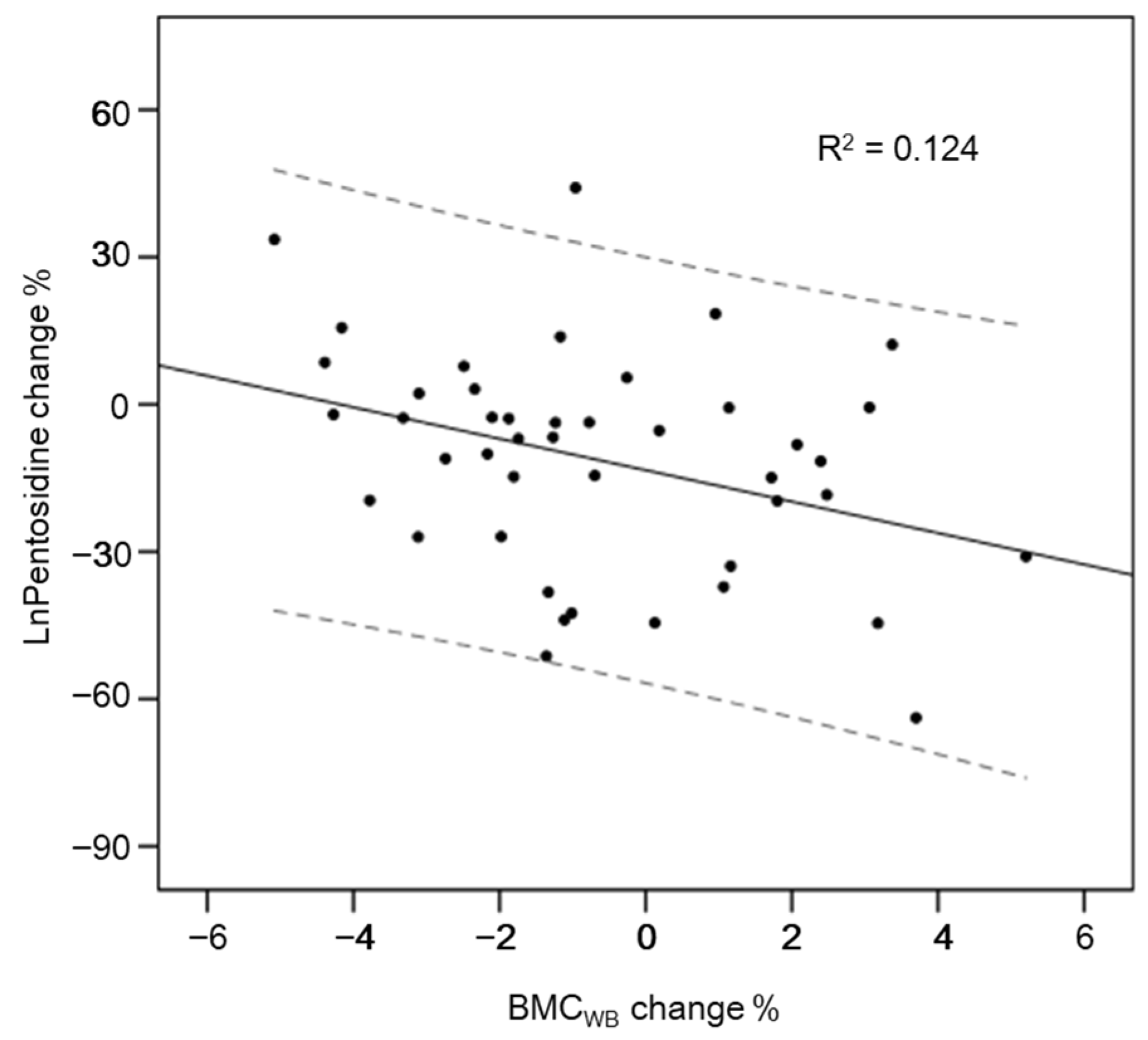
3.4. Associations between Biomarkers and BMC/BMD
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Moayeri, A.; Mohamadpour, M.; Mousavi, S.F.; Shirzadpour, E.; Mohamadpour, S.; Amraei, M. Fracture risk in patients with type 2 diabetes mellitus and possible risk factors: A systematic review and meta-analysis. Ther. Clin. Risk Manag. 2017, 13, 455–468. [Google Scholar] [CrossRef]
- Upala, S.; Sanguankeo, A.; Jaruvongvanich, V. Association between nonalcoholic fatty liver disease and bone mineral density: A systematic review and meta-analysis. J. Endocrinol. Investig. 2015, 38, 931–932. [Google Scholar] [CrossRef]
- Cui, R.; Sheng, H.; Rui, X.F.; Cheng, X.Y.; Sheng, C.J.; Wang, J.Y.; Qu, S. Low bone mineral density in chinese adults with nonalcoholic Fatty liver disease. Int. J. Endocrinol. 2013, 2013, 396545. [Google Scholar] [CrossRef] [PubMed]
- Moon, S.S.; Lee, Y.S.; Kim, S.W. Association of nonalcoholic fatty liver disease with low bone mass in postmenopausal women. Endocrine 2012, 42, 423–429. [Google Scholar] [CrossRef] [PubMed]
- Xiao, J.; Wang, F.; Wong, N.K.; He, J.; Zhang, R.; Sun, R.; Xu, Y.; Liu, Y.; Li, W.; Koike, K.; et al. Global liver disease burdens and research trends: Analysis from a Chinese perspective. J. Hepatol. 2019, 71, 212–221. [Google Scholar] [CrossRef] [PubMed]
- Ng, K.W. Regulation of glucose metabolism and the skeleton. Clin. Endocrinol. 2011, 75, 147–155. [Google Scholar] [CrossRef]
- Lu, C.; Ivaska, K.K.; Alen, M.; Wang, Q.; Törmäkangas, T.; Xu, L.; Wiklund, P.; Mikkola, T.M.; Pekkala, S.; Tian, H.; et al. Serum osteocalcin is not associated with glucose but is inversely associated with leptin across generations of nondiabetic women. J. Clin. Endocrinol. Metab. 2012, 97, 4106–4114. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.M.; Mosialou, I.; Liu, J.M. Bone: Another potential target to treat, prevent and predict diabetes. Diabetes Obes. Metab. 2018, 20, 1817–1828. [Google Scholar] [CrossRef]
- Kiechl, S.; Wittmann, J.; Giaccari, A.; Knoflach, M.; Willeit, P.; Bozec, A.; Moschen, A.R.; Muscogiuri, G.; Sorice, G.P.; Kireva, T.; et al. Blockade of receptor activator of nuclear factor-κB (RANKL) signaling improves hepatic insulin resistance and prevents development of diabetes mellitus. Nat. Med. 2013, 19, 358–363. [Google Scholar] [CrossRef] [PubMed]
- Mantovani, A.; Sani, E.; Fassio, A.; Colecchia, A.; Viapiana, O.; Gatti, D.; Idolazzi, L.; Rossini, M.; Salvagno, G.; Lippi, G.; et al. Association between non-alcoholic fatty liver disease and bone turnover biomarkers in post-menopausal women with type 2 diabetes. Diabetes Metab. 2019, 45, 347–355. [Google Scholar] [CrossRef]
- Choi, D.H.; Lee, S.M.; Lim, S.A.; Choi, Y.S. Feasibility of Serum Pentosidine Level as a Potential Risk Factor for Osteoporotic Vertebral Compression Fracture. Asian Spine J. 2018, 12, 992–997. [Google Scholar] [CrossRef]
- Yamamoto, M.; Yamaguchi, T.; Yamauchi, M.; Yano, S.; Sugimoto, T. Serum pentosidine levels are positively associated with the presence of vertebral fractures in postmenopausal women with type 2 diabetes. J. Clin. Endocrinol. Metab. 2008, 93, 1013–1019. [Google Scholar] [CrossRef]
- Guadalupe-Grau, A.; Fuentes, T.; Guerra, B.; Calbet, J.A. Exercise and bone mass in adults. Sports Med. 2009, 39, 439–468. [Google Scholar] [CrossRef]
- Tschentscher, M.; Niederseer, D.; Niebauer, J. Health benefits of Nordic walking: A systematic review. Am. J. Prev. Med. 2013, 44, 76–84. [Google Scholar] [CrossRef] [PubMed]
- Cugusi, L.; Manca, A.; Yeo, T.J.; Bassareo, P.P.; Mercuro, G.; Kaski, J.C. Nordic walking for individuals with cardiovascular disease: A systematic review and meta-analysis of randomized controlled trials. Eur. J. Prev. Cardiol. 2017, 24, 1938–1955. [Google Scholar] [CrossRef] [PubMed]
- Cugusi, L.; Manca, A.; Dragone, D.; Deriu, F.; Solla, P.; Secci, C.; Monticone, M.; Mercuro, G. Nordic Walking for the Management of People with Parkinson Disease: A Systematic Review. PM & R 2017, 9, 1157–1166. [Google Scholar]
- Sánchez-Lastra, M.A.; Torres, J. Nordic walking for women with breast cancer: A systematic review. Eur. J. Cancer Care 2019, 28, e13130. [Google Scholar] [CrossRef]
- Shim, J.M.; Kwon, H.Y.; Kim, H.R.; Kim, B.I.; Jung, J.H. Comparison of the Effects of Walking with and without Nordic Pole on Upper Extremity and Lower Extremity Muscle Activation. J. Phys. Ther. Sci. 2013, 25, 1553–1556. [Google Scholar] [CrossRef]
- Liu, W.Y.; Lu, D.J.; Du, X.M.; Sun, J.Q.; Ge, J.; Wang, R.W.; Wang, R.; Zou, J.; Xu, C.; Ren, J.; et al. Effect of aerobic exercise and low carbohydrate diet on pre-diabetic non-alcoholic fatty liver disease in postmenopausal women and middle aged men—The role of gut microbiota composition: Study protocol for the AELC randomized controlled trial. BMC Public Health 2014, 14, 48. [Google Scholar] [CrossRef] [PubMed]
- Cheng, S.; Ge, J.; Zhao, C.; Le, S.; Yang, Y.; Ke, D.; Wu, N.; Tan, X.; Zhang, X.; Du, X.; et al. Effect of aerobic exercise and diet on liver fat in pre-diabetic patients with non-alcoholic-fatty-liver-disease: A randomized controlled trial. Sci. Rep. 2017, 7, 15952. [Google Scholar] [CrossRef]
- Matthews, D.R.; Hosker, J.P.; Rudenski, A.S.; Naylor, B.A.; Treacher, D.F.; Turner, R.C. Homeostasis model assessment: Insulin resistance and beta-cell function from fasting plasma glucose and insulin concentrations in man. Diabetologia 1985, 28, 412–419. [Google Scholar] [CrossRef]
- Bonjour, J.P.; Chevalley, T.; Ferrari, S.; Rizzoli, R. The importance and relevance of peak bone mass in the prevalence of osteoporosis. Salud Publica Mex. 2009, 51 (Suppl. 1), S5–S17. [Google Scholar] [CrossRef]
- Cheng, X.G.; Yang, D.Z.; Zhou, Q.; Zhuo, T.J.; Zhang, H.C.; Xiang, J.; Wang, H.F.; Ou, P.Z.; Liu, J.L.; Xu, L.; et al. Age-related bone mineral density, bone loss rate, prevalence of osteoporosis, and reference database of women at multiple centers in China. J. Clin. Densitom. 2007, 10, 276–284. [Google Scholar] [CrossRef]
- Kemmler, W.; Bebenek, M.; von Stengel, S.; Engelke, K.; Kalender, W.A. Effect of block-periodized exercise training on bone and coronary heart disease risk factors in early post-menopausal women: A randomized controlled study. Scand. J. Med. Sci. Sports 2013, 23, 121–129. [Google Scholar] [CrossRef] [PubMed]
- Skoradal, M.B.; Helge, E.W. Osteogenic impact of football training in 55- to 70-year-old women and men with prediabetes. Scand. J. Med. Sci. Sports 2018, 28 (Suppl. 1), 52–60. [Google Scholar] [CrossRef] [PubMed]
- Chien, M.Y.; Wu, Y.T.; Hsu, A.T.; Yang, R.S.; Lai, J.S. Efficacy of a 24-week aerobic exercise program for osteopenic postmenopausal women. Calcif. Tissue Int. 2000, 67, 443–448. [Google Scholar] [CrossRef]
- Martin, D.; Notelovitz, M. Effects of aerobic training on bone mineral density of postmenopausal women. J. Bone Miner. Res. 1993, 8, 931–936. [Google Scholar] [CrossRef]
- Borer, K.T.; Fogleman, K.; Gross, M.; La New, J.M.; Dengel, D. Walking intensity for postmenopausal bone mineral preservation and accrual. Bone 2007, 41, 713–721. [Google Scholar] [CrossRef] [PubMed]
- Cavanaugh, D.J.; Cann, C.E. Brisk walking does not stop bone loss in postmenopausal women. Bone 1988, 9, 201–204. [Google Scholar] [CrossRef]
- Willson, J.; Torry, M.R.; Decker, M.J.; Kernozek, T.; Steadman, J.R. Effects of walking poles on lower extremity gait mechanics. Med. Sci. Sports Exerc. 2001, 33, 142–147. [Google Scholar] [CrossRef]
- Lanyon, L.E. Functional strain as a determinant for bone remodeling. Calcif. Tissue Int. 1984, 36 (Suppl. 1), S56–S61. [Google Scholar] [CrossRef] [PubMed]
- Bemben, D.A.; Fetters, N.L.; Bemben, M.G.; Nabavi, N.; Koh, E.T. Musculoskeletal responses to high- and low-intensity resistance training in early postmenopausal women. Med. Sci. Sports Exerc. 2000, 32, 1949–1957. [Google Scholar] [CrossRef]
- Danz, A.M.; Zittermann, A.; Schiedermaier, U.; Klein, K.; Hötzel, D.; Schönau, E. The effect of a specific strength-development exercise on bone mineral density in perimenopausal and postmenopausal women. J. Womens Health 1998, 7, 701–709. [Google Scholar] [CrossRef] [PubMed]
- Shibata, Y.; Ohsawa, I.; Watanabe, T.; Miura, T.; Sato, Y. Effects of physical training on bone mineral density and bone metabolism. J. Physiol. Anthropol. Appl. Hum. Sci. 2003, 22, 203–208. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Wochna, K.; Nowak, A.; Huta-Osiecka, A.; Sobczak, K.; Kasprzak, Z.; Leszczyński, P. Bone Mineral Density and Bone Turnover Markers in Postmenopausal Women Subjected to an Aqua Fitness Training Program. Int. J. Environ. Res. Public Health 2019, 16, 2505. [Google Scholar] [CrossRef] [PubMed]
- Boyle, W.J.; Simonet, W.S.; Lacey, D.L. Osteoclast differentiation and activation. Nature 2003, 423, 337–342. [Google Scholar] [CrossRef]
- Marques, E.A.; Wanderley, F.; Machado, L.; Sousa, F.; Viana, J.L.; Moreira-Gonçalves, D.; Moreira, P.; Mota, J.; Carvalho, J. Effects of resistance and aerobic exercise on physical function, bone mineral density, OPG and RANKL in older women. Exp. Gerontol. 2011, 46, 524–532. [Google Scholar] [CrossRef]
- Marques, E.A.; Mota, J.; Viana, J.L.; Tuna, D.; Figueiredo, P.; Guimarães, J.T.; Carvalho, J. Response of bone mineral density, inflammatory cytokines, and biochemical bone markers to a 32-week combined loading exercise programme in older men and women. Arch. Gerontol. Geriatr. 2013, 57, 226–233. [Google Scholar] [CrossRef]
- Esen, H.; Bueyuekyazi, G.; Ulman, C.; Taneli, F.; Tikiz, H. Do walking programs affect C-reactive protein, osteoprotegerin and soluble receptor activator of nuclear factor-kappa β ligand? Türk Biyokim. Derg. 2009, 34, 178–186. [Google Scholar]
- Yamamoto, M.; Sugimoto, T. Advanced Glycation End Products, Diabetes, and Bone Strength. Curr. Osteoporos. Rep. 2016, 14, 320–326. [Google Scholar] [CrossRef]
- Franke, S.; Rüster, C.; Pester, J.; Hofmann, G.; Oelzner, P.; Wolf, G. Advanced glycation end products affect growth and function of osteoblasts. Clin. Exp. Rheumatol. 2011, 29, 650–660. [Google Scholar] [PubMed]
- Okazaki, K.; Yamaguchi, T.; Tanaka, K.; Notsu, M.; Ogawa, N.; Yano, S.; Sugimoto, T. Advanced glycation end products (AGEs), but not high glucose, inhibit the osteoblastic differentiation of mouse stromal ST2 cells through the suppression of osterix expression, and inhibit cell growth and increasing cell apoptosis. Calcif. Tissue Int. 2012, 91, 286–296. [Google Scholar] [CrossRef] [PubMed]
- Sanguineti, R.; Storace, D.; Monacelli, F.; Federici, A.; Odetti, P. Pentosidine effects on human osteoblasts in vitro. Ann. N. Y. Acad. Sci. 2008, 1126, 166–172. [Google Scholar] [CrossRef] [PubMed]
- Valcourt, U.; Merle, B.; Gineyts, E.; Viguet-Carrin, S.; Delmas, P.D.; Garnero, P. Non-enzymatic glycation of bone collagen modifies osteoclastic activity and differentiation. J. Biol. Chem. 2007, 282, 5691–5703. [Google Scholar] [CrossRef]
- Ma, L.; Oei, L.; Jiang, L.; Estrada, K.; Chen, H.; Wang, Z.; Yu, Q.; Zillikens, M.C.; Gao, X.; Rivadeneira, F. Association between bone mineral density and type 2 diabetes mellitus: A meta-analysis of observational studies. Eur. J. Epidemiol. 2012, 27, 319–332. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Exercise Group (n = 33) | Control Group (n = 30) | |
|---|---|---|
| Age (years) | 59.8 (58.5, 61.1) | 59.7 (58.2, 61.1) |
| Height (m) | 159.6 (157.6, 161.7) | 157 (154.5, 159.5) |
| Weight (kg) | 67.1 (64, 70.2) | 63.8 (59.5, 68.1) |
| BMI (kg/m2) | 26.4 (25.2, 27.6) | 25.8 (24.4, 27.2) |
| Age at menopause (years) | 49.1 (47.2, 51.0) | 51 (49.4, 52.6) |
| Years post-menopausal (years) | 10.6 (8.4, 12.9) | 8.7 (6.8, 10.5) |
| FPG (mmol/L) | 5.61 (5.39, 5.83) | 5.55 (5.3, 5.81) |
| 2hPG (mmol/L) | 8.08 (7.47, 8.7) | 8.20 (7.68, 8.72) |
| HbA1c (%) | 6.12 (6, 6.24) | 6.21 (6.09, 6.33) |
| FSH (nmol/L) | 50.9 (41.5, 60.4) | 50.1 (42.6, 57.5) |
| Osteocalcin (ng/mL) | 236.4 (208.3, 264.4) | 225 (189.8, 260.2) |
| Pentosidine (ng/mL) | 13.7 (7.9, 19.4) | 11.5 (6.1, 17.0) |
| RANKL (pg/mL) | 46.4 (30.9, 62.0) | 42.7 (32.6, 52.8) |
| Calcium intake (mg) | 580.7 (452.2, 709.1) | 666.2 (560.5, 771.9) |
| Physical activity (h/week) | 2.45 (1.8, 3.1) | 2.45 (1.83, 3.07) |
| Whole body T-score | −0.13 (−0.47, 0.22) | −0.20 (−0.54, 0.14) |
| Total femur T-score | −0.07 (−0.45, 0.31) | −0.20 (−0.61, 0.20) |
| Femoral neck T-score | −0.62 (−0.97, −0.26) | −0.54 (−0.93, −0.15) |
| Lumbar spine T-score | −0.13 (−0.65, 0.38) | −0.15 (−0.72, 0.42) |
| Exercise Group | Control Group | Time by Group | |||||
|---|---|---|---|---|---|---|---|
| Pre | Post | p | Pre | Post | p | p | |
| Whole-body | |||||||
| BMC (kg) | 2.07 (1.98, 2.16) | 2.06 (1.96, 2.16) | 0.195 | 2.00 (1.89, 2.11) | 1.99 (1.87, 2.10) | 0.589 | 0.216 |
| BMD (g/cm2) | 1.07 (1.03, 1.11) | 1.07 (1.03, 1.12) | 0.961 | 1.07 (1.03, 1.11) | 1.06 (1.02, 1.11) | 0.756 | 0.952 |
| Total-femur | |||||||
| BMC (g) | 29.2 (27.5, 30.9) | 29.3 (27.6, 31.1) | 0.927 | 28.1 (26.3, 29.9) | 27.6 (25.8, 29.3) | 0.008 | 0.587 |
| BMD (g/cm2) | 0.96 (0.91, 1.01) | 0.96 (0.91, 1.02) | 0.074 | 0.95 (0.89, 1) | 0.93 (0.88, 0.98) | 0.001 | 0.183 |
| Femoral neck | |||||||
| BMC (g) | 4.02 (3.79, 4.25) | 4.06 (3.83, 4.29) | 0.016 | 3.98 (3.7, 4.25) | 4.27 (3.93, 4.61) | 0.131 | 0.579 |
| BMD (g/cm2) | 0.86 (0.82, 0.91) | 0.87 (0.82, 0.92) | 0.156 | 0.87 (0.82, 0.91) | 0.86 (0.82, 0.91) | 0.606 | 0.297 |
| Lumbar spine | |||||||
| BMC (g) | 46.0 (43.1, 48.8) | 45.8 (42.7, 48.9) | 0.821 | 43.8 (40.5, 47.1) | 42.7 (39.3, 46.1) | 0.141 | 0.323 |
| BMD (g/cm2) | 1.12 (1.06, 1.18) | 1.12 (1.06, 1.18) | 0.592 | 1.11 (1.05, 1.18) | 1.09 (1.02, 1.15) | 0.002 | 0.013 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Du, X.; Zhang, C.; Zhang, X.; Qi, Z.; Cheng, S.; Le, S. The Impact of Nordic Walking on Bone Properties in Postmenopausal Women with Pre-Diabetes and Non-Alcohol Fatty Liver Disease. Int. J. Environ. Res. Public Health 2021, 18, 7570. https://doi.org/10.3390/ijerph18147570
Du X, Zhang C, Zhang X, Qi Z, Cheng S, Le S. The Impact of Nordic Walking on Bone Properties in Postmenopausal Women with Pre-Diabetes and Non-Alcohol Fatty Liver Disease. International Journal of Environmental Research and Public Health. 2021; 18(14):7570. https://doi.org/10.3390/ijerph18147570
Chicago/Turabian StyleDu, Xiaming, Chao Zhang, Xiangqi Zhang, Zhen Qi, Sulin Cheng, and Shenglong Le. 2021. "The Impact of Nordic Walking on Bone Properties in Postmenopausal Women with Pre-Diabetes and Non-Alcohol Fatty Liver Disease" International Journal of Environmental Research and Public Health 18, no. 14: 7570. https://doi.org/10.3390/ijerph18147570
APA StyleDu, X., Zhang, C., Zhang, X., Qi, Z., Cheng, S., & Le, S. (2021). The Impact of Nordic Walking on Bone Properties in Postmenopausal Women with Pre-Diabetes and Non-Alcohol Fatty Liver Disease. International Journal of Environmental Research and Public Health, 18(14), 7570. https://doi.org/10.3390/ijerph18147570