
Cariogenic Risk and COVID-19 Lockdown in a Paediatric Population


 , , ,
, , , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Survey Methodology
2.2. Mediterranean Diet Quality Index (KIDMED) Questionnaire
2.3. Cariogenic Risk during COVID-19 Questionnaire
2.4. Statistical Analyses
3. Results
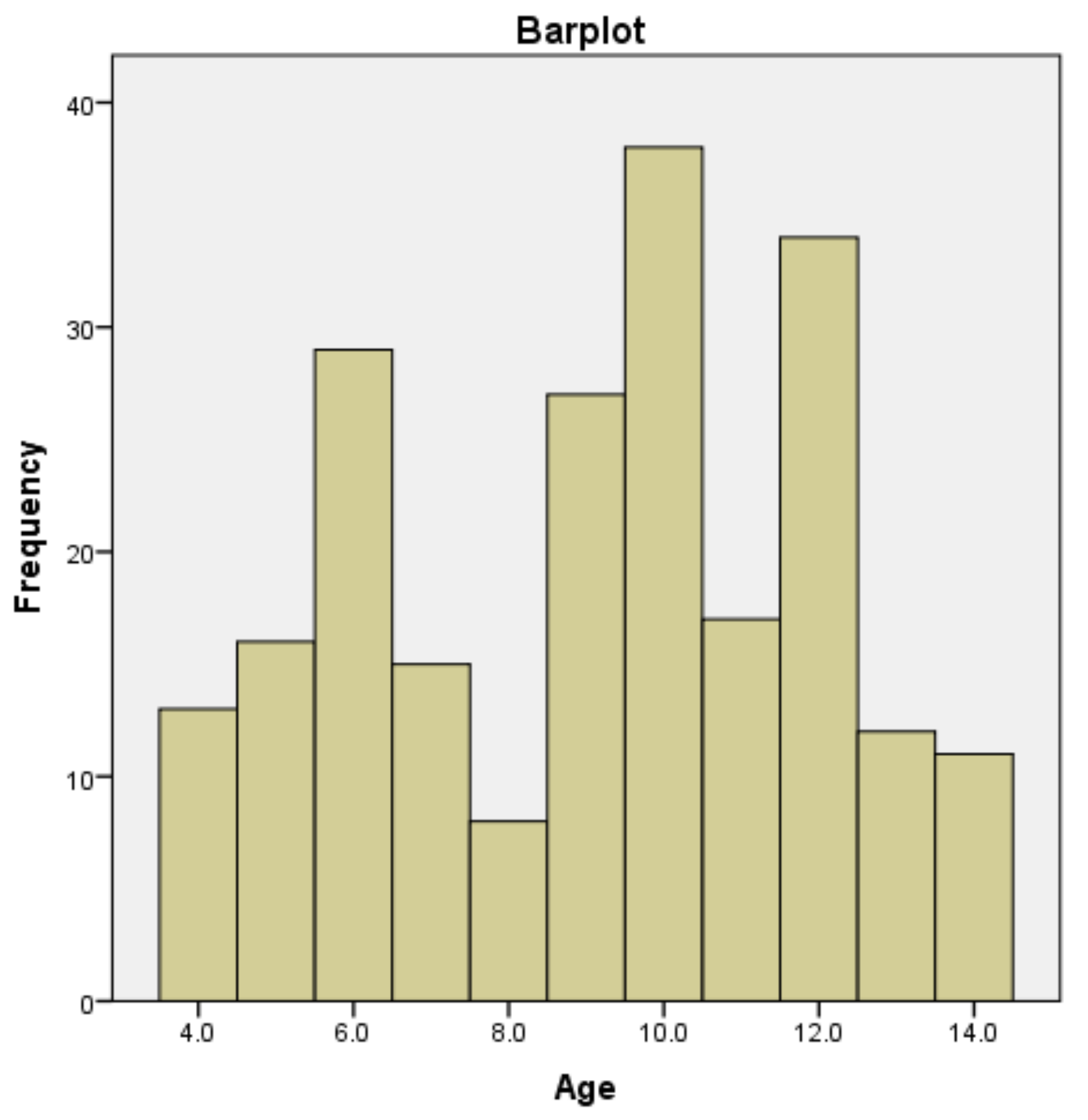
3.1. Participants
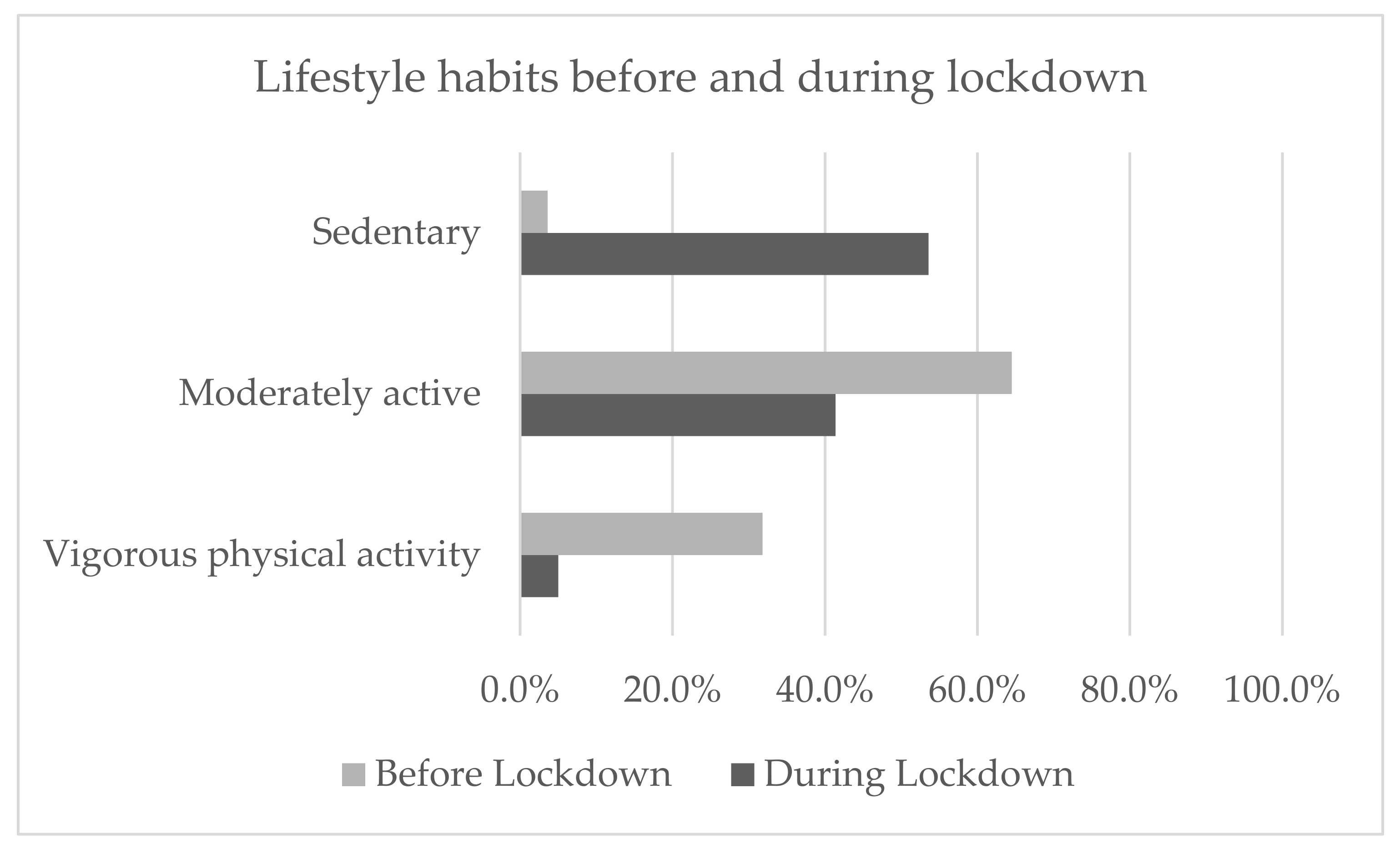
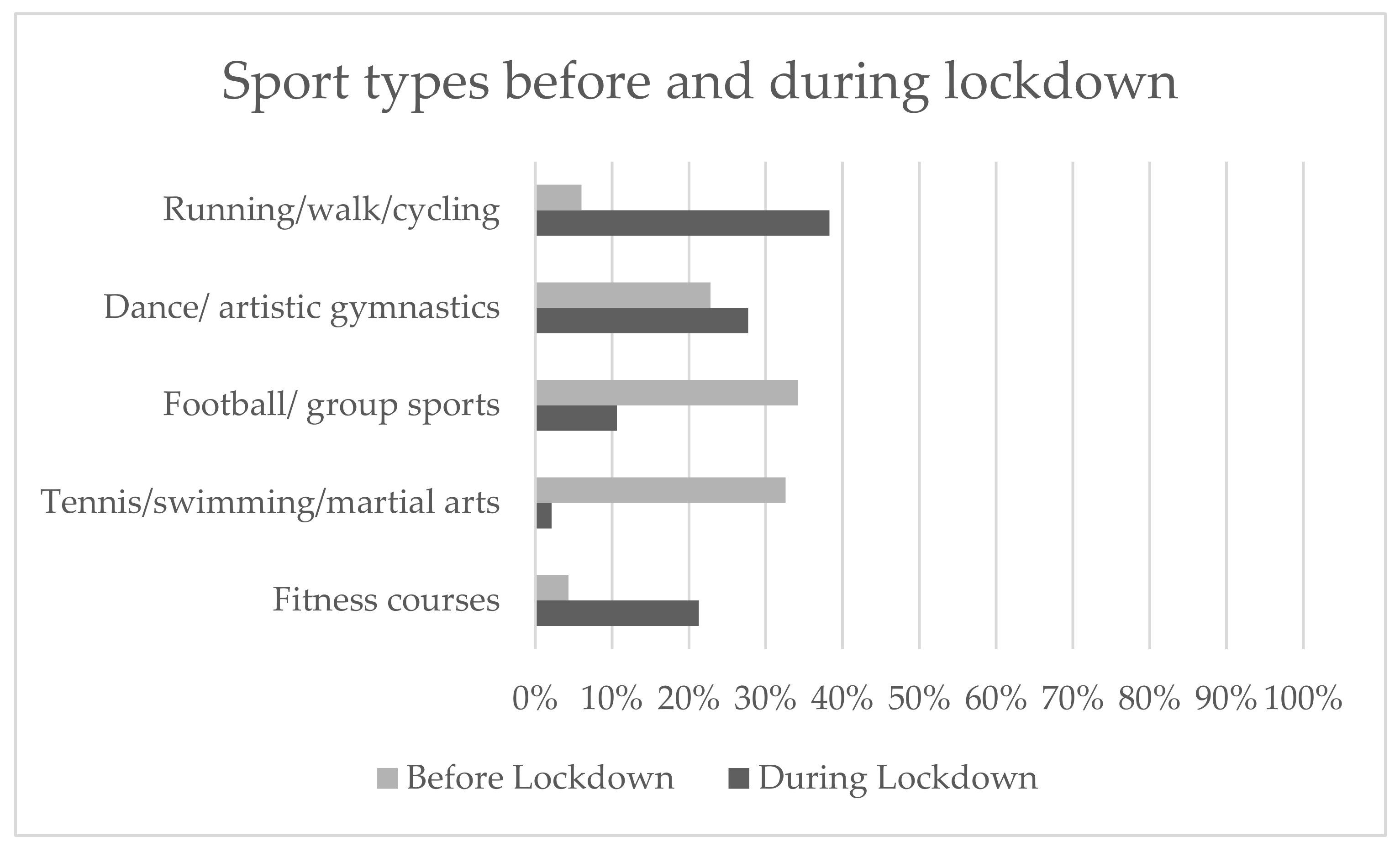
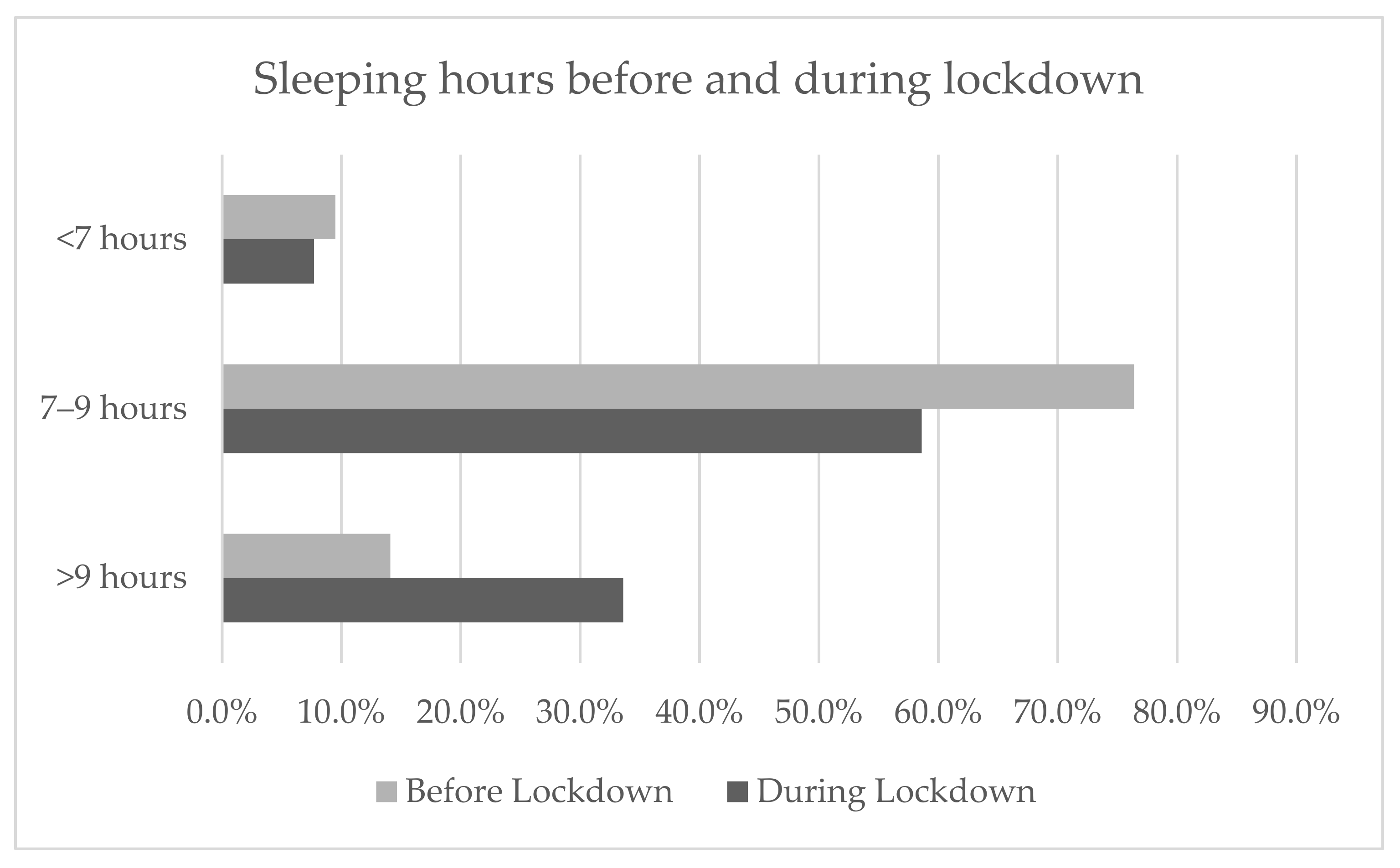
3.2. Lifestyle
3.3. Oral Hygiene
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Questions | Answers | |
|---|---|---|
| 1. Parent 1 gender | Male/Female | |
| 2. Parent 1 weight | Weight in kg | |
| 3. Parent 1 height | Height in cm | |
| 4. Parent 1 ethnicity | Caucasian/Hispanic/Afro-American/Asian | |
| 5. Parent 1 nationality is Italian? | Yes/No | |
| 6. Parent 1 degree of education | None/Elementary School Diploma/Superior School Diploma/Master’s Degree/Post-Master’s Degree Diploma | |
| Socio-economic status of the family | 7. Parent 1 occupation | Employee/Manager/Teacher/Freelance Merchant/Artisan/Parasanitary personnel/Workmen/Retired/Unemployed/ Armed forces and security/Other |
| 8. Parent 2 gender | Male/Female | |
| 9. Parent 2 weight | Weight in kg | |
| 10. Parent 2 height | Height in cm. | |
| 11. Parent 2 ethnicity | Caucasian/Hispanic/Afro-American/Asian | |
| 12. Parent 2 nationality: Italian? | Yes/No | |
| 13. Parent 2 degree of education | None/Elementary School Diploma/Superior School Diploma/Master’s Degree/Post-Master’s Degree Diploma | |
| 14. Parent 2 occupation | Employee/Manager/Teacher/Freelance/ Merchant/Artisan/Parasanitary personnel/Workmen/Retired/Unemployed/ Armed forces and security/Other | |
| 15. Child gender | Male/Female | |
| 16. Age | 4/5/6/7/8/9/10/11/12/13/14 | |
| 17. Region of residence | Valle D’Aosta/Piemonte/Liguria/Lombardia Trentino-Alto Adige/Veneto/Friuli-Venezia Giulia/Emilia Romagna/Toscana/Umbria Marche/Lazio/Abruzzo/Molise/Campania Puglia/Basilicata/Calabria/Sicilia/Sardegna | |
| Personal and anthropometric data for the child | 18. Province of residence | AG/AL/AN/AO/AQ/AR/AP/AT/AV/BA/BT/BL BN/BG/BI/BO/BZ/BS/BR/CA/CB/CL/CI/CE CT/CZ/CH/CO/CS/CR/KR/CN/EN/FM/FE/FI FG/FC/FR/GE/GO/GR/IM/IS/SP/LT/LE/LC LI/LO/LU/MC/MN/MS/MT/VS/ME/MI/MO MB/NA/NO/NU/OG/OT/OR/PD/PA/PR/PV PG/PU/PE/PC/PI/PT/PN/PZ/PO/RG/RA/RC RE/RI/RN/RM/RO/SA/SS/SV/SI/SR/SO/TA TE/TR/TO/TP/TN/TV/TS/UD/VA/VE/VB/VC VR/VV/VI/VT |
| 19. Child height | Height in cm | |
| 20. Child weight | Weight in kg | |
| 21. Lactation prevalent in the first 6 months of life | Breastfeeding/Formula milk/Mixed | |
| 22. Before the lockdown, did the child have caries? | Yes/No | |
| 23. During the lockdown, has the child experienced teeth pain? | Yes/No | |
| 24. During the lockdown, did the child have dental abscesses? | Yes/No | |
| 25. Before the lockdown, how many times a day did the child brush their teeth? | 0/1/2/3/4/5 | |
| Child oral health before and during lockdown | 26. Before the lockdown, did the child use fluoride toothpaste? | Never/Sometimes/Often/Always |
| 27. During the lockdown, did the child use fluoride toothpaste? | Never/Sometimes/Often/Always | |
| 28. During the lockdown, has the child used the parents’ toothpaste or personal toothpaste, or none? | No toothpaste/His/her personal toothpaste/Parents’ toothpaste | |
| 29. During the lockdown, has the child’s teeth-brushing habits changed? | Have not changed/The frequency of tooth cleaning has increased/The frequency of tooth cleaning has decreased | |
| 30. Before the lockdown, did the child brush their teeth before going to sleep? | Yes/No | |
| 31. During the lockdown, has the child brushed their teeth before going to sleep? | Yes/No | |
| 32. Before the lockdown, how many meals did the child have during the day? | 0/1/2/3/4/5/6/7/8 | |
| 33. During the lockdown, how many meals has the child eaten a day? | 0/1/2/3/4/5/6/7/8 | |
| 34. Before the lockdown, did the child eat between meals? | Yes/No | |
| Eating habits of the child before and during lockdown | 35. During the lockdown, has the child eaten between meals? | Yes/No |
| 36. Before the lockdown, did the child eat candies/chocolate, or drink milk/herbal tea before going to sleep? | Never/1 time a week/2 times a week/3 times a week/4 times a week/5 times a week/6 times a week/7 times a week | |
| 37. During the lockdown, has the child eaten snacks, cookies, or drank milk before going to sleep? | Never/1 time a week/2 times a week/3 times a week/4 times a week/5 times a week/6 times a week/7 times a week | |
| 38. Did the child take probiotic supplements before the lockdown? | Yes/No | |
| 39. Has the child taken probiotic supplements during the lockdown? | Yes/No | |
| 40. During the lockdown, how did the diet change—increase or decrease in terms of sugary food? | Not modified/Preferred sweets more/Reduced intake of sweet foods/Drank more sugary drinks/Reduced intake of sugary drinks/He/she was bored and sedentary and eating activities compensated | |
| 41. During the lockdown, has the child consumed a fruit or fruit centrifuge/juice once a day? | Yes/No | |
| 42. During the lockdown, has a second fruit been consumed every day by the child? | Yes/No | |
| 43. During the lockdown, has the child regularly consumed vegetables once a day? | Yes/No | |
| 44. During the lockdown, did the child eat multiple servings of raw or cooked vegetables per day? | Yes/No | |
| 45. During the lockdown, has fish been consumed regularly, twice or three times a week, by the child? | Yes/No | |
| 46. During the lockdown, has fast food been consumed more than once a week by the child? | Yes/No | |
| 47. During the lockdown, have legumes been consumed more than once a week by the child? | Yes/No | |
| 48. During the lockdown, has pasta or rice been consumed every day (5 or more days a week) by the child? | Yes/No | |
| Child feeding during lockdown | 49. During the lockdown, has the child consumed cereals (cornflakes) or bread for breakfast? | Yes/No |
| 50. During the lockdown, have dry fruits like almonds or nuts been consumed regularly (2–3 times a week) by the child? | Yes/No | |
| 51. During the lockdown, has the child consumed olive oil? | Yes/No | |
| 52. During the lockdown, has the child skipped breakfast? | Yes/No | |
| 53. During the lockdown, has the child eaten dairy products such as yogurt or milk for breakfast? | Yes/No | |
| 54. During the lockdown, has the child consumed cookies, cakes, or snacks for breakfast? | Yes/No | |
| 55. During the lockdown, has the child consumed 2 yogurts or cheese every day? | Yes/No | |
| 56. During the lockdown, has the child eaten candies, sweetened foods (cookies, cakes, ice creams etc.) more often? | Yes/No | |
| 57. During the lockdown, has the child consumed more sweetened foods? | Yes/No | |
| 58. During the lockdown, how many eggs did the child consume per week? | 0/0.5/1/2/3/4/5/6/7/8/9/10 | |
| 59. During the lockdown how much water did the child drink? | Less than 1 L/Between 1 L and 2 L/More than 2 L | |
| 60. Before the lockdown, what was the lifestyle habit of the child? | Sedentary hypokinetic/Sedentary/Moderately Active/Intense physical activity | |
| 61. During the lockdown, what was the lifestyle habit of the child? | Sedentary hypokinetic/Sedentary/Moderately active/Intense physical activity | |
| 62. Before the lockdown, how many hours of sleep did the child get? | Less than 7 h/Between 7 and 9 h/More than 9 h | |
| 63. During the lockdown, how many hours of sleep did the child get? | Less than 7 h/Between 7 and 9 h/More than 9 h | |
| 64. Before the lockdown, did the child do any physical activities? | Yes/No | |
| Child lifestyle before and during lockdown | 65. Before the lockdown, what sport did the child play? | Fitness Course/Running/Walking/Cycling, Football/Basket/Volleyball/Martial Arts/Tennis, Paddle/Swim/Dance/Artistic Gymnastics |
| 66. Before the lockdown, how many weekly hours of physical activity did the child do? | 1/2/3/4/5/6/7/8/9/10/11/12/13/14/15/16/17/18/19/20 | |
| 67. During the lockdown, did the child play any sports? | Yes/No | |
| 68. What sport did the child play during lockdown? | Fitness Course/Running/Walking/Cycling, Football/Basket/Volleyball/Martial Arts/Tennis, Paddle/Swim/Dance/Artistic Gymnastics | |
| 69. During the lockdown, how many weekly hours of physical activity did the child do? | 1/2/3/4/5/6/7/8/9/10/11/12/13/14/15/16/17/18/19/20 | |
| 70. Before the lockdown, how many hours a day did the child spend playing videogames or watching TV? | 0/0.5/1/2/3/4/5/6/7/8 | |
| 71. During the lockdown, how many hours per day did the child spend playing videogames or watching tv? | 0/0.5/1/2/3/4/5/6/7/8 | |
| 72. During the lockdown, how many hours per day did the child spend doing online classes? | 0/0.5/1/2/3/4/5/6 |
Appendix B

References
- Saadat, S.; Rawtani, D.; Hussain, C.M. Environmental Perspective of COVID-19. Sci. Total Environ. 2020, 728, 138870. [Google Scholar] [CrossRef]
- Di Renzo, L.; Gualtieri, P.; Pivari, F.; Soldati, L.; Attinà, A.; Cinelli, G.; Leggeri, C.; Caparello, G.; Barrea, L.; Scerbo, F.; et al. Eating Habits and Lifestyle Changes during COVID-19 Lockdown: An Italian Survey. J. Transl. Med. 2020, 18, 229. [Google Scholar] [CrossRef]
- Coronavirus, la Normativa Vigente. Available online: www.governo.it/it/coronavirus-normativa#:~:text=74%2C%20recante%3A%20%C2%ABUlteriori%20misure,del%20virus%20COVID%2D19%C2%BB (accessed on 6 April 2021).
- Di Renzo, L.; Gualtieri, P.; Cinelli, G.; Bigioni, G.; Soldati, L.; Attinà, A.; Bianco, F.F.; Caparello, G.; Camodeca, V.; Carrano, E.; et al. Psychological Aspects and Eating Habits during COVID-19 Home Confinement: Results of EHLC-COVID-19 Italian Online Survey. Nutrients 2020, 12, 2152. [Google Scholar] [CrossRef]
- Selwitz, R.H.; Ismail, A.I.; Pitts, N.B. Dental Caries. Lancet 2007, 369, 51–59. [Google Scholar] [CrossRef]
- WHO. Oral Health. Available online: www.who.int/health-topics/oral-health/#tab=tab_1 (accessed on 6 April 2021).
- Pitts, N.B.; Zero, D.T.; Marsh, P.D.; Ekstrand, K.; Weintraub, J.A.; Ramos-Gomez, F.; Tagami, J.; Twetman, S.; Tsakos, G.; Ismail, A. Dental Caries. Nat. Rev. Dis. Primers 2017, 3, 17030. [Google Scholar] [CrossRef]
- Costacurta, M.; Epis, M.; Docimo, R. Evaluation of DMFT in Paediatric Patients with Social Vulnerability Conditions. Eur. J. Paediatr. Dent. 2020, 70–73. [Google Scholar] [CrossRef]
- Ferrazzano, G.F.; Cantile, T.; Sangianantoni, G.; Ingenito, A.; Rengo, S.; Alcidi, B.; Spagnuolo, G. Oral Health Status and Unmet Restorative Treatment Needs (UTN) in Disadvantaged Migrant and Not Migrant Children in Italy. Eur. J. Paediatr. Dent. 2019, 10–14. [Google Scholar] [CrossRef]
- Moynihan, P. Sugars and Dental Caries: Evidence for Setting a Recommended Threshold for Intake. Adv. Nutr. 2016, 7, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Paglia, L. The Sweet Danger of Added Sugars. Eur. J. Paediatr. Dent. 2019, 89. [Google Scholar] [CrossRef]
- Paglia, L.; Scaglioni, S.; Torchia, V.; De Cosmi, V.; Moretti, M.; Marzo, G.; Giuca, M.R. Familial and Dietary Risk Factors in Early Childhood Caries. Eur. J. Paediatr. Dent. 2016, 17, 93–99. [Google Scholar] [PubMed]
- Anil, S.; Anand, P.S. Early Childhood Caries: Prevalence, Risk Factors, and Prevention. Front. Pediatr. 2017, 5, 157. [Google Scholar] [CrossRef]
- WHO. Guideline; World Health Organization: Geneva, Switzerland, 2015; ISBN 978-92-4-069422-4. [Google Scholar]
- Breda, J.; Jewell, J.; Keller, A. The Importance of the World Health Organization Sugar Guidelines for Dental Health and Obesity Prevention. Caries Res. 2019, 53, 149–152. [Google Scholar] [CrossRef] [PubMed]
- Hong, J.; Whelton, H.; Douglas, G.; Kang, J. Consumption Frequency of Added Sugars and UK Children’s Dental Caries. Community Dent. Oral Epidemiol. 2018, 46, 457–464. [Google Scholar] [CrossRef]
- Newens, K.J.; Walton, J. A Review of Sugar Consumption from Nationally Representative Dietary Surveys across the World. J. Hum. Nutr. Diet. 2016, 29, 225–240. [Google Scholar] [CrossRef] [PubMed]
- Azaïs-Braesco, V.; Sluik, D.; Maillot, M.; Kok, F.; Moreno, L.A. A Review of Total & Added Sugar Intakes and Dietary Sources in Europe. Nutr. J. 2017, 16, 6. [Google Scholar] [CrossRef] [PubMed]
- Come Mangia Tuo Figlio Scopri se ha Rischio di Sviluppare Carie. Available online: www.Pattoincucina.It/2020/07/16/Come-Mangia-Tuo-Figlio-Scopri-Se-Ha-Rischio-Di-Sviluppare-Carie (accessed on 6 April 2021).
- Data Reportal. 2020. Available online: https://Datareportal.Com/Reports/Digital-2020-Italy (accessed on 6 April 2021).
- Serra-Majem, L.; Ribas, L.; Ngo, J.; Ortega, R.M.; García, A.; Pérez-Rodrigo, C.; Aranceta, J. Food, Youth and the Mediterranean Diet in Spain. Development of KIDMED, Mediterranean Diet Quality Index in Children and Adolescents. Public Health Nutr. 2004, 7, 931–935. [Google Scholar] [CrossRef]
- La Sorveglianza HBSC 2018—Health Behaviour in School-Aged Children: Risultati dello Studio Italiano Tra i Ragazzi di 11, 13 e 15 Anni. Available online: www.iss.it/documents/20126/0/HBSC.pdf/97b1cfee-444c-bfd4-ab58-d0b1dcb504fb?t=1603882812589 (accessed on 12 May 2021).
- Società Italiana di Nutrizione Umana—SINU, LARN. 2014. Available online: https://Sinu.It/2019/07/09/Acqua/ (accessed on 12 May 2021).
- Pietrobelli, A.; Pecoraro, L.; Ferruzzi, A.; Heo, M.; Faith, M.; Zoller, T.; Antoniazzi, F.; Piacentini, G.; Fearnbach, S.N.; Heymsfield, S.B. Effects of COVID-19 Lockdown on Lifestyle Behaviors in Children with Obesity Living in Verona, Italy: A Longitudinal Study. Obesity 2020, 28, 1382–1385. [Google Scholar] [CrossRef]
- Medrano, M.; Cadenas-Sanchez, C.; Oses, M.; Arenaza, L.; Amasene, M.; Labayen, I. Changes in Lifestyle Behaviours during the COVID -19 Confinement in Spanish Children: A Longitudinal Analysis from the MUGI Project. Pediatr. Obes. 2021, 16, e12731. [Google Scholar] [CrossRef]
- Trichopoulou, A.; Martínez-González, M.A.; Tong, T.Y.; Forouhi, N.G.; Khandelwal, S.; Prabhakaran, D.; Mozaffarian, D.; de Lorgeril, M. Definitions and Potential Health Benefits of the Mediterranean Diet: Views from Experts around the World. BMC Med. 2014, 12, 112. [Google Scholar] [CrossRef] [PubMed]
- López-Bueno, R.; López-Sánchez, G.F.; Casajús, J.A.; Calatayud, J.; Gil-Salmerón, A.; Grabovac, I.; Tully, M.A.; Smith, L. Health-Related Behaviors Among School-Aged Children and Adolescents During the Spanish Covid-19 Confinement. Front. Pediatr. 2020, 8, 573. [Google Scholar] [CrossRef]
- Dunton, G.F.; Do, B.; Wang, S.D. Early Effects of the COVID-19 Pandemic on Physical Activity and Sedentary Behavior in Children Living in the U.S. BMC Public Health 2020, 20, 1351. [Google Scholar] [CrossRef] [PubMed]
- Bates, L.; Zieff, G.; Stanford, K.; Moore, J.; Kerr, Z.; Hanson, E.; Barone Gibbs, B.; Kline, C.; Stoner, L. COVID-19 Impact on Behaviors across the 24-Hour Day in Children and Adolescents: Physical Activity, Sedentary Behavior, and Sleep. Children 2020, 7, 138. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Henry, B.M.; Sanchis-Gomar, F. Physical Inactivity and Cardiovascular Disease at the Time of Coronavirus Disease 2019 (COVID-19). Eur. J. Prev. Cardiol. 2020, 27, 906–908. [Google Scholar] [CrossRef]
- Vozza, I.; Capasso, F.; Marrese, E.; Polimeni, A.; Ottolenghi, L. Infant and Child Oral Health Risk Status Correlated to Behavioral Habits of Parents or Caregivers: A Survey in Central Italy. J. Int. Soc. Prev. Community Dent. 2017, 7, 95. [Google Scholar] [CrossRef]
- McCormack, G.R.; Doyle-Baker, P.K.; Petersen, J.A.; Ghoneim, D. Parent Anxiety and Perceptions of Their Child’s Physical Activity and Sedentary Behaviour during the COVID-19 Pandemic in Canada. Prev. Med. Rep. 2020, 20, 101275. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, R.; Dubey, M.J.; Chatterjee, S.; Dubey, S. Impact of COVID -19 on Children: Special Focus on the Psychosocial Aspect. Minerva Pediatr. 2020, 72, S0026–S4946. [Google Scholar] [CrossRef]
- Scarmozzino, F.; Visioli, F. Covid-19 and the Subsequent Lockdown Modified Dietary Habits of Almost Half the Population in an Italian Sample. Foods 2020, 9, 675. [Google Scholar] [CrossRef]
- Ma, Y.; Ratnasabapathy, R.; Gardiner, J. Carbohydrate Craving: Not Everything Is Sweet. Curr. Opin. Clin. Nutr. Metab. Care 2017, 20, 261–265. [Google Scholar] [CrossRef] [PubMed]
- Philippe, K.; Chabanet, C.; Issanchou, S.; Monnery-Patris, S. Child Eating Behaviors, Parental Feeding Practices and Food Shopping Motivations during the COVID-19 Lockdown in France: (How) Did They Change? Appetite 2021, 161, 105132. [Google Scholar] [CrossRef] [PubMed]
- Jansen, E.; Thapaliya, G.; Aghababian, A.; Sadler, J.; Smith, K.; Carnell, S. Parental Stress, Food Parenting Practices and Child Snack Intake during the COVID-19 Pandemic. Appetite 2021, 161, 105119. [Google Scholar] [CrossRef]
- Linee Guida Nazionali per la Promo. Available online: www.salute.gov.it/imgs/C_17_pubblicazioni_2073_allegato.pdf (accessed on 6 April 2021).
- Wang, K.; Pang, L.; Fan, C.; Cui, T.; Yu, L.; Lin, H. Enamel and Dentin Caries Risk Factors of Adolescents in the Context of the International Caries Detection and Assessment System (ICDAS): A Longitudinal Study. Front. Pediatr. 2020, 8, 419. [Google Scholar] [CrossRef]
- Costacurta, M.; Di Renzo, L.; Bianchi, A.; Fabiocchi, F.; De Lorenzo, A.; Docimo, R. Obesity and Dental Caries in Paediatric Patients. A Cross-Sectional Study. Eur. J. Paediatr. Dent. 2011, 12, 112–116. [Google Scholar]
- Costacurta, M.; DiRenzo, L.; Sicuro, L.; Gratteri, S.; De Lorenzo, A.; Docimo, R. Dental Caries and Childhood Obesity: Analysis of Food Intakes, Lifestyle. Eur. J. Paediatr. Dent. 2014, 15, 343–348. [Google Scholar]
- Johansson, I.; Lif Holgerson, P.; Kressin, N.R.; Nunn, M.E.; Tanner, A.C. Snacking Habits and Caries in Young Children. Caries Res. 2010, 44, 421–430. [Google Scholar] [CrossRef] [PubMed]
- Lingström, P.; van Houte, J.; Kashket, S. Food Starches and Dental Caries. Crit. Rev. Oral. Biol. Med. 2000, 11, 366–380. [Google Scholar] [CrossRef] [PubMed]
- Du, Q.; Fu, M.; Zhou, Y.; Cao, Y.; Guo, T.; Zhou, Z.; Li, M.; Peng, X.; Zheng, X.; Li, Y.; et al. Sucrose Promotes Caries Progression by Disrupting the Microecological Balance in Oral Biofilms: An in Vitro Study. Sci. Rep. 2020, 10, 2961. [Google Scholar] [CrossRef] [PubMed]
- Hobbs, M.; Marek, L.; Clarke, R.; McCarthy, J.; Tomintz, M.; Wade, A.; Campbell, M.; Kingham, S. Investigating the Prevalence of Non-Fluoride Toothpaste Use in Adults and Children Using Nationally Representative Data from New Zealand: A Cross-Sectional Study. Br. Dent. J. 2020, 228, 269–276. [Google Scholar] [CrossRef] [PubMed]
- American Academy of Pediatric Dentistry. Fluoride Therapy. In The Reference Manual of Pediatric Dentistry; American Academy of Pediatric Dentistry: Chicago, IL, USA, 2020; pp. 288–291. [Google Scholar]
- Rugg-Gunn, A. Preventing the Preventable—The Enigma of Dental Caries. Br. Dent. J. 2001, 191, 478–488. [Google Scholar] [CrossRef]
- Ashkenazi, M.; Bidoosi, M.; Levin, L. Effect of Preventive Oral Hygiene Measures on the Development of New Carious Lesions. Oral Health Prev. Dent. 2014, 12, 61–69. [Google Scholar] [CrossRef]
- Calcagnile, F.; Pietrunti, D.; Pranno, N.; Di Giorgio, G.; Ottolenghi, L.; Vozza, I. Oral Health Knowledge in Pre-School Children: A Survey among Parents in Central Italy. J. Clin. Exp. Dent. 2019, 11, e327. [Google Scholar] [CrossRef]
- De Lorenzo, A.; Tarsitano, M.G.; Falcone, C.; Di Renzo, L.; Romano, L.; Macheda, S.; Ferrarelli, A.; Labate, D.; Tescione, M.; Bilotta, F.; et al. Fat mass affects nutritional status of ICU COVID-19 patients. J. Transl. Med. 2020, 18, 299. [Google Scholar] [CrossRef]
- Luzzi, V.; Ierardo, G.; Bossù, M.; Polimeni, A. Paediatric Oral Health during and after the COVID-19 Pandemic. Int. J. Paediatr. Dent. 2021, 31, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Brian, Z.; Weintraub, J.A. Oral Health and COVID-19: Increasing the Need for Prevention and Access. Prev. Chronic Dis. 2020, 17, 200266. [Google Scholar] [CrossRef] [PubMed]
- Thang Le, V.N.; Kim, J.G.; Yang, Y.M.; Lee, D.W. Risk Factors for Early Childhood Caries: An Umbrella Review. Pediatr. Dent. 2021, 43, 176–194. [Google Scholar]
- Chen, K.J.; Gao, S.S.; Duangthip, D.; Lo, E.C.M.; Chu, C.H. Randomized Clinical Trial on Sodium Fluoride with Tricalcium Phosphate. J. Dent. Res. 2021, 100, 66–73. [Google Scholar] [CrossRef] [PubMed]



| Whole Samples (n = 220) | p | |
|---|---|---|
| Age | 9.10 ± 2.86 | <0.001 |
| Gender (F) | 111 (50.5) | <0.001 |
| Weight (kg) | 35.84 ± 15.72 | <0.001 |
| Height (cm) | 137.01 ± 18.48 | <0.05 |
| BMI (kg/cm2) | 18.45 ± 17.74 | <0.001 |
| TMI (kg/cm2) | 13.63 ± 3.65 | <0.001 |
| Type of lactation (First 6 months) | ||
| Formula milk | 43 (19.5) | |
| Mixed lactation | 70 (31.8) | |
| Breastfeeding | 107 (48.6) | |
| n = 220 | |
|---|---|
| KIDMED TEST | |
| Had a fruit every day | 145 (65.9) |
| Had a second fruit every day | 72 (32.7) |
| Had fresh or cooked vegetables regularly once a day | 135 (61.4) |
| Had fresh or cooked vegetables more than once a day | 63 (28.6) |
| Consumed fish regularly (at least 2–3 times per week) | 110 (50.0) |
| Went more than once a week to a fast-food (hamburger) restaurant | 20 (9.1) |
| Liked pulses and ate them more than once a week | 111 (50.5) |
| Consumed pasta or rice almost every day (5 or more times per week) | 197 (89.5) |
| Had cereals or grains (bread, etc.) for breakfast | 131 (59.5) |
| Consumed nuts regularly (at least 2–3 times per week) | 61 (27.7) |
| Used olive oil at home | 219 (99.5) |
| Skipped breakfast | 56 (25.5) |
| Had a dairy product for breakfast (yogurt, milk, etc.) | 191 (86.8) |
| Had commercially baked goods or pastries for breakfast | 165 (75.0) |
| Had two yogurts and/or some cheese (40 g) daily | 65 (29.5) |
| Had sweets and candy several times every day | 110 (50.0) |
| KIDMED score | 5.00 [3.00] |
| Low adherence | 50 (22.7) |
| Medium adherence | 129 (58.6) |
| High adherence | 41 (18.6) |
| Eggs | 2.00 [1.00] |
| Water | |
| <1 Liters | 103 (46.8) |
| 1–2 L Liters | 102 (46.4) |
| >2 L Liters | 15 (6.8) |
| Eating-habit changes | |
| No change | 112 (50.9) |
| More sweets | 45 (20.5) |
| Less sweets | 15 (6.8) |
| Compensatory food and sedentary for boredom | 44 (20.0) |
| More sugary beverages | 4 (1.8) |
| Increase of sweets consumption (yes) | 113 (51.4) |
| before Lockdown (n = 220) | during Lockdown (n = 220) | p | |
|---|---|---|---|
| Use of fluoride toothpaste | |||
| Never | 34 (15.5) | 37 (16.8) | 0.025 |
| Sometimes | 65 (29.5) | 65 (29.5) | |
| Often | 50 (22.7) | 50 (22.7) | |
| Always | 71 (32.3) | 60 (30.9) | |
| Teeth brushing before going to sleep (yes) | 199 (90.5) | 195 (88.6) | 0.388 |
| Drinking/eating after brushing teeth (times/week) | 0.77 ± 1.41 | 1.08 ± 1.70 | <0.001 |
| Dental pain or discomfort (yes) | 22 (10.0) | ||
| Dental abscesses (yes) | 6 (2.7) | ||
| Toothpaste used | |||
| Personal | 146 (66.4) | ||
| Parents’ toothpaste | 72 (32.7) | ||
| None | 2 (0.9) | ||
| Tooth-brushing habits | |||
| Not changed | 165 (75.0) | ||
| Less frequency brushing | 33 (15.0) | ||
| More frequency brushing | 22 (10.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Docimo, R.; Costacurta, M.; Gualtieri, P.; Pujia, A.; Leggeri, C.; Attinà, A.; Cinelli, G.; Giannattasio, S.; Rampello, T.; Di Renzo, L. Cariogenic Risk and COVID-19 Lockdown in a Paediatric Population. Int. J. Environ. Res. Public Health 2021, 18, 7558. https://doi.org/10.3390/ijerph18147558
Docimo R, Costacurta M, Gualtieri P, Pujia A, Leggeri C, Attinà A, Cinelli G, Giannattasio S, Rampello T, Di Renzo L. Cariogenic Risk and COVID-19 Lockdown in a Paediatric Population. International Journal of Environmental Research and Public Health. 2021; 18(14):7558. https://doi.org/10.3390/ijerph18147558
Chicago/Turabian StyleDocimo, Raffaella, Micaela Costacurta, Paola Gualtieri, Alberto Pujia, Claudia Leggeri, Alda Attinà, Giulia Cinelli, Silvia Giannattasio, Tiziana Rampello, and Laura Di Renzo. 2021. "Cariogenic Risk and COVID-19 Lockdown in a Paediatric Population" International Journal of Environmental Research and Public Health 18, no. 14: 7558. https://doi.org/10.3390/ijerph18147558
APA StyleDocimo, R., Costacurta, M., Gualtieri, P., Pujia, A., Leggeri, C., Attinà, A., Cinelli, G., Giannattasio, S., Rampello, T., & Di Renzo, L. (2021). Cariogenic Risk and COVID-19 Lockdown in a Paediatric Population. International Journal of Environmental Research and Public Health, 18(14), 7558. https://doi.org/10.3390/ijerph18147558